

Extension of Interval-Valued Fermatean Fuzzy TOPSIS for Evaluating and Benchmarking COVID-19 Vaccines



Abstract
:1. Introduction
- Citizens live at elevated risk of health problems and higher mortality from COVID-19 and related comorbidities.
- There is a growing probability of the emergence of a black market for vaccines against COVID-19.
- Elderly and vulnerable people can easily fall victim to vaccine fraud.
- Vaccines shortages—require a solving budget, transportation, and logistics problems such as supply chain disruptions and delays caused by suppliers.
- Providing an informed choice of vaccine—raises the question of comparing available vaccines based on different indicators and objective decision-making.
- Vaccine hesitancy—specific concerns of some communities can be overcome through coordinated public information campaigns at the local and global levels.
- Delayed vaccination and lack of immunity—require more restrictions if the pandemic returns.
- (1)
- We analyze and summarize the existing multi-criteria approaches for COVID-19 vaccines selection. We classify them according to the included techniques and types of estimates (numeric, interval and linguistic values; crisp and fuzzy numbers) and divide them into three main categories by their complexity (number of multi-criteria techniques), flexibility (fuzziness character) and iteration (single or repeated data processing), respectively.
- (2)
- We design a theoretical framework for ranking COVID-19 vaccines based on single and hybrid methods with both crisp and fuzzy estimates. The former employ only one weight determination or ranking method, while the latter uses a combination of weight determination and ranking methods. We also apply several auxiliary techniques such as fuzzy interval arithmetic operations, robustness, and sensitivity analysis to improve the efficacy of decision analysis and approach benchmark rankings. To enhance the efficiency of the developed fuzzy Fermatean group TOPSIS method, we implement a recently proposed 3D distance metric to achieve a better multi-criteria comparison of vaccines’ features.
- (3)
- Finally, we construct static and dynamic rankings with real-world COVID-19 datasets based on single or repeated multi-criteria decision analysis. In the former case, we employ experts’ opinions as input for decision matrices. In the latter case, the ranking depends on measuring public attitudes towards vaccines. The dynamics detection may also be based on the user’s behavior and feelings, expressed in social media data. The comparative analysis of obtained results with other multi-criteria baselines shows the effectiveness as well as the necessity of proposed ideas.
2. Related Work
2.1. Literature Review on MCDM and Its Applications in COVID-19 Vaccine Evaluation
- (1)
- The majority of proposed multi-criteria solutions do not offer a holistic (multi-stage) solution but focus only on specific parts of the problem such as: (1) determining the relative importance of a few medical attributes in the criteria system [18] or (2) generating of vaccines ranking based on only one multi-criteria method [19,21].
- (2)
- (3)
2.2. Literature Review on Proposed Vaccines’ Evaluation Criteria
- (1)
- Vaccine Type
- Viral vector vaccines—these vaccines use a harmless virus version called “vector” to deliver to the body a gene of SARS-CoV-2. Cells employ it to produce a harmless fragment of the coronavirus, or so-called “spike” protein, found on the surface of SARS-CoV-2. Once the immune system recognizes this foreign protein, it creates antibodies and defensive white blood cells. If the body later becomes infected with the COVID-19 virus, the antibodies will fight it. The Jcovden COVID-19 vaccine (Janssen) is a vector vaccine. AstraZeneca and the University of Oxford have also developed a vector COVID-19 vaccine (Vaxzevria).
- Antigen vaccines—they use specific antigens to stimulate the immune system. Subunit antigen vaccines include only the parts of a virus that stimulate the immune system. This type of COVID-19 vaccine also contains harmless proteins. The immune system recognizes it as a foreign protein and thus activates the body’s natural defenses. Nuvaxovid (Novavax) is a protein subunit COVID-19 vaccine. The second group of antigen vaccines is those with the inactivated whole virus. They are produced using traditional vaccine technology and has established methods and a high level of safety. A theoretical advantage of inactivated vaccines is that they contain additional viral proteins, which could broaden protection beyond anti-spike protein responses and reduce the escape of variants from vaccine immunity. Valneva COVID-19 vaccine (VLA2001) is currently the only whole virus, inactivated vaccine candidate in clinical trials against COVID-19 in Europe.
- Nucleic acid vaccines—messenger RiboNucleic Acid (mRNA) teaches cells how to produce a protein (or part of a protein) that elicits an immune response. The technology for creating an mRNA vaccine has been developed for several decades. These vaccines do not contain live viruses and do not affect human DNA. mRNAs are the vaccines of Pfizer/Biontech and Moderna, Comirnaty, and Spikevax, respectively.
- (2)
- Number of doses and dose schedule
- (3)
- Storage Advantages
- (4)
- Efficacy
- (5)
- Side Effects
2.3. Literature Review on COVID-19 Vaccines
- Comirnaty (also known as Pfizer-BioNTech COVID-19 Vaccine) (BNT162b2), Pfizer, New York City, NY, USA, https://www.pfizer.com; BioNTech, Mainz, Germany (https://www.biontech.com, accessed on 7 July 2022)
- 2.
- Spikevax (previously COVID-19 Vaccine Moderna) (mRNA-1273), Moderna, Cambridge, MA, USA (https://www.modernatx.com, accessed on 7 July 2022)
- 3.
- Convidecia (Ad5-nCoV), CanSino Biologics, Tianjin, China, (https://www.cansinotech.com, accessed on 7 July 2022)
- 4.
- Sputnik V (Gam-COVID-Vac), Gamaleya Research Institute of Epidemiology and Microbiology, Moscow, Russia, (https://gamaleya.org/en, accessed on 7 July 2022)
- 5.
- EpiVacCorona (Aurora-CoV), Vektor State Research Center of Virology and Biotechnology, Koltsovo, Novosibirsk Oblast, Russia (http://www.vector.nsc.ru/, accessed on 7 July 2022)
- 6.
- BBIBP COVID-19 vaccine (BBIBP-CorV), Beijing Institute of Biological Products Co., Ltd., China National Pharmaceutical Group Corporation (CNPGC, Sinopharm), Beijing, China, (http://www.sinopharm.com, accessed on 7 July 2022)
- 7.
- WIBP COVID-19 vaccine (WIBP-CorV), China National Pharmaceutical Group Corporation (CNPGC, Sinopharm), Wuhan, China (http://www.sinopharm.com, accessed on 7 July 2022)
- 8.
- CoronaVac (PiCoVacc), Sinovac Biotech, Beijing, China, (www.sinovac.com, accessed on 7 July 2022)
- 9.
- Vaxzevria (previously COVID-19 Vaccine AstraZeneca) (AZD1222), University of Oxford, Oxford, UK; AstraZeneca Cambridge, UK (https://www.astrazeneca.com, accessed on 7 July 2022)
- 10.
- Nuvaxovid (NVX-CoV2373), Novavax, Gaithersburg, MD, USA (https://www.novavax.com/, accessed on 7 July 2022)
- 11.
- Jcovden (previously COVID-19 Vaccine Janssen), Janssen Pharmaceutical, Beerse, Belgium (https://www.janssen.com, accessed on 7 July 2022)
- 12.
- INO-4800, Inovio Pharmaceuticals, Plymouth Meeting, PA, USA, https://www.inovio.com, International Vaccine Institute, Seoul, South Korea (https://www.ivi.int/, accessed on 7 July 2022)
- 13.
- Covaxin (BBV152), Bharat Biotech, Turkapally, Hyderabad, India (https://www.bharatbiotech.com, accessed on 7 July 2022)
- 14.
- Covifenz (CoVLP+AS03), Medicago, Quebec, QC, Canada, https://medicago.com/en; GSK, London, UK (https://www.gsk.com, accessed on 7 July 2022)
- 15.
- Covishield (AZD1222), Serum Institute of India, Pune, Maharashtra, India (https://www.seruminstitute.com, accessed on 7 July 2022)
- Viral vector vaccines—Convidecia, Sputnik V, Vaxzevria, Jcovden, Covishield (5);
- Antigen vaccines: inactivated virus vaccines—BBIBP, Wuhan Sinopharm inactivated vaccine, CoronaVac, Covaxin (4); protein-based vaccines—EpiVacCorona, Nuvaxovid, Covifenz (3);
- mRNA/DNA vaccines—Comirnaty, Spikevax (2); Spike DNA-based—INO-4800 (1).
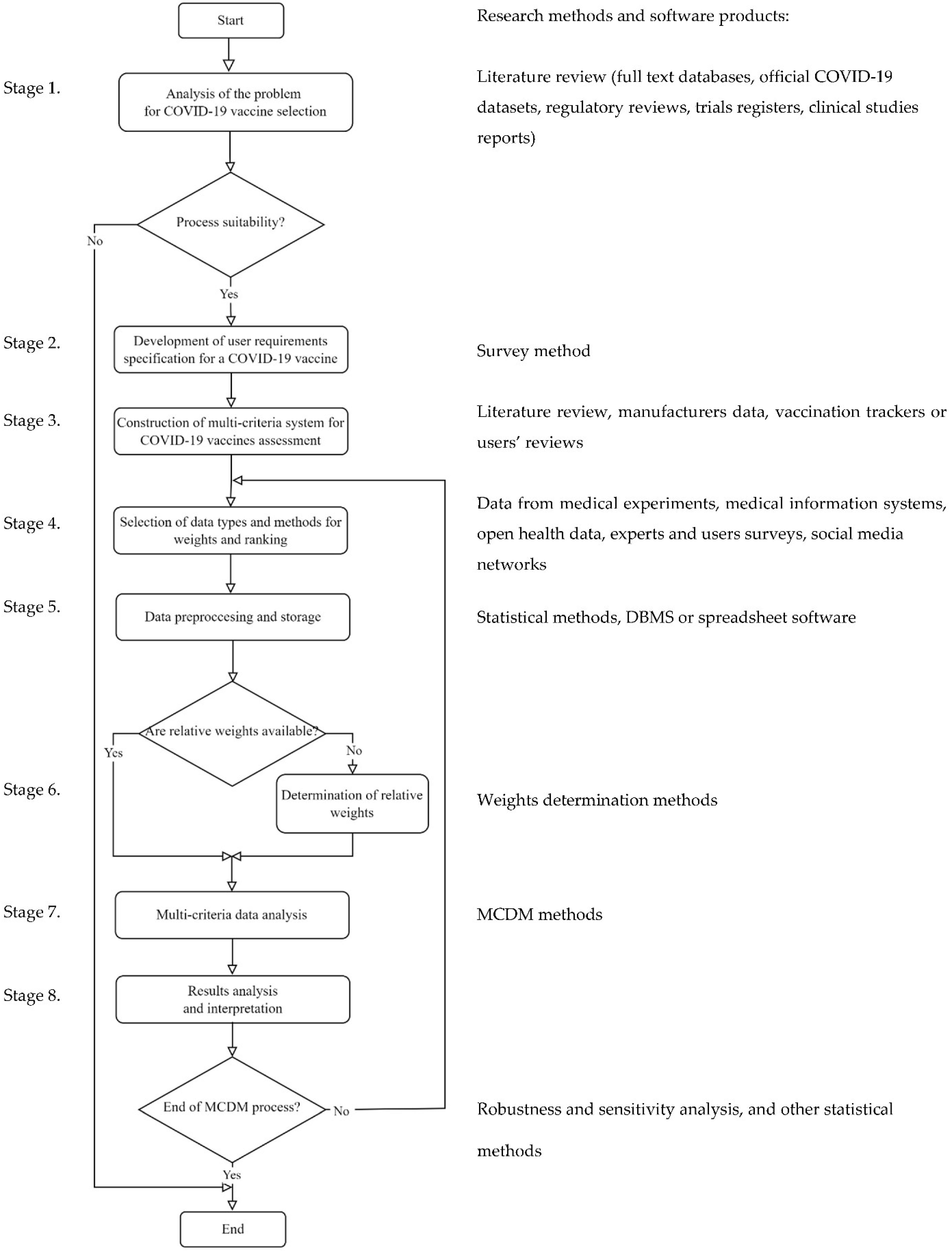
3. Methodological Framework for Vaccine Selection
3.1. Methodological Foundations of MCDM Methods
- They can be used in both modes—individual and group by decision-making experts.
- They can easily be combined in pairs consisting of the relative weight determination method and method for alternative ranking.
- They do not require large datasets and high-performance computing.
- The input data (the characteristics of alternatives and criteria weights) could be heterogeneous, evaluated with both crisp values and uncertain estimates—discrete or interval values, linguistic variables, fuzzy (symmetric or asymmetric; type-1 or type-2 fuzzy numbers; spherical, Fermatean, etc.), estimates.
3.2. Interval Value Fermatean Fuzzy Numbers—Some Basic Definitions and Operations
3.3. TOPSIS in IVFFNs Environment
| Algorithm 1. Pseudocode of IVFFNs TOPSIS. | ||
| Step 1: | Formulation of DM problem: | |
| identify | // is the set of given alternatives | |
| identify and | // is the set of identified criteria for A evaluation // is the set of relative weights of criteria | |
| // Empty decision matrix | ||
| Step 2: | Input of X | |
| Step 2.1: | Data transformation | |
| ; | ||
| for k in {1..K} | ||
| for i in {1..N} | ||
| for j in {1..M} | ||
| // Input of assessments of kth expert in matrix | ||
| // Transform X matrices in IVFFNs values | ||
| endfor | ||
| endfor | ||
| endfor | ||
| Step 2.2: | Data processing | |
| for i in {1..N} | ||
| for j in {1..M} | ||
| //Averaging for the group of experts according to Equation (10), where the experts have equal weight (1/K) | ||
| endfor | ||
| endfor | ||
| Step 2.3: | Data normalization | |
| for i in {1..N} | ||
| for j in {1..M} | ||
| //Normalizing each using its score function according to Equation (2) | ||
| endfor | ||
| endfor | ||
| Step 3: | Calculation of weighted value of assessments for each criterion | |
| for i in {1..N} | ||
| for j in {1..M} | ||
| //Weighting according to Equation (8) | ||
| endfor | ||
| endfor | ||
| Step 4: | Calculation of ideal and negative ideal solution for each criterion | |
| for i in {1..N} | ||
| for j in {1..M} | ||
| // Computation of the ideal and the negative ideal solution for beneficial and cost criteria ). | ||
| endfor | ||
| endfor | ||
| Step 5: | Calculation of Euclidean distances to the ideal and negative ideal solutions for each alternative | |
| for i in {1..N} | ||
| // Computation of Euclidean distances from each alternative to the ideal and negative ideal solutions. | ||
| Step 6: | for i in {1..N} | // Computation of the relative closeness of each alternative to the ideal solution |
| Step 7: | Output of alternatives’ ranks in descending order of their assessment | |
3.4. Theoretical Framework for COVID-19 Vaccine Selection
4. Practical Examples
4.1. A Case Study of Quality-Based Evaluation of COVID-19 Vaccines
- SAW: A5A10A3A4A6A7A11A8A14A9A1A2A12A15A13,
- TOPSIS: A5A10A3A4A6A7A11A8A14A9A1A2A12A15A13; ,
- WASPAS: A5A4A10A4A6A7A11A14A1A8A9A2A12A15A13, ,
- EDAS: A5A10A4A6A7A3A14A8A11A9A1A2A15A12A13,
- IVFFNs TOPSIS: A5A11A3A12A10A4A6A7A8A9A14A2A1A13A15, .
4.2. A Case Study of Dynamic Attitude-Based Evaluation of COVID-19 Vaccines
5. Conclusions, Limitations, and Future Work
- In addition to interval-valued membership and non-membership grades, the interval-valued hesitancy degree is also included.
- The length of belongingness, non-belongingness, and hesitancy intervals also participates in distance calculation.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Đukić, A.; Štaka, M.; Drašković, D. The Impact of the COVID-19 Pandemic on the Macroeconomic Aggregates of the European Union. Economics 2021, 9, 91–108. [Google Scholar] [CrossRef]
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 30 June 2022).
- Collins, F.S.; Stoffels, P. Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV): An unprecedented partnership for unprecedented times. JAMA 2020, 323, 2455–2457. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19): Herd Immunity, Lockdowns and COVID-19. 31 December 2020. Available online: https://www.who.int/news-room/questions-and-answers/item/herd-immunity-lockdowns-and-covid-19 (accessed on 11 June 2022).
- Marco-Franco, J.E.; Pita-Barros, P.; Vivas-Orts, D.; González-de-Julián, S.; Vivas-Consuelo, D. COVID-19, fake news, and vaccines: Should regulation be implemented? Int. J. Environ. Res. 2021, 18, 744. [Google Scholar] [CrossRef]
- Scrima, F.; Miceli, S.; Caci, B.; Cardaci, M. The relationship between fear of COVID-19 and intention to get vaccinated. The serial mediation roles of existential anxiety and conspiracy beliefs. Person. Individ. Differ. 2022, 184, 111188. [Google Scholar] [CrossRef]
- World Health Organization. Strategy to Achieve Global COVID-19 Vaccination by Mid-2022. Available online: https://cdn.who.int/media/docs/default-source/immunization/covid-19/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022.pdf (accessed on 30 June 2022).
- Council of the European Union. Available online: https://www.consilium.europa.eu/bg/policies/coronavirus/covid-19-research-and-vaccines (accessed on 30 June 2022).
- Our World in Data. Available online: https://ourworldindata.org/covid-vaccinations?country=OWID_WRL (accessed on 3 July 2022).
- Aruldoss, M.; Lakshmi, T.M.; Venkatesan, V.P. A survey on multi criteria decision making methods and its applications. Am. J. Inf. Syst. 2013, 1, 31–43. [Google Scholar]
- Ilieva, G.; Yankova, T. IoT System Selection as a Fuzzy Multi-Criteria Problem. Sensors 2022, 22, 4110. [Google Scholar] [CrossRef]
- Gavade, R.K. Multi-Criteria Decision Making: An overview of different selection problems and methods. Int. J. Comput. Sci. Inf. Technol. 2014, 5, 5643–5646. [Google Scholar]
- Senapati, T.; Yager, R.R. Fermatean fuzzy sets. J. Ambient Intell. Humaniz. Comput. 2020, 11, 663–674. [Google Scholar] [CrossRef]
- Gül, S. Fermatean fuzzy set extensions of SAW, ARAS, and VIKOR with applications in COVID-19 testing laboratory selection problem. Expert Syst. 2021, 38, e12769. [Google Scholar] [CrossRef] [PubMed]
- Kutlu Gündoğdu, F.; Kahraman, C. Spherical fuzzy sets and spherical fuzzy TOPSIS method. J. Intell. Fuzzy Syst. 2019, 36, 337–352. [Google Scholar] [CrossRef]
- Garg, H.; Sharaf, I.M. A new spherical aggregation function with the concept of spherical fuzzy difference for spherical fuzzy EDAS and its application to industrial robot selection. Comput. Appl. Math. 2022, 41, 212. [Google Scholar] [CrossRef]
- Lopez, D.; Gunasekaran, M. Assessment of vaccination strategies using fuzzy multi-criteria decision making. In Proceedings of the Fifth International Conference on Fuzzy and Neuro Computing (FANCCO-2015), Hyderabad, India, 17–19 December 2015. [Google Scholar]
- Öztaş, G.Z.; Bars, A.; Genç, V.; Erdem, S. Criteria Assessment for COVID-19 Vaccine Selection via BWM. In Proceedings of the International Workshop on Best-Worst Method, Delft, The Netherlands, 10–11 June 2021. [Google Scholar]
- Abdelwahab, S.F.; Issa, U.H.; Ashour, H.M. A Novel Vaccine Selection Decision-Making Model (VSDMM) for COVID-19. Vaccines 2021, 9, 718. [Google Scholar] [CrossRef]
- Ozsahin, D.U.; Gelisen, M.I.; Taiwo, M.; Agachan, Y.; Rahi, D.; Uzun, B. Decision analysis of the COVID-19 vaccines. Eurobiotech J. 2021, 5, 20–25. [Google Scholar] [CrossRef]
- Çetin, E.; Özen, H.; Özen, Ö. Primus inter pares: A Comparison and Ranking of COVID-19 Vaccines. Int. J. Anal. 2021, 1, 1–19. [Google Scholar]
- Öztürk, C.; Yildizbasi, A.; Yilmaz, I.; Ariöz, Y. Vaccine Selection Using Interval-Valued Intuitionistic Fuzzy VIKOR: A Case Study of COVID-19 Pandemic. In Proceedings of the International Conference on Intelligent and Fuzzy Systems (INFUS 2021), Istanbul, Turkey, 24–26 August 2021. [Google Scholar]
- Forestal, R.L.; Pi, S.M. A hybrid approach based on ELECTRE III-genetic algorithm and TOPSIS method for selection of optimal COVID-19 vaccines. J. Multi-Criteria Decis. Anal. 2022, 29, 80–91. [Google Scholar] [CrossRef]
- Ecer, F. An extended MAIRCA method using intuitionistic fuzzy sets for coronavirus vaccine selection in the age of COVID-19. Neural Comput. Appl. 2022, 34, 5603–5623. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2021, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Al Kaabi, N.; Oulhaj, A.; Ganesan, S.; Al Hosani, F.I.; Najim, O.; Ibrahim, H.; Acuna, J.; Alsuwaidi, A.R.; Kamour, A.M.; Alzaabi, A.; et al. Effectiveness of BBIBP-CorV vaccine against severe outcomes of COVID-19 in Abu Dhabi, United Arab Emirates. Nat. Commun. 2022, 13, 3215. [Google Scholar] [CrossRef] [PubMed]
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 inactivated SARS-CoV-2 vaccines on symptomatic COVID-19 infection in adults: A randomized clinical trial. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef]
- Dunkle, L.M.; Kotloff, K.L.; Gay, C.L.; Áñez, G.; Adelglass, J.M.; Barrat Hernández, A.Q.; Harper, W.L.; Duncanson, D.M.; McArthur, M.A.; Florescu, D.F.; et al. Efficacy and safety of NVX-CoV2373 in adults in the United States and Mexico. N. Engl. J. Med. 2022, 386, 531–543. [Google Scholar] [CrossRef]
- Lin, D.Y.; Gu, Y.; Wheeler, B.; Young, H.; Holloway, S.; Sunny, S.K.; Moore, Z.; Zeng, D. Effectiveness of COVID-19 vaccines over a 9-month period in North Carolina. N. Engl. J. Med. 2022, 386, 933–941. [Google Scholar] [CrossRef]
- Tebas, P.; Agnes, J.; Giffear, M.; Kraynyak, K.A.; Blackwood, E.; Amante, D.; Reuschel, E.; Liu, N.; Purwar, M.; Christensen-Quick, A.; et al. Safety and Immunogenicity of INO-4800, a COVID-19 DNA Vaccine as a Primary Series and Booster. Open Forum Infect. Dis. 2021, 8, S387–S388. [Google Scholar] [CrossRef]
- Keshavarz-Ghorabaee, M.; Amiri, M.; Zavadskas, E.K.; Turskis, Z.; Antucheviciene, J. Determination of objective weights using a new method based on the removal effects of criteria (MEREC). Symmetry 2021, 13, 525. [Google Scholar] [CrossRef]
- Hwang, C.L.; Yoon, K. Methods for multiple attribute decision making. In Multiple Attribute Decision Making; Springer: Berlin/Heidelberg, Germany, 1981; pp. 58–191. [Google Scholar]
- Zavadskas, E.K.; Turskis, Z. A new additive ratio assessment (ARAS) method in multicriteria decision-making. Technol. Econ. Dev. Econ. 2010, 16, 159–172. [Google Scholar] [CrossRef]
- Chakraborty, S.; Zavadskas, E.K. Applications of WASPAS Method in Manufacturing Decision Making. Informatica 2014, 25, 1–20. [Google Scholar] [CrossRef]
- Keshavarz Ghorabaee, M.K.; Zavadskas, E.K.; Olftat, L.; Turslis, Z. Multi-criteria inventory classification using a new method of evaluation based on distance from average solution (EDAS). Informatica 2015, 26, 435–451. [Google Scholar] [CrossRef]
- Pamučar, D.; Ćirović, G. The selection of transport and handling resources in logistics centers using Multi-Attribute Border Approximation area Comparison (MABAC). Expert Syst. Appl. 2015, 42, 3016–3028. [Google Scholar] [CrossRef]
- Gigović, L.; Pamučar, D.; Bajić, Z.; Milićević, M. The Combination of Expert Judgment and GIS-MAIRCA Analysis for the Selection of Sites for Ammunition Depots. Sustainability 2016, 8, 372. [Google Scholar] [CrossRef]
- Keshavarz Ghorabaee, M.; Zavadskas, E.K.; Turskis, Z.; Antucheviciene, J. A New Combinative Distance-based Assessment (CODAS) Method for Multi-Criteria Decision-Making. Econ. Comput. Econ. Cybern. Stud. Res. 2016, 50, 25–44. [Google Scholar]
- Stević, Ž.; Pamučar, D.; Puška, A.; Chatterjee, P. Sustainable supplier selection in healthcare industries using a new MCDM method: Measurement of alternatives and ranking according to compromise solution (MARCOS). Comput. Ind. Eng. 2020, 140, 106231. [Google Scholar] [CrossRef]
- Rani, P.; Mishra, A.R. Interval-valued Fermatean fuzzy sets with multi-criteria weighted aggregated sum product assessment-based decision analysis framework. Neural Comput. Appl. 2022, 34, 8051–8067. [Google Scholar] [CrossRef]
- Jeevaraj, S. Ordering of interval-valued Fermatean fuzzy sets and its applications. Expert Syst. Appl. 2021, 185, 115613. [Google Scholar]


{kind=link}
| N | Brand Name | Company | Vaccine Type | Vaccine Storage | Dosing Schedule | Efficacy |
|---|---|---|---|---|---|---|
| 1 | Comirnaty (also known as Pfizer-BioNTech) | Pfizer-BioNTech | Messenger RNA (mRNA) | Frozen between −90 °C to −60 °C for up to 9 months. | Two doses, 21 days apart | 95% |
| 2 | Spikevax (previously Moderna) | Moderna | mRNA | Frozen between −25 °C to −15 °C for up to 9 months. | Two doses, 28 days apart | 94.1% |
| 3 | Convidecia | CanSino Biologics | Viral vector | Refrigerated between 2 °C to 8 °C for up to 12 months. | Single dose | 63.7% |
| 4 | Sputnik V | Gamaleya Research Institute of Epidemiology and Microbiology | Adenoviral based | Frozen at −18 °C or less. The shelf life is 3 months from the date of production. | Two doses, 21 days apart | 85.7% |
| 5 | EpiVacCorona | Vektor State Research Center of Virology and Biotechnology | Antigens-based | Refrigerated between 2 °C to 8 °C. | Two doses, 14 days apart | 100% |
| 6 | BBIBP-CorV | Sinopharm | Whole inactivated virus | Refrigerated between 2 °C to 8 °C for up to 24 months. | Two doses, 21 days apart | 79.6% |
| 7 | WIBP-CorV | Sinopharm | Inactivated virus | Refrigerated between 2 °C to 8 °C for up to 6 months. | Two doses, 21 days apart | 72.8% |
| 8 | CoronaVac | Sinovac | Whole inactivated virus | Refrigerated between 2 °C to 8 °C for up to 12 months. | 2 doses, 14 days apart | 83.5% |
| 9 | Vaxzevria (previously AstraZeneca) | Oxford-AstraZeneca | Carrier vaccine | Refrigerated between 2 °C to 8 °C for up to 6 months. | Two doses, four to 12 weeks apart | 79% |
| 10 | Nuvaxovid | Novavax | Protein adjuvant | Refrigerated between 2 °C to 8 °C for up to 9 months. | Two doses, 21 days apart | 92.6% |
| 11 | Jcovden (previously Janssen) | Janssen, Johnson & Johnson | Carrier vaccine | Frozen between −25 ° to −15 °C for up to 24 months. | Single dose | 74.8% |
| 12 | INO-4800 | Inovio Pharmaceuticals | DNA-based | Five-year projected shelf life and does not need to be frozen during transport or storage. | Two doses, 28 days apart | 95% |
| 13 | Covaxin | Bharat Biotech | Whole inactivated virus-based | Refrigerated between 2 °C to 8 °C for up to 9 months. | Two doses, 28 days apart | 78% |
| 14 | Covifenz | Medicago | Virus-like particles of SARS-CoV-2 spike protein | Refrigerated between 2 °C to 8 °C. | Two doses, 21 days apart | 95% |
| 15 | Covishield | Serum Institute of India | Adenovirus-based | Refrigerated between 2 °C to 8 °C for up to 6 months. | Two doses, 4 to 12 weeks apart | 62% |
| Criteria Alternative | C1 | C2 | C3 | C4 | C5 |
|---|---|---|---|---|---|
| A1 | VH | VL | VL | VH | VH |
| A2 | VH | M | VL | VH | M |
| A3 | VL | M | VH | VL | M |
| A4 | VH | VL | VL | VH | VL |
| A5 | VH | M | VH | VH | VL |
| A6 | VH | VL | VH | M | H |
| A7 | VH | VL | VH | M | H |
| A8 | VH | M | VH | M | M |
| A9 | VH | M | VH | M | H |
| A10 | VH | VL | VH | H | M |
| A11 | VL | VH | VH | L | M |
| A12 | VH | M | VL | VH | H |
| A13 | VH | M | VL | L | H |
| A14 | VH | VL | VL | VH | M |
| A15 | VH | VL | VL | VL | M |
| Criterion type |
| Linguistic Term | IVFFN |
|---|---|
| Very Low (VL) | ([0, 0.2], [0.8, 0.95]) |
| Low (L) | ([0.3, 0.4], [0.6, 0.7]) |
| Medium (M) | ([0.45, 0.55], [0.4, 0.55]) |
| High (H) | ([0.6, 0.7], [0.2, 0.3]) |
| Very High (VH) | ([0.8, 0.95], [0, 0.15]) |
| A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 | A11 | A12 | A13 | A14 | A15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IVFFNSs | Score | 0.33 | 0.39 | 0.61 | 0.54 | 0.73 | 0.51 | 0.51 | 0.50 | 0.47 | 0.57 | 0.64 | 0.58 | 0.22 | 0.43 | 0.21 |
| Rank | 13 | 12 | 3 | 6 | 1 | 7 | 8 | 9 | 10 | 5 | 2 | 4 | 14 | 11 | 15 | |
| CrispNs | Score | 0.45 | 0.44 | 0.56 | 0.55 | 0.62 | 0.53 | 0.53 | 0.50 | 0.47 | 0.59 | 0.53 | 0.41 | 0.25 | 0.50 | 0.38 |
| Rank | 11 | 12 | 3 | 4 | 1 | 5 | 6 | 8 | 10 | 2 | 7 | 13 | 15 | 9 | 14 | |
| SAW | WASPAS | EDAS | ||||
|---|---|---|---|---|---|---|
| Alternative | Score | Rank | Score | Rank | Score | Rank |
| A1 | 1.87 | 11 | 1.30 | 9 | 0.42 | 11 |
| A2 | 1.86 | 12 | 1.04 | 12 | 0.33 | 12 |
| A3 | 3.11 | 3 | 1.44 | 7 | 0.62 | 6 |
| A4 | 2.87 | 4 | 1.72 | 2 | 0.77 | 3 |
| A5 | 3.50 | 1 | 1.80 | 1 | 0.87 | 1 |
| A6 | 2.70 | 6 | 1.54 | 4 | 0.69 | 4 |
| A7 | 2.70 | 7 | 1.54 | 5 | 0.69 | 5 |
| A8 | 2.57 | 8 | 1.24 | 10 | 0.52 | 8 |
| A9 | 2.28 | 10 | 1.20 | 11 | 0.44 | 10 |
| A10 | 3.22 | 2 | 1.69 | 3 | 0.86 | 2 |
| A11 | 2.76 | 5 | 1.48 | 6 | 0.45 | 9 |
| A12 | 1.62 | 13 | 0.99 | 13 | 0.24 | 14 |
| A13 | 1.25 | 15 | 0.69 | 15 | 0.00 | 15 |
| A14 | 2.37 | 9 | 1.37 | 8 | 0.59 | 7 |
| A15 | 1.50 | 14 | 0.97 | 14 | 0.26 | 13 |
| Spearman’s | 0.94 | 0.96 | ||||
| Date | First Day | Last Day | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alternative Emotion | A1 | A2 | A3 | A4 | A5 | A6 | A1 | A2 | A3 | A4 | A5 | A6 |
| Joy | 0.652 | 0.678 | 0.779 | 0.795 | 0.679 | 0.859 | 0.796 | 0.794 | 0.746 | 0.900 | 0.800 | 0.758 |
| Anger | 0.002 | 0.008 | 0.000 | 0.000 | 0.004 | 0.000 | 0.000 | 0.004 | 0.000 | 0.002 | 0.000 | 0.000 |
| Disgust | 0.014 | 0.002 | 0.002 | 0.005 | 0.002 | 0.004 | 0.000 | 0.000 | 0.000 | 0.000 | 0.004 | 0.002 |
| Fear | 0.072 | 0.098 | 0.160 | 0.073 | 0.125 | 0.025 | 0.056 | 0.064 | 0.234 | 0.042 | 0.082 | 0.052 |
| Sadness | 0.042 | 0.032 | 0.002 | 0.025 | 0.006 | 0.007 | 0.006 | 0.024 | 0.000 | 0.008 | 0.018 | 0.024 |
| Surprise | 0.218 | 0.182 | 0.056 | 0.101 | 0.183 | 0.106 | 0.142 | 0.114 | 0.020 | 0.048 | 0.096 | 0.164 |
| BG | 0.652 | 0.678 | 0.779 | 0.795 | 0.679 | 0.859 | 0.796 | 0.794 | 0.746 | 0.900 | 0.800 | 0.758 |
| NG | 0.130 | 0.140 | 0.165 | 0.104 | 0.137 | 0.035 | 0.062 | 0.092 | 0.234 | 0.052 | 0.104 | 0.078 |
| Alternative | Score | Rank | ||||
|---|---|---|---|---|---|---|
| A1 | 0.652 | 0.796 | 0.062 | 0.130 | 0.390 | 6 |
| A2 | 0.678 | 0.794 | 0.092 | 0.140 | 0.404 | 5 |
| A3 | 0.779 | 0.746 | 0.165 | 0.234 | 0.436 | 3 |
| A4 | 0.795 | 0.900 | 0.104 | 0.052 | 0.616 | 1 |
| A5 | 0.679 | 0.800 | 0.104 | 0.137 | 0.411 | 4 |
| A6 | 0.859 | 0.758 | 0.035 | 0.078 | 0.534 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilieva, G.; Yankova, T. Extension of Interval-Valued Fermatean Fuzzy TOPSIS for Evaluating and Benchmarking COVID-19 Vaccines. Mathematics 2022, 10, 3514. https://doi.org/10.3390/math10193514
Ilieva G, Yankova T. Extension of Interval-Valued Fermatean Fuzzy TOPSIS for Evaluating and Benchmarking COVID-19 Vaccines. Mathematics. 2022; 10(19):3514. https://doi.org/10.3390/math10193514
Chicago/Turabian StyleIlieva, Galina, and Tania Yankova. 2022. "Extension of Interval-Valued Fermatean Fuzzy TOPSIS for Evaluating and Benchmarking COVID-19 Vaccines" Mathematics 10, no. 19: 3514. https://doi.org/10.3390/math10193514
APA StyleIlieva, G., & Yankova, T. (2022). Extension of Interval-Valued Fermatean Fuzzy TOPSIS for Evaluating and Benchmarking COVID-19 Vaccines. Mathematics, 10(19), 3514. https://doi.org/10.3390/math10193514