
Can Yoga, Qigong, and Tai Chi Breathing Work Support the Psycho-Immune Homeostasis during and after the COVID-19 Pandemic? A Narrative Review


 and
and 
{kind=link}
Abstract
:1. Introduction
1.1. Breathing Biodynamics
1.2. Traditional and Complementary Medicines
1.2.1. Traditional Chinese Medicine
1.2.2. Ayurveda Medicine
- “Vata” governs breathing, blinking, muscle and tissue movement, pulsation of the heart, and all movements in the cytoplasm and cell membranes. In balance, “vata” promotes creativity and flexibility. Out of balance, “vata” produces fear and anxiety.
- “Pitta” governs digestion, absorption, assimilation, nutrition, metabolism and body temperature. In balance, “pitta” promotes understanding and intelligence. Out of balance, “pitta” arouses anger, hatred and jealousy.
- “Kapha” forms the body’s structure, such as bones, muscles, and tendons, and provides the “glue” that holds the cells together. “Kapha” supplies the water for all bodily parts and systems. It lubricates joints, moisturizes the skin and maintains immunity. In balance, “kapha” is expressed as love, calmness and forgiveness. Out of balance, it leads to attachment, greed and envy.
2. Methods—Literature Search
- -
- Qigong—“Qigong”, “Qi Gong”, “Chi Kung”, “Qi kung” and “Chi Gong”;
- -
- Tai Chi—“Tai Chi” (some studies were excluded from the count given that they referred to Tai Chi T’ao, a journalist with particular socio-political relevance);
- -
- Yoga—“Yoga”.
3. Results
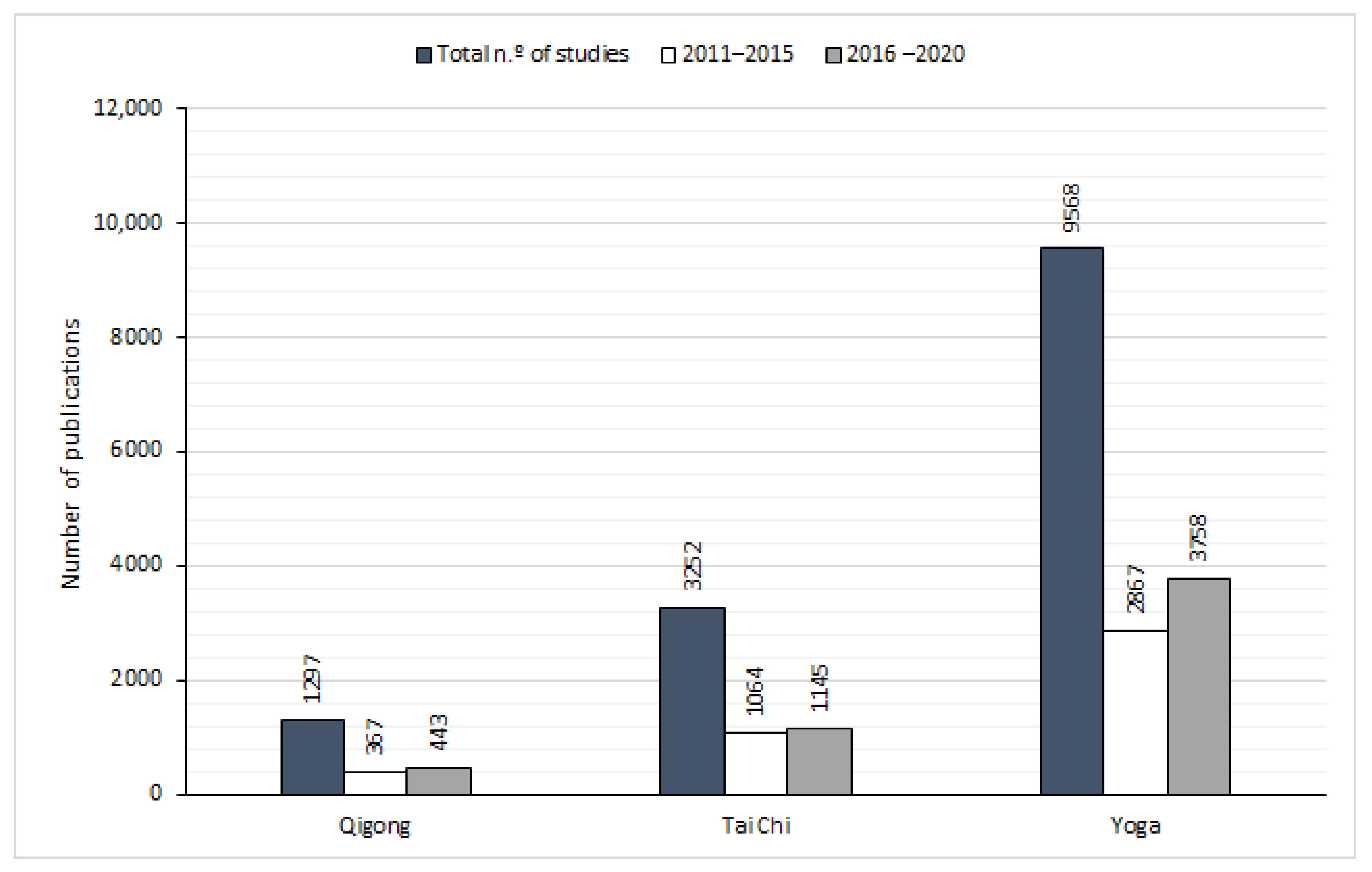
3.1. Quantitative Analysis
3.2. Qualitative Analyses Based on Review—General Reported Effects
3.2.1. Conventional Medicine
3.2.2. Qigong Breathing Effects
3.2.3. Tai Chi Breathing Effects
3.2.4. Yoga Breathing Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merriam-Webster. Medicine|Definition of Medicine. 2018. Available online: https://www.merriam-webster.com/dictionary/medicine (accessed on 1 February 2018).
- Mrazek, M.D.; Franklin, M.S.; Phillips, D.T.; Baird, B.; Schooler, J.W. Mindfulness training improves working memory capacity and GRE performance while reducing mind wandering. Psychol. Sci. 2013, 24, 776–781. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Reyes, J.A.; Iglesias-Julios, M.; Martín-Elola, C.; Losada-Pérez, M.; Monedero, I.; Pita, M.; Turiégano, E. Cambios en la preferencia por rostros masculinos durante el ciclo menstrual en población española. An. Psicol. Ann. Psychol. 2014, 30, 667–675. [Google Scholar] [CrossRef]
- Bodeker, G.; Ong, C.-K. WHO Global Atlas of Traditional, Complementary and Alternative Medicine; World Health Organization: Geneva, Switzerland, 2005; Volume 1. [Google Scholar]
- Xue, C.C. Traditional, complementary and alternative medicine: Policy and public health perspectives. Bull. World Health Organ. 2008, 86, 77. [Google Scholar] [CrossRef]
- Shukla, M.; Chauhan, D.; Raj, R. Breathing exercises and pranayamas to decrease perceived exertion during breath-holding while locked-down due to COVID-19 online randomized study. Complement Clin Pract. 2020, 41, 101248. [Google Scholar] [CrossRef] [PubMed]
- Parimala, S.; Kanchibhotla, D. Association Between Yogic Breathing Practice with Perceived Impact of COVID-19: A Cross-Sectional Study from India. Asia Pac. J. Public Health 2021, 33, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Adhikari, C.; Saha, S.; Saxena, D. Yoga, immunity and COVID-19: A scoping review. J. Fam. Med. Prim. Care 2022, 11, 1683–1701. [Google Scholar]
- Sawant, R.S.; Zinjurke, B.D.; Binorkar, S.V. Preventive aspect of ayurveda and yoga towards newly emerging disease COVID-19. J. Complement Integr. Med. 2021, 18, 667–678. [Google Scholar] [CrossRef]
- Feng, F.; Tuchman, S.; Denninger, J.W.; Fricchione, G.L.; Yeung, A. Qigong for the Prevention, Treatment, and Rehabilitation of COVID-19 Infection in Older Adults. Am. J. Geriatr. Psychiatry 2020, 28, 812–819. [Google Scholar] [CrossRef]
- Badakhsh, M.; Dastras, M.; Sarchahi, Z.; Doostkami, M.; Mir, A.; Bouya, S. Complementary and alternative medicine therapies and COVID-19: A systematic review. Rev. Environ. Health 2021, 36, 443–450. [Google Scholar] [CrossRef]
- Xu, S.; Baker, J.S.; Ren, F. The Positive Role of Tai Chi in Responding to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7479. [Google Scholar] [CrossRef]
- Damasio, A. The Strange Order of Things: Life, Feeling, and the Making of Cultures; Vintage: New York, NY, USA, 2019. [Google Scholar]
- Fromknecht, R.; Goncalves, M.; Greten, H.J.; Machado, J. Are conduits superconductor-like and supported by tetrahedra structure of hyaluronic matrix in living systems? New perspectives. J. Complement. Integr. Med. 2013, 10, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Seeley, R.R.; Stephens, T.D.; Tate, P. Essentials of Anatomy and Physiology; McGraw-Hill: New York, NY, USA, 2002. [Google Scholar]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilo, G.; Revera, M.; Bussotti, M.; Bonacina, D.; Styczkiewicz, K.; Caldara, G.; Giglio, A.; Faini, A.; Giuliano, A.; Lombardi, C. Effects of slow deep breathing at high altitude on oxygen saturation, pulmonary and systemic hemodynamics. PLoS ONE 2012, 7, e49074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferris, B.G.; Pollard, D.S. Effect of deep and quiet breathing on pulmonary compliance in man. J. Clin. Investig. 1960, 39, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haldane, J.; Meakins, J.; Priestley, J. The effects of shallow breathing. J. Physiol. 1919, 52, 433. [Google Scholar] [CrossRef] [Green Version]
- Tobin, M.J.; Chadha, T.S.; Jenouri, G.; Birch, S.J.; Gazeroglu, H.B.; Sackner, M.A. Breathing patterns: 2. Diseased subjects. Chest 1983, 84, 286–294. [Google Scholar] [CrossRef]
- Kunik, M.E.; Roundy, K.; Veazey, C.; Souchek, J.; Richardson, P.; Wray, N.P.; Stanley, M.A. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest 2005, 127, 1205–1211. [Google Scholar] [CrossRef]
- Bhargava, R.; Gogate, M.; Mascarenhas, J. Autonomic responses to breath holding and its variations following pranayama. Ind. J. Physiol. Pharmacol. 1988, 32, 257–264. [Google Scholar]
- Hsieh, C.-W.; Mao, C.-W.; Young, M.-S.; Yeh, T.-L.; Yeh, S.-J. Respiratory effect on the pulse spectrum. J. Med. Eng. Technol. 2003, 27, 77–84. [Google Scholar] [CrossRef]
- Osada, T.; Katsumura, T.; Hamaoka, T.; Murase, N.; Naka, M.; Shimomitsu, T. Quantitative effects of respiration on venous return during single knee extension-flexion. Int. J. Sport. Med. 2002, 23, 183–190. [Google Scholar] [CrossRef]
- Ovadia-Blechman, Z.; Gavish, B.; Levy-Aharoni, D.; Shashar, D.; Aharonson, V. The coupling between peripheral microcirculation and slow breathing. Med. Eng. Phys. 2017, 39, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Kimura, B.J.; Dalugdugan, R.; Gilcrease, G.W., III; Phan, J.N.; Showalter, B.K.; Wolfson, T. The effect of breathing manner on inferior vena caval diameter. Eur. J. Echocardiogr. 2011, 12, 120–123. [Google Scholar] [CrossRef]
- Byeon, K.; Choi, J.-O.; Yang, J.H.; Sung, J.; Park, S.W.; Oh, J.K.; Hong, K.P. The response of the vena cava to abdominal breathing. J. Altern. Complement. Med. 2012, 18, 153–157. [Google Scholar] [CrossRef]
- Nivethitha, L.; Mooventhan, A.; Manjunath, N.; Bathala, L.; Sharma, V.K. Cerebrovascular hemodynamics during the practice of Bhramari Pranayama, Kapalbhati and Bahir-Kumbhaka: An exploratory study. Appl. Psychophysiol. Biofeedback 2018, 43, 87–92. [Google Scholar] [CrossRef]
- Burgess, J.; Ekanayake, B.; Lowe, A.; Dunt, D.; Thien, F.; Dharmage, S.C. Systematic review of the effectiveness of breathing retraining in asthma management. Expert Rev. Respir. Med. 2011, 5, 789–807. [Google Scholar] [CrossRef]
- Vanderlei, L.C.M.; Pastre, C.M.; Hoshi, R.A.; Carvalho, T.D.d.; Godoy, M.F.d. Noções básicas de variabilidade da frequência cardíaca e sua aplicabilidade clínica. Braz. J. Cardiovasc. Surg. 2009, 24, 205–217. [Google Scholar] [CrossRef] [Green Version]
- Cooke, W.H.; Cox, J.F.; Diedrich, A.M.; Taylor, J.A.; Beightol, L.A.; Ames, J.E., IV; Hoag, J.B.; Seidel, H.; Eckberg, D.L. Controlled breathing protocols probe human autonomic cardiovascular rhythms. Am. J. Physiol. Heart Circ. Physiol. 1998, 274, H709–H718. [Google Scholar] [CrossRef]
- Paschoal, M.A.; Petrelluzzi, K.F.S. Estudo da variabilidade da freqüência cardíaca em pacientes com doença pulmonar obstrutiva crônica. Rev. Ciên. Méd. 2012, 11, 27–37. [Google Scholar]
- Stauss, H.M. Heart rate variability. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 285, R927–R931. [Google Scholar] [CrossRef] [Green Version]
- Coote, J.; Chauhan, R. The sympathetic innervation of the heart: Important new insights. Auton. Neurosci. 2016, 199, 17–23. [Google Scholar] [CrossRef]
- KOLÁŘ, P.; Neuwirth, J.; Šanda, J.; Suchanek, V.; Svata, Z.; Volejnik, J.; Pivec, M. Analysis of diaphragm movement during tidal breathing and during its activation while breath holding using MRI synchronized with spirometry. Physiol. Res. 2009, 58, 383–392. [Google Scholar] [CrossRef]
- Vostatek, P.; Novak, D.; Rychnovský, T.; Rychnovská, Š. Diaphragm postural function analysis using magnetic resonance imaging. PLoS ONE 2013, 8, e56724. [Google Scholar] [CrossRef] [Green Version]
- Paterson, D.J.; Nye, P.C. Reflexes arising from the arterial chemoreceptors. Arter. Chemorecept. 1994, 360, 71–86. [Google Scholar]
- Nattie, E.; Li, A. Central chemoreceptors: Locations and functions. Compr. Physiol. 2011, 2, 221–254. [Google Scholar]
- Bernardi, L.; Gabutti, A.; Porta, C.; Spicuzza, L. Slow breathing reduces chemoreflex response to hypoxia and hypercapnia, and increases baroreflex sensitivity. J. Hypertens. 2001, 19, 2221–2229. [Google Scholar] [CrossRef]
- Dick, T.E.; Hsieh, Y.-H.; Dhingra, R.R.; Baekey, D.M.; Galán, R.F.; Wehrwein, E.; Morris, K.F. Cardiorespiratory coupling: Common rhythms in cardiac, sympathetic, and respiratory activities. Prog. Brain Res. 2014, 209, 191–205. [Google Scholar]
- Berntson, G.G.; Cacioppo, J.T.; Quigley, K.S. Respiratory sinus arrhythmia: Autonomic origins, physiological mechanisms, and psychophysiological implications. Psychophysiology 1993, 30, 183–196. [Google Scholar] [CrossRef]
- Yasuma, F.; Hayano, J.-I. Respiratory sinus arrhythmia: Why does the heartbeat synchronize with respiratory rhythm? Chest 2004, 125, 683–690. [Google Scholar] [CrossRef]
- Hayano, J.; Yasuma, F. Hypothesis: Respiratory sinus arrhythmia is an intrinsic resting function of cardiopulmonary system. Cardiovasc. Res. 2003, 58, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Billman, G.E. Heart rate variability—A historical perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef] [Green Version]
- Thoits, P.A. Stress and health: Major findings and policy implications. J. Health Soc. Behav. 2010, 51 (Suppl. S1), S41–S53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porkert, M.; Hempen, C.-H. Classical Acupuncture: The Standard Textbook; Media, Acta Medicinae Sinensis: Dinkelscherben, Germany, 1995. [Google Scholar]
- Lu, A.-P.; Jia, H.-W.; Xiao, C.; Lu, Q.-P. Theory of traditional Chinese medicine and therapeutic method of diseases. World J. Gastroenterol. 2004, 10, 1854–1856. [Google Scholar] [CrossRef]
- Bell, I.R.; Caspi, O.; Schwartz, G.E.; Grant, K.L.; Gaudet, T.W.; Rychener, D.; Maizes, V.; Weil, A. Integrative medicine and systemic outcomes research: Issues in the emergence of a new model for primary health care. Arch. Intern. Med. 2002, 162, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Winslow, L.C.; Shapiro, H. Physicians want education about complementary and alternative medicine to enhance communication with their patients. Arch. Intern. Med. 2002, 162, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Greten, H.J. Chinese medicine as vegetative systems biology: Part I: Therapeutic methods. HNO 2011, 59, 1160–1164. [Google Scholar] [CrossRef]
- Levinovitz, A. Chairman Mao Invented Traditional Chinese Medicine; The Slate Group: Brooklyn, NY, USA, 2013. [Google Scholar]
- Greten, H.J. Chinese medicine as a model of system biology: Diagnosis as the foundation of acupoint selection. In Current Research in Acupuncture; Springer: New York, NY, USA, 2013; pp. 621–657. [Google Scholar]
- Tsokos, G.C.; Nepom, G.T. Gene therapy in the treatment of autoimmune diseases. J. Clin. Investig. 2000, 106, 181–183. [Google Scholar] [CrossRef]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J.; Lin, F. A comprehensive review of health benefits of qigong and tai chi. Am. J. Health Promot. 2010, 24, e1–e25. [Google Scholar]
- Lad, V. The Human Constitution. Ayurveda: The Science of Self-Healing; Lotus Press: Wilmot, ON, USA, 1985; pp. 26–36. [Google Scholar]
- Patwardhan, B.; Warude, D.; Pushpangadan, P.; Bhatt, N. Ayurveda and traditional Chinese medicine: A comparative overview. Evid. Based Complement. Altern. Med. 2005, 2, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Patwardhan, B. Bridging Ayurveda with evidence-based scientific approaches in medicine. EPMA J. 2014, 5, 19. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.; Miller, B. Ayurveda and Aromatheraphy: The Earth Essential Guide to Ancient Wisdom and Modern Healing; Motilal Banarsidass Publ.: New Delhi, India, 1998. [Google Scholar]
- Ninivaggi, F.J. Ayurveda: A Comprehensive Guide to Traditional Indian Medicine for the West; Rowman & Littlefield: Lanham, MD, USA, 2010. [Google Scholar]
- Hankey, A. CAM modalities can stimulate advances in theoretical biology. Evid. Based Complement. Altern. Med. 2005, 2, 5–12. [Google Scholar]
- Ventegodt, S.; Kandel, I.; Merrick, J. A short history of clinical holistic medicine. Sci. World J. 2007, 7, 1622–1630. [Google Scholar] [CrossRef] [Green Version]
- Jaiswal, Y.S.; Williams, L.L. A glimpse of Ayurveda–The forgotten history and principles of Indian traditional medicine. J. Tradit. Complement. Med. 2017, 7, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhu, Q.; Zhan, C.; Cheng, W.; Mingfang, X.; Fang, M.; Fang, L. Acupressure therapy and Liu Zi Jue Qigong for pulmonary function and quality of life in patients with severe novel coronavirus pneumonia (COVID-19): A study protocol for a randomized controlled trial. Trials 2020, 21, 751. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.B.; Shirley, M.A. Reducing the risk of acid aspiration during cesarean section. Anesth. Analg. 1974, 53, 859–868. [Google Scholar] [CrossRef] [PubMed]
- McGrady, E.; Litchfield, K. Epidural analgesia in labour. Contin. Educ. Anaesth. Crit. Care Pain 2004, 4, 114–117. [Google Scholar] [CrossRef] [Green Version]
- Kamalifard, M.; Shahnazi, M.; Melli, M.S.; Allahverdizadeh, S.; Toraby, S.; Ghahvechi, A. The efficacy of massage therapy and breathing techniques on pain intensity and physiological responses to labor pain. J. Caring Sci. 2012, 1, 73. [Google Scholar]
- Yu, W.-J.; Song, J.-E. Effects of abdominal breathing on state anxiety, stress, and tocolytic dosage for pregnant women in preterm labor. J. Korean Acad. Nurs. 2010, 40, 442–452. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.-B.; Kim, H.-S.; Ko, Y.-H.; Bae, C.-H.; An, S.-E. Effects of abdominal breathing on anxiety, blood pressure, peripheral skin temperature and saturation oxygen of pregnant women in preterm labor. Korean J. Women Health Nurs. 2009, 15, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Chitkara, D.K.; Van Tilburg, M.; Whitehead, W.E.; Talley, N.J. Teaching diaphragmatic breathing for rumination syndrome. Am. J. Gastroenterol. 2006, 101, 2449–2452. [Google Scholar] [CrossRef]
- Ma, X.; Yue, Z.-Q.; Gong, Z.-Q.; Zhang, H.; Duan, N.-Y.; Shi, Y.-T.; Wei, G.-X.; Li, Y.-F. The effect of diaphragmatic breathing on attention, negative affect and stress in healthy adults. Front. Psychol. 2017, 8, 874. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, R.; Kaushik, R.M.; Mahajan, S.K.; Rajesh, V. Biofeedback assisted diaphragmatic breathing and systematic relaxation versus propranolol in long term prophylaxis of migraine. Complement. Ther. Med. 2005, 13, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Meuret, A.E.; Ritz, T.; Wilhelm, F.H.; Roth, W.T. Voluntary hyperventilation in the treatment of panic disorder—Functions of hyperventilation, their implications for breathing training, and recommendations for standardization. Clin. Psychol. Rev. 2005, 25, 285–306. [Google Scholar] [CrossRef] [PubMed]
- Rhinewine, J.P.; Williams, O.J. Holotropic breathwork: The potential role of a prolonged, voluntary hyperventilation procedure as an adjunct to psychotherapy. J. Altern. Complement. Med. 2007, 13, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, H.M.D.; Klipper, M. The Relaxation Response. 1992. Available online: http://www.upegroup.com/uploads/1/1/0/4/11040867/relaxation_response.pdf (accessed on 27 August 2018).
- Goodale, I.L.; Domar, A.D.; Benson, H. Alleviation of premenstrual syndrome symptoms with the relaxation response. Obstet. Gynecol. 1990, 75, 649–655. [Google Scholar] [PubMed]
- Benson, H.; Marzetta, B.; Rosner, B.; Klemchuk, H. Decreased blood-pressure in pharmacologically treated hypertensive patients who regularly elicited the relaxation response. Lancet 1974, 303, 289–291. [Google Scholar] [CrossRef]
- Bourgeois, P. De la désensibilisation systématique aux modifications cognitives sous hypnose. In Annales Médico-Psychologiques; Elsevier Science: Paris, France, 1982. [Google Scholar]
- Sundram, B.M.; Dahlui, M.; Chinna, K. Effectiveness of progressive muscle relaxation therapy as a worksite health promotion program in the automobile assembly line. Ind. Health 2016, 54, 204–214. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health and Human Services. Healthy People 2010; Office of Disease Prevention and Health Promotion, US Department of Health and Human Services: Washington, DC, USA, 2000.
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sport. Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Kopelman, P. Health risks associated with overweight and obesity. Obes. Rev. 2007, 8, 13–17. [Google Scholar] [CrossRef]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Chlif, M.; Keochkerian, D.; Choquet, D.; Vaidie, A.; Ahmaidi, S. Effects of obesity on breathing pattern, ventilatory neural drive and mechanics. Respir. Physiol. Neurobiol. 2009, 168, 198–202. [Google Scholar] [CrossRef]
- Gruzelier, J.; Smith, F.; Nagy, A.; Henderson, D. Cellular and humoral immunity, mood and exam stress: The influences of self-hypnosis and personality predictors. Int. J. Psychophysiol. 2001, 42, 55–71. [Google Scholar] [CrossRef]
- Lee, M.S.; Huh, H.J.; Jeong, S.M.; Jang, H.-S.; Ryu, H.; Park, J.-H.; Chung, H.-T.; Woo, W.-H. Effects of Qigong on immune cells. Am. J. Chin. Med. 2003, 31, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.M. Changes in cytokine production in healthy subjects practicing Guolin Qigong: A pilot study. BMC Complement. Altern. Med. 2001, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Kang, C.W.; Lim, H.J.; Lee, M.S. Effects of Qi-training on anxiety and plasma concentrations of cortisol, ACTH, and aldosterone: A randomized placebo-controlled pilot study. Stress Health 2004, 20, 243–248. [Google Scholar] [CrossRef]
- Lee, M.S.; Lee, M.S.; Choi, E.-S.; Chung, H.-T. Effects of Qigong on blood pressure, blood pressure determinants and ventilatory function in middle-aged patients with essential hypertension. Am. J. Chin. Med. 2003, 31, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Motivala, S.J.; Sollers, J.; Thayer, J.; Irwin, M.R. Tai Chi Chih acutely decreases sympathetic nervous system activity in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1177–1180. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Wei, T.-T.; Wang, C.-C.; Chen, W.-C.; Wang, Y.-M.; Tsai, S.-Y. Acute physiological and psychological effects of qigong exercise in older practitioners. Evid. Based Complement. Altern. Med. 2018, 2018, 4960978. [Google Scholar] [CrossRef] [Green Version]
- Chow, Y.W.; Tsang, H.W. Biopsychosocial effects of qigong as a mindful exercise for people with anxiety disorders: A speculative review. J. Altern. Complement. Med. 2007, 13, 831–840. [Google Scholar] [CrossRef]
- UCLA Center for East-West Medicine. Health Benefits of Tai Chi & Qi Gong and Their Relationship to TCM Therapies. Explore Integrative Medicine 2021. Available online: https://exploreim.ucla.edu/education/health-benefits-of-tai-chi-qi-gong-and-their-relationship-to-tcm-therapies/ (accessed on 4 March 2021).
- Matos, L.; Goncalves, M.; Silva, A.; Mendes, J.; Machado, J.; Greten, H. Assessment of Qigong-related effects by infrared thermography: A case study. J. Chin. Integr. Med. 2012, 10, 663–666. [Google Scholar] [CrossRef]
- Matos, L.C.; Lopes, L.T.; Freire, V.A.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Can the electrical potential of acupoints be used to assess the functional state of meridians and the effects of therapeutics? An exploratory data analysis. J. Bodyw. Mov. Ther. 2021, 26, 309–317. [Google Scholar] [CrossRef]
- Matos, L.C.; Machado, J.; Greten, H.J.; Monteiro, F.J. Changes of skin electrical potential in acupoints from Ren Mai and Du Mai conduits during Qigong practice: Documentation of a clinical phenomenon. J. Bodyw. Mov. Ther. 2019, 23, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Poon, C.; Choy, T.; Koide, F. A reliable method for locating electropermeable points on the skin surface. Am. J. Chin. Med. 1980, 8, 283–289. [Google Scholar] [CrossRef]
- Comunetti, A.; Laage, S.; Schiessl, N.; Kistler, A. Characterization of human skin conductance at acupuncture points. Experientia 1995, 51, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Shang, C. Emerging paradigms in mind–body medicine. J. Altern. Complement. Med. 2001, 7, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Weng, C.-S.; Hung, Y.-L.; Shyu, L.-Y.; Chang, Y.-H. A study of electrical conductance of meridian in the obese during weight reduction. Am. J. Chin. Med. 2004, 32, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-T.; Chang, Y.-H.; Lin, W.-Y.; Xu, J.-M.; Chen, H.-Y.; Chou, P.-L.; Cheng, C.-W.; Chen, Y.-L.; Lin, F.-Y.; Tsai, F.-J.; et al. Applications of Meridian Electrical Conductance for Renal Colic: A Prospective Study. J. Altern. Complement. Med. 2010, 16, 861–866. [Google Scholar] [CrossRef] [Green Version]
- Matos, L.C.; Santos, S.C.; Anderson, J.G.; Machado, J.; Greten, H.J.; Monteiro, F.J. Instrumental Measurements of Water and the Surrounding Space During a Randomized Blinded Controlled Trial of Focused Intention. J. Evid. Based Complement. Altern. Med. 2017, 22, 675–686. [Google Scholar] [CrossRef] [Green Version]
- Matos, L.C.; Santos, S.C.; Anderson, J.G.; Machado, J.; Greten, H.J.; Monteiro, F.J. Can measurements be physically conditioned by thought? Further observations following a focused intention experiment. J. Complement Integr. Med. 2020. [Google Scholar] [CrossRef]
- Matos, L.C.; Sousa, C.M.; Gonçalves, M.; Gabriel, J.; Machado, J.; Greten, H.J. Qigong as a Traditional Vegetative Biofeedback Therapy: Long-Term Conditioning of Physiological Mind-Body Effects. BioMed Res. Int. 2015, 2015, 531789. [Google Scholar] [CrossRef]
- Moreira, A.; Matos, L.C.; Conceição, A.M. Does Qigong Practice Have Benefits on the Management of Parkinson’s Disease? J 2019, 2, 352–363. [Google Scholar] [CrossRef] [Green Version]
- Duarte, L.; Gonçalves, M.; Mendes, P.; Matos, L.C.; Greten, H.J.; Machado, J. Can Qigong improve attention in adolescents? A prospective randomized controlled trial. J. Bodyw. Mov. Ther. 2019, 24, 175–181. [Google Scholar] [CrossRef]
- Rodrigues, J.M.S.; Mestre, M.I.C.; Matos, L.C.; Machado, J.P. Effects of taijiquan and qigong practice over behavioural disorders in school-age children: A pilot study. J. Bodyw. Mov. Ther. 2019, 23, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Posadzki, P. The psychology of qi gong: A qualitative study. Complement. Health Pract. Rev. 2010, 15, 84–97. [Google Scholar] [CrossRef]
- Wang, C.-W.; Ng, S.-M.; Ho, R.T.; Ziea, E.T.; Wong, V.C.; Chan, C.L. The effect of qigong exercise on immunity and infections: A systematic review of controlled trials. Am. J. Chin. Med. 2012, 40, 1143–1156. [Google Scholar] [CrossRef]
- Zeng, Y.; Luo, T.; Xie, H.; Huang, M.; Cheng, A.S. Health benefits of qigong or tai chi for cancer patients: A systematic review and meta-analyses. Complement. Ther. Med. 2014, 22, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Bai, Z.; Guan, Z.; Fan, Y.; Liu, C.; Yang, K.; Ma, B.; Wu, B. The Effects of Qigong for Adults with Chronic Pain: Systematic Review and Meta-Analysis. Am. J. Chin. Med. 2015, 43, 1525–1539. [Google Scholar] [CrossRef] [PubMed]
- Phansuea, P.; Tangwongchai, S.; Rattananupong, T.; Lohsoonthorn, V.; Lertmaharit, S. Effectiveness of a Qigong program on sleep quality among community-dwelling older adults with mild to moderate depression: A randomized controlled trial. J. Health Res. 2020, 34, 305–315. [Google Scholar] [CrossRef]
- Chan, J.S.; Ho, R.T.; Chung, K.-F.; Wang, C.-W.; Yao, T.-J.; Ng, S.-M.; Chan, C.L. Qigong exercise alleviates fatigue, anxiety, and depressive symptoms, improves sleep quality, and shortens sleep latency in persons with chronic fatigue syndrome-like illness. Evid. Based Complement. Altern. Med. 2014, 2014, 106048. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.-J.; Zhang, Y.-X.; Du, W.-S.; Jiang, L.-D.; Jin, R.-F.; Yu, H.-Y.; Liu, J.-M.; Han, M. Effect of Qigong on self-rating depression and anxiety scale scores of COPD patients: A meta-analysis. Medicine 2019, 98, e15776. [Google Scholar] [CrossRef]
- Cheung, B.; Lo, J.; Fong, D.; Chan, M.; Wong, S.; Wong, V.; Lam, K.; Lau, C.; Karlberg, J. Randomised controlled trial of qigong in the treatment of mild essential hypertension. J. Hum. Hypertens. 2005, 19, 697. [Google Scholar] [CrossRef] [Green Version]
- Tsang, H.W.; Fung, K.M.; Chan, A.S.; Lee, G.; Chan, F. Effect of a qigong exercise programme on elderly with depression. Int. J. Geriatr. Psychiatry A J. Psychiatry Late Life Allied Sci. 2006, 21, 890–897. [Google Scholar] [CrossRef]
- Edition, F. Diagnostic and statistical manual of mental disorders. Am. Psychiatr. Assoc. 2013, 21, 591–643. [Google Scholar]
- Liu, D.; Yi, L.; Sheng, M.; Wang, G.; Zou, Y. The Efficacy of Tai Chi and Qigong Exercises on Blood Pressure and Blood Levels of Nitric Oxide and Endothelin-1 in Patients with Essential Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2020, 2020, 3267971. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Lee, M.S.; Kim, H.-J.; Choi, E.-S. Effects of qigong on blood pressure, high-density lipoprotein cholesterol and other lipid levels in essential hypertension patients. Int. J. Neurosci. 2004, 114, 777–786. [Google Scholar] [CrossRef]
- Yeh, G.Y.; Wood, M.J.; Lorell, B.H.; Stevenson, L.W.; Eisenberg, D.M.; Wayne, P.M.; Goldberger, A.L.; Davis, R.B. Effects of tai chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure: A randomized controlled trial. Am. J. Med. 2004, 117, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Pippa, L.; Manzoli, L.; Corti, I.; Congedo, G.; Romanazzi, L.; Parruti, G. Functional capacity after traditional Chinese medicine (qi gong) training in patients with chronic atrial fibrillation: A randomized controlled trial. Prev. Cardiol. 2007, 10, 22–25. [Google Scholar] [CrossRef] [Green Version]
- Barrow, D.; Bedford, A.; Ives, G.; OToole, L.; Channer, K. An evaluation of the effects of Tai Chi Chuan and Chi Kung training in patients with symptomatic heart failure: A randomized controlled pilot study. Postgrad. Med. J. 2007, 83, 717–721. [Google Scholar] [CrossRef] [Green Version]
- Mustian, K.M.; Katula, J.A.; Zhao, H. A pilot study to assess the influence of tai chi chuan on functional capacity among breast cancer survivors. J. Support Oncol. 2006, 4, 139–145. [Google Scholar]
- Li, F.; Harmer, P.; McAuley, E.; Fisher, K.J.; Duncan, T.E.; Duncan, S.C. Tai Chi, self-efficacy, and physical function in the elderly. Prev. Sci. 2001, 2, 229–239. [Google Scholar] [CrossRef]
- Stenlund, T.; Lindström, B.; Granlund, M.; Burell, G. Cardiac rehabilitation for the elderly: Qi Gong and group discussions. Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 5–11. [Google Scholar] [CrossRef]
- Gatts, S.K.; Woollacott, M.H. Neural mechanisms underlying balance improvement with short term Tai Chi training. Aging Clin. Exp. Res. 2006, 18, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Verkuilen, J.V.; Rosengren, K.S.; Grubisich, S.A.; Reed, M.R.; Hsiao-Wecksler, E.T. Effect of combined Taiji and Qigong training on balance mechanisms: A randomized controlled trial of older adults. Med. Sci. Monit. 2007, 13, CR339–CR348. [Google Scholar] [PubMed]
- Liu, X.L.; Chen, S.; Wang, Y. Effects of health Qigong exercises on relieving symptoms of Parkinson’s disease. Evid. Based Complement. Altern. Med. 2016, 2016, 5935782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, J.M.; Mestre, M.; Fredes, L.I. Qigong in the treatment of children with autism spectrum disorder: A systematic review. J. Integr. Med. 2019, 17, 250–260. [Google Scholar] [CrossRef]
- Lee, M.-S.; Lim, H.-J.; Lee, M.S. Impact of qigong exercise on self-efficacy and other cognitive perceptual variables in patients with essential hypertension. J. Altern. Complement. Med. 2004, 10, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Lansinger, B.; Larsson, E.; Persson, L.C.; Carlsson, J.Y. Qigong and exercise therapy in patients with long-term neck pain: A prospective randomized trial. Spine 2007, 32, 2415–2422. [Google Scholar] [CrossRef]
- Mannerkorpi, K.; Arndorw, M. Efficacy and feasibility of a combination of body awareness therapy and qigong in patients with fibromyalgia: A pilot study. J. Rehabil. Med. 2004, 36, 279–281. [Google Scholar] [CrossRef] [Green Version]
- Manzaneque, J.M.; Vera, F.M.; Maldonado, E.F.; Carranque, G.; Cubero, V.M.; Morell, M.; Blanca, M.J. Assessment of immunological parameters following a qigong training program. Med. Sci. Monit. 2004, 10, CR264–CR270. [Google Scholar]
- Oh, B.; Bae, K.; Lamoury, G.; Eade, T.; Boyle, F.; Corless, B.; Clarke, S.; Yeung, A.; Rosenthal, D.; Schapira, L. The effects of tai chi and qigong on immune responses: A systematic review and meta-analysis. Medicines 2020, 7, 39. [Google Scholar] [CrossRef]
- Chen, H.-H.; Yeh, M.-L.; Lee, F.-Y. The effects of Baduanjin qigong in the prevention of bone loss for middle-aged women. Am. J. Chin. Med. 2006, 34, 741–747. [Google Scholar] [CrossRef]
- Spahija, J.; de Marchie, M.; Grassino, A. Effects of imposed pursed-lips breathing on respiratory mechanics and dyspnea at rest and during exercise in COPD. Chest 2005, 128, 640–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Araujo, C.L.P.; Karloh, M.; Reis, C.M.D.; Palú, M.; Mayer, A.F. Pursed-lips breathing reduces dynamic hyperinflation induced by activities of daily living test in patients with chronic obstructive pulmonary disease: A randomized cross-over study. J. Rehabil. Med. 2015, 47, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Greten, H. Handbuch des funktionell therapeutischen Qigong-I Diagnosengerechte Übungspraxis. In Handbook of Functional Therapeutic Qigong I Exercises According to Diagnosis; Heidelberg School of Chinese Medicine: Heidelberg, Germany, 2009; pp. 973–978. [Google Scholar]
- Wang, C.; Collet, J.P.; Lau, J. The effect of Tai Chi on health outcomes in patients with chronic conditions: A systematic review. Arch. Intern. Med. 2004, 164, 493–501. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J. Tai chi chuan: A slow dance for health. Physician Sportsmed. 1999, 27, 109–110. [Google Scholar] [CrossRef]
- Chan, K.; Qin, L.; Lau, M.; Woo, J.; Au, S.; Choy, W.; Lee, K.; Lee, S. A randomized, prospective study of the effects of Tai Chi Chun exercise on bone mineral density in postmenopausal women. Arch. Phys. Med. Rehabil. 2004, 85, 717–722. [Google Scholar] [CrossRef]
- Channer, K.; Barrow, D.; Barrow, R.; Osborne, M.; Ives, G. Changes in haemodynamic parameters following Tai Chi Chuan and aerobic exercise in patients recovering from acute myocardial infarction. Postgrad. Med. J. 1996, 72, 349–351. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.N.; Hong, A.W.; Tomlinson, B.; Lau, E.; Lam, C.W.; Sanderson, J.E.; Woo, J. Effects of Tai Chi and resistance training on cardiovascular risk factors in elderly Chinese subjects: A 12-month longitudinal, randomized, controlled intervention study. Clin. Endocrinol. 2005, 63, 663–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audette, J.F.; Jin, Y.S.; Newcomer, R.; Stein, L.; Duncan, G.; Frontera, W.R. Tai Chi versus brisk walking in elderly women. Age Ageing 2006, 35, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Young, D.R.; Appel, L.J.; Jee, S.; Miller, E.R., III. The effects of aerobic exercise and T’ai Chi on blood pressure in older people: Results of a randomized trial. J. Am. Geriatr. Soc. 1999, 47, 277–284. [Google Scholar] [CrossRef]
- Yeh, G.Y.; McCarthy, E.P.; Wayne, P.M.; Stevenson, L.W.; Wood, M.J.; Forman, D.; Davis, R.B.; Phillips, R.S. Tai chi exercise in patients with chronic heart failure: A randomized clinical trial. Arch. Intern. Med. 2011, 171, 750–757. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Hong, A.; Lau, E.; Lynn, H. A randomized controlled trial of Tai Chi and resistance exercise on bone health, muscle strength and balance in community-living elderly people. Age Ageing 2007, 36, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Kutner, N.G.; Barnhart, H.; Wolf, S.L.; McNeely, E.; Xu, T. Self-report benefits of Tai Chi practice by older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1997, 52, P242–P246. [Google Scholar] [CrossRef]
- Faber, M.J.; Bosscher, R.J.; Paw, M.J.C.A.; van Wieringen, P.C. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: A multicenter randomized controlled trial. Arch. Phys. Med. Rehabil. 2006, 87, 885–896. [Google Scholar] [CrossRef] [Green Version]
- Greenspan, A.I.; Wolf, S.L.; Kelley, M.E.; O’Grady, M. Tai chi and perceived health status in older adults who are transitionally frail: A randomized controlled trial. Phys. Ther. 2007, 87, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Fisher, K.J.; Harmer, P.; Irbe, D.; Tearse, R.G.; Weimer, C. Tai Chi and self-rated quality of sleep and daytime sleepiness in older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2004, 52, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; Nairn, L.; Winstanley, J.; Lam, P.; Edmonds, J. Physical activity for osteoarthritis management: A randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Care Res. 2007, 57, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Jin, P. Efficacy of Tai Chi, brisk walking, meditation, and reading in reducing mental and emotional stress. J. Psychosom. Res. 1992, 36, 361–370. [Google Scholar] [CrossRef]
- Irwin, M.R.; Pike, J.L.; Cole, J.C.; Oxman, M.N. Effects of a Behavioral Intervention, Tai Chi Chih, on Varicella-Zoster Virus Specific Immunity and Health Functioning in Older Adults. Psychosom. Med. 2003, 65, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Xusheng, S.; Yugi, X.; Yunjian, X. Determination of E-rosette-forming lymphocytes in aged subjects with Taichiquan exercise. Int. J. Sport. Med. 1989, 10, 217–219. [Google Scholar] [CrossRef]
- Li, Z.; Shen, Q. The impact of the performance of Wu’s Tai Chi Chuan on the activity of natural killer cells in peripheral blood in the elderly. Chin. J. Sports Med. 1995, 14, 53–56. [Google Scholar]
- Shen, C.-L.; Williams, J.S.; Chyu, M.-C.; Paige, R.L.; Stephens, A.L.; Chauncey, K.B.; Prabhu, F.R.; Ferris, L.T.; Yeh, J.K. Comparison of the effects of Tai Chi and resistance training on bone metabolism in the elderly: A feasibility study. Am. J. Chin. Med. 2007, 35, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.; Lee, D.T.; Woo, J. Effect of Tai Chi on state self-esteem and health-related quality of life in older Chinese residential care home residents. J. Clin. Nurs. 2007, 16, 1580–1582. [Google Scholar] [CrossRef]
- Chou, K.L.; Lee, P.W.; Yu, E.C.; Macfarlane, D.; Cheng, Y.H.; Chan, S.S.; Chi, I. Effect of Tai Chi on depressive symptoms amongst Chinese older patients with depressive disorders: A randomized clinical trial. Int. J. Geriatr. Psychiatry 2004, 19, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.A.; Antonacci, D.J.; Bloch, R.M. Exercise, yoga, and meditation for depressive and anxiety disorders. Am. Fam. Physician 2010, 81, 981–986. [Google Scholar] [PubMed]
- Zhang, G. The impacts of 48-form tai chi chuan and yi qi yang fei gong on the serum levels of IgG, IgM, IgA, and IgE in human. J. Beijing Inst. Phys. Educ. 1990, 4, 12–14. [Google Scholar]
- What is Samadhi? Definition from Yogapedia. 2018. Available online: https://www.yogapedia.com/definition/4995/samadhi (accessed on 25 April 2018).
- Siegel, P.; Barros, N.F.D. Yoga as Medicine: The Yogic Prescription for Health and Healing; SciELO Public Health: São Paulo, Brazil, 2009. [Google Scholar]
- Mooventhan, A.; Khode, V. Effect of Bhramari pranayama and OM chanting on pulmonary function in healthy individuals: A prospective randomized control trial. Int. J. Yoga 2014, 7, 104. [Google Scholar]
- The Power of Breathing: 4 Pranayama Techniques Worth Practicing. 2012. Available online: https://www.onemedical.com/blog/live-well/breathing-pranayama-techniques (accessed on 25 April 2018).
- Awandare, G.A.; Goka, B.; Boeuf, P.; Tetteh, J.K.; Kurtzhals, J.A.; Behr, C.; Akanmori, B.D. Increased levels of inflammatory mediators in children with severe Plasmodium falciparum malaria with respiratory distress. J. Infect. Dis. 2006, 194, 1438–1446. [Google Scholar] [CrossRef] [Green Version]
- Kuntsevich, V.; Bushell, W.C.; Theise, N.D. Mechanisms of yogic practices in health, aging, and disease. Mt. Sinai J. Med. J. Transl. Pers. Med. 2010, 77, 559–569. [Google Scholar]
- Bushell, W.; Castle, R.; Williams, M.A.; Brouwer, K.C.; Tanzi, R.E.; Chopra, D.; Mills, P.J. Meditation and yoga practices as potential adjunctive treatment of SARS-CoV-2 infection and COVID-19: A brief overview of key subjects. J. Altern. Complement. Med. 2020, 26, 547–556. [Google Scholar] [CrossRef]
- Vijayalakshmi, P.; Surendiran, A. Effect of slow and fast pranayams on reaction time and cardiorespiratory variables. Ind. J. Physiol. Pharm. 2005, 49, 313–318. [Google Scholar]
- Kaminsky, D.A.; Guntupalli, K.K.; Lippmann, J.; Burns, S.M.; Brock, M.A.; Skelly, J.; DeSarno, M.; Pecott-Grimm, H.; Mohsin, A.; LaRock-McMahon, C. Effect of yoga breathing (pranayama) on exercise tolerance in patients with chronic obstructive pulmonary disease: A randomized, controlled trial. J. Altern. Complement. Med. 2017, 23, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Papp, M.E.; Wandell, P.; Lindfors, P.; Nygren-Bonnier, M. Effects of yogic exercises on functional capacity, lung function and quality of life in participants with obstructive pulmonary disease: A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Tillu, G.; Chaturvedi, S.; Chopra, A.; Patwardhan, B. Public health approach of ayurveda and yoga for COVID-19 prophylaxis. J. Altern. Complement. Med. 2020, 26, 360–364. [Google Scholar] [CrossRef] [Green Version]
- Morgan, N.; Irwin, M.R.; Chung, M.; Wang, C. The effects of mind-body therapies on the immune system: Meta-analysis. PLoS ONE 2014, 9, e100903. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, L.; Barrett, B.; Chase, J.; Brown, R.; Ewers, T. Self-reported mental health predicts acute respiratory infection. WMJ Off. Publ. State Med. Soc. Wis. 2015, 114, 100. [Google Scholar]
- Abel, A.N.; Lloyd, L.K.; Williams, J.S. The effects of regular yoga practice on pulmonary function in healthy individuals: A literature review. J. Altern. Complement. Med. 2013, 19, 185–190. [Google Scholar] [CrossRef]
- Cahn, B.R.; Goodman, M.S.; Peterson, C.T.; Maturi, R.; Mills, P.J. Yoga, meditation and mind-body health: Increased BDNF, cortisol awakening response, and altered inflammatory marker expression after a 3-month yoga and meditation retreat. Front. Hum. Neurosci. 2017, 11, 315. [Google Scholar] [CrossRef] [Green Version]
- Jang, J.H.; Park, H.Y.; Lee, U.S.; Lee, K.-J.; Kang, D.-H. Effects of mind-body training on cytokines and their interactions with catecholamines. Psychiatry Investig. 2017, 14, 483. [Google Scholar] [CrossRef]
- Chatterjee, S.S.; Kumar, V. Holistic psychopharmacology and promiscuous plants and principles of Ayurveda. Am. J. Plant Sci. 2012, 3, 1015–1021. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.W.; Lee, A.; Suen, L.K.; Tam, W.W. Tai chi Qigong improves lung functions and activity tolerance in COPD clients: A single blind, randomized controlled trial. Complement. Ther. Med. 2011, 19, 3–11. [Google Scholar] [CrossRef]
- Raghuraj, P.; Telles, S. Immediate effect of specific nostril manipulating yoga breathing practices on autonomic and respiratory variables. Appl. Psychophysiol. Biofeedback 2008, 33, 65–75. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. 2020. Available online: https://www.who.int/news/item/14-05-2020-substantial-investment-needed-to-avert-mental-health-crisis (accessed on 7 August 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendo, B.; Gonçalves, M.; Lopes, L.; Matos, L.C.; Machado, J. Can Yoga, Qigong, and Tai Chi Breathing Work Support the Psycho-Immune Homeostasis during and after the COVID-19 Pandemic? A Narrative Review. Healthcare 2022, 10, 1934. https://doi.org/10.3390/healthcare10101934
Mendo B, Gonçalves M, Lopes L, Matos LC, Machado J. Can Yoga, Qigong, and Tai Chi Breathing Work Support the Psycho-Immune Homeostasis during and after the COVID-19 Pandemic? A Narrative Review. Healthcare. 2022; 10(10):1934. https://doi.org/10.3390/healthcare10101934
Chicago/Turabian StyleMendo, Bruno, Mário Gonçalves, Lara Lopes, Luís Carlos Matos, and Jorge Machado. 2022. "Can Yoga, Qigong, and Tai Chi Breathing Work Support the Psycho-Immune Homeostasis during and after the COVID-19 Pandemic? A Narrative Review" Healthcare 10, no. 10: 1934. https://doi.org/10.3390/healthcare10101934
APA StyleMendo, B., Gonçalves, M., Lopes, L., Matos, L. C., & Machado, J. (2022). Can Yoga, Qigong, and Tai Chi Breathing Work Support the Psycho-Immune Homeostasis during and after the COVID-19 Pandemic? A Narrative Review. Healthcare, 10(10), 1934. https://doi.org/10.3390/healthcare10101934