
Knowledge and Attitude towards Obstructive Sleep Apnea among Primary Care Physicians in Northern Regions of Saudi Arabia: A Multicenter Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Description
2.2. Inclusion and Exclusion Criteria
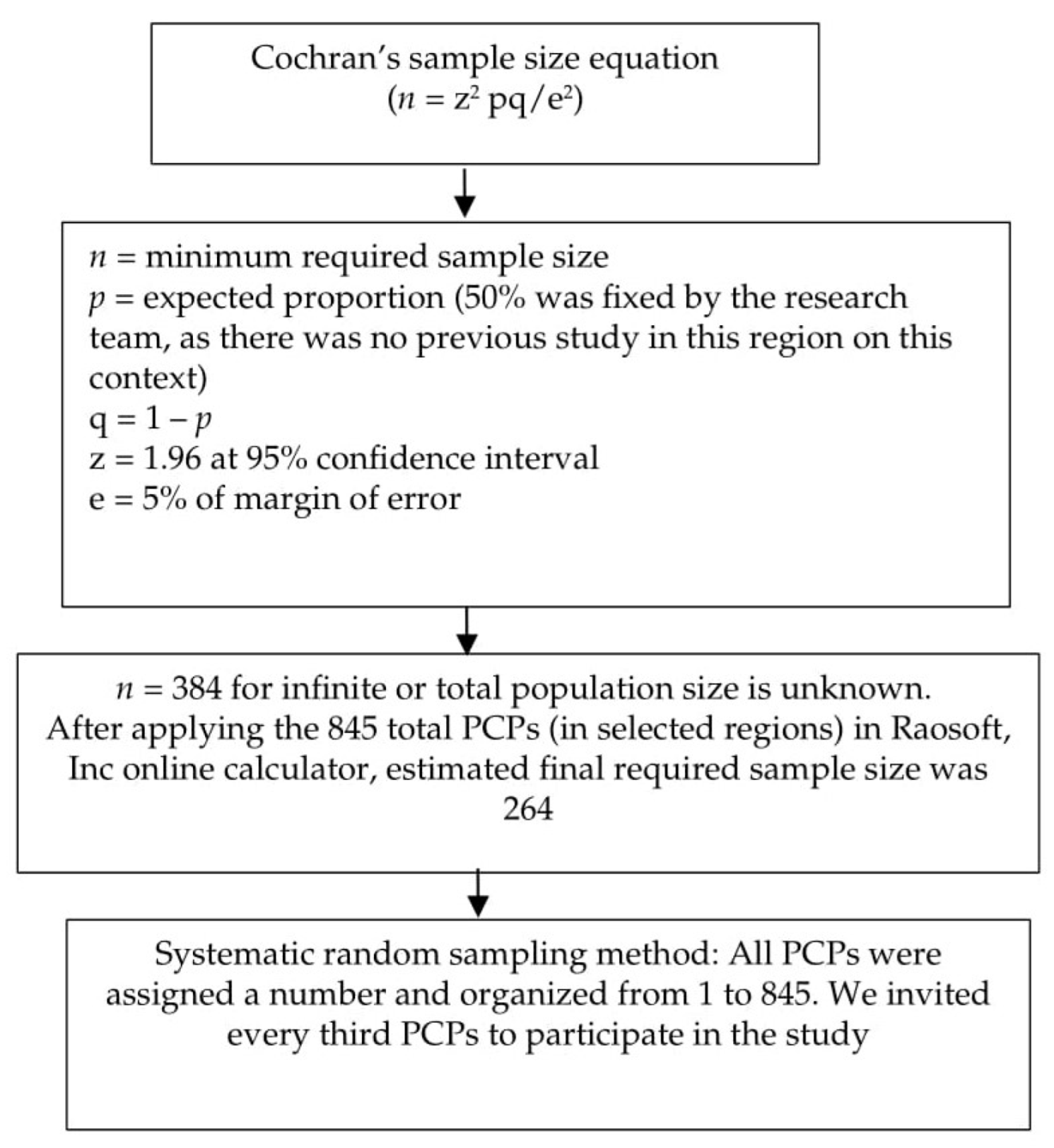
2.3. Sample Size
2.4. Data Collection
2.4.1. Part I: Personal Information
2.4.2. Part II: The Obstructive Sleep Apnea Knowledge and Attitude (OSAKA) Questionnaire
2.5. Statistical Analysis
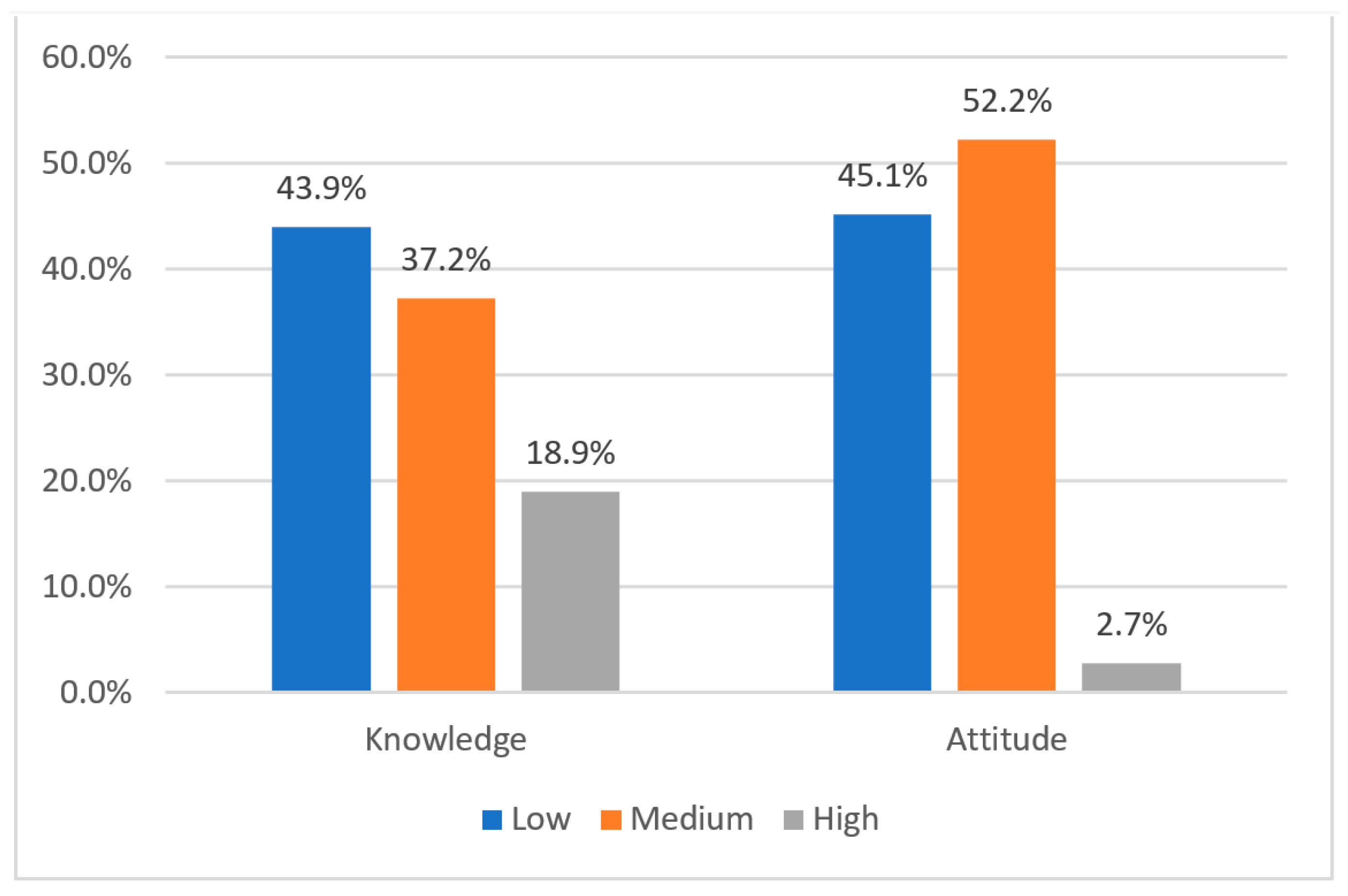
3. Results
4. Discussion
5. Strengths and Weaknesses of the Present Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. CDC—Data and Statistics—Sleep and Sleep Disorders. Available online: https://www.cdc.gov/sleep/data_statistics.html (accessed on 15 March 2022).
- Almeneessier, A.S.; BaHammam, A.S. Sleep Medicine in Saudi Arabia. J. Clin. Sleep Med. 2017, 13, 641–645. [Google Scholar] [CrossRef]
- Wali, S.O.; Abalkhail, B.; Krayem, A. Prevalence and risk factors of obstructive sleep apnea syndrome in a Saudi Arabian population. Ann. Thorac Med. 2017, 12, 88–94. [Google Scholar] [CrossRef]
- Alsultan, A.; Al Sahlawi, M.; Agha, M. Prevalence of Obstructive Sleep Apnea Symptoms Among the Adult Population in Al-Ahsa, Saudi Arabia. Cureus 2022, 14, e31082. [Google Scholar] [CrossRef]
- Alhejaili, F.; Hafez, A.; Wali, S.; Alshumrani, R.; Alzehairi, A.M.; Balkhyour, M.; Pandi-Perumal, S.R. Prevalence of Obstructive Sleep Apnea Among Saudi Pilots. Nat. Sci. Sleep 2021, 13, 537–545. [Google Scholar] [CrossRef]
- Almeneessier, A.S.; Alangari, M.; Aldubayan, A.; Alsharidah, A.; Altaki, A.; Olaish, A.H.; Sabr, Y.S.; BaHammam, A.S. Prevalence of symptoms and risk of obstructive sleep apnea in Saudi pregnant women. Ann. Thorac. Med. 2020, 15, 163. [Google Scholar] [CrossRef]
- Karna, B.; Sankari, A.; Tatikonda, G. Sleep disorder. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.A.; Jairam, S.; Hussain, M.R.; Shapiro, C.M. Knowledge of sleep apnea in a sample grouping of primary care physicians. Sleep Breath 2001, 5, 115–121. [Google Scholar] [CrossRef]
- Thirunavukkarasu, A.; Almulhim, A.K.; Albalawi, F.A.; Alruwaili, Z.M.; Almajed, O.A.; Alruwaili, S.H.; Almugharriq, M.M.; Alruwaili, A.S.; Alkuwaykibi, M.K. Knowledge, Attitudes, and Practices towards Diabetic Retinopathy among Primary Care Physicians of Saudi Arabia: A Multicenter Cross-Sectional Study. Healthcare 2021, 9, 1697. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, N.K. Knowledge, attitude, and practice regarding obstructive sleep apnea among primary care physicians. Sleep Breath 2020, 24, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.N.; Berger, A.M. Screening and assessment for obstructive sleep apnea in primary care. Sleep Med. Rev. 2016, 29, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Al-Khafaji, H.; Bilgay, I.B.; Tamim, H.; Hoteit, R.; Assaf, G. Knowledge and attitude of primary care physicians towards obstructive sleep apnea in the Middle East and North Africa region. Sleep Breath 2021, 25, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Hu, A. Knowledge and confidence in managing obstructive sleep apnea patients in Canadian otolaryngology—Head and neck surgery residents: A cross sectional survey. J. Otolaryngol. Head Neck Surg. 2020, 49, 21. [Google Scholar] [CrossRef] [PubMed]
- Hodibi, M.; Aljubran, Z.; Sattar, A. Knowledge and attitude of primary health care physicians in Al-hasa towards obstructive sleep apnea. Hypertension 2020, 77, 114. [Google Scholar]
- Devani, N.; Aslan, T.; Leske, F.; Mansell, S.K.; Morgan, S.; Mandal, S. Integrated diagnostic pathway for patients referred with suspected OSA: A model for collaboration across the primary-secondary care interface. BMJ Open Respir. Res. 2020, 7, e000743. [Google Scholar] [CrossRef]
- Cochran, W.G. Sampling Techniques; John Wiley & Sons: Hoboken, NJ, USA, 1977. [Google Scholar]
- Schotland, H.M.; Jeffe, D.B. Development of the obstructive sleep apnea knowledge and attitudes (OSAKA) questionnaire. Sleep Med. 2003, 4, 443–450. [Google Scholar] [CrossRef]
- Thirunavukkarasu, A.; Al-Hazmi, A.H.; Dar, U.F.; Alruwaili, A.M.; Alsharari, S.D.; Alazmi, F.A.; Alruwaili, S.F.; Alarjan, A.M. Knowledge, attitude and practice towards bio-medical waste management among healthcare workers: A northern Saudi study. PeerJ 2022, 10, e13773. [Google Scholar] [CrossRef]
- Asdaq, S.M.B.; Alshari, A.S.; Imran, M.; Sreeharsha, N.; Sultana, R. Knowledge, attitude and practices of healthcare professionals of Riyadh, Saudi Arabia towards COVID-19: A cross-sectional study. Saudi J. Biol. Sci. 2021, 28, 5275–5282. [Google Scholar] [CrossRef]
- Corso, R.M.; Sorbello, M.; Buccioli, M.; Carretta, E.; Nanni, O.; Piraccini, E.; Merli, G.; Petrini, F.; Guarino, A.; Frova, G. Survey of Knowledge and Attitudes about Obstructive Sleep Apnoea Among Italian Anaesthetists. Turk. J. Anaesthesiol. Reanim. 2017, 45, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Embarak, S.; Zake, L.G.; Abd-El-Azem, W.; Sileem, A.E. Awareness of obstructive sleep apnea among critical care physicians in Sharkia Governorate, Egypt. Egypt. J. Bronchol. 2020, 14, 6. [Google Scholar] [CrossRef]
- Chérrez-Ojeda, I.; Calderón, J.C.; Fernández García, A.; Jeffe, D.B.; Santoro, I.; Vanegas, E.; Cherrez, A.; Cano, J.; Betancourt, F.; Simancas-Racines, D. Obstructive sleep apnea knowledge and attitudes among recent medical graduates training in Ecuador. Multidiscip. Respir. Med. 2018, 13, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherrez Ojeda, I.; Jeffe, D.B.; Guerrero, T.; Mantilla, R.; Santoro, I.; Gabino, G.; Calderon, J.C.; Caballero, F.; Mori, J.; Cherrez, A. Attitudes and knowledge about obstructive sleep apnea among Latin American primary care physicians. Sleep Med. 2013, 14, 973–977. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.R.; Akemokwe, F.M.; Marangu, D.M.; Chisunkha, B.; Irekpita, E.; Obasikene, G.; Kagima, J.W.; Obonyo, C.O. Obstructive Sleep Apnea Awareness among Primary Care Physicians in Africa. Ann. Am. Thorac Soc. 2020, 17, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Simmons, M.; Sayre, J.; Schotland, H.; Jeffe, D. Obstructive sleep apnea knowledge among dentists and physicians. J. Dent. Sleep Med. 2021, 8. [Google Scholar] [CrossRef]
- Alshehri, A.M.; Alshehri, M.S.; Alamri, O.M.; Alshehri, F.S.; Alshahrani, M.; Alflan, M.A.; Alshahrani, M.S. Knowledge, Awareness, and Attitudes Toward Obstructive Sleep Apnea among the Population of the Asir Region of Saudi Arabia in 2019. Cureus 2020, 12, e7254. [Google Scholar] [CrossRef] [Green Version]
- Bendapudi, N.M.; Berry, L.L.; Frey, K.A.; Parish, J.T.; Rayburn, W.L. Patients’ perspectives on ideal physician behaviors. Mayo Clin. Proc. 2006, 81, 338–344. [Google Scholar] [CrossRef] [Green Version]
- Howard, M.; Langevin, J.; Bernard, C.; Tan, A.; Klein, D.; Slaven, M.; Barwich, D.; Elston, D.; Arora, N.; Heyland, D.K. Primary care clinicians’ confidence, willingness participation and perceptions of roles in advance care planning discussions with patients: A multi-site survey. Fam. Pract. 2020, 37, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Owens, K.M.; Keller, S. Exploring workforce confidence and patient experiences: A quantitative analysis. Patient Exp. J. 2018, 5, 97–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 127 | 48.1 |
| Female | 137 | 51.9 |
| Age in years, mean (SD) | 33 (8.01) | |
| Regions | ||
| Aljouf | 59 | 22.3 |
| Tabuk | 89 | 33.7 |
| Northern border | 116 | 43.9 |
| Latest qualification | ||
| MBBS | 126 | 47.7 |
| MD | 69 | 26.1 |
| Board certified | 42 | 15.9 |
| Others | 27 | 10.2 |
| Current position | ||
| Residents | 153 | 57.9 |
| Specialists/Registrars | 63 | 23.9 |
| Consultants | 48 | 18.2 |
| Practice duration in years, mean (SD) | 8 (6.6) | |
| Rate OSA Cases encountered Mean (SD) | 2.63 (2.22) | |
| Specialty | Frequency | Percentage |
|---|---|---|
| ENT | 104 | 39.4 |
| Sleep clinic | 57 | 21.0 |
| Respiratory | 48 | 18.2 |
| Neurology | 13 | 4.9 |
| Pediatrics | 4 | 1.5 |
| Others | 25 | 9.5 |
| None | 13 | 4.9 |
| Question Number | OSAKA Questions | Correct Answer n (%) |
|---|---|---|
| 1 | Females with OSA (obstructive sleep apnea) may have only fatigue | 149 (56.45) |
| 2 | Uvulopalatopharyngoplasty is a cure for most patients with OSA | 130 (50.8) |
| 3 | Adult OSA prevalence is estimated to be between 2 and 10% | 108 (40) |
| 4 | Snoring is present in most of the patients with OSA | 215 (81.4) |
| 5 | OSA has an association with hypertension | 175 (66.3) |
| 6 | The gold standard for the diagnosis of OSA is overnight sleep study | 206 (78) |
| 7 | CPAP therapy may lead to nasal congestion | 163 (61.7) |
| 8 | Laser-assisted uvuloplasty is an appropriate treatment for severe OSA | 134 (50.8) |
| 9 | OSA may be due to a loss of upper airway muscle tone during sleep | 184 (69.7) |
| 10 | In children, adenoids and large tonsils most commonly cause OSA | 216 (81.8) |
| 11 | A useful examination in suspected OSA is a craniofacial and oropharyngeal examination | 193 (73.1) |
| 12 | Alcohol at bedtime improves OSA | 81 (30.7) |
| 13 | Untreated OSA has an association with a higher incidence of car related accidents | 180 (68.2) |
| 14 | A collar size greater than 17 is associated with OSA in males | 108 (40.9) |
| 15 | Females suffer from OSA more than males | 141 (53.4) |
| 16 | CPAP is the first therapy for severe OSA | 92 (34.8) |
| 17 | In adults, it is normal to have five apneas or hypopneas in one hour | 95 (36) |
| 18 | There may be an association between untreated OSA and arrhythmias of the heart | 171 (64.8) |
| Median (IQR) of the correct answer (%) in the knowledge category | 59.14 (33.3%) |
| Knowledge | ||||
|---|---|---|---|---|
| Total (264) | Low/Average (214) n (%) | High (50) n (%) | p-Value | |
| Gender * | ||||
| Male | 127 | 107 (84.3) | 20 (15.7) | 0.213 |
| Female | 137 | 107 (78.1) | 30 (21.9) | |
| Age in years: Mean (SD) ** | 33.40 (8.41) | 32.98 (8.11) | 0.744 | |
| Regions * | ||||
| Aljouf | 59 | 51 (86.4) | 8 (13.6) | 0.002 *** |
| Tabuk | 89 | 81 (91.0) | 8 (9.0) | |
| Northern border | 116 | 81 (70.7) | 34 (29.3) | |
| Latest qualification* | ||||
| MBBS | 126 | 97 (77.0) | 29 (23.0) | 0.056 |
| MD/MS | 69 | 58 (84.1) | 11 (15.9) | |
| Saudi Board certified | 42 | 33 (78.6) | 9 (21.4) | |
| Others (Fellowship, PhD) | 27 | 26(96.3) | 1 (2.0) | |
| Current position * | ||||
| Residents | 153 | 121 (79.1) | 32 (20.9) | 0.585 |
| Specialists/Registrars | 63 | 52 (82.5) | 11 (17.5) | |
| Consultants | 48 | 41 (85.4) | 7 (14.6) | |
| Practice duration in years, mean (SD) ** | 7.99 (6.55) | 6.82 (5.68) | 0.267 | |
| Item | Frequency | Proportion |
|---|---|---|
| Importance of identifying OSA patients (data shown are either important or very importance) | ||
| OSA is an important disease | 134 | 50.8 |
| Diagnosis of people with OSA is very much essential | 136 | 51.5 |
| Self-confidence (data shown are either agree or strongly agree) | ||
| Confident in diagnosing patients with a high risk of developing OSA | 195 | 73.9 |
| Confident in their capability to care for OSA patients | 150 | 56.8 |
| Confident in their skills to manage OSA patients on CPAP treatment | 125 | 47.3 |
| Spearman’s Coefficient Value (Rho) | p-Value | |
|---|---|---|
| Knowledge–Attitude | 0.151 | 0.017 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Rasheedi, A.N.; Thirunavukkarasu, A.; Almutairi, A.; Alruwaili, S.; Alotaibi, H.; Alzaid, W.; Albalawi, F.; Alwadani, O.; Dilli, A. Knowledge and Attitude towards Obstructive Sleep Apnea among Primary Care Physicians in Northern Regions of Saudi Arabia: A Multicenter Study. Healthcare 2022, 10, 2369. https://doi.org/10.3390/healthcare10122369
Al-Rasheedi AN, Thirunavukkarasu A, Almutairi A, Alruwaili S, Alotaibi H, Alzaid W, Albalawi F, Alwadani O, Dilli A. Knowledge and Attitude towards Obstructive Sleep Apnea among Primary Care Physicians in Northern Regions of Saudi Arabia: A Multicenter Study. Healthcare. 2022; 10(12):2369. https://doi.org/10.3390/healthcare10122369
Chicago/Turabian StyleAl-Rasheedi, Abdullah N., Ashokkumar Thirunavukkarasu, Abdulhakeem Almutairi, Sultan Alruwaili, Hatem Alotaibi, Wasan Alzaid, Faisal Albalawi, Osama Alwadani, and Ahmed Dilli. 2022. "Knowledge and Attitude towards Obstructive Sleep Apnea among Primary Care Physicians in Northern Regions of Saudi Arabia: A Multicenter Study" Healthcare 10, no. 12: 2369. https://doi.org/10.3390/healthcare10122369
APA StyleAl-Rasheedi, A. N., Thirunavukkarasu, A., Almutairi, A., Alruwaili, S., Alotaibi, H., Alzaid, W., Albalawi, F., Alwadani, O., & Dilli, A. (2022). Knowledge and Attitude towards Obstructive Sleep Apnea among Primary Care Physicians in Northern Regions of Saudi Arabia: A Multicenter Study. Healthcare, 10(12), 2369. https://doi.org/10.3390/healthcare10122369