
The Role of Pharmacists in Providing Pharmaceutical Care in Primary and Secondary Prevention of Stroke: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
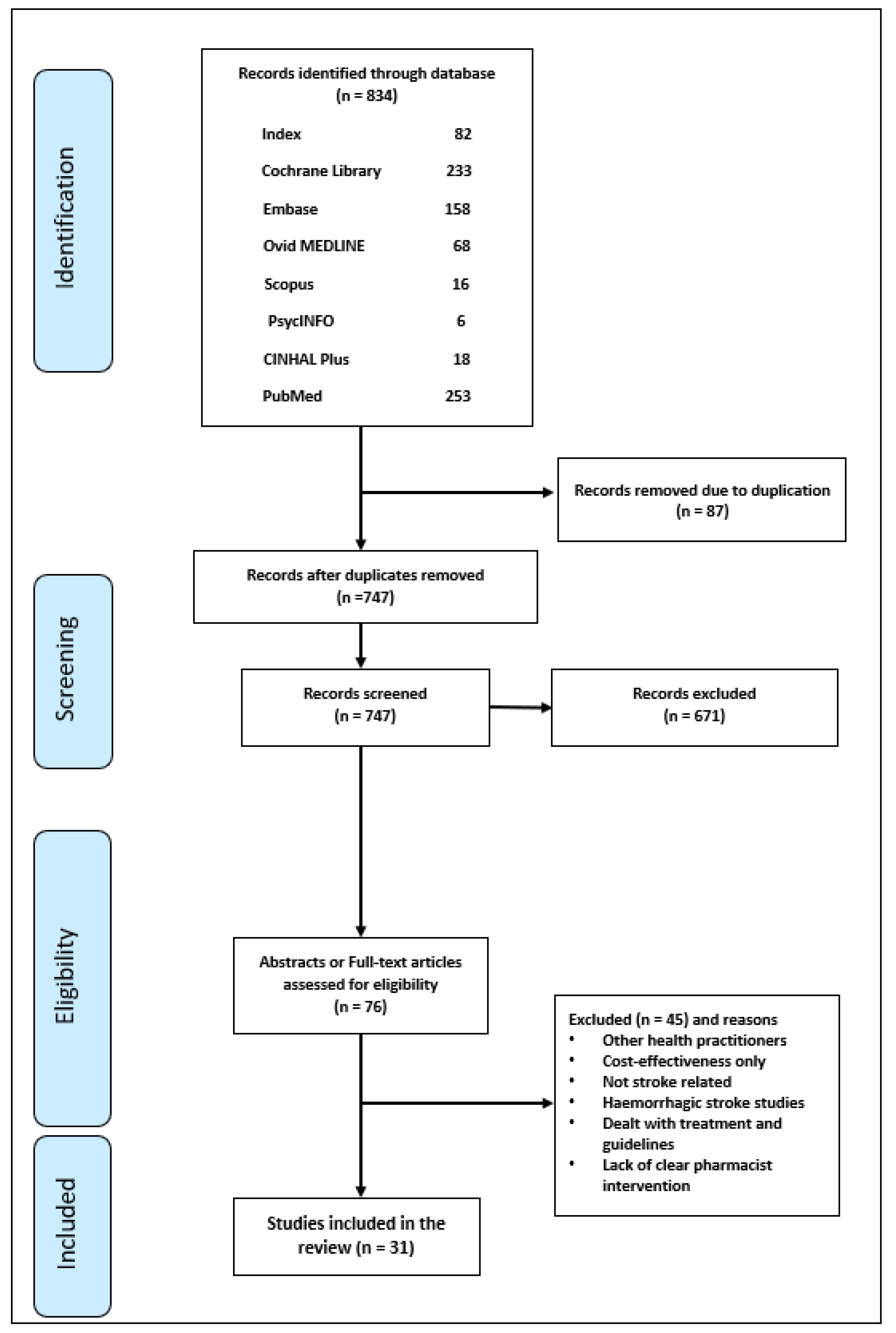
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
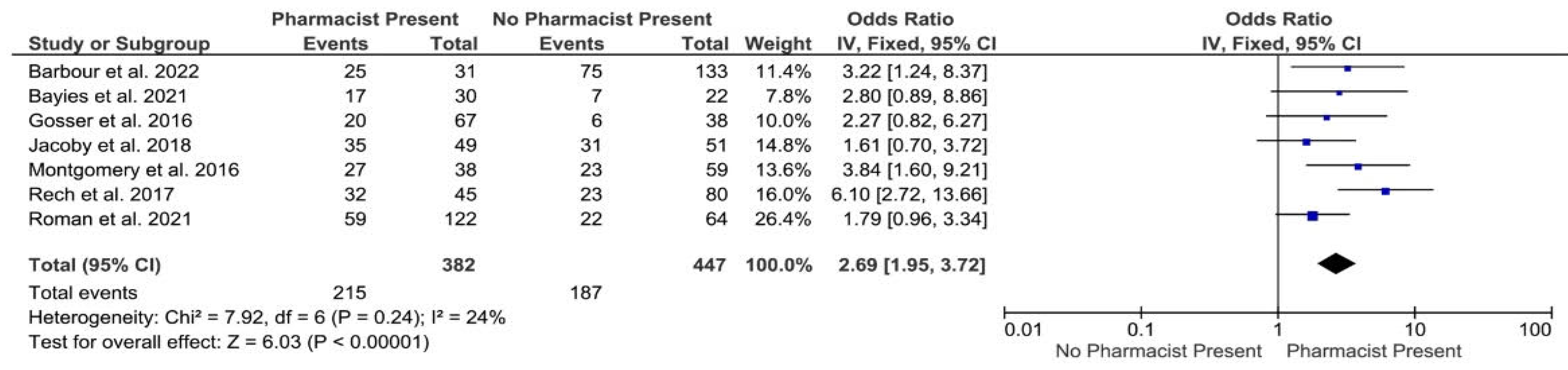
2.4. Data Analysis
2.5. Quality Assessment
3. Results

| Risk of Bias Domain | Chiu et al. [21] | Hedegaard et al. [22] | Hohmann et al. [26] | Hohmann et al. [25] | McAlister et al. [24] |
|---|---|---|---|---|---|
| Selection bias (random sequence generation) | Low | Low | Low | Low | Low |
| Selection bias (allocation concealment) | High | Low | Low | High | High |
| Reporting bias (selective reporting) | High | Low | Low | Low | Low |
| Other bias (other sources of bias) | Low | Low | Low | Low | Low |
| Performance bias—blinding (participants and personnel) | High | Low | Low | Low | Low |
| Detection bias—blinding (outcome assessment) | High | Low | Low | High | High |
| Attrition bias (Incomplete outcome data) | Low | Low | Low | Low | Low |
| Total quality assessment score for each study | 43% (Medium) | 100% (High) | 100% (High) | 71% (High) | 71% (High) |
| JBI Critical Appraisal Checklists for Cross-Sectional Studies | Hohmann et al. [34] | Lindblad and Howorko [31] | Lowres et al. [32] | Pandya et al. [35] |
|---|---|---|---|---|
| Were the criteria for inclusion in the sample clearly defined? | YES | YES | YES | YES |
| Were the study subjects and the setting described in detail? | YES | YES | YES | YES |
| Was the exposure measured in a valid and reliable way? | NC | YES | YES | NO |
| Were objective, standard criteria used for measurement of the condition? | YES | YES | YES | YES |
| Were confounding factors identified? | NO | NC | NC | NO |
| Were strategies to deal with confounding factors stated? | NO | NC | NC | NO |
| Were the outcomes measured in a valid and reliable way? | NC | NC | YES | YES |
| Was appropriate statistical analysis used? | YES | NC | YES | NO |
| Total quality assessment score for each study | 50% (Medium) | 50% (Medium) | 75% (High) | 50% (Medium) |
| JBI Critical Appraisal Checklists for Quasi-Experimental Studies | Bajorek et al. [28] | Hohmann et al. [27] | Jackson and Peterson [29] | Vo et al. [30] |
|---|---|---|---|---|
| Is it clear in the study what is the ‘cause’ and what is the ‘effect’ (i.e., there is no confusion about which variable comes first)? | YES | YES | YES | YES |
| Were the participants included in any comparisons similar? | YES | YES | NO | YES |
| Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? | YES | NO | YES | YES |
| Was there a control group? | NO | YES | NO | NO |
| Were there multiple measurements of the outcome both pre and post the intervention/exposure? | YES | YES | NO | YES |
| Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analysed? | YES | YES | YES | NO |
| Were the outcomes of participants included in any comparisons measured in the same way? | YES | YES | YES | YES |
| Were outcomes measured in a reliable way? | YES | YES | YES | YES |
| Was appropriate statistical analysis used? | YES | YES | YES | YES |
| Total quality assessment score for each study | 88.9% (High) | 88.9% (High) | 66.7% (High) | 77.8% (High) |
| JBI Critical Appraisal Checklists for Cohort Studies | Andres et al. [45] | Gosser et al. [37] | Greger et al. [49] | Lee et al. [36] | Montgomery et al. [38] | Nathans et al. [39] | Rech et al. [42] |
|---|---|---|---|---|---|---|---|
| Were the two groups similar and recruited from the same population? | YES | YES | YES | YES | YES | YES | YES |
| Were the exposures measured similarly to assign people to both exposed and unexposed groups? | YES | YES | YES | YES | YES | YES | YES |
| Was the exposure measured in a valid and reliable way? | YES | YES | YES | YES | YES | YES | YES |
| Were confounding factors identified? | NO | NO | YES | NO | NO | YES | YES |
| Were strategies to deal with confounding factors stated? | NO | NO | YES | NO | NO | YES | NO |
| Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | YES | YES | YES | YES | YES | YES | YES |
| Were the outcomes measured in a valid and reliable way? | YES | YES | YES | YES | YES | YES | YES |
| Was the follow up time reported and sufficient to be long enough for outcomes to occur? | YES | NA | YES | NC | NA | NC | YES |
| Was follow up complete, and if not, were the reasons to loss to follow up described and explored? | YES | NA | NC | NC | NA | NC | NO |
| Were strategies to address incomplete follow up utilized? | NC | NA | NO | NO | NA | NC | NO |
| Was appropriate statistical analysis used? | NO | YES | YES | YES | YES | YES | YES |
| Total quality assessment score for each study | 63.6% (Medium) | 54.5% (Medium) | 81.8% (High) | 54.5% (Medium) | 54.5% (Medium) | 72.7% (High) | 72.7% (High) |
| Author(s) and Year of Publication | Target Population | Study Aim(s) | Study Design & Setting | Description of Pharmacist/Pharmacy Student Intervention | Results/Outcomes |
|---|---|---|---|---|---|
| Bajorek et al. [28] | Patients aged ≥65 years, diagnosed with AF or at high risk of AF. | To establish, assess, and perform a multidisciplinary pharmacist-led hospital-based intervention to optimize the antithrombotic therapy in elderly patients with AF at high risk of stroke. | Before and after study conducted over 6 months in an Australian teaching hospital. | Pharmacist-led screening, interview, communication, education, consultation, risk assessment and recommendations for suitable antithrombotic therapy for AF patients based on a pre-set algorithm. | 78 of 218 patients (35.8%) required changes to their existing antithrombotic therapy. 60 of the 78 therapy changes (76.9%) were to more-effective treatment options. The proportion of patients with AF protected with antithrombotic therapy was significantly increased at discharge from (59.6% pre-intervention to 81.2% post-intervention, p < 0.001). |
| Jackson and Peterson [29] | Patients diagnosed with AF or at high risk of AF. | To implement and assess a pharmacist-led stroke risk assessment for hospital in-patients with AF. | Before and after study conducted over 17 months in an Australian hospital. | Pharmacist-led stroke risk assessment for AF patients and recommendations regarding suitable antithrombotic therapy. | 50 of 134 (37%) of patients assessed were recommended a change in therapy; 44 of these recommendations resulted in a change to antithrombotic therapy when compared to admission. 30 of the 44 therapy changes (68%) were to more effective treatment options. The use of warfarin at discharge was significantly increased compared to admission (74% pre-intervention to 98% post-intervention, p < 0.001). |
| Lee et al. [36] | Patients diagnosed with AF and initially prescribed dabigatran. | To determine if pharmacist monitoring of dabigatran therapy in the first months (3 months) of treatment in patients with AF improves adherence. | Retrospective cohort study conducted over 13 months in an American VA hospital. | Pharmacist-led adherence education about dabigatran, and follow-up telephone calls or visits. | No significant difference in adherence as measured by MPR between intervention and groups ACC (n = 20), UC (n = 48) over 3 months. Mean MPR values in (ACC pharmacist) = 93.1% and UC = 88.3%, (p = 0.16). |
| Lowres et al. [32] | Older adults, aged ≥65 years, attending (customers of) selected community pharmacies. | To find out the impact, utility and cost-effectiveness of screening in community pharmacy by using iPhone ECG technology to identify undiagnosed AF with referral to GP for management and review. The eventual aim was to reduce stroke and thromboembolism burden. | Cross sectional study conducted over 8 months in 10 Australian community pharmacies. | Pharmacist screening of medical history, pulse palpation, ECG test and interpretation with GP referral in cases of suspected AF. | 1.5% (95% CI, 0.8–2.5%) of 1000 pharmacy customers were newly detected with AF. Prevalence of AF was 6.7%. The cost-effectiveness of ICER per QALY gained and stroke prevention of screening against unscreened women and men at age 65 to 84 years was calculated. ICER for one stroke prevention was $AUD 30,481, and ICER per QALY was $AUD 5988. |
| Papastergiou [33] | Patients at risk of AF or QT-interval prolongation or a CHADS2 score of >2. | To assess iECG screening in community pharmacies for the detection of undiagnosed AF in patients at high risk. | Cross sectional study conducted in 2 Canadian community pharmacies. (Only published abstract available) | Pharmacist screening and Interpreting (iECG) reading. | 10 (28.6%) of the 35 high risk patients were found to have on abnormal rhythms and were referred to their primary care physician. |
| Virdee and Stewart [50] | Patients with AF history and not anticoagulated and with a CHA2DS2-VASc ≥1/≥2 (n = 497). | To evaluate
The role of pharmacist intervention to optimize therapy. | Clinical audit against NICE guidelines using 12 months of data from 15 UK medical practices. | Pharmacist review of patient medical records and discussion with GPs for optimisation of anticoagulant therapy. | 65.8% (n = 327) of patients were not taking anticoagulants in accordance with NICE guidelines. 77% of 382 pharmacist recommendations to optimize therapy were agreed by GPs. |
| Vo et al. [30] | General public (attendees at community health fairs) aged ≥18 years. | To assess the effect of Act FAST educational intervention carried out by pharmacy students on public alertness. | Before and after study Community health fairs held over a 10-month period in Vallejo, US. | Pharmacy student general health screening of blood glucose levels and blood pressure with a 10-min educational intervention. | The questionnaire was used to assess the knowledge of public regarding signs, symptoms, management. The scale for assessing the knowledge included low knowledge (<2), moderate knowledge (3), and high knowledge (≥4). The scale for assessing the knowledge regarding the risk factors of stroke included low knowledge (≤4), moderate knowledge (6–8), and high knowledge (9). The scores were measured in both scales by summing the correct answers out of 6 and 9 total potential correct response. Participant knowledge of the signs, symptoms, risk factors and management of stroke improved significantly post-intervention (p < 0.0001). |
| Author(s) and Year of Publication | Target Population | Study Aim(s) | Study Design & Setting | Description of Pharmacist Intervention | Results/Outcomes |
|---|---|---|---|---|---|
| Barbour et al. [46] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke at ED. | To assess the impact of pharmacist presence on DTN times and patient outcomes. | Retrospective cohort study conducted in a US stroke centre with data collection covering a period of 3 years and 10 months. | Addition of a pharmacist to the ‘stroke response team’ with responsibility for thrombolytic (rtPA) contraindications, screening dose calculation and preparation. | 164 patient records were included with 31 allocated to the pharmacist present group and 133 to the pharmacist absent group. Median Door-to-needle (rtPA) times:
|
| Bayies et al. [47] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke at ED. | To assess the impact of pharmacist presence on DTN times. | Retrospective cohort study conducted in a US stroke centre with data collection covering a period of 1 year and 6 months. (Only published abstract available) | NA | Median Door-to-needle (rtPA) times:
|
| Brandon et al. [41] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke at ED. | To improve the process for thrombolytic dose calculation and preparation to reduce administration times. Establish zero min decision to needle time goal in addition of pharmacist to stroke team. | A cohort study conducted in unnamed US hospital(s) with a retrospective chart review and prospective data collection post intervention. (Only published abstract available) | Addition of a pharmacist to the ‘code stroke team’ with responsibility for thrombolytic (rtPA) dose calculation and preparation plus patient/carer counselling and education. | Improved decision to needle times reported. In the year prior to the intervention, the target zero-minute decision to needle time was not achieved (no case numbers reported). Post intervention zero-minute decision to needle time targets were achieved in 60% of administrations and 78% of administrations in the subsequent two years (no case numbers or actual times reported). |
| Gosser et al. [37] | Patients aged ≥18 years who received thrombolytic (rtPA) for acute ischaemic stroke. | To examine the impact of pharmacist involvement on rtPA dosing accuracy and door-to-needle time. | Retrospective cohort study conducted in a US stroke centre with data collection covering a period of 4 years and 9 months. Participants were assigned to a pharmacist present or pharmacist absent group for analysis. | Pharmacist involvement included documentation in notes, order entry and/or dispensing. | 105 patient records were included with 67 allocated to the pharmacist present group and 38 to the pharmacist absent group. Dosing accuracy: Pharmacist present 96.6% vs. pharmacist absent 95.6% (p = 0.8953). Door-to-needle (rtPA) times:
|
| Hosoya et al. [48] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke at ED. | To evaluate the pharmacists’ role on rtPA therapy for acute ischaemic stroke patients. | Retrospective cohort study conducted in a Japanese hospital with data collection covering a period of 4 years. | Investigating medications administration and patient allergies information through patient notebook and patient family and rtPA preparation. | Median Door-to-needle (rtPA) times:
|
| Jacoby et al. [43] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke at ED. | To assess the impact of pharmacist presence on DTN times and patient outcomes. | Retrospective cohort study conducted in a US stroke centre with data collection covering a period of 2 years and 1 month. | Interview patients and their family and review medication history, manage patient’s blood glucose and pressure, verifying INR for patients on warfarin, calculate rtPA dose, prepare and administer rtPA. | 100 patient records were included with 49 allocated to the pharmacist present group and 51 to the pharmacist absent group. Median Door-to-needle (rtPA) times:
|
| Montgomery et al. [38] | Patients who received thrombolytic (drug unspecified) for treatment of acute ischaemic stroke. | To assess the impact of ED pharmacists on thrombolytic administration times. | Retrospective cohort study conducted in a US Hospital with data collection covering a period of 2 years and 9 months. Participants were assigned to a pharmacist present or pharmacist absent group for analysis. | Reviewing contraindications and co-ordinating administration of thrombolytics including dosing and reconstitution. | 97 patient records were included with 38 allocated to the pharmacist present group and 59 to the pharmacist absent group. Door-to-needle times:
|
| Pandya et al. [35] | Patients who received thrombolytic (rtPA) for treatment of acute ischaemic stroke. | To evaluate and define the pharmacist role on stroke response. | Retrospective cross-sectional study of pharmacy resident stroke team pages/calls conducted in a US hospital with data collection covering a period of 12 months. | To respond to emergency stroke team calls and ensure compliance with a site-specific ischaemic stroke acute treatment protocol for blood pressure management, thrombolytic dosing, preparation, and monitoring. Provided as part of an on-call residency; also drug information and clinical pharmacokinetics services. | Of 256 stroke team calls, 46 patients received thrombolytic (rtPA). Of these, thrombolytic had been administered external to the study hospital in 22 cases. For the 24 cases treated at the study hospital there were no deviations from protocol meaning all patients were given thrombolytic within 3 h of symptom onset and there was no thrombolytic drug waste. No door to needle times reported. Three medication errors (including one thrombolytic dosing error) were identified in patients administered thrombolytic external to the study hospital. |
| Rech et al. [42] | Patients aged ≥18 years who received thrombolytic (rtPA) for acute ischaemic stroke in 4.5 h of stroke symptom onset. | To determine whether pharmacist intervention at bedside in acute ischaemic stroke can reduce door to needle times for thrombolytic treatment. | Retrospective Cohort study conducted in a US Hospital with data collection covering a period of 4 years. Participants were assigned to a pharmacist present or pharmacist absent group for analysis. | Evaluate rtPA contraindications, elicit and review medical and medication histories, manage blood pressure. Calculate rtPA dose, prepare and administer rtPA and monitor after administration. Counsel patients and/or carers. | 125 patient records were included with 45 allocated to the pharmacist present group and 80 to the pharmacist absent group. Door-to-needle (rtPA) times:
|
| Roman et al. [44] | Stroke patients who received rtPA. | To assess the impact of EM pharmacists on thrombolytic administration times. | Pre/post-implementation cohort study conducted at an Australian hospital with data collection retrospectively and prospectively covering a pre period of 2 years and 7 months and post period of 3 years and 11 years. | Elicit and review medication history, manage acute blood pressure, calculate rtPA dose, prepare and administer rtPA and monitor after administration. | Door-to-needle (rtPA) times:
|
| Tsai et al. [40] | Patients who received thrombolytic (drug unspecified) for treatment of acute ischaemic stroke. | To evaluate the quality of patient care and cost avoidance when pharmacists are involved in a multidisciplinary ischaemic stroke team. | Retrospective cohort study conducted in a Taiwan hospital with data collection covering a period of 1 year and 10 months pre- and post-intervention. (Only published abstract available) | Pharmacist participation in medical rounds. | 648 patient records were examined. The number of records pre and post intervention were not reported. Pharmaceutical care quality measured against five measures as set out by the American Heart Association and American Stroke Association Get with the Guidelines—Stroke Program.
|
| Author(s) and Year of Publication | Target Population | Study Aim(s) | Study Design & Setting | Description of Pharmacist/Pharmacy Student Intervention | Results/Outcomes |
|---|---|---|---|---|---|
| Andres et al. [45] | Patients with a stroke or TIA (n = 455) | To determine if patients receiving care from the SPC have better outcomes than patients who received UC. To evaluate the total change in BP, LDL, and HbA1c from the time of stroke/TIA to most recent value post SPC intervention. | Retrospective cohort study conducted in a US Hospital over 4 months. | Pharmacotherapy intervention: medication review and education. | The composite end point of hospital readmissions for stroke/TIA, MI, or new or incidental PAD in the SPC group (n = 257) attained. Statistical significance (p = 0.013) when compared to the control group (n = 198). Patients who visited the SPC had 4% fewer hospital admissions for stroke/TIA (p = 0.125). All surrogate markers, including blood pressure, Low Density Lipoprotein, Haemoglobin A1c, and smoking status, improved in the SPC group. |
| Chiu et al. [21] | Patients with ischemic stroke outpatients who visited clinics regularly after stroke for more than 12 months. (n = 160) | To assess the management of modifiable risk factors (MRF) adequacy in IS outpatients’ group. To evaluate the importance of pharmacist intervention in a randomized controlled study in hospital. | Randomized controlled study (RCT) conducted in a Taiwan hospital, over 6 months. | Educational intervention programme over 6 months regarding side effects, drug interactions, identifying and solving DRPs, and a medication review. | Differences in lipid profiles, blood glucose, and blood pressure before and after the study. BP control change Intervention 83% Control 43% (p = 0.00) Lipid normal level Intervention 40% Control 27% (p = 0.16) Glucose control Intervention 35% Control 46%. (p= 0.40) |
| Greger et al. [49] | Post-stroke or post-TIA patients. (n = 342) | To determine pharmacist interventions along with anti-platelet medication monitoring when compared to usual care. | Retrospective matched (n = 171 for each group) cohort study conducted in a US single centre, outpatient neurology practice. | Medication review, reconciliation, adherence counselling, and risk factors modifications. | Responsiveness to antiplatelet medication after Pharmacist interventions. Patients’ responsiveness was 83% at pharmacist intervention group (p < 0.0001) Selected interventions frequency in pharmacist group compared to usual care group. Drug-drug interactions (p < 0.0001) and counselling on adherence (p < 0.0008) were identified in pharmacist group compared to usual care. |
| Hedegaard et al. [22] | Patients with acute first-time ischaemic stroke, aged ≥18 years and in an emergency ward or neurology department. (n = 200) | To assess the multifaceted pharmacist intervention in improving medication adherence for secondary stroke prevention. | Randomized controlled study (RCT) conducted in a Denmark hospital over 6 months. | Medication review, an interview, consultation, and three follow-ups via telephone calls. | MPR of antiplatelets, anticoagulants, and statin one year after discharge. Median MPRs after 12 months MMPRs (IQR) were 0.95 (0.77–1) in the intervention group and 0.91 (0.83–0.99) in the control group. MPR reduction (3 to 12 months). 5% and 9% in the intervention and control groups, respectively (p < 0.05). |
| Hohmann et al. [26] | Patients diagnosed with TIA or ischemic stroke. (n = 255) | To assess if the pharmaceutical care increases the patient’s health related quality of life (HQL). | A cluster cohort study conducted in a German rehabilitation hospital and community pharmacies over 12 months. | Counselling interview about medications, mainly secondary preventions regarding side effects, drug interactions, DRP identification and resolution, and a review of medication. | Patient’s HRQoL Significant decrease observed in 7/8 subscales at CG. Vitality subscale was significantly decreased in CG than IG (p = 0.027) Secondary prevention 85.3% (IG) and 86.3% (CG) of patients were prescribed with antiplatelet and oral anticoagulant medications accordant with DGN and DSG guidelines. Patients’ satisfaction with pharmacist interventions IG was more satisfied with pharmacist interventions compared to CG (p < 0.016). |
| Hohmann et al. [25] | Patients with TIA or ischemic stroke with a Barthel index of over 30 points at discharge time. (n = 255) | To assess the impact of of pharmaceutical care on HRQoL by using a SF-36. | A cluster cohort study conducted in a German rehabilitation hospital and community pharmacies, over 12 months. | Counselling, medication review, and interviews regarding secondary preventive medications. | HRQoL VT subscale was significantly decreased in CG than IG (p = 0.027) Bodily pain significantly dropped in IG (p = 0.0001) A significant decrease between the PCS and MCS in CG (PCS: p = 0.023; MCS: p = 0.001) No statistically significant between the PCS and MCS in IG. A significant drop in the HRQoL was noticed in 7/8 (RP, BP, GH, VT, SF, RE, and MH) subscales in CG (p < 0.05; p < 0.01; p < 0.001). |
| Hohmann et al. [34] | Patients with TIA or IS aged ≥18 years and were taking two or more medications during admission and discharge. (n = 156) | To explore the frequency and type of DRPs over the pharmaceutical interventions to detect them with TIA patients or IS from admission to discharge from hospital. | A cross sectional study conducted in a German hospital, over 6 months. | Medication reconciliation on admission and at discharge, providing information about medication modifications during the period of hospital admission, and reasons for antithrombotic therapy changes, ward rounds participation and detecting DRP. | Percentage of patients who had a DRA 271 DRPs happened in 105 out of 155 (67.7%) patients. Percentage of physician’s acceptance for pharmacist interventions 89% of pharmacist interventions were accepted by GPs. |
| Hohmann et al. [27] | Patients with TIA or IS aged ≥18 years and were taking two or more medications during admission and at discharge. (n = 312) | To evaluate the adherence of primary care clinicians to prescribing the medication regimes started at the time of in-hospital stroke treatment following pharmacist intervention to improve discharge letter communication. | Non-randomized trial conducted in a German hospital over 6 months. | Listing the drugs at admission and discharge in the discharge letter, 3 follow-up calls, providing information in details about the change of drugs during hospital admission, modifications of drugs. | Overall adherence to pharmacist recommendations by PCPs IG + 7.6% (90.9% for IG—83.3% for CG) (p = 0.01) Antithrombotic drugs adherence to pharmacist recommendations by PCPs IG + 8.1% (91.9% for IG—83.3% for CG) (p = 0.033) Statin adherence to pharmacist recommendations by PCPs IG + 17.9% (87.7% for IG—69.8% for CG) (p < 0.001). |
| Khalil et al. [51] | Patients who diagnosed with IS, and aged ≥18 years. (n = 124) | To examine the management of pharmacological treatment of stroke patients and measure the adherence to stroke management guidelines with and without pharmacist intervention. | Retrospective audit conducted in an Australian hospital, over 5 months. | Medication reconciliation and review. | Percentage of discharged patients on antihypertensive, lipid lowering medications, and antithrombotic. Antihypertensive prescribed for secondary prevention: 83% of patients who were reviewed by pharmacists 59% patients who were not seen by pharmacists (p = 0.005). Lipid lowering agents: 68% of patients who were reviewed by pharmacists 66% patients who were seen by pharmacists. (p = 0.849). Antithrombotic agents: 92% of patients who were reviewed by pharmacists 77% patients who were not seen by pharmacists. (p = 0.025). |
| Lindblad and Howorko [31] | Patients who were recruited with TIA or IS at discharge and with outpatients. | To identify the number and type of pharmacist interventions. | Cross sectional study conducted in a Canadian hospital over 6 months. | Medication counselling, a review of medical records, followed-up calls and medication reconciliation. | Average number of interventions per patient encounter. 2.8 interventions per encounter. Average number of patient outcomes associated with pharmacist’s interventions. 1.9 outcomes per intervention. Proportion of accepted and rejected pharmacist interventions by prescriber. Accepted 63.9% |
| McAlister et al. [24] | Patients diagnosed with confirmed TIA or IS and who had hypertension and dyslipidaemia. (n = 275) | To assess the impact of two types of case management (pharmacist-led and nurse-led groups) on global risk of vascular. | Randomized controlled study (RCT) conducted in Canada community-dwelling adults, over 6 and 12 months. | Providing lifestyle advice, initiating, and adjusting antihypertensive and lipid-lowering therapy, and discussing risk factor assessments with primary care physicians. | FRS estimated 10-year risk At 6 months: median 4.8% (IQR 0.3–11.3%) for the pharmacist arm vs. 5.1% (IQR 1.9–12.5%) for the nurse arm (p = 0.44). At 12 months: median 6.4% (1.2–11.6%) vs. 5.5% (2.0–12.0%) (p = 0.83). CDLEM estimated 10-year risk At 6 months: median 10.0% (0.1–31.6%) vs. 12.5% (2.1–30.5%) (p = 0.37). At 12 months: median 8.4% (0.1–28.3%) vs. 13.1% (1.6–31.6%) (p= 0.20). Percentage of participants at six months who obtained normal BP (SBP ≤ 40 mm and fasting LDL ≤ 2.0 mm). Pharmacist arm 53.1% vs. nurse arm 31.3% achieved the goals of controlling (SBP) and (LDL) (p = 0.005). |
| Nathans et al. [39] | Patients with a stroke or TIA (n = 94) | To determine the effect of a pharmacist TOC on hospital readmissions, ED visits, and recurrent events. | Retrospective matched cohort Study conducted in a US university hospital over 18 months. | Adjustment of the medication dose. Therapy addition or discontinuation. Monitoring and requesting laboratory tests. Counselling. | Primary endpoint was 30-day hospital readmissions rate. No significant difference was found in 30-day readmissions. (p = 0.12). Secondary endpoints included 90-day readmissions, 30 and 90-day emergency department visits, and recurrent stroke rates. Significant difference found in 90-day readmissions (5.3% vs. 21.3%). (p = 0.001). |
| Nguyen et al. [23] | Patients with stroke history. (n = 30) | To assess whether a clinical pharmacist intervention could improve adherence to stroke medications and achieve prevention of stroke goals. | Randomized controlled study (RCT) conducted in a US hospital over 6 months. (Only published abstract available) | Telephone follow-up calls at 3 and 6 months which include medication adherence evaluation, stroke education, stroke prevention goals reassessment. | Medication Adherence. Pharmacists’ intervention group 56% vs. Usual care group 36% Adherence to antithrombotic only (73% vs. 57%). Achieving the stroke prevention goals. BP (73% vs. 57%) LDL-C goals (75% vs. 50%) Blood glucose control (75% vs. 50%). |
3.1. Primary Prevention Interventions
3.2. Secondary Prevention Interventions
3.2.1. Emergency and Acute Care Interventions
3.2.2. Long-Term Care Interventions
3.3. Common Outcome Measures across All Interventions
3.3.1. Medicines Adherence
3.3.2. Medicines Optimisation
Medicines Optimisation for Primary Prevention of Stroke
Medicines Optimisation for Secondary Prevention of Stroke
3.3.3. Modification of Clinical Risk Factors
Blood Pressure
Lipid and Blood Glucose Control
3.3.4. Clinical Outcomes
3.3.5. Patient Outcomes
4. Discussion
4.1. Primary Prevention
4.2. Secondary Prevention Emergency Treatment
4.3. Secondary Prevention Long-Term Management
4.4. Common Findings for Both Primary and Secondary Prevention of Stroke
5. Limitations of the Review
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rajsic, S.; Gothe, H.; Borba, H.H.; Sroczynski, G.; Vujicic, J.; Toell, T.; Siebert, U. Economic burden of stroke: A systematic review on post-stroke care. Eur. J. Health Econ. 2019, 20, 107–134. [Google Scholar] [CrossRef] [PubMed]
- Avan, A.; Digaleh, H.; Di Napoli, M.; Stranges, S.; Behrouz, R.; Shojaeianbabaei, G.; Amiri, A.; Tabrizi, R.; Mokhber, N.; Spence, J.D.; et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden: An ecological analysis from the Global Burden of Disease Study 2017. BMC Med. 2019, 17, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, K.M.; Wolfe, C.D.; Rudd, A.G.; Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Grieve, A.P. Risk and cumulative risk of stroke recurrence: A systematic review and meta-analysis. Stroke 2011, 42, 1489–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakhan, S.E.; Sapko, M.T. Blood pressure lowering treatment for preventing stroke recurrence: A systematic review and meta-analysis. Int. Arch. Med. 2009, 2, 30. [Google Scholar] [CrossRef] [Green Version]
- Chróinín, D.N.; Asplund, K.; Åsberg, S.; Callaly, E.; Cuadrado-Godia, E.; Díez-Tejedor, E.; Di Napoli, M.; Engelter, S.T.; Furie, K.L.; Giannopoulos, S.; et al. Statin therapy and outcome after ischemic stroke: Systematic review and meta-analysis of observational studies and randomized trials. Stroke 2013, 44, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Antithrombotic, T.C. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002, 324, 71–86. [Google Scholar]
- Lyons, R.; Rudd, A.G. Health Policy and Outcomes 2006. Stroke 2007, 38, 229–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awada, A. Primary and secondary prevention of ischemic stroke. J. Med. Liban. Leban. Med. J. 2011, 59, 213–219. [Google Scholar]
- Murray, R. Community Pharmacy Clinical Services Review; NHS England: London, UK, 2016; Volume 16.
- Kislan, M.M.; Bernstein, A.T.; Fearrington, L.R.; Ives, T.J. Advanced Practice Pharmacists: A retrospective evaluation of the efficacy and cost of ClinicaL Pharmacist PractitionErs managing ambulatory Medicare patients in North Carolina (APPLE-NC). BMC Health Serv. Res. 2016, 16, 607, Erratum in BMC Health Serv. Res. 2016, 16, 673. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.D.; Tran, V.; Chan, C.; Mitchell, W.M.; Atayee, R.S. Retrospective analysis of pharmacist interventions in an ambulatory palliative care practice. J. Oncol. Pharm. Pract. 2016, 22, 757–765. [Google Scholar] [CrossRef]
- Rudd, K.M.; Dier, J.G. Comparison of Two Different Models of Anticoagulation Management Services with Usual Medical Care. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2010, 30, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.; Jett, B.P.; Cradick, M.; Zuber, J. Effect of Clinical Pharmacist Intervention on Hemoglobin A1C Reduction in Veteran Patients with Type 2 Diabetes in a Rural Setting. Ann. Pharmacother. 2016, 50, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.G.; Park, I.; Sutherland, S.E.; Ray, L. Assessing pharmacist-led annual wellness visits: Interventions made and patient and physician satisfaction. J. Am. Pharm. Assoc. 2015, 55, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felling, R.J.; Sun, L.R.; Maxwell, E.C.; Goldenberg, N.; Bernard, T. Pediatric arterial ischemic stroke: Epidemiology, risk factors, and management. Blood Cells Mol. Dis. 2017, 67, 23–33. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Miami, FL, USA, 2020; Available online: https://synthesismanual.jbi.global (accessed on 10 November 2020).
- Van Eikenhorst, L.; Salema, N.-E.; Anderson, C. A systematic review in select countries of the role of the pharmacist in consultations and sales of non-prescription medicines in community pharmacy. Res. Soc. Adm. Pharm. 2017, 13, 17–38. [Google Scholar] [CrossRef]
- Chiu, C.-C.; Wu, S.-S.; Lee, P.-Y.; Huang, Y.-C.; Tan, T.-Y.; Chang, K.-C. Control of modifiable risk factors in ischemic stroke outpatients by pharmacist intervention: An equal allocation stratified randomized study. J. Clin. Pharm. Ther. 2008, 33, 529–535. [Google Scholar] [CrossRef]
- Hedegaard, U.; Kjeldsen, L.J.; Pottegård, A.; Bak, S.; Hallas, J. Multifaceted Intervention Including Motivational Interviewing to Support Medication Adherence after Stroke/Transient Ischemic Attack: A Randomized Trial. Cerebrovasc. Dis. Extra 2014, 4, 221–234. [Google Scholar] [CrossRef]
- Nguyen, V.-H.V.; Poon, J.; Tokuda, L.; Sayers, J.; Wallis, R.-A.; Dergalust, S. (Eds.) Pharmacist Telephone Interventions Improve Adherence to Stroke Preventive Medications and Reduce Stroke Risk Factors: A Randomized Controlled Trial; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- McAlister, F.A.; Grover, S.; Padwal, R.S.; Youngson, E.; Fradette, M.; Thompson, A.; Buck, B.; Dean, N.; Tsuyuki, R.T.; Shuaib, A.; et al. Case management reduces global vascular risk after stroke: Secondary results from the The preventing recurrent vascular events and neurological worsening through intensive organized case-management randomized controlled trial. Am. Heart J. 2014, 168, 924–930. [Google Scholar] [CrossRef]
- Hohmann, C.; Radziwill, R.; Klotz, J.M.; Jacobs, A.H. Health-Related Quality of Life after Ischemic Stroke: The Impact of Pharmaceutical Interventions on Drug Therapy (Pharmaceutical Care Concept). Health Qual. Life Outcomes 2010, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Hohmann, C.; Klotz, J.M.; Radziwill, R.; Jacobs, A.H.; Kissel, T. Pharmaceutical care for patients with ischemic stroke: Improving the patients quality of life. Pharm. Weekbl. Sci. Ed. 2009, 31, 550–558. [Google Scholar] [CrossRef]
- Hohmann, C.; Neumann-Haefelin, T.; Klotz, J.M.; Freidank, A.; Radziwill, R. Adherence to hospital discharge medication in patients with ischemic stroke: A prospective, interventional 2-phase study. Stroke 2013, 44, 522–524. [Google Scholar] [CrossRef] [Green Version]
- Bajorek, B.V.; Krass, I.; Ogle, S.J.; Duguid, M.J.; Shenfield, G.M. Optimizing the Use of Antithrombotic Therapy for Atrial Fibrillation in Older People: A Pharmacist-Led Multidisciplinary Intervention. J. Am. Geriatr. Soc. 2005, 53, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.L.; Peterson, G.M. Stroke risk assessment for atrial fibrillation: Hospital-based stroke risk assessment and intervention program. J. Clin. Pharm. Ther. 2011, 36, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Vo, L.P.; Souksavong, J.H.; Tran, A.; Chang, J.; Lor, K.B. Impact of the Act FAST stroke campaign delivered by student pharmacists on the primary prevention of stroke. J. Am. Pharm. Assoc. 2017, 57, 326-332.e6. [Google Scholar]
- Lindblad, A.J.; Howorko, J. Integration of a Pharmacist into a Stroke Prevention Clinic Team. Can. J. Hosp. Pharm. 2008, 61, 431–463. [Google Scholar] [CrossRef]
- Lowres, N.; Neubeck, L.; Salkeld, G.; Krass, I.; McLachlan, A.J.; Redfern, J.; Bennett, A.A.; Briffa, T.; Bauman, A.; Martinez, C.; et al. Feasibility and cost-effectiveness of stroke prevention through community screening for atrial fibrillation using iPhone ECG in pharmacies. Thromb. Haemost. 2014, 111, 1167–1176. [Google Scholar] [CrossRef]
- Papastergiou, J. Pharmacy Practice Research Abstracts. Can. Pharm. J. Rev. Pharm. Can. 2016, 149, S1–S46. [Google Scholar]
- Hohmann, C.; Neumann-Haefelin, T.; Klotz, J.M.; Freidank, A.; Radziwill, R. Drug-related problems in patients with ischemic stroke in hospital. Int. J. Clin. Pharm. 2012, 34, 828–831. [Google Scholar] [CrossRef]
- Pandya, K.A.; Ruf, K.M.; Winstead, P.S.; Cook, A.; Weant, K. Pharmacy resident participation with a 24-hour multidisciplinary stroke response team. Am. J. Health Pharm. 2010, 67, 1901–1907. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.-Y.; Han, S.Y.; Miyahara, R.K. Adherence and outcomes of patients treated with dabigatran: Pharmacist-managed anticoagulation clinic versus usual care. Am. J. Health Pharm. 2013, 70, 1154–1161. [Google Scholar] [CrossRef]
- Gosser, R.A.; Arndt, R.F.; Schaafsma, K.; Dang, C.H. Pharmacist Impact on Ischemic Stroke Care in the Emergency Department. J. Emerg. Med. 2015, 50, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, K.; Hall, A.B.; Keriazes, G. Impact of an emergency medicine pharmacist on time to thrombolysis in acute ischemic stroke. Am. J. Emerg. Med. 2016, 34, 1997–1999. [Google Scholar] [CrossRef] [PubMed]
- Nathans, A.M.; Bhole, R.; Finch, C.K.; George, C.M.; Alexandrov, A.V.; March, K.L. Impact of a Pharmacist-Driven Poststroke Transitions of Care Clinic on 30 and 90-Day Hospital Readmission Rates. J. Stroke Cerebrovasc. Dis. 2020, 29, 104648. [Google Scholar] [CrossRef]
- Tsai, Y.J.; Leu, W.J.; Lin, Y.M.; Lu, T.H. PCV22 Pharmacist’s Involvement in a Multidisciplinary Ischemic Stroke Team in and its Associated Cost Avoidance. Value Health 2012, 15, A632. [Google Scholar] [CrossRef] [Green Version]
- Brandon, K.; Kramer, A.; Mulawka, C. Abstract WP343: Role of the Clinical Pharmacist in Reducing Decision-to-Needle tPa Times during Code Stroke in the Emergency Department. Stroke 2013, 44, AWP343. [Google Scholar] [CrossRef]
- Rech, M.A.; Bennett, S.; Donahey, E. Pharmacist Participation in Acute Ischemic Stroke Decreases Door-to-Needle Time to Recombinant Tissue Plasminogen Activator. Ann. Pharmacother. 2017, 51, 1084–1089. [Google Scholar] [CrossRef]
- Jacoby, J.S.; Draper, H.M.; Dumkow, L.E.; Farooq, M.U.; Deyoung, G.R.; Brandt, K.L. Emergency Medicine Pharmacist Impact on Door-to-Needle Time in Patients with Acute Ischemic Stroke. Neurohospitalist 2017, 8, 60–65. [Google Scholar] [CrossRef]
- Roman, C.; Cloud, G.; Dooley, M.; Mitra, B. Involvement of emergency medicine pharmacists in stroke thrombolysis: A cohort study. J. Clin. Pharm. Ther. 2021, 46, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Andres, J.; Stanton-Ameisen, O.; Walton, S.; Ruchalski, C. Pharmacists’ Impact on Secondary Stroke Prevention. J. Pharm. Pract. 2018, 32, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.; Hushen, P.; Newman, G.C.; Vidal, J. Impact of an emergency medicine pharmacist on door to needle alteplase time and patient outcomes in acute ischemic stroke. Am. J. Emerg. Med. 2021, 51, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Bayies, A.L.; Kiley, A.; Eng, C.C. Abstract P29: Improving Door to Needle Alteplase Times: Pharmacist Involvement during Code Stroke. Stroke 2021, 52 (Suppl. S1), AP29-AP. [Google Scholar] [CrossRef]
- Hosoya, R.; Ichijo, M.; Shima, S.; Miyamae, R.; Kamata, T.; Hino, S. Pharmacists’ impact on door-to-rtPA time in patient with acute ischemic stroke. J. Jpn. Soc. Emerg. Med. 2020, 23, 600–607. [Google Scholar]
- Greger, J.; Wojcik, R.; Westphal, E.; Aladeen, T.; Landolf, K.; Boyce, S.; Rainka, M.; Gengo, F.; Bates, V. Pharmacist intervention and anti-platelet medication monitoring in patients following stroke and transient ischemic attack. JACCP J. Am. Coll. Clin. Pharm. 2020, 4, 311–317. [Google Scholar] [CrossRef]
- Virdee, M.S.; Stewart, D. Optimizing the use of oral anticoagulant therapy for atrial fibrilation in primary care: A pharmacist-led intervention. Int. J. Clin. Pharm. 2017, 39, 173–180. [Google Scholar] [CrossRef]
- Khalil, V.; Li, M.; Hua, Q.A. An audit of the pharmacological management of ischaemic stroke patients in a metropolitan Australian hospital. Int. J. Clin. Pharm. 2014, 37, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Lees, K.R.; Bluhmki, E.; von Kummer, R.; Brott, T.G.; Toni, D.; Grotta, J.C.; Albers, G.W.; Kaste, M.; Marler, J.R.; Hamilton, S.A.; et al. Time to treatment with intravenous alteplase and outcome in stroke: An updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010, 375, 1695–1703. [Google Scholar] [CrossRef]
- Strbian, D.; Soinne, L.; Sairanen, T.; Häppölä, O.; Lindsberg, P.J.; Tatlisumak, T.; Kaste, M. Ultra-early thrombolysis in acute ischemic stroke is associated with better outcome and lower mortality. Stroke 2010, 41, 712–716. [Google Scholar] [CrossRef] [Green Version]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Almekhlafi, M.; Dippel, D.W.; Campbell, B.C.V.; Muir, K.; Demchuk, A.M.; Bracard, S.; Davalos, A.; Guillemin, F.; Jovin, T.G.; et al. Rapid alteplase administration improves functional outcomes in patients with stroke due to large vessel occlusions: Meta-analysis of the noninterventional arm from the HERMES collaboration. Stroke 2019, 50, 645–651. [Google Scholar] [CrossRef] [Green Version]
- Atlantis, T. Association of outcome with early stroke treatment: Pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004, 363, 768–774. [Google Scholar]
- Lees, K.R.; Emberson, J.; Blackwell, L.; Bluhmki, E.; Davis, S.M.; Donnan, G.A.; Grotta, J.C.; Kaste, M.; von Kummer, R.; Lansberg, M.G.; et al. Effects of alteplase for acute stroke on the distribution of functional outcomes: A pooled analysis of 9 trials. Stroke 2016, 47, 2373–2379. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Smith, E.E.; Saver, J.L.; Reeves, M.J.; Hernandez, A.F.; Peterson, E.D.; Sacco, R.L.; Schwamm, L.H. Improving door-to-needle times in acute ischemic stroke: The design and rationale for the American Heart Association/American Stroke Association’s Target: Stroke initiative. Stroke 2011, 42, 2983–2989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basaraba, J.E.; Picard, M.; George-Phillips, K.; Mysak, T. Pharmacists as Care Providers for Stroke Patients: A Systematic Review. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2018, 45, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, K.; Hillier-Brown, F.; Walton, N.; Bilaj, M.; Bambra, C.; Todd, A. The effects of community pharmacy-delivered public health interventions on population health and health inequalities: A review of reviews. Prev. Med. 2019, 124, 98–109. [Google Scholar] [CrossRef]
- Ayorinde, A.A.; Porteous, T.; Sharma, P. Screening for major diseases in community pharmacies: A systematic review. Int. J. Pharm. Pract. 2013, 21, 349–361. [Google Scholar] [CrossRef]
- NHS. National Stroke Programme. 2007. Available online: https://www.england.nhs.uk/ourwork/clinical-policy/stroke/ (accessed on 4 April 2019).
- Wall, H.K.; Beagan, B.M.; O’Neill, H.J.; Foell, K.M.; Boddie-Willis, C.L. Addressing Stroke Signs and Symptoms through Public Education: The Stroke Heroes Act FAST Campaign. Prev. Chronic Dis. 2008, 5, A49. [Google Scholar]
- Dunn, S.P.; Birtcher, K.K.; Beavers, C.J.; Baker, W.; Brouse, S.D.; Page, R.L.; Bittner, V.; Walsh, M.N. The Role of the Clinical Pharmacist in the Care of Patients with Cardiovascular Disease. J. Am. Coll. Cardiol. 2015, 66, 2129–2213. [Google Scholar] [CrossRef] [Green Version]
- Stern, E.B.; Berman, M.; Thomas, J.J.; Klassen, A.C. Community education for stroke awareness: An efficacy study. Stroke 1999, 30, 720–723. [Google Scholar] [CrossRef] [Green Version]
- Chiquette, E.; Amato, M.G.; Bussey, H.I. Comparison of an anticoagulation clinic with usual medical care: Anticoagulation control, patient outcomes, and health care costs. Arch. Intern. Med. 1998, 158, 1641–1647. [Google Scholar] [CrossRef] [Green Version]
- Garabedian-Ruffalo, S.M.; Gray, D.R.; Sax, M.J.; Ruffalo, R.L. Retrospective evaluation of a pharmacist-managed warfarin anticoagulation clinic. Am. J. Hosp. Pharm. 1985, 42, 304–308. [Google Scholar] [CrossRef]
- Holden, J.; Holden, K. Comparative effectiveness of general practitioner versus pharmacist dosing of patients requiring anticoagulation in the community. J. Clin. Pharm. Ther. 2000, 25, 49–54. [Google Scholar] [CrossRef]
- Langebrake, C.; Hilgarth, H. Clinical pharmacists’ interventions in a German University Hospital. Pharm. Weekbl. Sci. Ed. 2010, 32, 194–199. [Google Scholar] [CrossRef]
- Blix, H.S.; Viktil, K.K.; Moger, T.A.; Reikvam, Å. Characteristics of drug-related problems discussed by hospital pharmacists in multidisciplinary teams. Pharm. Weekbl. Sci. Ed. 2006, 28, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Lampert, M.L.; Kraehenbuehl, S.; Hug, B.L. Drug-related problems: Evaluation of a classification system in the daily practice of a Swiss University Hospital. Pharm. Weekbl. Sci. Ed. 2008, 30, 768–776. [Google Scholar] [CrossRef] [Green Version]
- Standards for the Initial Education and Training of Pharmacists: General Pharmaceutical Council. 2021. Available online: www.pharmacyregulation.org/sites/default/files/document/standards-for-the-initial-education-and-training-of-pharmacists-january-2021_0.pdf (accessed on 8 March 2020).
- Wardlaw, J.M.; Murray, V.; Berge, E.; Del Zoppo, G.J. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, 7, CD000213. [Google Scholar]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar]
- Stroke and Transient Ischaemic Attack in over 16s: Diagnosis and Initial Management. National Institute for Health and Care Excellence (NICE) Guideline [NG128]. NICE. 2019. Available online: https://www.nice.org.uk/guidance/ng128/resources/2021-exceptional-surveillance-of-stroke-and-transient-ischaemic-attack-in-over-16s-nice-guideline-ng128-9071981821/chapter/Surveillance-decision?tab=evidence (accessed on 25 May 2021).
- Abu-Ramaileh, A.M.; Shane, R.; Churchill, W.; Steffenhagen, A.; Patka, J.; Rothschild, J.M. Evaluating and classifying pharmacists’ quality interventions in the emergency department. Am. J. Health Pharm. 2011, 68, 2271–2275. [Google Scholar] [CrossRef]
- Patanwala, A.E.; Sanders, A.B.; Thomas, M.C.; Acquisto, N.M.; Weant, K.A.; Baker, S.N.; Merritt, E.M.; Erstad, B.L. A Prospective, Multicenter Study of Pharmacist Activities Resulting in Medication Error Interception in the Emergency Department. Ann. Emerg. Med. 2012, 59, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Mangiapane, S.; Schulz, M.; Mühlig, S.; Ihle, P.; Schubert, I.; Waldmann, H.-C. Community Pharmacy–Based Pharmaceutical Care for Asthma Patients. Ann. Pharmacother. 2005, 39, 1817–1822. [Google Scholar] [CrossRef] [PubMed]
- Cesarz, J.L.; Steffenhagen, A.L.; Svenson, J.; Hamedani, A.G. Emergency Department Discharge Prescription Interventions by Emergency Medicine Pharmacists. Ann. Emerg. Med. 2013, 61, 209-214.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattanavipanon, W.; Chaiyasothi, T.; Puchsaka, P.; Mungkornkaew, R.; Nathisuwan, S.; Veettil, S.K.; Chaiyakunapruk, N. Effects of pharmacist interventions on cardiovascular risk factors and outcomes: An umbrella review of meta-analysis of randomized controlled trials. Br. J. Clin. Pharmacol. 2022, 88, 3064–3077. [Google Scholar] [CrossRef]
- Grimes, T.; Duggan, C.; Gallagher, P.; Strawbridge, J. Care of the stroke patient-communication between the community pharmacist and prescribers in the Republic of Ireland. Pharm. World Sci. 2009, 31, 648–655. [Google Scholar] [CrossRef]
- Marconi, G.P.; Claudius, I. Impact of an Emergency Department Pharmacy on Medication Omission and Delay. Pediatr. Emerg. Care 2012, 28, 30–33. [Google Scholar] [CrossRef]
- Côté, I.; Moisan, J.; Chabot, I.; Grégoire, J. Health-related quality of life in hypertension: Impact of a pharmacy intervention programme. J. Clin. Pharm. Ther. 2005, 30, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Griese-Mammen, N.; Schumacher, P.M.; Anker, S.D.; Koehler, F.; Ruckes, C.; Rettig-Ewen, V.; Wachter, R.; Trenk, D.; Böhm, M.; et al. The impact of pharmacist/physician care on quality of life in elderly heart failure patients: Results of the PHARM-CHF randomized controlled trial. ESC Heart Fail. 2020, 7, 3310–3319. [Google Scholar] [CrossRef]
- Milosavljevic, A.; Aspden, T.; Harrison, J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: A systematic review. Int. J. Pharm. Pract. 2018, 26, 387–397. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Isaac, T.; Lauffenburger, J.; Gopalakrishnan, C.; Lee, M.; Vachon, A.; Iliadis, T.L.; Hollands, W.; Elman, S.; Kraft, J.M.; et al. Effect of a Remotely Delivered Tailored Multicomponent Approach to Enhance Medication Taking for Patients with Hyperlipidemia, Hypertension, and Diabetes. JAMA Intern. Med. 2018, 178, 1182–1189. [Google Scholar] [CrossRef]
- Ho, P.M.; Lambert-Kerzner, A.; Carey, E.P.; Fahdi, I.E.; Bryson, C.L.; Melnyk, S.D.; Bosworth, H.B.; Radcliff, T.; Davis, R.; Mun, H.; et al. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 186–193. [Google Scholar] [CrossRef]
- Taitel, M.; Jiang, J.; Rudkin, K.; Chane, D.; Duncan, I.; Ewing, S. The impact of pharmacist face-to-face counseling to improve medication adherence among patients initiating statin therapy. Patient Prefer. Adher. 2012, 6, 323–329. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Qahtani, S.; Jalal, Z.; Paudyal, V.; Mahmood, S.; Mason, J. The Role of Pharmacists in Providing Pharmaceutical Care in Primary and Secondary Prevention of Stroke: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 2315. https://doi.org/10.3390/healthcare10112315
Al-Qahtani S, Jalal Z, Paudyal V, Mahmood S, Mason J. The Role of Pharmacists in Providing Pharmaceutical Care in Primary and Secondary Prevention of Stroke: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(11):2315. https://doi.org/10.3390/healthcare10112315
Chicago/Turabian StyleAl-Qahtani, Saeed, Zahraa Jalal, Vibhu Paudyal, Sajid Mahmood, and Julie Mason. 2022. "The Role of Pharmacists in Providing Pharmaceutical Care in Primary and Secondary Prevention of Stroke: A Systematic Review and Meta-Analysis" Healthcare 10, no. 11: 2315. https://doi.org/10.3390/healthcare10112315
APA StyleAl-Qahtani, S., Jalal, Z., Paudyal, V., Mahmood, S., & Mason, J. (2022). The Role of Pharmacists in Providing Pharmaceutical Care in Primary and Secondary Prevention of Stroke: A Systematic Review and Meta-Analysis. Healthcare, 10(11), 2315. https://doi.org/10.3390/healthcare10112315