
Development of a Bamlanivimab Infusion Process in the Emergency Department for Outpatient COVID-19 Patients


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
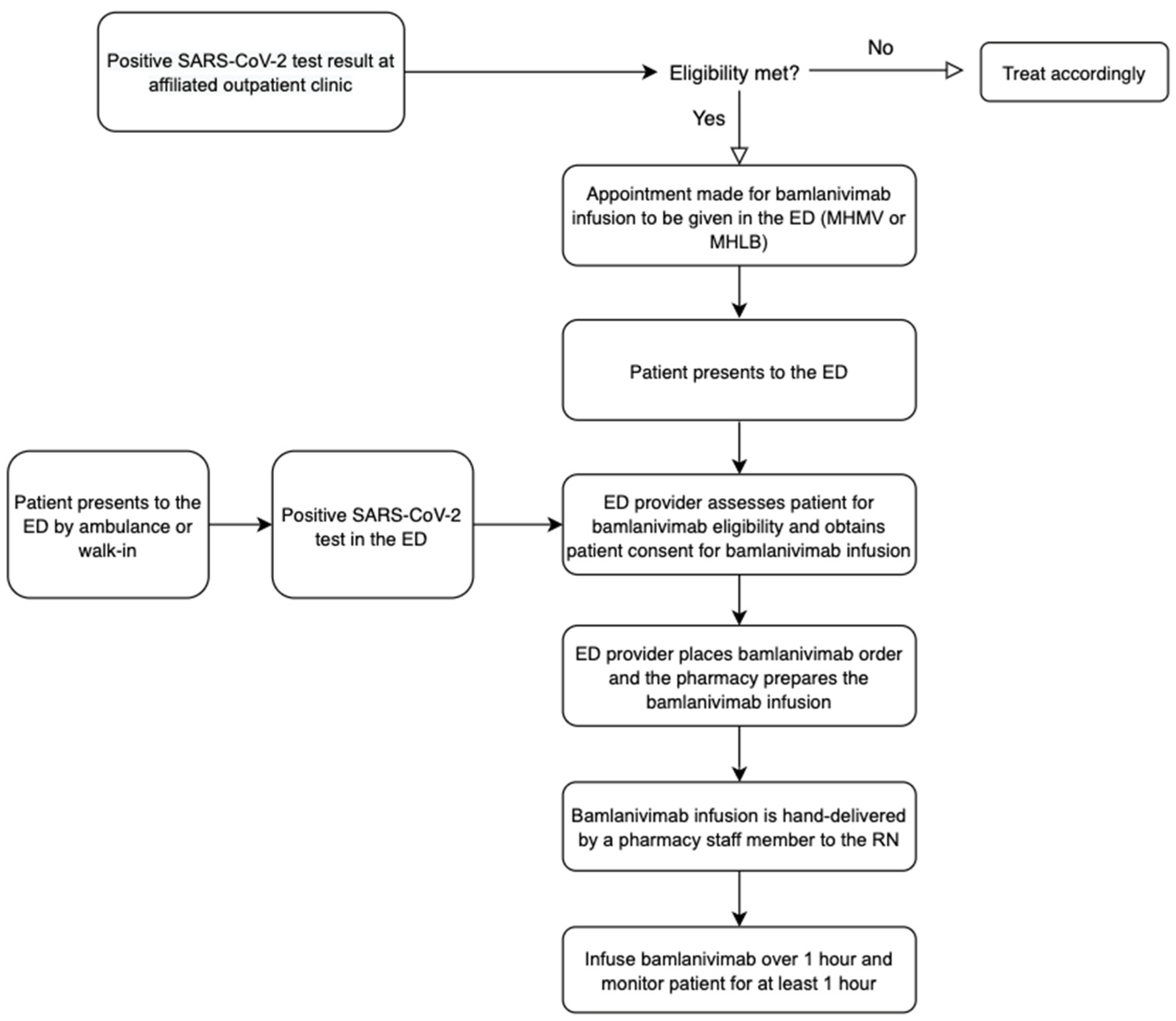
2.1. Providence Mission Hospital Mission Viejo and Providence Mission Hospital Laguna Beach
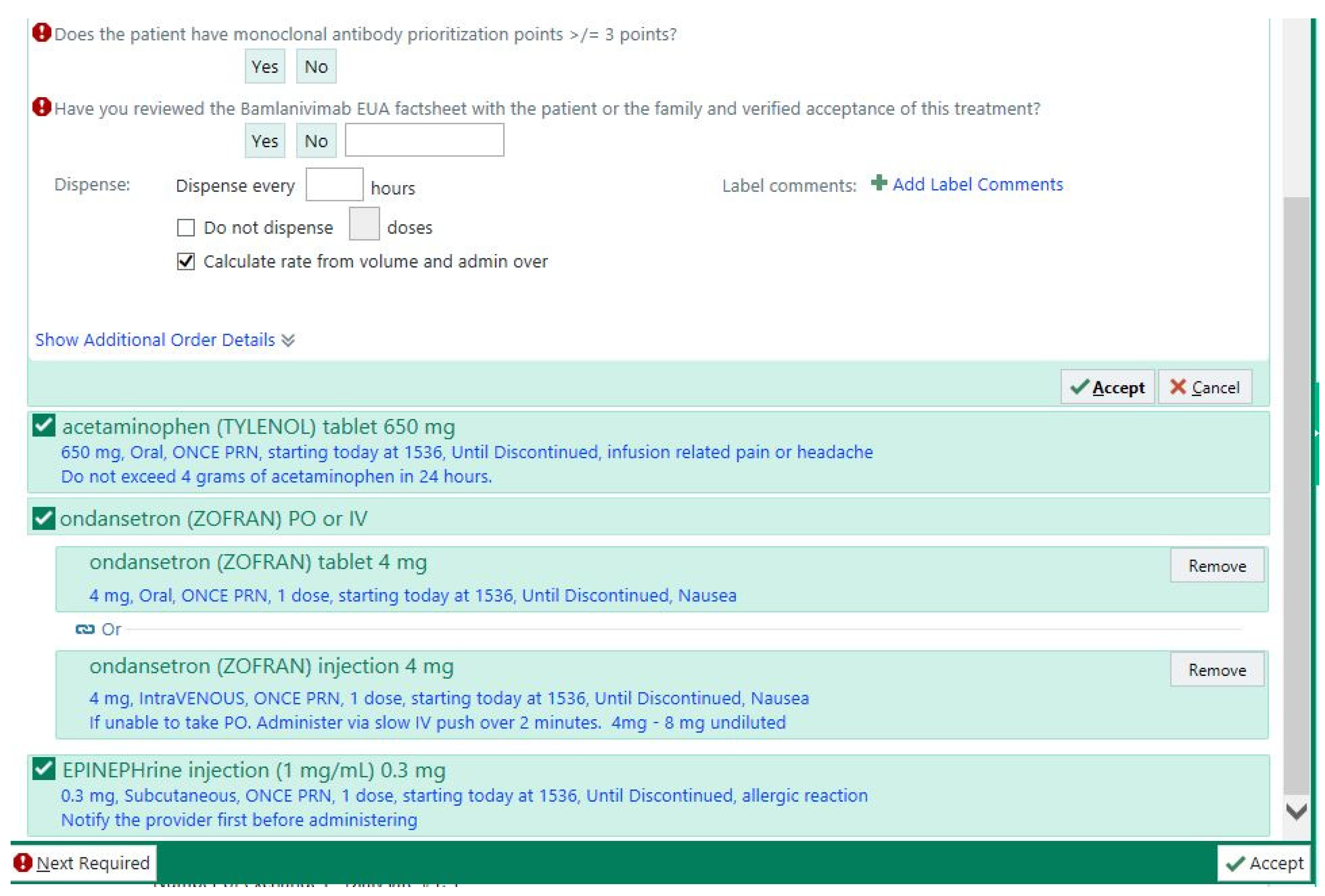
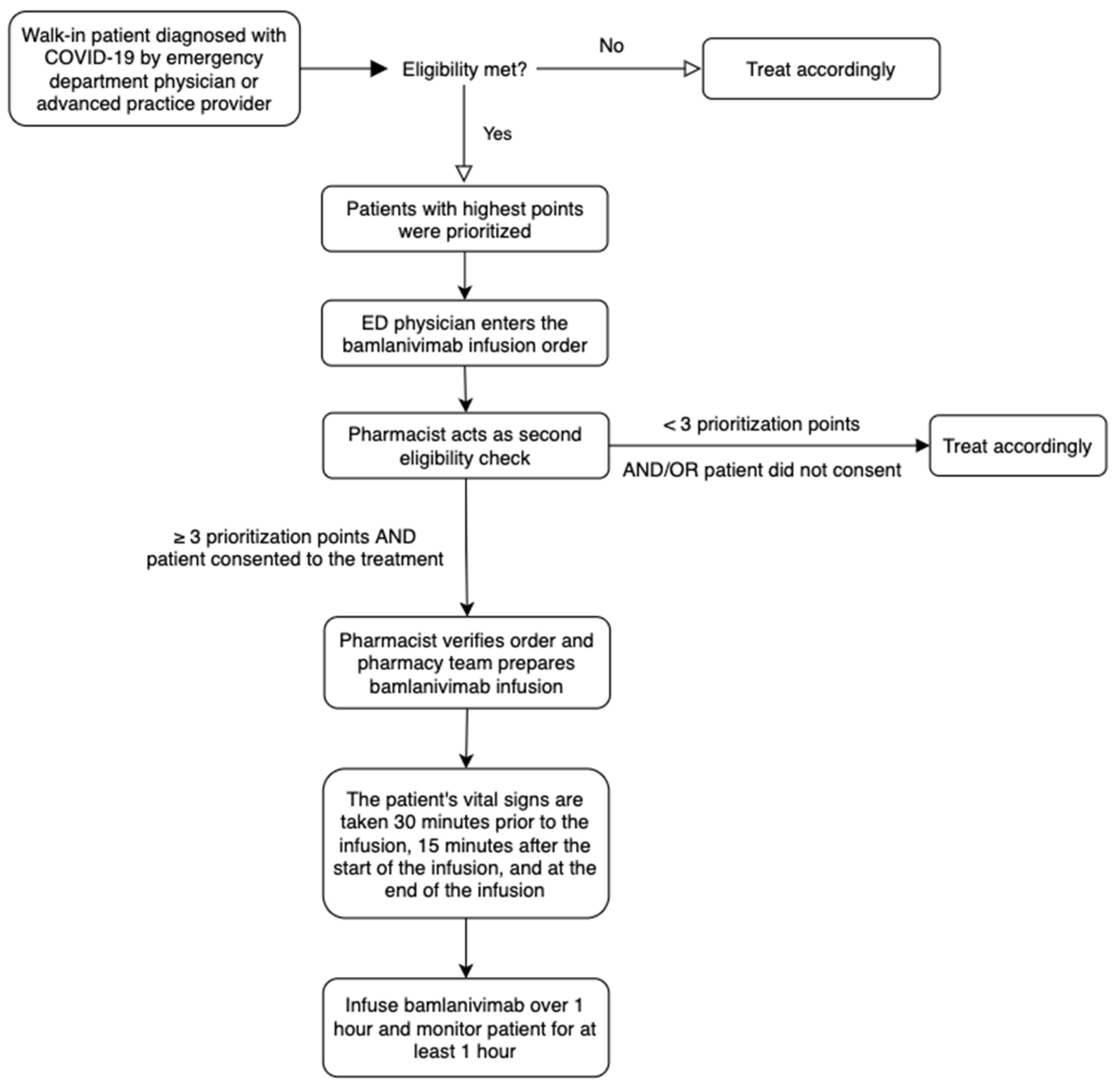
2.2. University of California Irvine Medical Center
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. World Health Organization. Available online: https://covid19.who.int/ (accessed on 2 November 2021).
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X. Human neutralizing antibodies elicited by SARS-COV-2 infection. Nature 2020, 584, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Health Care Providers Emergency Use Authorization (eua) of Bamlanivimab. Available online: https://www.fda.gov/media/143603/download (accessed on 15 May 2021).
- ACTIV-3/TICO LY-CoV555 Study Group. A neutralizing monoclonal antibody for hospitalized patients with COVID-19. N. Engl. J. Med. 2020, 384, 905–914. [Google Scholar]
- Chen, P.; Nirula, A.; Heller, B.; Gottlieb, R.L.; Boscia, J.; Morris, J.; Huhn, G. SARS-COV-2 neutralizing antibody LY-Cov555 in outpatients with Covid-19. N. Engl. J. Med. 2021, 384, 229–237. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 15 May 2021).
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Infectious Diseases Society of America 2021; Version 5.1.2. Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/ (accessed on 15 May 2021).
- Dotan, I.; Panaccione, R.; Kaplan, G.G.; O’Morain, C.; Lindsay, J.O.; Abreu, M.T. Best Practice Guidance for Adult Infusion Centres during the COVID-19 Pandemic: Report from the COVID-19 International Organization for the Study of IBD [IOIBD] Task Force. J. Crohn’s Colitis 2020, 14 (Suppl. S3), S785–S790. [Google Scholar]
- Payette, C.; Brooks, J.T.; Shesser, R. Emergency department administration of COVID-19 antibody therapies: Early experience. Am. J. Emerg. Med. 2021, 49, 432–433. [Google Scholar] [CrossRef] [PubMed]
- Jodoin, K.; Farcy, D.; Caldera, A.; Dalley, M.; Patel, B.; Stuart, W.; Telas, G.; Atisha, M. Covid-19 monoclonal antibody infusions: A multidisciplinary initiative to operationalize EUA Novel Treatment Options. J. Clin. Outcomes Manag. 2021, 28, 70–81. [Google Scholar] [CrossRef]
- Cohen, M.S.; Nirula, A.; Mulligan, M.J. Effect of bamlanivimab vs placebo on incidence of COVID-19 among residents and staff of skilled nursing and assisted living facilities—A randomized clinical trial. JAMA 2021, 326, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Nirula, A.; Chen, P. Effect of Bamlanivimab as Monotherapy or in Combination with Etesevimab on Viral Load in Patients with Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef] [PubMed]
- California Department of Public Health. Health Alert: Concerns re: The use of Bamlanivimab Monotherapy in the Setting of SARS-CoV2 Variants. 19 March 2021. Available online: http://publichealth.lacounty.gov/eprp/lahan/alerts/CAHANBamlanivimabandSARSCoV2Variants.pdf (accessed on 20 December 2021).
- U.S. Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab. 16 April 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab (accessed on 15 May 2021).
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T. Regn-COV2, a neutralizing antibody cocktail, in outpatients with covid-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal Antibodies for Treatment of COVID-19. 21 November 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-monoclonal-antibodies-treatment-covid-19 (accessed on 15 May 2021).
- U.S. Food and Drug Administration. FDA authorizes Bamlanivimab and Etesevimab Monoclonal Antibody Therapy for Post-Exposure Prophylaxis (Prevention) for COVID-19. 9 February 2021. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-authorizes-bamlanivimab-and-etesevimab-monoclonal-antibody-therapy-post-exposure-prophylaxis (accessed on 20 December 2021).
- Dougan, M.; Nirula, A.; Azizad, M. Bamlanivimab plus Etesevimab in Mild or Moderate Covid-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians. ACEP Statement on Monoclonal Antibody Infusion. 1 February 2021. Available online: https://www.acep.org/corona/COVID-19-alert/covid-19-articles/acep-statement-on-monoclonal-antibody-infusion/ (accessed on 20 December 2021).




{kind=link}
{kind=link}
{kind=link}
Inclusion Criteria:
|
Exclusion Criteria
|
| Age ≥ 80 years (4 points) |
| Age 65–79 years (2 points) |
| Age ≥ 50 years (1 point) |
| Solid organ transplant (3 points) |
| Body mass index (BMI) ≥ 35 kg/m2 (2 points) |
| Hematologic cancer (2 points) |
| Male sex (1 point) |
| Ethnicity non-white (1 point) |
| Chronic kidney disease (1 point) |
| Cirrhosis (1 point) |
| COPD (1 point) |
| Hypertension (1 point) |
| Heart disease (1 point) |
| Diabetes (1 point) |
| Recent (within 1 year) non-hematologic cancer (1 point) |
| Currently receiving immunosuppressive treatment (1 point) |
| Pregnancy (1 point) |
| Symptoms < 4 days (1 point) |
| Age, years (Mean ± SD) | 62 ± 16 |
| Male, n (%) | 308 (51.2) |
| Hypertension, n (%) | 340 (56.6) |
| Chronic kidney disease, n (%) | 79 (13.1) |
| Immunosuppressive disease or on immunosuppressive treatment, n (%) | 142 (23.6) |
| Body mass index ≥ 35 kg/m2, n (%) | 109 (18.1) |
| Diabetes, n (%) | 170 (28.3) |
| Asthma, n (%) | 98 (16.3) |
| Chronic obstructive pulmonary disorder, n (%) | 25 (4.2) |
| Sickle cell anemia, n (%) | 9 (1.5) |
| Heart disease (congenital or acquired), n (%) | 141 (23.5) |
| Neurodevelopmental disorders, n (%) | 101 (16.8) |
| Medical-related device dependence *, n (%) | 16 (2.7) |
| Hospitalization for COVID-19 within 10 days of receiving bamlanivimab, n (%) | 87 (14.5) |
| Admission for COVID-19 within 10 days of receiving bamlanivimab, n (%) | 43 (7.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pham, D.H.; Wong, S.; Nguyen, C.T.; Lee, S.C.; Won, K.J. Development of a Bamlanivimab Infusion Process in the Emergency Department for Outpatient COVID-19 Patients. Healthcare 2022, 10, 42. https://doi.org/10.3390/healthcare10010042
Pham DH, Wong S, Nguyen CT, Lee SC, Won KJ. Development of a Bamlanivimab Infusion Process in the Emergency Department for Outpatient COVID-19 Patients. Healthcare. 2022; 10(1):42. https://doi.org/10.3390/healthcare10010042
Chicago/Turabian StylePham, Danny H., Sandy Wong, Christina T. Nguyen, Stephen C. Lee, and Kimberly J. Won. 2022. "Development of a Bamlanivimab Infusion Process in the Emergency Department for Outpatient COVID-19 Patients" Healthcare 10, no. 1: 42. https://doi.org/10.3390/healthcare10010042
APA StylePham, D. H., Wong, S., Nguyen, C. T., Lee, S. C., & Won, K. J. (2022). Development of a Bamlanivimab Infusion Process in the Emergency Department for Outpatient COVID-19 Patients. Healthcare, 10(1), 42. https://doi.org/10.3390/healthcare10010042