
The Implementation of a Geriatrics Co-Management Model of Care Reduces Hospital Length of Stay

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Age-Friendly Hospital Principles Implantation in CTUs of Hospital Adventista Silvestre
2.2. The Geriatrics Co-Management Intervention
2.3. The Role of the Geriatric Team
2.4. Data Collection
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Creditor, M.C. Hazards of hospitalization of the elderly. Ann. Intern. Med. 1993, 118, 219–223. [Google Scholar] [CrossRef]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effects of 10 Days of Bed Rest on Skeletal Muscle in Healthy Older Adults. JAMA 2007, 297, 1769–1774. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Comprehensive geriatric assessment: From miracle to reality. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 473–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juma, S.; Taabazuing, M.M.; Montero-Odasso, M. Clinical frailty scale in an acute medicine unit: A simple tool that predicts length of stay. Can. Geriatr. J. 2016, 19, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruthappu, M.; Hasan, A.; Zeltner, T. Enablers and barriers in implementing integrated care. Health Syst. Reform. 2015, 1, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef]
- Ha, J.F.; Longnecker, N. Doctor-patient communication: A review. Ochsner J. 2010, 10, 38–43. [Google Scholar] [PubMed]
- Lai, L.; Wong, R. Leading best practice: Acute Care for Elders Units (ACE)-evidence and keys to successful operation. Can. Geriatr. J. CME 2017, 7, 1–9. [Google Scholar]
- Friedman, S.M.; Mendelson, D.A.; Kates, S.L.; McCann, R.M. Geriatric co-management of proximal femur fractures: Total quality management and protocol-driven care result in better outcomes for a frail patient population. J. Am. Geriatr. Soc. 2008, 56, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Van Grootven, B.; Flamaing, J.; Dierckx de Casterlé, B.; Dubois, C.; Fagard, K.; Herregods, M.C.; Hornikx, M.; Laenen, A.; Meuris, B.; Rex, S.; et al. Effectiveness of in-hospital geriatric co-management: A systematic review and meta-analysis. Age Ageing 2017, 46, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Raîche, M.; Hébert, R.; Dubois, M.F. PRISMA-7: A case-finding tool to identify older adults with moderate to severe disabilities. Arch. Gerontol. Geriatr. 2008, 47, 9–18. [Google Scholar] [CrossRef]
- Katz, S. Assessing Self-maintenance: Activities of Daily Living, Mobility, and Instrumental Activities. J. Am. Geriatr. Soc. 1979, 31, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Törnquist, K.; Lövgren, M.; Söderfeldt, B. Sensitivity, specificity, and predictive value in Katz’s and Barthel’s ADL indices applied on patients in long term nursing care. Scan Jour Caring Sci. 1990, 4, 99–106. [Google Scholar] [CrossRef]
- Ranhoff, A.H.; Gjoen, A.U.; Mowe, M. Screening for malnutrition in elderly acute medical patients: The usefulness of MNA-SF. J. Nutr. Health Aging. 2005, 9, 221–225. [Google Scholar]
- Cereda, E. Mini nutritional assessment. Curr. Opin. Clin. Nutr. Metab. Care. 2012, 15, 29–41. [Google Scholar] [CrossRef]
- Wei, L.A.; Fearing, M.A.; Sternberg, E.J.; Inouye, S.K. The Confusion Assessment Method: A systematic review of current usage. J. Am. Geriatr. Soc. 2008, 56, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.R.; Larente, N.; Morais, J.A. Moving towards the age-friendly hospital: A paradigm shift for the hospital-based care of the elderly. Can. Geriatr. J. 2011, 14, 100–103. [Google Scholar] [CrossRef] [Green Version]
- Cameron, I.D.; Kurrle, S. Geriatric consultation services-are wards more effective than teams? BMC Med. 2013, 11, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Dharmarajan, K.; Han, L.; Gahbauer, E.A.; Leo-Summers, L.S.; Gill, T.M. Disability and Recovery After Hospitalization for Medical Illness Among Community-Living Older Persons: A Prospective Cohort Study. J. Am. Geriatr. Soc. 2020, 68, 486–495. [Google Scholar] [CrossRef]
- Berian, J.R.; Mohanty, S.; Ko, C.Y.; Rosenthal, R.A.; Robinson, T.N. Association of loss of independence with readmission and death after discharge in older patients after surgical procedures. JAMA Surg. 2016, 151, e161689. [Google Scholar] [CrossRef] [Green Version]
- Baztán, J.J.; Suárez-García, F.M.; López-Arrieta, J.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Meta-analysis. BMJ 2009, 338, 334–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, G.; Whitehead, M.A.; Robinson, D.; O’Neill, D.; Langhorne, P. Comprehensive geriatric assessment for older adults admitted to hospital: Meta-analysis of randomised controlled trials. BMJ 2011, 343, 1034. [Google Scholar] [CrossRef]
- Van Craen, K.; Braes, T.; Wellens, N.; Denhaerynck, K.; Flamaing, J.; Moons, P.; Boonen, S.; Gosset, C.; Petermans, J.; Milisen, K. The effectiveness of inpatient geriatric evaluation and management units: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2010, 58, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Berenson, R.A.; Paulus, R.A.; Kalman, N.S. Medicare’s Readmissions-Reduction Program—A Positive Alternative. N. Engl. J. Med. 2012, 366, 1364–1366. [Google Scholar] [CrossRef]
- Gruneir, A.; Fung, K.; Fischer, H.D.; Bronskill, S.E.; Panjwani, D.; Bell, C.M.; Dhalla, I.; Rochon, P.; Anderson, G. Care setting and 30-day hospital readmissions among older adults: A population-based cohort study. CMAJ 2018, 190, E1124–E1133. [Google Scholar] [CrossRef] [Green Version]
- Dhalla, I.A.; O’Brien, T.; Morra, D.; Thorpe, K.E.; Wong, B.M.; Mehta, R.; Frost, D.W.; Abrams, H.; Ko, F.; van Rooyen, P.; et al. Effect of a postdischarge virtual ward on readmission or death for high-risk patients: A randomized clinical trial. J. Am. Med. Assoc. 2014, 312, 1305–1312. [Google Scholar] [CrossRef]
- Flood, K.L.; MacLennan, P.A.; McGrew, D.; Green, D.; Dodd, C.; Brown, C.J. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA Intern. Med. 2013, 173, 981–987. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | 2015 | 2016 | p Value |
|---|---|---|---|
| Total number of patients admitted (n) | 641 | 743 | - |
| Average number of patients admitted/month | 106.8 ± 24.8 | 123.8 ± 21.8 | 0.36 |
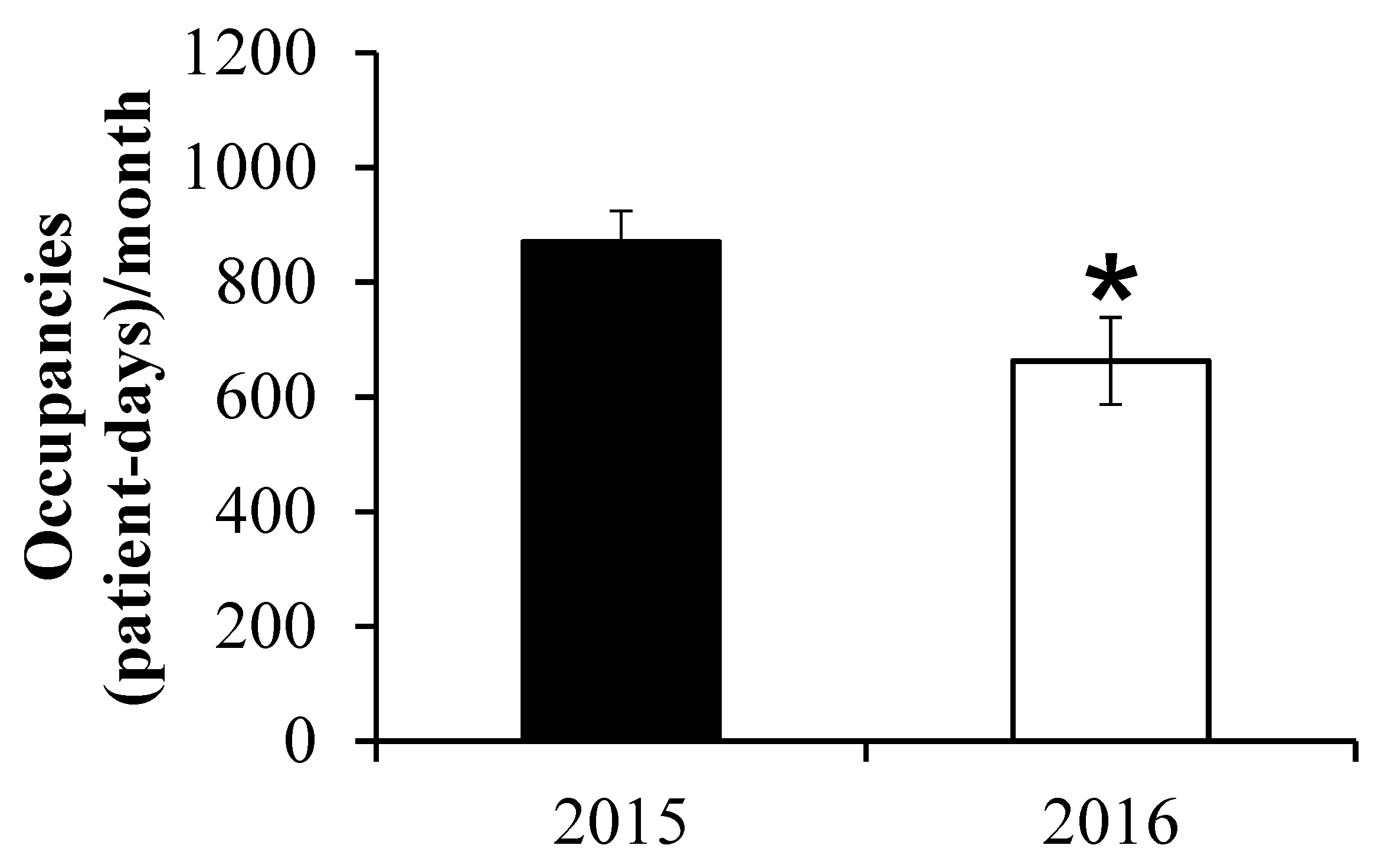
| Total number of patient days occupancy/month | 870.3 ± 132.2 | 662.8 ± 185.2 | 0.04 |
| Average length of patient-stay (days) | 8.7 ± 2.7 | 5.4 ± 1.7 | 0.03 |
| Readmission at 30 days (n) | 36 | 26 | - |
| 30-day readmission/month | 6.0 ± 3.1 | 4.3 ± 1.0 | 0.33 |
| % Readmission/month | 9.2 ± 6.8 | 4.6 ± 1.1 | 0.13 |
| Post-discharge legal cases | 4 | 1 | - |
| Total hospital costs (USD) | 2,054,140 ± 83,620 | 1,820,350 ± 119,310 | 0.52 |
| Total hospital costs/patient (USD) | 3018 ± 1363 | 2319 ± 1114 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leite, H.T.; Manhães, A.C.; Antunes, L.A.; Chan, T.; Hajj-Boutros, G.; Morais, J.A. The Implementation of a Geriatrics Co-Management Model of Care Reduces Hospital Length of Stay. Healthcare 2022, 10, 2160. https://doi.org/10.3390/healthcare10112160
Leite HT, Manhães AC, Antunes LA, Chan T, Hajj-Boutros G, Morais JA. The Implementation of a Geriatrics Co-Management Model of Care Reduces Hospital Length of Stay. Healthcare. 2022; 10(11):2160. https://doi.org/10.3390/healthcare10112160
Chicago/Turabian StyleLeite, Homero Teixeira, Alex C. Manhães, Luisa A. Antunes, Tevy Chan, Guy Hajj-Boutros, and José A. Morais. 2022. "The Implementation of a Geriatrics Co-Management Model of Care Reduces Hospital Length of Stay" Healthcare 10, no. 11: 2160. https://doi.org/10.3390/healthcare10112160
APA StyleLeite, H. T., Manhães, A. C., Antunes, L. A., Chan, T., Hajj-Boutros, G., & Morais, J. A. (2022). The Implementation of a Geriatrics Co-Management Model of Care Reduces Hospital Length of Stay. Healthcare, 10(11), 2160. https://doi.org/10.3390/healthcare10112160