



Deep Learning-Based Classification of Abrasion and Ischemic Diabetic Foot Sores Using Camera-Captured Images

 ,
,  ,
, 
Abstract
:1. Introduction
- We present a novel deep learning-based model, in which features are extracted using Vgg-19 and then given to six layers of CNN to produce a final classification system. Furthermore, we also compared the proposed model with state-of-the-art (SOTA) models.
- The quality of AFS and ischemic DFS images were increased using noise reduction and data pre-processing algorithms, which eliminated artefacts and noise from images. After evaluating our dataset, we selected preparation methods and parameter configurations that yielded the best results.
- Statistical evaluations using ANOVA and Friedman tests were performed on the proposed method to validate its efficiency.
- Image segmentation was performed using UNet++.
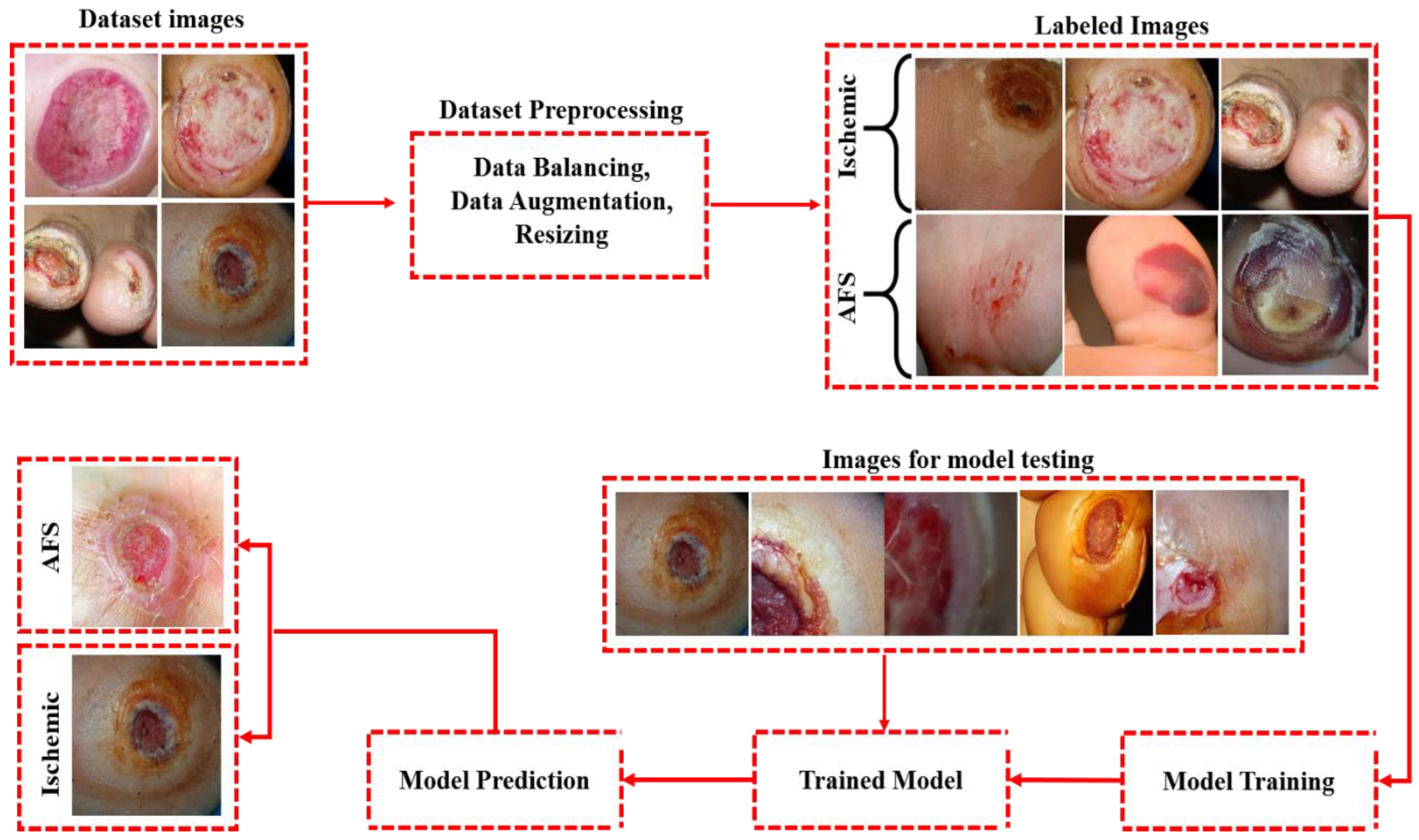
- AFS and ischemic DFS images were used to train and evaluate the proposed model. Images of these two diseases were collected from publicly available databases to researchers [30,31]. Both datasets have a combined total of 2826 camera-captured images, in which 1413 images belonged to AFS and 1413 images belonged to ischemia DFS. A data augmentation technique was applied to enhance the number of images in the datasets, improving its classification performance. A total of 8478 images were used in the proposed model, with 70% representing the training set, 20% representing the validation set, and 10% representing the testing set.
- The proposed model accomplished the following results: an accuracy score of 99.05%, a precision score of 98.99%, a recall score of 99.01%, an MCC score of 0.9801, and an f1 score of 99.04%.
- The CNN-based pre-trained models, namely Inception-v3 and MobileNet, were fine-tuned and re-trained on the same datasets for the classification of foot ulcers. The results of these models were then compared with the results of the proposed model in terms of performance evaluation metrics. In the classification, the performance of the proposed model was found to be superior to that of the two pre-trained techniques.
- We conducted an in-depth analysis of the most recent research on CNN-based classifiers in addition to the conventional machine learning approaches used for classifying AFS and ischemia DFS.
2. Literature Review
3. Materials and Methods
3.1. Dataset Description
3.2. Data Augmentation and Preprocessing
3.3. Image Segmentation Using UNet++
3.4. Proposed Methodology
3.4.1. Vgg-19
3.4.2. Input Layer
3.4.3. Convolutional Layer
3.4.4. ReLU
3.4.5. Global Average Pooling
3.4.6. Dropout
3.4.7. FCL
3.4.8. Sigmoid Layer
3.5. Performance Evaluation Metrics
3.6. Statistical Analysis
4. Results and Discussion
4.1. Experimental Setup
4.2. Result Analysis
4.3. Comparison with Other SOTA Models
4.4. Discussion
5. Limitation of the Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naeem, A.; Farooq, M.S.; Khelifi, A.; Abid, A. Malignant melanoma classification using deep learning: Datasets, performance measurements, challenges and opportunities. IEEE Access 2020, 8, 110575–110597. [Google Scholar] [CrossRef]
- Li, Y.; Wei, X. Pantograph slide plate abrasion detection based on deep learning network. In Proceedings of the International Conference on Electrical and Information Technologies for Rail Transportation, Changsha, China, 20–22 October 2017; Springer: Singapore, 2018; pp. 215–224. [Google Scholar]
- Goyal, M.; Reeves, N.D.; Rajbhandari, S.; Ahmad, N.; Wang, C.; Yap, M.H. Recognition of ischaemia and infection in diabetic foot ulcers: Dataset and techniques. Comput. Biol. Med. 2020, 117, 103616. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, W.G.; Dos Santos, M.H.D.P.; Lobato, F.M.F.; Ribeiro-dos-Santos, Â.; de Araújo, G.S. Deep learning in gastric tissue diseases: A systematic review. BMJ Open Gastroenterol. 2020, 7, e000371. [Google Scholar] [CrossRef]
- Maghanoy, J.A.W.; Guzman, D.G.; Paz, J.S.D.; Policarpio, D.R.; Yanga, A.D.; Ambat, S. E-Aid: Open Wound Identifier and Analyzer Using Smartphone Through Captured Image. In ICT Analysis and Applications; Springer: Singapore, 2022; pp. 691–697. [Google Scholar]
- Malik, H.; Farooq, M.S.; Khelifi, A.; Abid, A.; Qureshi, J.N.; Hussain, M. A Comparison of Transfer Learning Performance Versus Health Experts in Disease Diagnosis from Medical Imaging. IEEE Access 2020, 8, 139367–139386. [Google Scholar] [CrossRef]
- Lefrancois, T.; Mehta, K.; Sullivan, V.; Lin, S.; Glazebrook, M. Evidence based review of literature on detriments to healing of diabetic foot ulcers. Foot Ankle Surg. 2017, 23, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Idf.org. Diabetic Foot Ulcer. Available online: https://idf.org/our-activities/care-prevention/diabetic-foot.html (accessed on 30 June 2023).
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.; Attinger, C.; Abbas, Z.; Bal, A.; Rojas, N.; Xu, Z.R. Cost of treating diabetic foot ulcers in five different countries. Diabetes/Metab. Res. Rev. 2012, 28, 107–111. [Google Scholar] [CrossRef]
- Fathimaa, M.R.; Rekha, A. CT Scan of the Foot in Patients with Chronic Non-Healing Diabetic Foot Ulcer. Case Rep. Clin. Med. 2020, 9, 335. [Google Scholar] [CrossRef]
- Eren, M.A.; Karakaş, E.; Torun, A.N.; Sabuncu, T. The Clinical Value of Diffusion-Weighted Magnetic Resonance Imaging in Diabetic Foot Infection. J. Am. Podiatr. Med. Assoc. 2019, 109, 277–281. [Google Scholar] [CrossRef]
- Goyal, M.; Reeves, N.D.; Davison, A.K.; Rajbhandari, S.; Spragg, J.; Yap, M.H. Dfunet: Convolutional neural networks for diabetic foot ulcer classification. IEEE Trans. Emerg. Top. Comput. Intell. 2018, 4, 728–739. [Google Scholar] [CrossRef]
- Goyal, M.; Reeves, N.D.; Rajbhandari, S.; Yap, M.H. Robust methods for real-time diabetic foot ulcer detection and localization on mobile devices. IEEE J. Biomed. Health Inform. 2018, 23, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed]
- Rastgarpour, M.; Shanbehzadeh, J. Application of AI techniques in medical image segmentation and novel categorization of available methods and tools. In Proceedings of the IMECS 2011—International Multi Conference of Engineers and Computer Scientists, Hong Kong, 16–18 March 2011; Volume 1, pp. 519–523. [Google Scholar]
- Yap, M.H.; Hachiuma, R.; Alavi, A.; Brüngel, R.; Cassidy, B.; Goyal, M.; Zhu, H.; Ruckert, J.; Olshansky, M.; Huang, X.; et al. Deep learning in diabetic foot ulcers detection: A comprehensive evaluation. Comput. Biol. Med. 2021, 135, 104596. [Google Scholar] [CrossRef] [PubMed]
- Naeem, A.; Anees, T.; Naqvi, R.A.; Loh, W.K. A Comprehensive Analysis of Recent Deep and Federated-Learning-Based Methodologies for Brain Tumor Diagnosis. J. Pers. Med. 2022, 12, 275. [Google Scholar] [CrossRef]
- Saeed, H.; Malik, H.; Bashir, U.; Ahmad, A.; Riaz, S.; Ilyas, M.; Zhu, H.; Ruckert, J.; Olshanksy, M.; Huang, X.; et al. Blockchain technology in healthcare: A systematic review. PLoS ONE 2022, 17, e0266462. [Google Scholar] [CrossRef]
- Cireşan, D.C.; Giusti, A.; Gambardella, L.M.; Schmidhuber, J. Mitosis detection in breast cancer histology images with deep neural networks. Lect. Notes Comput. Sci. 2013, 8150, 411–418. [Google Scholar] [CrossRef]
- Mohsen, H.; El-Dahshan, E.-S.A.; El-Horbaty, E.-S.M.; Salem, A.-B.M. Classification using deep learning neural networks for brain tumors. Futur. Comput. Inform. J. 2018, 3, 68–71. [Google Scholar] [CrossRef]
- Naeem, A.; Anees, T.; Fiza, M.; Naqvi, R.A.; Lee, S.W. SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images. Sensors 2022, 22, 5652. [Google Scholar] [CrossRef]
- Quang, D.; Xie, X. DanQ: A hybrid convolutional and recurrent deep neural network for quantifying the function of DNA sequences. Nucleic Acids Res. 2016, 44, e107. [Google Scholar] [CrossRef]
- Gururajarao, S.B.; Venkatappa, U.; Shivaram, J.M.; Sikkandar, M.Y.; Al Amoudi, A. Infrared thermography and soft computing for diabetic foot assessment. In Machine Learning in Bio-Signal Analysis and Diagnostic Imaging; Academic Press: Cambridge, MA, USA, 2019; pp. 73–97. [Google Scholar]
- Guo, S.; Liu, X.; Zhang, H.; Lin, Q.; Xu, L.; Shi, C.; Gao, Z.; Guzzo, A.; Fortino, G. Causal knowledge fusion for 3D cross-modality cardiac image segmentation. Inf. Fusion 2023, 99, 101864. [Google Scholar] [CrossRef]
- Chen, Y.; Han, G.; Lin, T.; Liu, X. CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation. Sensors 2022, 22, 5053. [Google Scholar] [CrossRef]
- Zhi, Y.; Hau, W.K.; Zhang, H.; Gao, Z. Vessel Contour Detection in Intracoronary Images via Bilateral Cross-Domain Adaptation. IEEE J. Biomed. Health Inform. 2023, 27, 3314–3325. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, S.; Li, F.; Raj, A.N.J.; Ding, W.; Zhou, W.; Zhuang, Z. Automatic segmentation for ultrasound image of carotid intimal-media based on improved superpixel generation algorithm and fractal theory. Comput. Methods Programs Biomed. 2021, 205, 106084. [Google Scholar] [CrossRef] [PubMed]
- Vilcahuaman, L.; Harba, R.; Canals, R.; Zequera, M.; Wilches, C.; Arista, M.T.; Torres, L.; Arbañil, H. Automatic analysis of plantar foot thermal images in at-risk type II diabetes by using an infrared camera. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Toronto, ON, Canada, 7–12 June 2015; Springer: Cham, Switzerland, 2015; pp. 228–231. [Google Scholar]
- Alzubaidi, L.; Fadhel, M.A.; Oleiwi, S.R.; Al-Shamma, O.; Zhang, J. DFU_QUTNet: Diabetic foot ulcer classification using novel deep convolutional neural network. Multimed. Tools Appl. 2020, 79, 15655–15677. [Google Scholar] [CrossRef]
- Ulcer Classification Dataset. Kaggle. 2021. Available online: https://www.kaggle.com/shlokmohanty/ulcer-classification (accessed on 30 June 2023).
- Al-Garaawi, N.; Ebsim, R.; Alharan, A.F.; Yap, M.H. Diabetic foot ulcer classification using mapped binary patterns and convolutional neural networks. Comput. Biol. Med. 2022, 140, 105055. [Google Scholar] [CrossRef]
- Das, S.K.; Roy, P.; Mishra, A.K. DFU_SPNet: A stacked parallel convolution layers based CNN to improve Diabetic Foot Ulcer classification. ICT Express 2021, 8, 271–275. [Google Scholar] [CrossRef]
- Thotad, P.N.; Bharamagoudar, G.R.; Anami, B.S. Diabetic foot ulcer detection using deep learning approaches. Sens. Int. 2023, 4, 100210. [Google Scholar] [CrossRef]
- Stefanopoulos, S.; Ayoub, S.; Qiu, Q.; Ren, G.; Osman, M.; Nazzal, M.; Ahmed, A. Machine learning prediction of diabetic foot ulcers in the inpatient population. Vascular 2021, 30, 17085381211040984. [Google Scholar] [CrossRef]
- Costa Oliveira, A.L.; de Carvalho, A.B.; Dantas, D.O. Faster R-CNN Approach for Diabetic Foot Ulcer Detection. In VISIGRAPP; Federal University of Sergipe: São Cristóvão, Brazil, 2021; Volume 4, pp. 677–684. [Google Scholar]
- Wang, C.; Yan, X.; Smith, M.; Kochhar, K.; Rubin, M.; Warren, S.M.; Wrobel, J.; Lee, H. A unified framework for automatic wound segmentation and analysis with deep convolutional neural networks. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 2415–2418. [Google Scholar]
- Cui, C.; Thurnhofer-Hemsi, K.; Soroushmehr, R.; Mishra, A.; Gryak, J.; Domínguez, E.; Najarian, K.; López-Rubio, E. Diabetic wound segmentation using convolutional neural networks. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1002–1005. [Google Scholar]
- Botros, F.S.; Taher, M.F.; ElSayed, N.M.; Fahmy, A.S. Prediction of diabetic foot ulceration using spatial and temporal dynamic plantar pressure. In Proceedings of the 2016 8th Cairo International Biomedical Engineering Conference (CIBEC), Cairo, Egypt, 15–17 December 2016; pp. 43–47. [Google Scholar]
- Keerthika, A.; Sangeetha, G.; JayaBharathi, C.; Pavithra, S. Prediction of Diabetic Foot Ulcer based on Region growth segmentation. Int. J. Pure Appl. Math. 2018, 119, 643–651. [Google Scholar]
- Pushpaleela, R.C.; Padmajavalli, R. Prediction of Type-2 Diabetes Foot Ulcer-A Comparative Study with Classification Algorithm. Int. J. Pure Appl. Math. 2017, 117, 219–230. [Google Scholar]
- Veredas, F.; Mesa, H.; Morente, L. Binary tissue classification on wound images with neural networks and bayesian classifiers. IEEE Trans. Med. Imaging 2009, 29, 410–427. [Google Scholar] [PubMed]
- Sudarvizhi, M.D.; Nivetha, M.; Priyadharshini, P.; Swetha, J.R. Identification and analysis of foot ulceration using load cell technique. IRJET 2019, 6, 7792–7797. [Google Scholar]
- Patel, S.; Patel, R.; Desai, D. Diabetic foot ulcer wound tissue detection and classification. In Proceedings of the 2017 International Conference on Innovations in Information, Embedded and Communication Systems (ICIIECS), Coimbatore, India, 17–18 March 2017; pp. 1–5. [Google Scholar]
- Liu, Z.; John, J.; Agu, E. Diabetic Foot Ulcer Ischemia and Infection Classification Using EfficientNet Deep Learning Models. IEEE Open J. Eng. Med. Biol. 2022, 3, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.; Ng, E.Y.; Oh, S.L.; Heng, M.L.; Hagiwara, Y.; Tan, J.H.; Tong, J.W.; Acharya, U.R. Automated detection of diabetic foot with and without neuropathy using double density-dual tree-complex wavelet transform on foot thermograms. Infrared Phys. Technol. 2018, 92, 270–279. [Google Scholar]
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data 2019, 6, 1–48. [Google Scholar]
- Ho, D.; Liang, E.; Liaw, R. 1000x Faster Data Augmentation, Berkeley Artificial Intelligence Research; University of California Berkley: Berkley, CA, USA, 2019. [Google Scholar]
- Zhou, Z.; Rahman Siddiquee, M.M.; Tajbakhsh, N.; Liang, J. Unet++: A nested u-net architecture for medical image segmentation. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support: 4th International Workshop, DLMIA 2018, and 8th International Workshop, ML-CDS 2018, Held in Conjunction with MICCAI 2018, Granada, Spain, 20 September 2018; Springer International Publishing: Cham, Switzerland, 2018; pp. 3–11. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2016; pp. 770–778. [Google Scholar]
- Naeem, A.; Anees, T.; Ahmed, K.T.; Naqvi, R.A.; Ahmad, S.; Whangbo, T. Deep learned vectors’ formation using auto-correlation, scaling, and derivations with CNN for complex and huge image retrieval. Complex Intell. Syst. 2022, 9, 1729–1751. [Google Scholar] [CrossRef]
- Mane, D.T.; Kulkarni, U.V. A survey on supervised convolutional neural network and its major applications. In Deep Learning and Neural Networks: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2020; pp. 1058–1071. [Google Scholar]
- Malik, H.; Anees, T.; Din, M.; Naeem, A. CDC_Net: Multi-classification convolutional neural network model for detection of COVID-19, pneumothorax, pneumonia, lung Cancer, and tuberculosis using chest X-rays. Multimed. Tools Appl. 2022, 82, 13855–13880. [Google Scholar] [CrossRef]
- Reshi, A.A.; Rustam, F.; Mehmood, A.; Alhossan, A.; Alrabiah, Z.; Ahmad, A.; Alsuwailem, H.; Choi, G.S. An Efficient CNN Model for COVID-19 Disease Detection Based on X-Ray Image Classification. Complexity 2021, 2021, 6621607. [Google Scholar] [CrossRef]
- Ibrahim, D.M.; Elshennawy, N.M.; Sarhan, A.M. Deep-chest: Multi-classification deep learning model for diagnosing COVID-19, pneumonia, and lung cancer chest diseases. Comput. Biol. Med. 2021, 132, 104348. [Google Scholar] [CrossRef]
- Manski, C.F. Bounding the Predictive Values of COVID-19 Antibody Tests; Technical Report No. w27226; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Malik, H.; Anees, T. BDCNet: Multi-classification convolutional neural network model for classification of COVID-19, pneumonia, and lung cancer from chest radiographs. Multimed. Syst. 2022, 28, 815–829. [Google Scholar] [CrossRef] [PubMed]
- Ruuska, S.; Hämäläinen, W.; Kajava, S.; Mughal, M.; Matilainen, P.; Mononen, J. Mononen, Evaluation of the confusion matrix method in the validation of an automated system for measuring feeding behaviour of cattle. Behav. Process. 2018, 148, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Japkowicz, N.; Shah, M. Evaluating Learning Algorithms: A Classification Perspective; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Demšar, J. Statistical comparisons of classifiers over multiple data sets. J. Mach. Learn. Res. 2006, 7, 1–30. [Google Scholar]
- Benavoli, A.; Corani, G.; Mangili, F. Should we really use post-hoc tests based on mean-ranks? J. Mach. Learn. Res. 2016, 17, 152–161. [Google Scholar]
- Garcia, S.; Herrera, F. An Extension on “Statistical Comparisons of Classifiers over Multiple Data Sets” for all Pairwise Comparisons. J. Mach. Learn. Res. 2008, 9, 2677–2694. [Google Scholar]
- Bisong, E. Building Machine Learning and Deep Learning Models on Google Cloud Platform; Apress: Berkeley, CA, USA, 2019; pp. 7–10. [Google Scholar]
- Dubey, A.K.; Jain, V. Automatic facial recognition using VGG16 based transfer learning model. J. Inf. Optim. Sci. 2020, 41, 1589–1596. [Google Scholar] [CrossRef]
- Seabold, S.; Perktold, J. Statsmodels: Statsmodels: Econometric and Statistical Modeling with Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; Volume 57. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Saha, P.; Sadi, M.S.; Islam, M.M. EMCNet: Automated COVID-19 diagnosis from X-ray images using convolutional neural network and ensemble of machine learning classifiers. Inform. Med. Unlocked 2021, 22, 100505. [Google Scholar] [CrossRef]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-ray8: Hospital-scale Chest X- ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 3462–3471. [Google Scholar] [CrossRef]
- Liu, C.; van Netten, J.J.; Van Baal, J.G.; Bus, S.A.; van Der Heijden, F. Automatic detection of diabetic foot complications with infrared thermography by asymmetric analysis. J. Biomed. Opt. 2015, 20, 026003. [Google Scholar] [CrossRef]
- Jegede, O.; Ferens, K.; Griffith, B.; Podaima, B. A smart shoe to prevent and manage diabetic foot diseases. In Proceedings of the International Conference on Health Informatics and Medical Systems, Iasi, Romania, 19–21 November 2015; pp. 47–54. [Google Scholar]
- Malik, H.; Bashir, U.; Ahmad, A. Multi-classification neural network model for detection of abnormal heartbeat audio signals. Biomed. Eng. Adv. 2022, 4, 100048. [Google Scholar] [CrossRef]
- Malik, H.; Naeem, A.; Naqvi, R.A.; Loh, W.K. DMFL_Net: A Federated Learning-Based Framework for the Classification of COVID-19 from Multiple Chest Diseases Using X-rays. Sensors 2023, 23, 743. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset Samples | Ischemic DFS | AFS | Total Samples |
|---|---|---|---|
| Original | 1413 | 1413 | 2826 |
| Data Augmentation | 4239 | 4239 | 8478 |
| Training | 2967 | 2967 | 5934 |
| Testing | 424 | 424 | 848 |
| Validation | 848 | 848 | 1696 |
| No. of Layers | Layer (Type) | Output Shape | Parameters |
|---|---|---|---|
| 1 | VGG19-vgg19 (Functional) | (None, 11, 11, 512) | 35,987,564 |
| 2 | reshape_layer | (None, 11, 11, 512) | 0 |
| 3 | conv2d_16 (Conv2D) | (None, 11, 11, 256) | 1,658,974 |
| 4 | activation_function_16 (Activation) | (None, 11, 11, 256) | 0 |
| 5 | global_pooling2d_layer_01 (GAP) | (None, 5, 5, 128) | 0 |
| 6 | droupout_layer_16 (Dropout) | (None, 5, 5, 128) | 0 |
| 7 | flatten_layer_11 (Flatten) | (None, 512) | 0 |
| 8 | dense_layer_12 (DenseLayer) | (None, 512) | 289,658 |
| 9 | droupout_layer_17 (Dropout) | (None, 512) | 0 |
| 10 | dense_layer_13 (DenseLayer) | (None, 2) | 2155 |
| Total Trainable Parameters: 37,938,351 Trainable Parameters: 37,938,000 Non-Trainable Parameters: 351 |
| Classifiers | Accuracy | Precision | Recall | F1-Score | Mcc | AUC |
|---|---|---|---|---|---|---|
| InceptionV3 | 95.52% | 95.31% | 95.75% | 95.53% | 0.9501 | 0.9305 |
| Mobile Net | 96.73% | 96.71% | 97.17% | 96.94% | 0.9612 | 0.9907 |
| Proposed Model | 98.70% | 98.81% | 98.58% | 98.69% | 0.9740 | 0.9953 |
| Proposed Model with UNet++ | 99.05% | 98.99% | 98.58% | 99.01% | 0.9801 | 0.9967 |
| Types | Sum of Squares | Degrees of Freedom | F | p-Value |
|---|---|---|---|---|
| C (treatments) | 0.176632 | 4 | 16.712736 | 1.69 × 10−11 |
| Residual | 0.327389 | 120 | - | - |
| Pair | p-Value | Holm’s Corrected Alpha | Null Hypothesis (NH) |
|---|---|---|---|
| Proposed Model vs. MobileNet | 0.0014 | 0.005 | Reject |
| Proposed Model vs. Inception-v3 | 0.0012 | 0.00556 | Reject |
| Ref | Model Name | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) |
|---|---|---|---|---|---|
| [30] | DFU_QUTNet | 92.5 | 95.4 | 93.6 | 94.5 |
| [35] | CTREE | 88 | 78.3 | 80.6 | - |
| [17] | Faster R-CNN | 72.30 | 74.5 | - | 74.30 |
| [38] | CNN framework | 93.4 | 72.2 | 94.7 | 93.9 |
| [43] | Load Cell | 94.6 | 95.2 | - | 93.2 |
| [46] | KNN | 93.1 | 98.0 | 90.9 | 92.2 |
| [37] | SVM | 76.3 | 73.3 | 94.6 | - |
| Proposed Model | Vgg-19 + CNN | 98.70 | 98.58 | 98.81 | 98.69 |
| Proposed Model with UNet++ | Proposed Model | 99.05 | 98.99 | 99.01 | 99.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalil, M.; Naeem, A.; Naqvi, R.A.; Zahra, K.; Moqurrab, S.A.; Lee, S.-W. Deep Learning-Based Classification of Abrasion and Ischemic Diabetic Foot Sores Using Camera-Captured Images. Mathematics 2023, 11, 3793. https://doi.org/10.3390/math11173793
Khalil M, Naeem A, Naqvi RA, Zahra K, Moqurrab SA, Lee S-W. Deep Learning-Based Classification of Abrasion and Ischemic Diabetic Foot Sores Using Camera-Captured Images. Mathematics. 2023; 11(17):3793. https://doi.org/10.3390/math11173793
Chicago/Turabian StyleKhalil, Mudassir, Ahmad Naeem, Rizwan Ali Naqvi, Kiran Zahra, Syed Atif Moqurrab, and Seung-Won Lee. 2023. "Deep Learning-Based Classification of Abrasion and Ischemic Diabetic Foot Sores Using Camera-Captured Images" Mathematics 11, no. 17: 3793. https://doi.org/10.3390/math11173793
APA StyleKhalil, M., Naeem, A., Naqvi, R. A., Zahra, K., Moqurrab, S. A., & Lee, S. -W. (2023). Deep Learning-Based Classification of Abrasion and Ischemic Diabetic Foot Sores Using Camera-Captured Images. Mathematics, 11(17), 3793. https://doi.org/10.3390/math11173793