
Baseline Quality of Life of Physical Function Is Highly Relevant for Overall Survival in Advanced Rectal Cancer


 , and
, and 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Cohort
2.2. Patient-Reported Outcome
2.3. Statistical Analyses
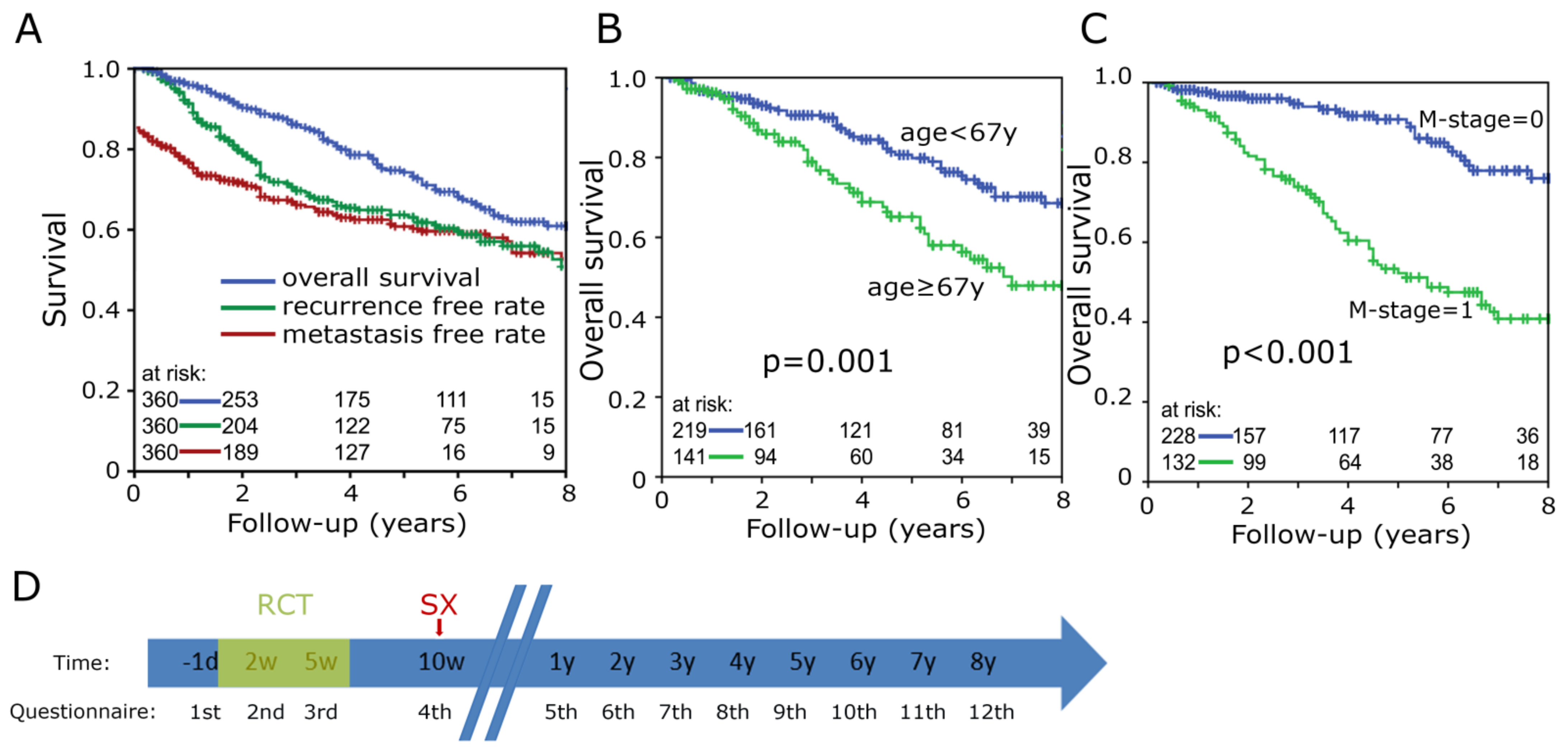
3. Results
3.1. Clinical Characteristics
3.2. Function and Symptom Scores
3.3. Physical Function Individual Questions
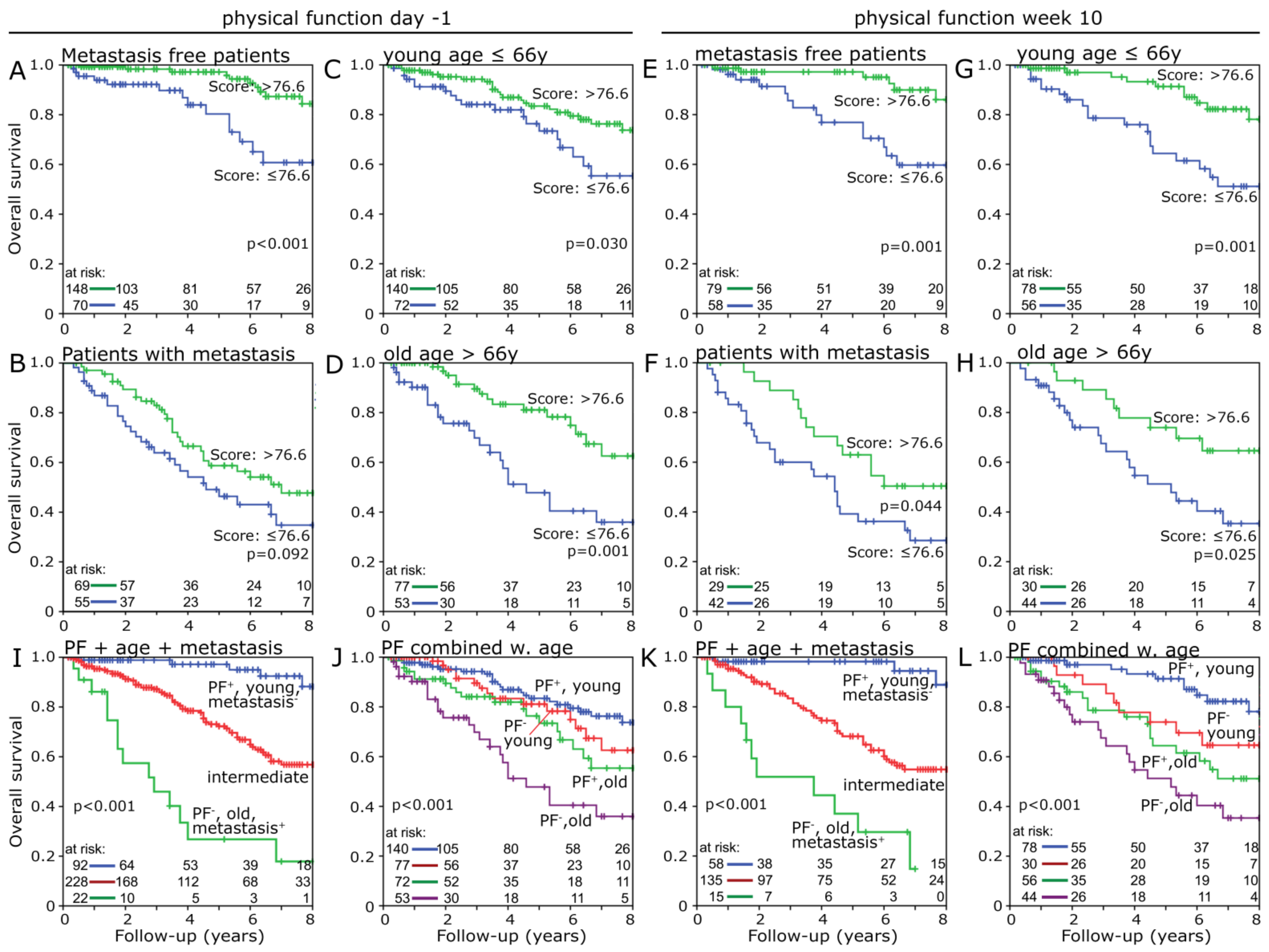
3.4. Physical Function
3.5. Change Score
3.6. Risk Factor Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RC | rectal cancer |
| RCT | radiochemotherapy |
| QOL | quality of life |
| EORCT | European Organization for Research and Treatment of Cancer |
| ROC | receiver operating characteristic |
| MET | metabolic equivalent of task (MET) |
References
- Nair, C.K.; George, P.S.; Rethnamma, K.S.; Bhargavan, R.; Rahman, S.A.; Mathew, A.P.; Muralee, M.; Cherian, K.; Augustine, P.; Ahamed, M.I. Factors affecting health related quality of life of rectal cancer patients undergoing surgery. Indian J. Surg. Oncol. 2014, 5, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonk-Klaassen, S.M.; De Vocht, H.M.; den Ouden, M.E.M.; Eddes, E.H.; Schuurmans, M.J. Ostomy-related problems and their impact on quality of life of colorectal cancer ostomates: A systematic review. Qual. Life Res. 2016, 25, 125–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, H.; Schrotz-King, P.; Holleczek, B.; Katalinic, A.; Hoffmeister, M. Declining Bowel Cancer Incidence and Mortality in Germany. Dtsch. Arztebl. Int. 2016, 113, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Lee, Y.; Jang, D.; Shin, A. Physical Activity after Colorectal Cancer Diagnosis and Mortality in a Nationwide Retrospective Cohort Study. Cancers 2021, 13, 4804. [Google Scholar] [CrossRef]
- Slattery, M.L.; Edwards, S.; Curtin, K.; Ma, K.; Edwards, R.; Holubkov, R.; Schaffer, D. Physical activity and colorectal cancer. Am. J. Epidemiol. 2003, 158, 214–224. [Google Scholar] [CrossRef] [Green Version]
- Van Blarigan, E.L.; Meyerhardt, J.A. Role of physical activity and diet after colorectal cancer diagnosis. J. Clin. Oncol. 2015, 33, 1825–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, F.; You, Y.; Huang, J.; Guan, C.; Chen, Z.; Fang, M.; Yao, F.; Han, J. Association between physical activity and digestive-system cancer: An updated systematic review and meta-analysis. J. Sport Health Sci. 2021, 10, 4–13. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.-M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; De Gonzalez, A.B.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Balhareth, A.; Aldossary, M.Y.; McNamara, D. Impact of physical activity and diet on colorectal cancer survivors’ quality of life: A systematic review. World J. Surg. Oncol. 2019, 17, 153. [Google Scholar] [CrossRef] [Green Version]
- Nolte, S.; Waldmann, A.; Liegl, G.; Petersen, M.A.; Groenvold, M.; Rose, M. Updated EORTC QLQ-C30 general population norm data for Germany. Eur. J. Cancer 2020, 137, 161–170. [Google Scholar] [CrossRef]
- Schmid, D.; Leitzmann, M.F. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: A systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1293–1311. [Google Scholar] [CrossRef]
- Qiu, S.; Jiang, C.; Zhou, L. Physical activity and mortality in patients with colorectal cancer: A meta-analysis of prospective cohort studies. Eur. J. Cancer Prev. 2020, 29, 15–26. [Google Scholar] [CrossRef]
- Walter, V.; Jansen, L.; Knebel, P.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Physical activity and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2017, 140, 1985–1997. [Google Scholar] [CrossRef] [Green Version]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Hardikar, S.; Newcomb, P.A.; Campbell, P.T.; Win, A.; Lindor, N.M.; Buchanan, D.; Makar, K.W.; Jenkins, M.; Potter, J.; Phipps, A.I. Prediagnostic Physical Activity and Colorectal Cancer Survival: Overall and Stratified by Tumor Characteristics. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 1130–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyl, R.E.; Xie, K.; Koch-Gallenkamp, L.; Brenner, H.; Arndt, V. Quality of life and physical activity in long-term (≥5 years post-diagnosis) colorectal cancer survivors—Systematic review. Health Qual. Life Outcomes 2018, 16, 112. [Google Scholar] [CrossRef]
- Schumacher, O.; Luo, H.; Taaffe, D.R.; Galvão, D.A.; Tang, C.; Chee, R.; Spry, N.; Newton, R.U. Effects of exercise during radiotherapy on physical function and treatment-related side effects in men with prostate cancer: A systematic review and meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 716–731. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Allenby, T.; Lin, J.; Rosenberg, J.; Simone, N.L.; Schmitz, K.H. Exercise Therapy and Radiation Therapy for Cancer: A Systematic Review. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Loughney, L.; West, M.A.; Moyses, H.; Bates, A.; Kemp, G.J.; Hawkins, L.; Varkonyi-Sepp, J.; Burke, S.; Barben, C.P.; Calverley, P.M.; et al. The effects of neoadjuvant chemoradiotherapy and an in-hospital exercise training programme on physical fitness and quality of life in locally advanced rectal cancer patients: A randomised controlled trial (The EMPOWER Trial). Perioper. Med. 2021, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Krebsgesellschaft, D.K. AWMF, S3-Leitlinie Kolorektales Karzinom (Langversion 2.1). 2019. Available online: https://www.awmf.org/uploads/tx_szleitlinien/021-007OLl_S3_Kolorektales-Karzinom-KRK_2019-01.pdf (accessed on 22 November 2020).
- Patel, S.G.; Ahnen, D.J. Colorectal Cancer in the Young. Curr. Gastroenterol. Rep. 2018, 20, 15. [Google Scholar] [CrossRef]
- Simon, K.; Simon, K. Colorectal cancer development and advances in screening. Clin. Interv. Aging 2016, 11, 967–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebsregisterdaten, Z.f. Anus-C21. 2018. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/kid_2021/kid_2021_c21_anus.pdf?__blob=publicationFile (accessed on 1 January 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Groups |
|---|---|
| Sex | female: 105 (29.2%); male: 255 (70.8%) |
| Age at diagnosis (yr) | mean: 62.47; min: 15; max: 86 |
| T category | pT1: 11 (3.1%); pT2: 40 (11.1%); pT3: 219 (60.8%); pT4: 89 (24.7%) |
| N category | N0: 103 (28.6%); N1: 178 (49.4%); N2: 78 (21.7%) |
| M category | M0: 228 (63.3%); M1: 132 (36.7%) |
| Stage | UICC I: 24 (6.7%); UICC II: 46 (12.8%); UICC III: 157 (43.6%); UICC IV: 132 (36.7%) |
| Histological grading | G1: 19 (5.3%); G2: 274 (76.1%); G3: 57 (15.8%) |
| Radiation dose (Gy) | 50.4: 344 (95.6%); >50.4: 16 (4.4%) |
| Chemotherapy | FOLFOX: 268 (74.4%); FOLFIRI: 18 (5%); FOLFOXIRI: 10 (2.8%); 5-FU solo: 52 (14.4%); XELOX: 8 (2.2%) |
| Surgery | Yes: 331 (91.9%); No: 29 (8.1%) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | Hazard Ratio | 95% C.I. | p | Hazard Ratio | 95% C.I. | p |
| Physical function ≤ 76.6 [n = 119] vs. >76.6 [n = 213] | 0.465 | 0.288–0.752 | 0.002 | 0.542 | 0.345–0.85 | 0.008 |
| Sex f [n = 97] vs. m [n = 235] | 1.639 | 0.927–2.896 | 0.089 | 1.486 | 0.867–2.547 | 0.150 |
| Age <67 [n = 205] vs. ≥67 [n = 127] | 1.931 | 1.219–3.06 | 0.005 | 2.047 | 1.302–3.216 | 0.002 |
| T1/2/3 [n = 249] vs. T4 [n = 83] | 1.092 | 0.641–1.862 | 0.746 | --- | --- | --- |
| N0 [n = 95] vs. N1/2 [n = 237] | 0.768 | 0.469–1.257 | 0.293 | --- | --- | --- |
| M0 [n = 210] vs. M1 [n = 122] | 4.566 | 2.727–7.645 | <0.001 | 4.669 | 2.81–7.758 | <0.001 |
| G1/2 [n = 278] vs. G3 [n = 54] | 1.572 | 0.886–2.789 | 0.122 | 1.538 | 0.876–2.699 | 0.134 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fitz, T.; Sörgel, C.; Rutzner, S.; Hecht, M.; Fietkau, R.; Distel, L.V. Baseline Quality of Life of Physical Function Is Highly Relevant for Overall Survival in Advanced Rectal Cancer. Healthcare 2022, 10, 141. https://doi.org/10.3390/healthcare10010141
Fitz T, Sörgel C, Rutzner S, Hecht M, Fietkau R, Distel LV. Baseline Quality of Life of Physical Function Is Highly Relevant for Overall Survival in Advanced Rectal Cancer. Healthcare. 2022; 10(1):141. https://doi.org/10.3390/healthcare10010141
Chicago/Turabian StyleFitz, Tim, Christopher Sörgel, Sandra Rutzner, Markus Hecht, Rainer Fietkau, and Luitpold V. Distel. 2022. "Baseline Quality of Life of Physical Function Is Highly Relevant for Overall Survival in Advanced Rectal Cancer" Healthcare 10, no. 1: 141. https://doi.org/10.3390/healthcare10010141
APA StyleFitz, T., Sörgel, C., Rutzner, S., Hecht, M., Fietkau, R., & Distel, L. V. (2022). Baseline Quality of Life of Physical Function Is Highly Relevant for Overall Survival in Advanced Rectal Cancer. Healthcare, 10(1), 141. https://doi.org/10.3390/healthcare10010141