
Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study

 , ,
, , 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection and Sample Size
- 1.
- First phase: A group of general practitioners (GPs) was selected by block randomization from the Local Health Authorities (LHA) archives.
- 2.
- Second phase: another randomization to select 25 patients over 64 years was performed by each GPs.
2.3. Measurement
- •
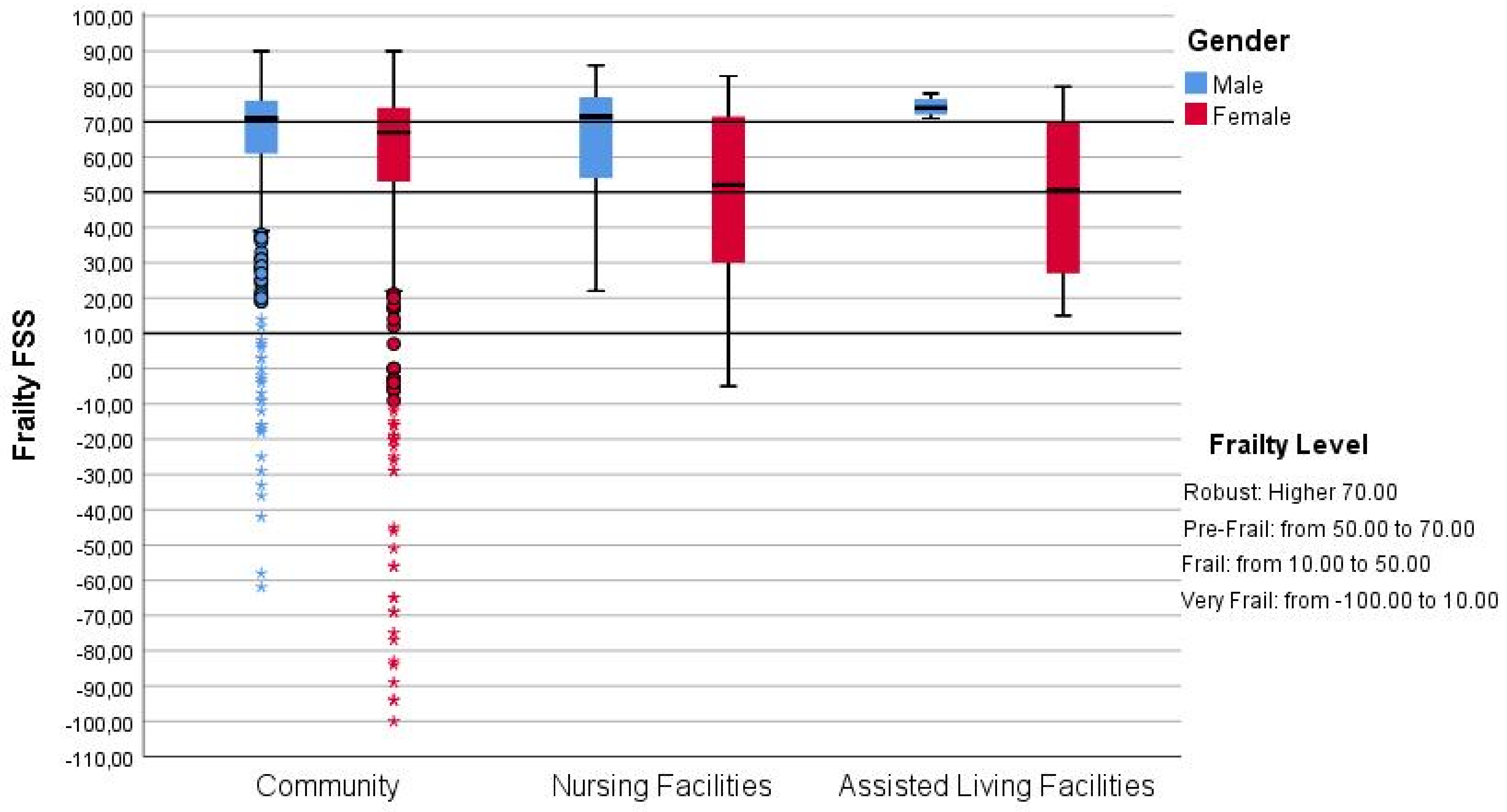
- The Functional Geriatric Evaluation (FGE) questionnaire [30] assesses the multidimensional bio-psycho-social frailty in older adults. The FGE was the Italian version [29,30] of Grauer functional rating scale [31] validated in 2005 by Palombi et al. [32]. This questionnaire analyzes five domains, physical health, mental health, functional state, social resources, and economic resources, contributing to the final synthetic score (FSS). The FSS identified four levels of frailty: Very Frail, Frail, Pre-Frail, and Robust, with a score of ≤10, a score of >10 but <50, a score of ≥50 but ≤70, and a score of >70, respectively. The final score ranges from 108 to −101.
- •
- A list of 21 diseases assessed, with the support of GPs, to evaluate the presence or absence of comorbidity. The presence of comorbidity was considered when there were two or more active disease.
- •
- Activities of Daily Life (ADL) [33] and Instrumental Activities of Daily Life (IADL) [34] questionnaires that were administrated to define the level of disability to each participant in the study. Moderate disability was defined by dependence in performing IADL while severe disability was defined by dependence in performing ADL.
- •
- The absolute number of accesses to nursing facilities or home care has been retrieved from the Regional Health Database and the GPs for each participant involved in the study.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| N (%) | Mean ± SD | |
|---|---|---|
| Gender Female | 14 (63.6) | |
| Age <74 years 75–85 years <85 years | 2 (9.1) 12 (54.5) 8 (36.4) | 82.18 ± 6.471 |
| Cohabitants Alone Spouse Child Others Paid assistant | 5 (22.7) 6 (27.3) 4 (18.2) 2 (9.1) 5 (22.7) | |
| Education No education Primary school Middle school High school Degree | 2 (9.1) 12 (54.5) 5 (22.7) 2 (9.1) 1 (4.5) | |
| Frailty Robust Pre-Frail Frail Very Frail | 3 (13.6) 5 (22.7) 5 (22.7) 9 (40.9) | 12.91 ± 55.39 |
| Comorbidity Presence of two or more disease | 20 (90.9) | |
| Disability No Moderate Severe | 7 (31.8) 6 (27.3) 9 (40.9) |
References
- Rechel, B.; Grundy, E.; Robine, J.-M.; Cylus, J.; Mackenbach, J.P.; Knai, C.; McKee, M. Ageing in the European Union. Lancet 2013, 381, 1312–1322. [Google Scholar] [CrossRef]
- World Health Organization. Ageing and Health; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Ellis, J.M. Psychological transition into a residential care facility: Older people’s experiences. J. Adv. Nurs. 2010, 66, 1159–1168. [Google Scholar] [CrossRef]
- World Health Organization. Lessons for Long-Term Care Policy the Cross-Cluster Initiative on Long-Term Care; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Luppa, M.; Luck, T.; Weyerer, S.; König, H.-H.; Brähler, E.; Riedel-Heller, S.G. Prediction of institutionalization in the elderly. A systematic review. Age Ageing 2010, 39, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Lopes, H.; Mateus, C.; Rosati, N. Identifying the long-term care beneficiaries: Differences between risk factors of nursing homes and community-based services admissions. Aging Clin. Exp. Res. 2020, 32, 2099–2110. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Duval, S.; Anderson, K.; Kane, R.L. Predicting nursing home admission in the U.S: A meta-analysis. BMC Geriatr. 2007, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luppa, M.; Riedel-Heller, S.G.; Luck, T.; Wiese, B.; Bussche, H.V.D.; Haller, F.; Sauder, M.; Mösch, E.; Pentzek, M.; Wollny, A.; et al. Age-related predictors of institutionalization: Results of the German study on ageing, cognition and dementia in primary care patients (AgeCoDe). Soc. Psychiatry 2010, 47, 263–327. [Google Scholar] [CrossRef] [PubMed]
- Tomiak, M.; Berthelot, J.-M.; Guimond, E.; Mustard, C.A. Factors associated with nursing-home entry for elders in Manitoba, Canada. J. Gerontol. Ser. A 2000, 55, M279–M287. [Google Scholar] [CrossRef] [Green Version]
- Luppa, M.; Luck, T.; Weyerer, S.; König, H.-H.; Riedel-Heller, S.G. Gender differences in predictors of nursing home placement in the elderly: A systematic review. Int. Psychogeriatr. 2009, 21, 1015–1025. [Google Scholar] [CrossRef]
- Hajek, A.; Brettschneider, C.; Lange, C.; Posselt, T.; Wiese, B.; Steinmann, S.; Weyerer, S.; Werle, J.; Pentzek, M.; Fuchs, A.; et al. Longitudinal Predictors of Institutionalization in Old Age. PLoS ONE 2015, 10, e0144203. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Cornally, N.; Weathers, E.T.; O’Sullivan, R.; Fitzgerald, C.; Orfila, F.; Clarnette, R.; Paúl, M.C.; Molloy, D.W. Risk prediction in the community: A systematic review of case-finding instruments that predict adverse healthcare outcomes in community-dwelling older adults. Maturitas 2015, 82, 3–21. [Google Scholar] [CrossRef]
- Sibolt, G.; Curtze, S.; Melkas, S.; Pohjasvaara, T.; Kaste, M.; Karhunen, P.J.; Oksala, N.K.J.; Erkinjuntti, T. Severe Cerebral White Matter Lesions in Ischemic Stroke Patients are Associated with Less Time Spent at Home and Early Institutionalization. Int. J. Stroke 2015, 10, 1192–1196. [Google Scholar] [CrossRef]
- Sibolt, G.; Curtze, S.; Jokinen, H.; Pohjasvaara, T.; Kaste, M.; Karhunen, P.; Erkinjuntti, T.; Melkas, S.; Oksala, N.K.J. Post-stroke dementia and permanent institutionalization. J. Neurol Sci. 2021, 421, 117307. [Google Scholar] [CrossRef]
- Toot, S.; Swinson, T.; Devine, M.; Challis, D.; Orrell, M. Causes of nursing home placement for older people with dementia: A systematic review and meta-analysis. Int. Psychogeriatr. 2017, 29, 195–208. [Google Scholar] [CrossRef] [Green Version]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentili, S.; Emberti Gialloreti, L.; Riccardi, F.; Scarcella, P.; Liotta, G. Predictors of Emergency Room Access and Not Urgent Emergency Room Access by the Frail Older Adults. Front. Public Health 2021, 9, 721634. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Mitnitski, A.; Song, X.; Steen, B.; Skoog, I. Long-Term Risks of Death and Institutionalization of Elderly People in Relation to Deficit Accumulation at Age 70. J. Am. Geriatr. Soc. 2006, 54, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a Predictor of Nursing Home Placement Among Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. J. Geriatr. Phys. Ther. 2018, 41, 42–48. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Shamliyan, T.A.; Talley, K.M.C.; Ramakrishnan, R.; Kane, R.L. Not just specific diseases: Systematic review of the association of geriatric syndromes with hospitalization or nursing home admission. Arch. Gerontol. Geriatr. 2013, 57, 16–26. [Google Scholar] [CrossRef]
- Bandeen-Roche, K.; Xue, Q.-L.; Ferrucci, L.; Walston, J.; Guralnik, J.M.; Chaves, P.; Zeger, S.L.; Fried, L.P. Phenotype of Frailty: Characterization in the Women’s Health and Aging Studies. J. Gerontol. Ser. A 2006, 61, 262–266. [Google Scholar] [CrossRef] [Green Version]
- Jones, D.; Song, X.; Mitnitski, A.; Rockwood, K. Evaluation of a frailty index based on a comprehensive geriatric assessment in a population based study of elderly Canadians. Aging Clin. Exp. Res. 2005, 17, 465–471. [Google Scholar] [CrossRef]
- Drubbel, I.; De Wit, N.J.; Bleijenberg, N.; Eijkemans, R.J.; Schuurmans, M.J.; Numans, M.E. Prediction of Adverse Health Outcomes in Older People Using a Frailty Index Based on Routine Primary Care Data. J. Gerontol. Ser. A 2013, 68, 301–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilotta, C.; Nicolini, P.; Casè, A.; Pina, G.; Rossi, S.; Vergani, C. Frailty syndrome diagnosed according to the Study of Osteoporotic Fractures (SOF) criteria and adverse health outcomes among community-dwelling older outpatients in Italy. A one-year prospective cohort study. Arch. Gerontol. Geriatr. 2012, 54, e23–e28. [Google Scholar] [CrossRef] [PubMed]
- Forti, P.; Rietti, E.; Pisacane, N.; Olivelli, V.; Maltoni, B.; Ravaglia, G. A comparison of frailty indexes for prediction of adverse health outcomes in an elderly cohort. Arch. Gerontol. Geriatr. 2012, 54, 16–20. [Google Scholar] [CrossRef]
- Coelho, T.; Paúl, M.C.; Gobbens, R.; Fernandes, L. Frailty as a predictor of short-term adverse outcomes. PeerJ 2015, 3, e1121. [Google Scholar] [CrossRef] [Green Version]
- Liotta, G.; O’Caoimh, R.; Gilardi, F.; Proietti, M.G.; Rocco, G.; Alvaro, R.; Scarcella, P.; Molloy, D.W.; Orlando, S.; Mancinelli, S.; et al. Assessment of frailty in community-dwelling older adults residents in the Lazio region (Italy): A model to plan regional community-based services. Arch. Gerontol. Geriatr. 2016, 68, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Scarcella, P.; Liotta, G.; Marazzi, M.; Carbini, R.; Palombi, L. Analysis of survival in a sample of elderly patients from Ragusa, Italy on the basis of a primary care level multidimensional evaluation. Arch. Gerontol. Geriatr. 2005, 40, 147–156. [Google Scholar] [CrossRef]
- Grauer, H.; Birnbom, F. A Geriatric Functional Rating Scale to Determine the Need for Institutional Care. J. Am. Geriatr. Soc. 1975, 23, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Palombi, L.; Liotta, G.; Scarcella, P.; Gilardi, F. Rapporto. La valutazione del grado di fragilità e del fabbisogno di assistenza continuativa degli ultrasessantaquattrenni nel Lazio; Università di Roma Tor Vergata: Rome, Italy, 2015. [Google Scholar]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Lawton, P.M.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Johnson, R.A.; Wichern, D.W. Applied Multivariate Statistical Analysis, 6th ed.; Pearson Prentice Hall USR: Upper Saddle River, NJ, USA, 2007. [Google Scholar]
- Cattell, R.B. The Meaning and Strategic Use of Factor Analysis. In Handbook of Multivariate Experimental Psychology. Perspectives on Individual Differences. Handbook of Multivariate Experimental Psychology; Nesselroade, J.R., Cattell, R.B., Eds.; Springer: Boston, MA, USA, 1988; pp. 131–203. [Google Scholar]
- Hair, J.F., Jr.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Pearson Prentice Hall USR: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Khangar, N.V.; Kamalja, K.K. Multiple Correspondence Analysis and its applications. Electron. J. Appl. Stat. Anal. 2017, 10, 432–462. [Google Scholar]
- Bharucha, A.J.; Pandav, R.; Shen, C.; Dodge, H.H.; Ganguli, M. Predictors of nursing facility admission: A 12-year epidemiological study in the United States. J. Am. Geriatr. Soc. 2004, 52, 434–439. [Google Scholar] [CrossRef]
- Agüero-Torres, H.; von Strauss, E.; Viitanen, M.; Winblad, B.; Fratiglioni, L. Institutionalization in the elderly The role of chronic diseases and dementia. Cross-sectional and longitudinal data from a population-based study. J. Clin. Epidemiol. 2001, 54, 795–801. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Lips, P.; Ribbe, M.W.; Deeg, D.J.H. The effect of frailty on residential/nursing home admission in the Netherlands independent of chronic diseases and functional limitations. Eur. J. Ageing 2005, 2, 264–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachs, M.S.; Williams, C.S.; O’Brien, S.; Pillemer, K.A. Adult Protective Service Use and Nursing Home Placement. Gerontologist 2002, 42, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Kersting, R.C. Impact of Social Support, Diversity, and Poverty on Nursing Home Utilization in a Nationally Representative Sample of Older Americans. Soc. Work Health Care 2001, 33, 67–87. [Google Scholar] [CrossRef] [PubMed]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Voshaar, R.O. Prevalence of Frailty in Community-Dwelling Older Persons: A Systematic Review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Russell, D.W.; Cutrona, C.E.; de la Mora, A.; Wallace, R.B. Loneliness and nursing home admission among rural older adults. Psychol. Aging 1997, 12, 574–589. [Google Scholar] [CrossRef]
- Hanratty, B.; Stow, D.; Moore, D.C.; Valtorta, N.K.; Matthews, F. Loneliness as a risk factor for care home admission in the English Longitudinal Study of Ageing. Age Ageing 2018, 47, 896–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurichi, J.E.; Streim, J.E.; Xie, D.; Hennessy, S.; Na, L.; Saliba, D.; Pan, Q.; Kwong, P.L.; Bogner, H.R. The Association Between Activity Limitation Stages and Admission to Facilities Providing Long-term Care Among Older Medicare Beneficiaries. Am. J. Phys. Med. Rehabil. 2017, 96, 464–472. [Google Scholar] [CrossRef] [PubMed]


| N (%) | Mean ± SD | χ 2 p-Value | |
|---|---|---|---|
| Gender Female | 651 (53.2) | NS. | |
| Age <74 years 75–85 years >85 years | 540 (44.1) 511 (41.7) 173 (14.1) | 76.25 ± 7.129 | NS. |
| Cohabitants Alone Spouse Child Others Homeworker | 253 (20.7) 638 (52.1) 267 (21.8) 40 (3.3) 26 (2.1) | NS. | |
| Education No education Primary school Middle school High school Degree | 94 (7.7) 577 (47.1) 305 (24.9) 187 (15.3) 60 (4.9) | NS. | |
| Frailty Robust Pre-Frail Frail Very Frail | 535 (43.7) 444 (36.3) 162 (13.2) 83 (6.8) | 59.25 ± 27.96 | 0.001 |
| Comorbidity Presence of two or more disease | 1041 (81.7) | 0.002 | |
| Disability No Moderate Severe | 858 (70.1) 290 (23.7) 76 (6.2) | NS. |
| FRAILTY LEVEL | LTC Facilities Rate per 1000 Observation/Year | 95%CI | |
|---|---|---|---|
| Robust | 11.2 | 5.9 | 16.4 |
| Pre-Frail | 8.1 | 3.1 | 13.1 |
| Frail | 28.4 | 5.9 | 50.8 |
| Very Frail | 18.1 | 0.0 | 39.9 |
| FRAILTY LEVEL | Without Social Support | With Social Support | Total | |
|---|---|---|---|---|
| Robust | Community-Dwelling | 62 (12.6) | 429 (87.4) | 491 (96.6) |
| LTC facilities | 1 (5.9) | 16 (94.1) | 17 (3.4) | |
| Pre-Frail | Community-Dwelling | 247 (61.8) | 153 (38.3) | 400 (97.5) |
| LTC facilities | 7 (70.0) | 3 (30.0) | 10 (2.5) | |
| Frail | Community-Dwelling | 89 (67.4) | 43 (32.6) | 132 (93.6) |
| LTC facilities | 6 (66.7) | 3 (33.3) | 9 (6.4) | |
| Very Frail | Community-Dwelling | 53 (74.6) | 18 (25.4) | 71 (95.9) |
| LTC facilities | 3 (100) | 3 (4.1) |
| 95% C.I per B | |||||||
|---|---|---|---|---|---|---|---|
| B | S.E. | β | t | p-Value | Lower | Higher | |
| FSS | 0.001 | <0.001 | 0.273 | 4.800 | <0.001 | 0.000 | 0.001 |
| Take medicine | 0.050 | 0.012 | 0.188 | 4.184 | <0.001 | 0.027 | 0.074 |
| Inhabitants | 0.006 | 0.003 | 0.072 | 2.461 | 0.015 | 0.001 | 0.011 |
| Cardiovascular disease | 0.009 | 0.002 | 0.111 | 3.663 | <0.001 | 0.004 | 0.014 |
| Managing money | 0.020 | 0.007 | 0.151 | 2.998 | 0.003 | 0.007 | 0.033 |
| Gender | 0.004 | 0.004 | 0.027 | 0.896 | 0.370 * | −0.005 | 0.013 |
| Age | 0.001 | <0.001 | 0.051 | 1.577 | 0.115 * | 0.000 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentili, S.; Riccardi, F.; Gialloreti, L.E.; Scarcella, P.; Stievano, A.; Proietti, M.G.; Rocco, G.; Liotta, G. Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare 2022, 10, 317. https://doi.org/10.3390/healthcare10020317
Gentili S, Riccardi F, Gialloreti LE, Scarcella P, Stievano A, Proietti MG, Rocco G, Liotta G. Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare. 2022; 10(2):317. https://doi.org/10.3390/healthcare10020317
Chicago/Turabian StyleGentili, Susanna, Fabio Riccardi, Leonardo Emberti Gialloreti, Paola Scarcella, Alessandro Stievano, Maria Grazia Proietti, Gennaro Rocco, and Giuseppe Liotta. 2022. "Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study" Healthcare 10, no. 2: 317. https://doi.org/10.3390/healthcare10020317
APA StyleGentili, S., Riccardi, F., Gialloreti, L. E., Scarcella, P., Stievano, A., Proietti, M. G., Rocco, G., & Liotta, G. (2022). Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare, 10(2), 317. https://doi.org/10.3390/healthcare10020317