
Reflective Practice in Healthcare Education: An Umbrella Review


Abstract
:1. Introduction
- Which models and definitions of reflection and reflective practice are in use?
- How does empirical research depict reflective practice in healthcare education (the design and evaluation of education interventions)?
- What are the future directions of reflective research and practice in healthcare education?
2. Materials and Methods
2.1. Identification of Relevant Studies
2.2. Search Method, Data Extraction, and Quality Assessment
2.3. Theoretical Stance
3. Results
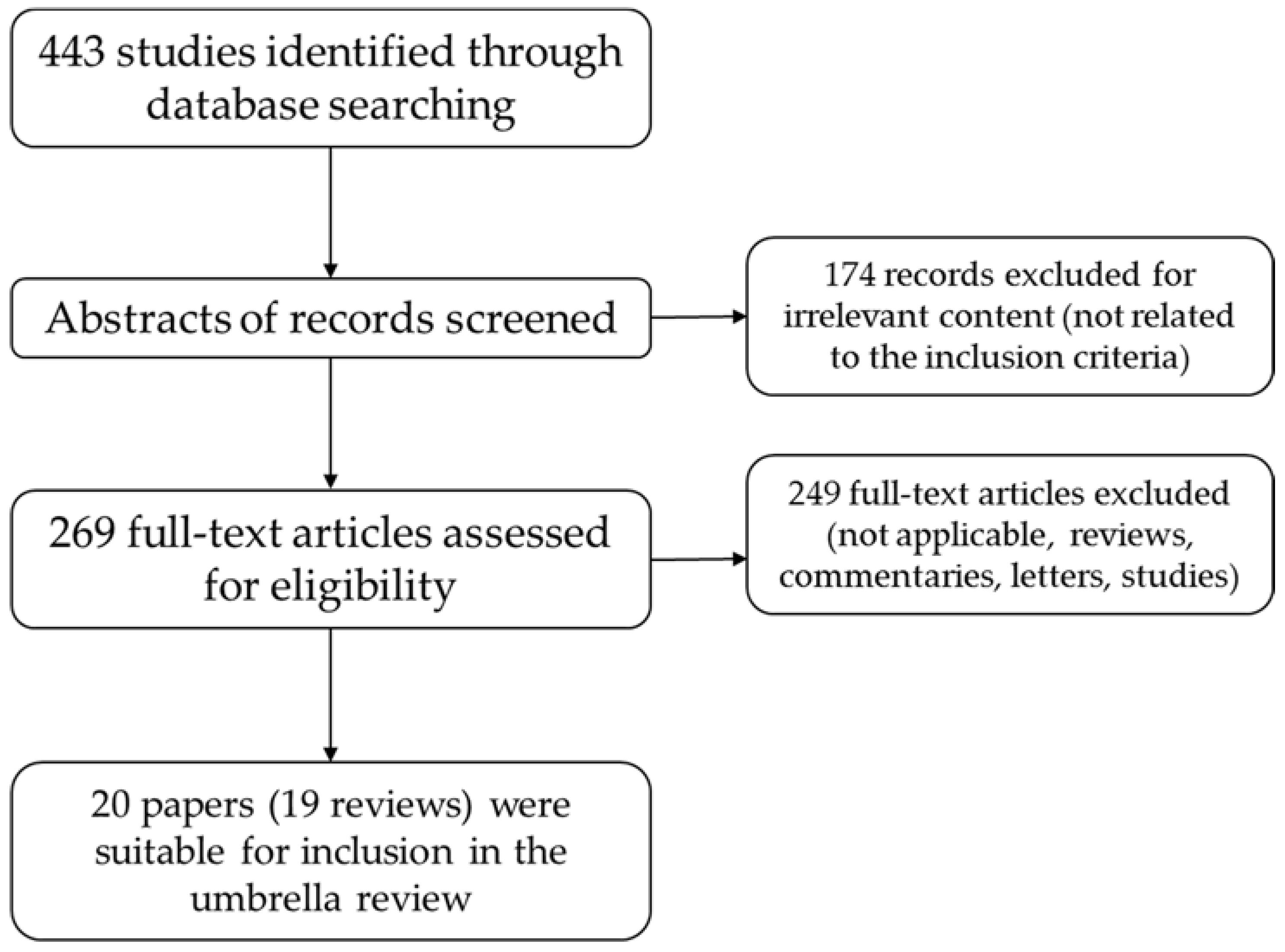
3.1. Description of Studies
3.2. Methodological Quality
3.3. Which Models and Definitions of Reflection and Reflective Practice Are Used?
3.4. How Does Empirical Research Depict Reflective Practice in Healthcare Education (Design and Evaluation of Education Interventions)?
3.5. What Are the Future Directions of Reflective Research and Practice in Healthcare Education?
4. Discussion and Conclusions
Conflicts of Interest
Abbreviations
| AMSTAR | Assessing the Methodological Quality of Systematic Reviews |
References
- Glazer, N. The schools of the minor professions. Minerva 1974, 12, 346–364. [Google Scholar] [CrossRef]
- Schön, D.A. The Reflective Practitioner: How Professionals Think in Action; Basic Books: New York, NY, USA, 1983. [Google Scholar]
- Frenk, J.; Chen, L.; Bhutta, Z.A.; Cohen, J.; Crisp, N.; Evans, T.; Fineberg, H.; Garcia, P.; Ke, Y.; Kelley, P.; et al. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. Lancet 2010, 376, 1923–1958. [Google Scholar] [CrossRef]
- Noar, S.M.; Zimmerman, R.S. Health behavior theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Educ. Res. 2005, 20, 275–290. [Google Scholar] [CrossRef] [PubMed]
- Zibrowski, E.M.; Weston, W.W.; Goldszmidt, M.A. “I don’t have time”: Issues of fragmentation, prioritisation and motivation for education scholarship among medical faculty. Med. Educ. 2008, 42, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, D.M.; Mann, K.V. Teaching and learning in medical education: How theory can inform practice. In Understanding Medical Education, 2nd ed.; Swanwick, T., Ed.; Wiley: Chichester, UK, 2014; pp. 16–36. [Google Scholar]
- Schön, D.A. Educating the Reflective Practitioner: Toward a New Design for Teaching and Learning in the Professions, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Onyura, B.; Baker, L.; Cameron, B.; Friesen, F.; Leslie, K. Evidence for curricular and instructional design approaches in undergraduate medical education: An umbrella review. Med. Teach. 2016, 38, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Tsagris, M.; Fragkos, K.C. Umbrella reviews, overviews of reviews, and meta-epidemiologic studies: Similarities and differences. In Umbrella Reviews: Evidence Synthesis with Overviews of Reviews and Meta-Epidemiologic Studies; Biondi-Zoccai, G., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 43–54. [Google Scholar]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Bouter, L.M.; Peterson, J.; Boers, M.; Andersson, N.; Ortiz, Z.; Ramsay, T.; Bai, A.; Shukla, V.K.; Grimshaw, J.M. External validation of a measurement tool to assess systematic reviews (amstar). PLoS ONE 2007, 2, e1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of amstar: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgley, A.; Stickley, T.; Timmons, S.; Meal, A. Critical realist review: Exploring the real, beyond the empirical. J. Furth. High. Educ. 2016, 40, 316–330. [Google Scholar] [CrossRef]
- Clegg, S. Evidence-based practice in educational research: A critical realist critique of systematic review. Br. J. Sociol. Educ. 2005, 26, 415–428. [Google Scholar] [CrossRef]
- Petitmengin, C. Describing one’s subjective experience in the second person: An interview method for the science of consciousness. Phenomenol. Cogn. Sci. 2006, 5, 229–269. [Google Scholar] [CrossRef]
- Williams, B. Developing critical reflection for professional practice through problem-based learning. J. Adv. Nurs. 2001, 34, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, R.A.; Pesut, D.J. Promoting cognitive and metacognitive reflective reasoning skills in nursing practice: Self-regulated learning theory. J. Adv. Nurs. 2004, 45, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Rushmer, R.; Kelly, D.; Lough, M.; Wilkinson, J.E.; Davies, H.T. Introducing the learning practice—III. Leadership, empowerment, protected time and reflective practice as core contextual conditions. J. Eval. Clin. Pract. 2004, 10, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Crowe, M.T.; O’Malley, J. Teaching critical reflection skills for advanced mental health nursing practice: A deconstructive-reconstructive approach. J. Adv. Nurs. 2006, 56, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Epp, S. The value of reflective journaling in undergraduate nursing education: A literature review. Int. J. Nurs. Stud. 2008, 45, 1379–1388. [Google Scholar] [CrossRef] [PubMed]
- Buckley, S.; Coleman, J.; Davison, I.; Khan, K.S.; Zamora, J.; Malick, S.; Morley, D.; Pollard, D.; Ashcroft, T.; Popovic, C.; et al. The educational effects of portfolios on undergraduate student learning: A best evidence medical education (beme) systematic review. Beme guide No. 11. Med. Teach. 2009, 31, 282–298. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.; Gordon, J.; MacLeod, A. Reflection and reflective practice in health professions education: A systematic review. Adv. Health Sci. Educ. Theory Pract. 2009, 14, 595–621. [Google Scholar] [CrossRef] [PubMed]
- Lethbridge, K.; Andrusyszyn, M.A.; Iwasiw, C.; Laschinger, H.K.; Fernando, R. Structural and psychological empowerment and reflective thinking: Is there a link? J. Nurs. Educ. 2011, 50, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Chaffey, L.J.; de Leeuw, E.J.; Finnigan, G.A. Facilitating students’ reflective practice in a medical course: Literature review. Educ. Health (Abingdon) 2012, 25, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Norrie, C.; Hammond, J.; D’Avray, L.; Collington, V.; Fook, J. Doing it differently? A review of literature on teaching reflective practice across health and social care professions. Reflect. Pract. 2012, 13, 565–578. [Google Scholar] [CrossRef]
- Prasko, J.; Mozny, P.; Novotny, M.; Slepecky, M.; Vyskocilova, J. Self-reflection in cognitive behavioural therapy and supervision. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. Repub. 2012, 156, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Jayatilleke, N.; Mackie, A. Reflection as part of continuous professional development for public health professionals: A literature review. J. Public Health (Oxf.) 2013, 35, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.; Forbes, C. Reflective writing and its impact on empathy in medical education: Systematic review. J. Educ. Eval. Health Prof. 2014, 11, 20. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.D.; Fernandez, N.; Karsenti, T.; Charlin, B. What is reflection? A conceptual analysis of major definitions and a proposal of a five-component model. Med. Educ. 2014, 48, 1176–1189. [Google Scholar] [CrossRef] [PubMed]
- McGillivray, J.; Gurtman, C.; Boganin, C.; Sheen, J. Self-practice and self-reflection in training of psychological interventions and therapist skills development: A qualitative meta-synthesis review. Aust. Psychol. 2015, 50, 434–444. [Google Scholar] [CrossRef]
- Miraglia, R.; Asselin, M.E. Reflection as an educational strategy in nursing professional development: An integrative review. J. Nurses Prof. Dev. 2015, 31, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.L.; Kinsella, E.A.; Friesen, F.; Hodges, B. Reclaiming a theoretical orientation to reflection in medical education research: A critical narrative review. Med. Educ. 2015, 49, 461–475. [Google Scholar] [CrossRef] [PubMed]
- Tsingos, C.; Bosnic-Anticevich, S.; Lonie, J.M.; Smith, L. A model for assessing reflective practices in pharmacy education. Am. J. Pharm. Educ. 2015, 79, 124. [Google Scholar] [CrossRef] [PubMed]
- Tsingos, C.; Bosnic-Anticevich, S.; Smith, L. Learning styles and approaches: Can reflective strategies encourage deep learning? Curr. Pharm. Teach. Learn. 2015, 7, 492–504. [Google Scholar] [CrossRef]
- Van Roy, K.; Vanheule, S.; Inslegers, R. Research on balint groups: A literature review. Patient Educ. Couns. 2015, 98, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Atkins, S.; Murphy, K. Reflection: A review of the literature. J. Adv. Nurs. 1993, 18, 1188–1192. [Google Scholar] [CrossRef] [PubMed]
- Carkhuff, M.H. Reflective learning: Work groups as learning groups. J. Contin. Educ. Nurs. 1996, 27, 209–214. [Google Scholar] [PubMed]
- Heath, H. Keeping a reflective practice diary: A practical guide. Nurse Educ. Today 1998, 18, 592–598. [Google Scholar] [CrossRef]
- Mackintosh, C. Reflection: A flawed strategy for the nursing profession. Nurse Educ. Today 1998, 18, 553–557. [Google Scholar] [CrossRef]
- Rooke, T.R. A critical review of reflective practice in its role towards personal and professional development. J. R. Nav. Med. Serv. 1998, 84, 66–70. [Google Scholar] [PubMed]
- Clouder, L. Reflective practice in physiotherapy education: A critical conversation. Stud. High. Educ. 2000, 25, 211–223. [Google Scholar] [CrossRef]
- Donaghy, M.E.; Morss, K. Guided reflection: A framework to facilitate and assess reflective practice within the discipline of physiotherapy. Physiother. Theory Pract. 2000, 16, 3–14. [Google Scholar] [CrossRef]
- Cotton, A.H. Private thoughts in public spheres: Issues in reflection and reflective practices in nursing. J. Adv. Nurs. 2001, 36, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C. Remembrance of things past: The utilisation of context dependant and autobiographical recall as means of enhancing reflection on action in nursing. Nurse Educ. Today 2004, 24, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Schutz, S. Reflection and reflective practice. Community Pract. 2007, 80, 26–29. [Google Scholar] [PubMed]
- Fowler, J. Experiential learning and its facilitation. Nurse Educ. Today 2008, 28, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Sandars, J. The use of reflection in medical education: Amee guide No. 44. Med. Teach. 2009, 31, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Koole, S.; Dornan, T.; Aper, L.; Scherpbier, A.; Valcke, M.; Cohen-Schotanus, J.; Derese, A. Factors confounding the assessment of reflection: A critical review. BMC Med. Educ. 2011, 11, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, A.W.; Gorgas, D.; Greenberger, S.; Jacques, A.; Khandelwal, S. The use of reflection in emergency medicine education. Acad. Emerg. Med. 2012, 19, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Murdoch-Eaton, D.; Sandars, J. Reflection: Moving from a mandatory ritual to meaningful professional development. Arch. Dis. Child. 2014, 99, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Wald, H.S. Refining a definition of reflection for the being as well as doing the work of a physician. Med. Teach. 2015, 37, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Dewey, J. How We Think, a Restatement of the Relation of Reflective Thinking to the Educative Process; D.C. Heath and Company: Boston, MA, USA; New York, NY, USA, 1933. [Google Scholar]
- Argyris, C.; Schön, D.A. Theory in Practice: Increasing Professional Effectiveness; Jossey-Bass: San Francisco, CA, USA, 1974. [Google Scholar]
- Argyris, C.; Schön, D.A. Organizational Learning: A Theory of Action Perspective; Addison-Wesley Reading: MA, USA, 1978. [Google Scholar]
- Boyd, E.M.; Fales, A.W. Reflective learning—Key to learning from experience. J. Humanist. Psychol. 1983, 23, 99–117. [Google Scholar] [CrossRef]
- Kolb, D.A. Experiential Learning: Experience as the Source of Learning and Development; Prentice-Hall: Englewood Cliffs, NJ, USA; London, UK, 1984. [Google Scholar]
- Boud, D.; Keogh, R.; Walker, D. Reflection, Turning Experience into Learning; Kogan Page; Nichols Pub.: London, UK; New York, NY, USA, 1985. [Google Scholar]
- Mezirow, J. Transformative Dimensions of Adult Learning, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1991. [Google Scholar]
- Van Manen, M. Linking ways of knowing with ways of being practical. Curric. Inq. 1977, 6, 205–228. [Google Scholar] [CrossRef]
- Van Manen, M. On the epistemology of reflective practice. Teach. Teach. Theory Pract. 1995, 1, 33–50. [Google Scholar] [CrossRef]
- Turner, S. Safeguarding children training in adult mental health care. Ment. Health Pract. 2009, 12, 28–32. [Google Scholar] [CrossRef]
- Kemp, P.; Rooks, J.; Mess, L. Work-based learning with staff in an acute care environment: A project review and evaluation. Ment. Health Pract. 2009, 12, 31–35. [Google Scholar] [CrossRef]
- Jenkins, E. Using cooperative inquiry and clinical supervision to improve practice. Br. J. Community Nurs. 2007, 12, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Ménard, L.; Ratnapalan, S. Reflection in medicine: Models and application. Can. Fam. Phys. 2013, 59, 105–107. [Google Scholar]
- Sobral, D.T. Medical students’ reflection in learning in relation to approaches to study and academic achievement. Med. Teach. 2001, 23, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Mamede, S.; Schmidt, H.G. The structure of reflective practice in medicine. Med. Educ. 2004, 38, 1302–1308. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Objective and Methods | Summary of Findings | AMSTAR Score |
|---|---|---|---|
| Williams [16] | Objective: To explore the influence of current learning traditions in nursing on the development of reflection and critical reflection as professional practice skills and to offer suggestions for nursing education for development of critical reflection. Organizational constructs: Mezirow’s transformative learning theory, Barrows conceptualization of problem-based learning. Integrative literature review of published literature related to nursing, health science education and professional education from 1983–2000. | Level of education: undergraduate, graduate, postgraduate Learner profession: nursing Findings: Specialized knowledge is clearly essential for professional practice; Self-consciousness (reflection) and continual self-critique (critical reflection) are crucial to continued competence. Strategies to facilitate reflection have been outlined in the literature, specific strategies to facilitate the development of critical reflection are less described. Development of these abilities should be linked to professional development and developed through active repeated guided practice. Problem based learning based on constructivism helps develop this skills. | 2 |
| Kuiper and Pesut [17] | Objective: To explore the impact of self-regulated learning theory on reflective practice in nursing, and to advance the idea that both cognitive and metacognitive skills support the development of clinical reasoning skills. Integrative review of published literature in social science, educational psychology, nursing education, and professional education | Level of education: undergraduate, graduate, postgraduate Learner profession: nursing Findings: Reflective clinical reasoning in nursing practice depends on the development of both cognitive and metacognitive skill acquisition. This skill acquisition is best accomplished through teaching-learning attention to self-regulation learning theory. | 4 |
| Rushmer, Kelly, Lough, Wilkinson and Davies [18] | Systematic literature review of contextual factors that play a key role in providing a facilitative context for a Learning Practice or manifest themselves as barriers to any Practice’s attempts to develop a learning culture. | Level of education: undergraduate, graduate, postgraduate Learner profession: healthcare Findings: Core contextual conditions are identified the requirement for strong and visionary leadership; the involvement and empowerment of staff; and setting-aside of times and places for learning and reflection. | 2 |
| Crowe and O’Malley [19] | Objective: Literature review conducted to establish what was already known about critical reflection in the nursing literature and what work had been done on using a critical social theory framework as the basis for critical reflection. | Level of education: undergraduate, graduate, postgraduate Learner profession: nursing, mental health nursing Findings: There were 490 articles related to “nursing” and “critical thinking”; 34 articles related to “nursing” and “critical reflection”; 23 articles related to “nursing” and “critical social theory”; 15 articles related to “mental health nursing” and “critical thinking”; and two articles related to “mental health nursing” and “critical reflection” Students were facilitated to deconstruct concepts and knowledge integral to their own practice. In the reconstructive phase, students implement a change project in clinical practice, supported by a mentor | 5 |
| Epp [20] | Objective: to ascertain the evidence for the use of reflective journaling as a tool to promote the pedagogical strategy of reflection for the purpose of learning from practice for practice in undergraduate nursing education. Systematic literature from 1992 to 2006. Nine studies met the inclusion criteria. | Level of education: undergraduate Learner profession: nursing, physiotherapy Findings: Educators struggle to incorporate reflective processes into education; research provided rationale and support for engaging undergraduate students in the reflective process. Researchers found reasonable levels of reflection in undergraduate students’ journaling and educators reported students’ learning as a result of reflective journaling. Writing reflectively improved over time; a learned skill also dependent on a good facilitator and trust. | 5 |
| Buckley, Coleman, Davison, Khan, Zamora, Malick, Morley, Pollard, Ashcroft, Popovic and Sayers [21] | Objective: A systematic review to assess use of portfolios in undergraduate education. Sixty-nine studies included (medicine, nursing, allied health professionals). | Level of education: undergraduate Learner profession: medicine, nursing, allied health professionals Findings: Portfolios were used mainly in the clinical setting, completion was mostly compulsory, reflection required and assessment (either formative, summative or a combination of both) the norm. Nine of the studies reported direct measurement of changes in student skills or attitudes and one study reported a change in student behaviour. The main effects of portfolio use identified by the included studies were: improvement in student knowledge and understanding, greater self-awareness and encouragement of reflection and the ability to learn independently, greater self-awareness and engagement in reflection. | 12 |
| Mann, Gordon and MacLeod [22] | Objective: systematic review of the research literature in the area of reflection and reflective learning in health professional education and practice. Twenty-nine studies identified | Level of education: undergraduate, graduate or postgraduate Learner profession: medicine, nursing, other health professions Findings: Eight studies explored reflective practice in practicing professionals; six were in medicine, and two in nursing. Reflection was a part of practice in all eight reports. Eight studies explored reflection in medical and health professions students, relating it to learning, professional identity development, and critical thinking Nine studies addressed whether reflective practice can be assessed. In several of the studies, relationships with other variables were explored, as a means of validating the instruments used and assessments made. Four studies addressed the development of reflective thinking. Twelve studies addressed the contextual influences which hinder or enable the development of reflection and reflective capability. | 7 |
| Lethbridge, Andrusyszyn, Iwasiw, Laschinger and Fernando [23] | Objective: integrative literature review; three concepts are examined and linked-structural empowerment (as conceptualized by Kanter), psychological empowerment (as described by Spreitzer), and reflective thinking (as characterized by Mezirow)-and a theoretical model for testing is proposed. Three dominant theories identified | Level of education: undergraduate or postgraduate Learner profession: nursing Findings: Students’ perceptions of empowerment in the nursing profession begin to form during their studies, and they are introduced to the process of reflective thinking. All three are required for learning and nursing practice. By preparing students to be empowered, reflective professionals, it is proposed that they will be more effective in their academic and future practice work. | 5 |
| Chaffey, de Leeuw and Finnigan [24] | Systematic review of the literature was undertaken using defined databases and the search terms “medical students”, “medical education”, “reflection”, “reflectFNx01” and “medicine”. The search was limited to peer-reviewed published material in English and between the years 2001 and 2011, and included research, reviews and opinion pieces. | Level of education: undergraduate, graduate or postgraduate Learner profession: medicine Findings: Thirty-six relevant articles identifying enhancing factors and barriers to effectively teaching reflective practice within medical curricula, relating to: The breadth of the meaning of reflection; facilitating reflection by medical educators; using written or web-based portfolios to facilitate reflection; and assessing the reflective work of students. | 6 |
| Norrie, Hammond, D’Avray, Collington and Fook [25] | Objective: What types of literature were found? What were the justifications for and criticisms of teaching reflection in the different professions? What were the learning contexts and the pedagogical approaches for teaching and assessing reflection in the different professions? Fifty-two studies included in review after systematic literature search | Level of education: undergraduate, graduate or postgraduate Learner profession: nursing, midwifery, physiotherapists, social work, multi/interprofessional Findings: the study identified and categorised literature available on teaching reflective practice in health and social care and compared this with what was available interprofessionally and multiprofessionally. Identified common reflective teaching methods and assessment methods. | 7 |
| Prasko, Mozny, Novotny, Slepecky and Vyskocilova [26] | Objective: To review aspects related to supervision in cognitive behavioural therapy and self-reflection in the literature. A literature review was performed using the PubMed, SciVerse Scopus, and Web of Science databases; additional references were found through bibliography reviews of relevant articles published prior to July 2011. | Level of education: undergraduate, graduate or postgraduate Learner profession: Therapists Findings: Self-reflection in therapy is a continuous process which is essential for the establishment of a therapeutic relationship, the professional growth of the therapist, and the ongoing development of therapeutic skills. The ability to self-reflect increases the ability to perceive other people’s inner emotions, kindles altruism, and increases attunement to subtle signals indicating what others need or want. Self-reflection may be practised by the therapists themselves using traditional cognitive behavioural therapy techniques, or it may be learned in the course of supervision. | 4 |
| Jayatilleke and Mackie [27] | Objective: To investigate the reported contribution, of reflection by public health workers as part of their professional practice. A systematic review of the literature to identify reflective experience in public health or health education. Thirteen papers met the inclusion criteria and were reviewed | Level of education: undergraduate, graduate or postgraduate Learner profession: nursing, allied health professionals Findings: Limited but growing evidence to suggest reflection improves practice in disciplines allied to public health. No specific models are currently recommended or widely used in public health. | 5 |
| Chen and Forbes [28] | Objective: to find the emotional effects of reflective writing interventions on medical and healthcare students Systematic literature Review with 8 final publications analysed | Level of education: undergraduate or graduate Learner profession: Medical students, pharmacy students Findings: The outcomes measured included impact of reflective writing exercises on student wellness, aptitude, and/or clinical skills. Of these studies, a significant change in student empathy was observed in 100% of the studies, demonstrating a significant change in outcomes. | 6 |
| Nguyen, Fernandez, Karsenti and Charlin [29] | Objective: to identify, explore and analyse the most influential conceptualisations of reflection, and to develop a new theory-informed and unified definition and model of reflection. Systematic review to identify the 15 most cited authors in papers on reflection published during the period from 2008 to 2012 (74 papers) An exploratory thematic analysis was carried out and identified seven initial categories. Categories were clustered and reworded to develop an integrative definition and model of reflection, which feature core components that define reflection and extrinsic elements that influence instances of reflection. | Level of education: undergraduate, graduate or postgraduate Learner profession: Medical Education Five core components of reflection and two extrinsic elements were identified: Reflection is defined as the process of engaging the self in attentive, critical, exploratory and iterative interactions with one’s thoughts and actions, and their underlying conceptual frame, with a view to changing them and a view on the change itself. Extrinsic elements: are the trigger of reflection and the context of reflection. | 7 |
| McGillivray, Gurtman, Boganin and Sheen [30] | Objective: To investigate the effect of self-practice and self-reflection on therapist skills development. Systematic Review of English studies that investigated the effect of self-practice and/or self-reflection on therapist skill development. No restriction on sample sizes, design of studies, dates of publication, or peer-reviewed papers. | Level of education: undergraduate, graduate or postgraduate Learner profession: Therapists Findings: Ten studies included in review. The meta-synthesis revealed inconsistencies between the qualitative and quantitative literature and a gap in relation to declarative knowledge. Six themes identified: improved technical skills, increased self-awareness, increased interpersonal, perceptual, and relational skills, appreciation for the limitations and value of the therapeutic model, increased empathy for clients, understanding of discomfort associated with self-disclosure. | 11 |
| Miraglia and Asselin [31] | Systematic review of the literature. 25 English studies that explored reflective education strategies in pot license nurses in a clinical setting. | Level of education: postgraduate Learner profession: Nursing (nursing professional development) Findings: Two themes for reflection as educational strategy: meeting a specific clinical practice goal and teaching nurses how to reflect to enhance individual reflective practice. Three themes emerged regarding the way in which reflection was used as an educational strategy: reflection nested into multifaceted educational programs, individual- versus group-facilitated reflection, and structured versus unstructured reflection. Overall, reflection is noted with an increase in knowledge, changed attitudes, values, beliefs, and assumptions of individual participants and the potential for group reflective strategies to make a meaningful impact at the organizational level. | 9 |
| Ng, Kinsella, Friesen and Hodges [32] | Non-systematic search of the literature with view to capture dominant reflective applications and relate them to theoretical approaches | Level of education: undergraduate, graduate or postgraduate Learner profession: Medical Education Findings: Theoretical orientations of reflection are: reflection as epistemology of practice and reflection as critical social inquiry. Three prevalent trends in the application of reflection: utilitarian applications of reflection; focus on the self as the object of reflection, and reflection and assessment. Trends align with dominant epistemological positions in medicine (e.g., evidence based medicine), but not with those that underpin reflection. | 4 |
| Tsingos, Bosnic-Anticevich, Lonie and Smith [33,34] | Objective. To research the literature and examine assessment strategies used in health education that measure reflection levels and to identify assessment strategies for use in pharmacy education. A systematic review approach of studies from the last 20 years | Level of education: undergraduate, graduate, postgraduate Learner profession: medicine, nursing, allied healthcare professionals Findings: The literature search identified assessment strategies and rubrics used in health education for assessing levels of reflection. Reflective techniques used: reflective journal, portfolio, log, blog, questionnaire, video and diary. There is a significant gap in the literature regarding reflective rubric use in pharmacy education. | 9 |
| Van Roy, Vanheule and Inslegers [35] | Objective: Systematic review looking at Balint groups. Ninety-four articles included; 35 are empirical studies adopting a qualitative, quantitative or mixed methodology. | Level of education: undergraduate, graduate, postgraduate Learner profession: medicine, nursing, allied healthcare professionals Findings: The research topics that emerged include outcome, characteristics of Balint group participants, themes addressed in Balint groups, Balint group processes, and leadership and Balint group evaluations. | 9 |
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fragkos, K.C. Reflective Practice in Healthcare Education: An Umbrella Review. Educ. Sci. 2016, 6, 27. https://doi.org/10.3390/educsci6030027
Fragkos KC. Reflective Practice in Healthcare Education: An Umbrella Review. Education Sciences. 2016; 6(3):27. https://doi.org/10.3390/educsci6030027
Chicago/Turabian StyleFragkos, Konstantinos C. 2016. "Reflective Practice in Healthcare Education: An Umbrella Review" Education Sciences 6, no. 3: 27. https://doi.org/10.3390/educsci6030027
APA StyleFragkos, K. C. (2016). Reflective Practice in Healthcare Education: An Umbrella Review. Education Sciences, 6(3), 27. https://doi.org/10.3390/educsci6030027