Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Extended Kalman Filter
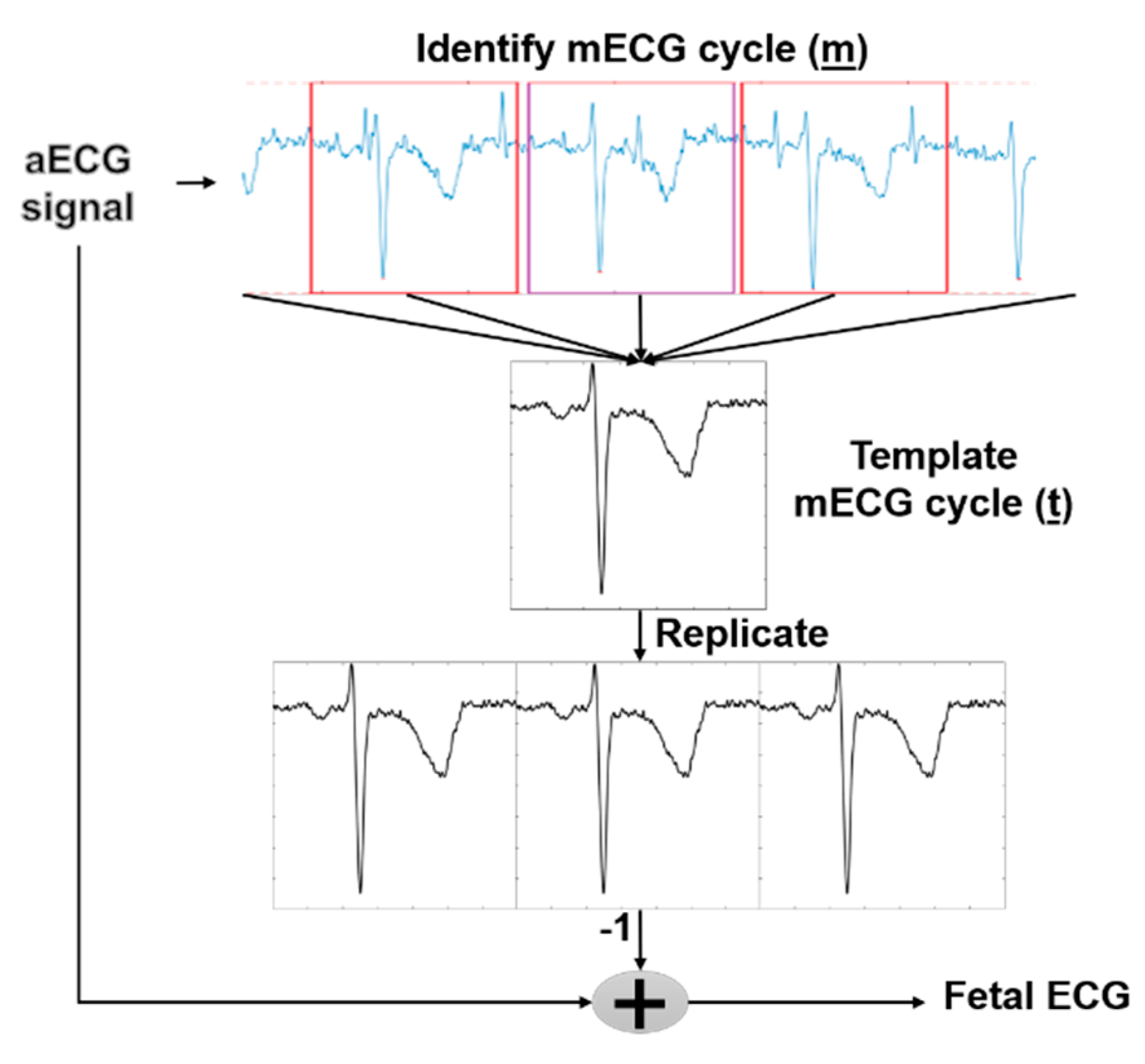
2.2. Template Subtraction (TS)
2.3. Independent Component Analysis (ICA)
| Algorithm 1: FastICA |
1.Pre-processing
|
| Algorithm 2: RobustICA |
| 1. No Pre-processing Required 2. Weight update
|
2.4. Fetal QRS Detection
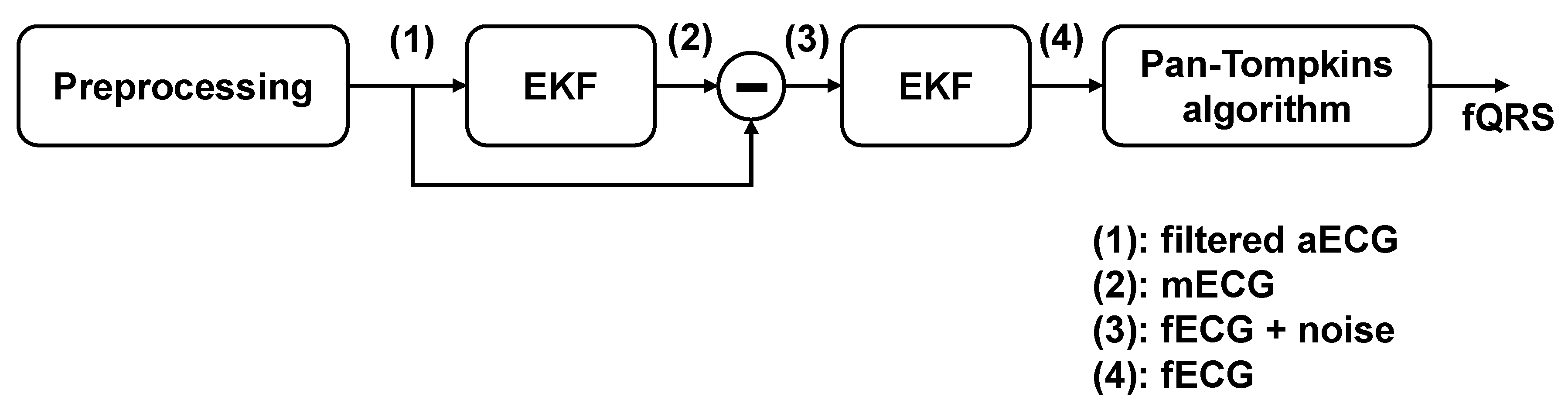
2.4.1. Fetal QRS Detection with EKF
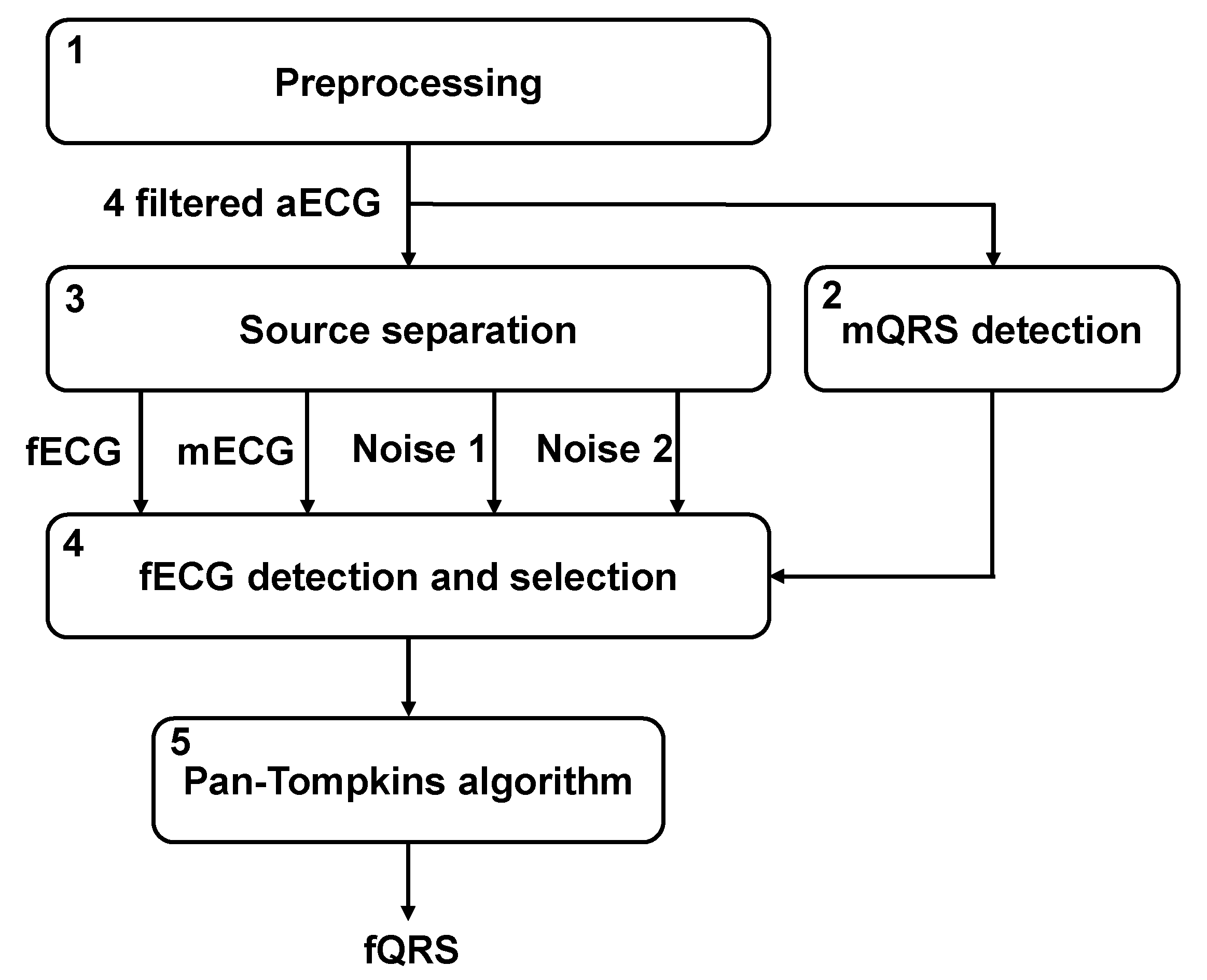
2.4.2. Fetal QRS Detection with TS, ICA and Their Combination
2.5. Experiments
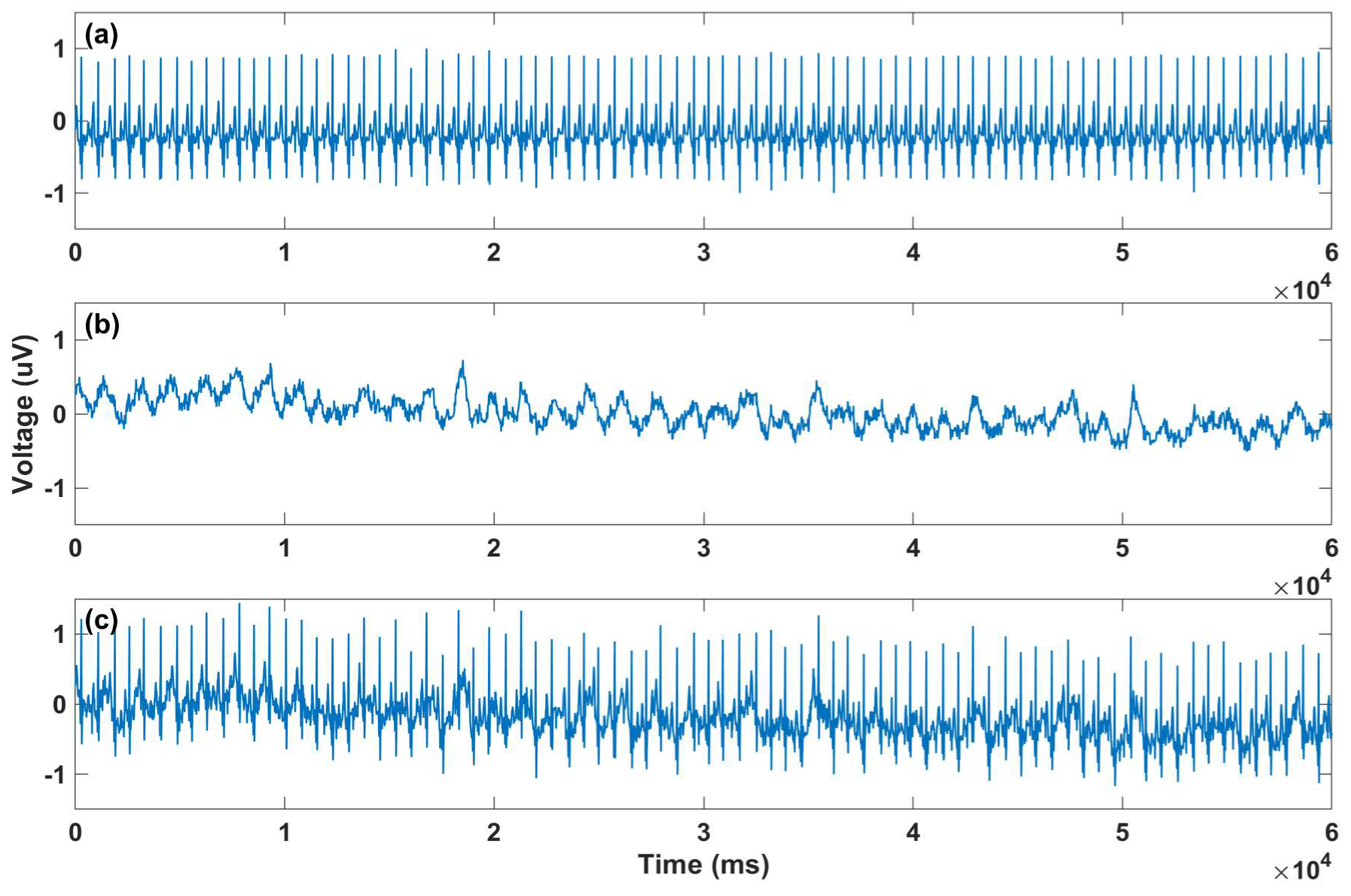
2.5.1. Modified Signals with Gaussian Noise Added
2.5.2. Modified Signals with Motional Artifacts Added
2.6. Comparison Schemes
2.6.1. F1 Score
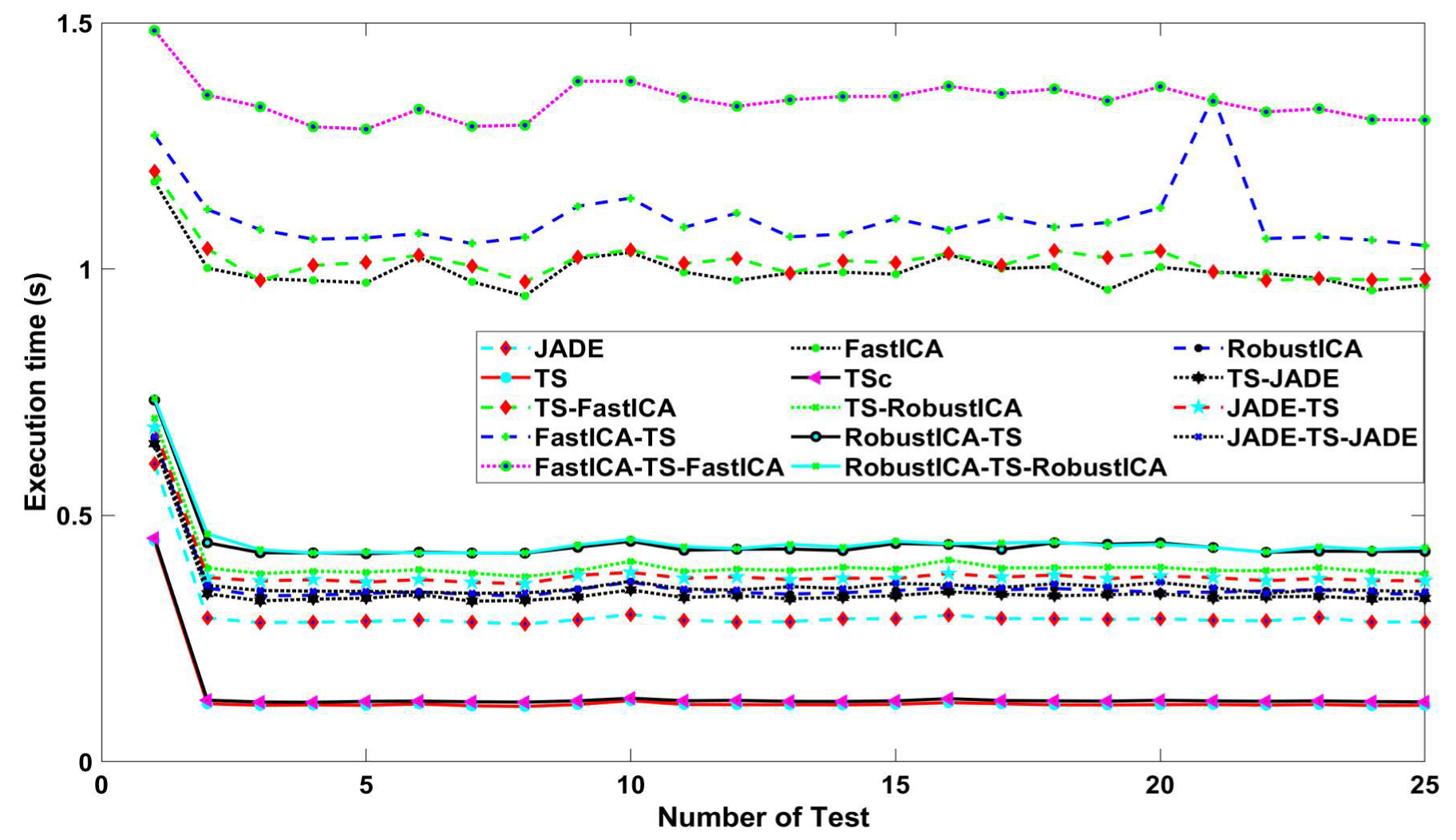
2.6.2. Time Execution
2.6.3. Allocated Memory
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gregory, E.C.W.; MacDorman, M.F.; Martin, J.A. Trends in Fetal and Perinatal Mortality in the United States, 2006–2012. Available online: https://www.cdc.gov/nchs/data/databriefs/db169.pdf (accessed on 4 June 2020).
- Hamelmann, P.; Vullings, R.; Kolen, A.F.; Bergmans, J.W.M.; van Laar, J.; Tortoli, P.; Mischi, M. Doppler Ultrasound Technology for Fetal Heart Rate Monitoring: A Review. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.C.A.; Braunlin, R.J.; Lansford, K.G.; Knoebel, S.B. Method for Obtaining a Fetal Electrocardiogram. U.S. Patent No 3,120,227, 4 Feburary 1964. [Google Scholar]
- Martinek, R.; Kahankova, R.; Nazeran, H.; Konecny, J.; Jezewski, J.; Janku, P.; Bilik, P.; Zidek, J.; Nedoma, J.; Fajkus, J. Non-Invasive Fetal Monitoring: A Maternal Surface ECG Electrode Placement-Based Novel Approach for Optimization of Adaptive Filter Control Parameters Using the LMS and RLS Algorithms. Sensors 2017, 17, 1154. [Google Scholar] [CrossRef] [PubMed]
- Fotiadou, E.; van Laar, J.O.E.H.; Oei, S.G.; Vullings, R. Enhancement of low-quality fetal electrocardiogram based on time-sequenced adaptive filtering. Med. Biol. Eng. Comput. 2018, 56, 2313–2323. [Google Scholar]
- Kaleem, A.M.; Kokate, R.D. An Efficient Adaptive Filter for Fetal ECG Extraction Using Neural Network. J. Intell. Syst. 2019, 28, 589. [Google Scholar] [CrossRef]
- Wu, S.; Shen, Y.; Zhou, Z.; Lin, L.; Zeng, Y.; Gao, X. Research of fetal ECG extraction using wavelet analysis and adaptive filtering. Comput. Biol. Med. 2013, 43, 1622–1627. [Google Scholar] [CrossRef]
- Sharma, M.; Ritchie, P.; Ghirmai, T.; Cao, H.; Lau, M.P. Unobtrusive acquisition and extraction of fetal and maternal ECG in the home setting. In Proceedings of the 2017 IEEE SENSORS, Glasgow, UK, 29 October–1 November 2017; pp. 1–3. [Google Scholar]
- Vullings, R.; Vries, B.d.; Bergmans, J.W.M. An Adaptive Kalman Filter for ECG Signal Enhancement. IEEE Trans. Biomed. Eng. 2011, 58, 1094–1103. [Google Scholar] [CrossRef] [Green Version]
- Suganthy, M.; Manjula, S. Enhancement of SNR in fetal ECG signal extraction using combined SWT and WLSR in parallel EKF. Clust. Comput. 2019, 22, 3875–3881. [Google Scholar] [CrossRef]
- Andreotti, F.; Riedl, M.; Himmelsbach, T.; Wedekind, D.; Zaunseder, S.; Wessel, N.; Malberg, H. Maternal signal estimation by Kalman filtering and Template Adaptation for fetal heart rate extraction. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 193–196. [Google Scholar]
- Jothi, S.; Prabha, K. Fetal Electrocardiogram Extraction Using Adaptive Neuro-fuzzy Inference Systems and Undecimated Wavelet Transform. IETE J. Res. 2012, 58, 469. [Google Scholar] [CrossRef]
- Martinek, R.; Kahankova, R.; Nedoma, J.; Fajkus, M.; Cholevova, K. Fetal ECG Preprocessing Using Wavelet Transform. In Proceedings of the 10th International Conference on Computer Modeling and Simulation, Sydney, Australia, 8–10 January 2018. [Google Scholar]
- Sameni, R. Extraction of Fetal Cardiac Signals from an Array of Maternal Abdominal Recordings. Ph.D. Thesis, Sharif University of Technology (SUT), Teheran, Iran, 2008. [Google Scholar]
- Gurve, D.; Pant, J.K.; Krishnan, S. Real-time fetal ECG extraction from multichannel abdominal ECG using compressive sensing and ICA. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; pp. 2794–2797. [Google Scholar]
- Rahmati, A.K.; Setarehdan, S.K.; Araabi, B.N. A PCA/ICA based Fetal ECG Extraction from Mother Abdominal Recordings by Means of a Novel Data-driven Approach to Fetal ECG Quality Assessment. J. Biomed. Phys. Eng. 2017, 7, 37–50. [Google Scholar]
- Martinek, R.; Kahankova, R.; Jezewski, J.; Jaros, R.; Mohylova, J.; Fajkus, M.; Nedoma, J.; Janku, P.; Nazeran, H. Comparative Effectiveness of ICA and PCA in Extraction of Fetal ECG From Abdominal Signals: Toward Non-invasive Fetal Monitoring. Front. Physiol. 2018, 9, 648. [Google Scholar] [CrossRef] [Green Version]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, U.; Nakamura, Y.; Yokouchi, H.; Hiroyasu, T. Improving the accuracy of the method for removing motion artifacts from fNIRS data using ICA and an accelerometer. In Proceedings of the 2014 World Automation Congress (WAC), Waikoloa, HI, USA, 3–7 August 2014; pp. 131–136. [Google Scholar]
- Yu, Q.; Yan, H.; Song, L.; Guo, W.; Liu, H.; Si, J.; Zhao, Y. Automatic identifying of maternal ECG source when applying ICA in fetal ECG extraction. Biocybern. Biomed. Eng. 2018, 38, 448–455. [Google Scholar] [CrossRef]
- Le, T.; Fortunato, J.; Maritato, N.; Cho, Y.; Nguyen, Q.; Ghirmai, T.; Cao, H.; Lau, M.P.H.; Han, H.D.; Nguyen, C.K.; et al. Home-based mobile fetal/maternal electrocardiogram acquisition and extraction with cloud assistance. In Proceedings of the 2019 IEEE MTT-S International Microwave Biomedical Conference (IMBioC), Nanjing, China, 6–8 May 2019; pp. 1–4. [Google Scholar]
- Ungureanu, M.; Johannes, W.M.B.; Swan, G.O.; Strungaru, R. Fetal ECG extraction during labor using an adaptive maternal beat subtraction technique. Biomed. Tech. 2007, 52, 56. [Google Scholar] [CrossRef] [PubMed]
- Varanini, M.; Tartarisco, G.; Billeci, L.; Macerata, A.; Pioggia, G.; Balocchi, R. An efficient unsupervised fetal QRS complex detection from abdominal maternal ECG. Physiol. Meas. 2014, 35, 1607–1619. [Google Scholar] [CrossRef] [PubMed]
- Zaunseder, S.; Andreotti, F.; Cruz, M.; Stepan, H.; Schmieder, C.; Malberg, H.; Wessel, N.; Jank, A. Fetal QRS detection by means of Kalman filtering and using the Event Synchronous Canceller. In Proceedings of the 7th International Workshop on Biosignal Interpretation, Como, Italy, 2–4 July 2012. [Google Scholar]
- Behar, J.; Oster, J.; Clifford, G.D. Combining and benchmarking methods of foetal ECG extraction without maternal or scalp electrode data. Physiol. Meas. 2014, 35, 1569–1589. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.J.; Lee, B. Sequential Total Variation Denoising for the Extraction of Fetal ECG from Single-Channel Maternal Abdominal ECG. Sensors 2016, 16, 1020. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Chen, D.; Sun, G. Detection of Fetal ECG R Wave From Single-Lead Abdominal ECG Using a Combination of RR Time-Series Smoothing and Template-Matching Approach. IEEE Access 2019, 7, 66633–66643. [Google Scholar] [CrossRef]
- Matonia, A.; Jezewski, J.; Horoba, K.; Gacek, A.; Labaj, P. The maternal ECG suppression algorithm for efficient extraction of the fetal ECG from abdominal signal. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 3106–3109. [Google Scholar]
- Clifford, G.D.; Silva, I.; Behar, J.; Moody, G.B. Non-invasive fetal ECG analysis. Physiol. Meas. 2014, 35, 1521–1536. [Google Scholar] [CrossRef]
- Silva, I.; Behar, J.; Sameni, R.; Zhu, T.; Oster, J.; Clifford, G.D.; Moody, G.B. Noninvasive fetal ECG: The PhysioNet/computing in cardiology challenge 2013. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 149–152. [Google Scholar]
- Behar, J.; Oster, J.; Clifford, G.D. Non-invasive FECG extraction from a set of abdominal sensors. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 297–300. [Google Scholar]
- Behar, J. Extraction of Clinical Information From the Non-Invasive Fetal Electrocardiogram. Ph.D. Thesis, University of Oxford, Oxford, UK, 2014. [Google Scholar]
- McSharry, P.E.; Clifford, G.D.; Tarassenko, L.; Smith, L.A. A dynamical model for generating synthetic electrocardiogram signals. IEEE Trans. Biomed. Eng. 2003, 50, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Sameni, R.; Shamsollahi, M.B.; Jutten, C.; Clifford, G.D. A nonlinear Bayesian filtering framework for ECG denoising. IEEE Trans. Biomed. Eng. 2007, 54, 2172–2185. [Google Scholar] [CrossRef] [Green Version]
- Cerutti, S.; Baselli, G.; Civardi, S.; Ferrazzi, E.; Anna, M.M.; Pagani, M.; Pardi, G. Variability analysis of fetal heart rate signals as obtained from abdominal electrocardiographic recordings. J. Perinat. Med.—Off. J. WAPM 1986, 14, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens, S.M.M.; Rabotti, C.; Mischi, M.; Sluijter, R.J. A robust fetal ECG detection method for abdominal recordings. Physiol. Meas. 2007, 28, 373–388. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.F.; Souloumiac, A. Blind beamforming for non-Gaussian signals. IEE Proc. F—Radar Signal Process. 1993, 140, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, J. High-Order Contrasts for Independent Component Analysis. Neural Comput. 1999, 11, 157–192. [Google Scholar] [CrossRef] [PubMed]
- Zarzoso, V.; Comon, P. Robust Independent Component Analysis by Iterative Maximization of the Kurtosis Contrast With Algebraic Optimal Step Size. IEEE Trans. Neural Netw. 2010, 21, 248–261. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Without Motion Noise | With Motion Noise |
|---|---|---|
| TS-FastICA | 92.61 | 85.02 |
| JADE-TS-JADE | 91.56 | 85.43 |
| TS-JADE | 91.16 | 82.35 |
| TS-RobustICA | 90.71 | 80.63 |
| JADE-TS | 90.57 | 85.10 |
| RobustICA-TS-RobustICA | 89.29 | 82.67 |
| RobustICA-TS | 87.43 | 83.21 |
| FastICA-TS-FastICA | 87.07 | 82.47 |
| TSc | 83.12 | 70.64 |
| FastICA-TS | 82.96 | 77.94 |
| TS | 82.65 | 71.02 |
| JADE | 61.27 | 59.81 |
| FastICA | 60.08 | 59.38 |
| RobustICA | 59.60 | 58.74 |
| EKF | 54.34 | 51.45 |
| Method | Without Motion Noise | With Motion Noise |
|---|---|---|
| EKF | 38 | 40 |
| RobustICA | 28 | 28 |
| FastICA | 22 | 27 |
| JADE | 18 | 19 |
| TSc | 10 | 17 |
| TS | 10 | 17 |
| FastICA-TS | 6 | 9 |
| FastICA-TS-FastICA | 5 | 5 |
| RobustICA-TS | 5 | 5 |
| RobustICA-TS-RobustICA | 2 | 5 |
| TS-RobustICA | 2 | 8 |
| TS-JADE | 1 | 7 |
| TS-FastICA | 1 | 4 |
| JADE-TS-JADE | 1 | 1 |
| JADE-TS | 0 | 3 |
| Method | Required Memory (MB) |
|---|---|
| EKF | 2940 |
| JADE-TS | 1222 |
| TS | 1220 |
| TS-FastICA | 1211 |
| TS-RobustICA | 1210 |
| FastICA-TS | 1206 |
| TSc | 1205 |
| TS-JADE | 1204 |
| RobustICA-TS-RobustICA | 1202 |
| RobustICA-TS | 1199 |
| FastICA-TS-FastICA | 1199 |
| RobustICA | 1199 |
| JADE-TS-JADE | 1192 |
| FastICA | 1183 |
| JADE | 1175 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarafan, S.; Le, T.; Naderi, A.M.; Nguyen, Q.-D.; Kuo, B.T.-Y.; Ghirmai, T.; Han, H.-D.; Lau, M.P.H.; Cao, H. Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios. Technologies 2020, 8, 33. https://doi.org/10.3390/technologies8020033
Sarafan S, Le T, Naderi AM, Nguyen Q-D, Kuo BT-Y, Ghirmai T, Han H-D, Lau MPH, Cao H. Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios. Technologies. 2020; 8(2):33. https://doi.org/10.3390/technologies8020033
Chicago/Turabian StyleSarafan, Sadaf, Tai Le, Amir Mohammad Naderi, Quoc-Dinh Nguyen, Brandon Tiang-Yu Kuo, Tadesse Ghirmai, Huy-Dung Han, Michael P. H. Lau, and Hung Cao. 2020. "Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios" Technologies 8, no. 2: 33. https://doi.org/10.3390/technologies8020033
APA StyleSarafan, S., Le, T., Naderi, A. M., Nguyen, Q. -D., Kuo, B. T. -Y., Ghirmai, T., Han, H. -D., Lau, M. P. H., & Cao, H. (2020). Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios. Technologies, 8(2), 33. https://doi.org/10.3390/technologies8020033