
Association between Overall Survival and Activities of Daily Living in Patients with Spinal Bone Metastases

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
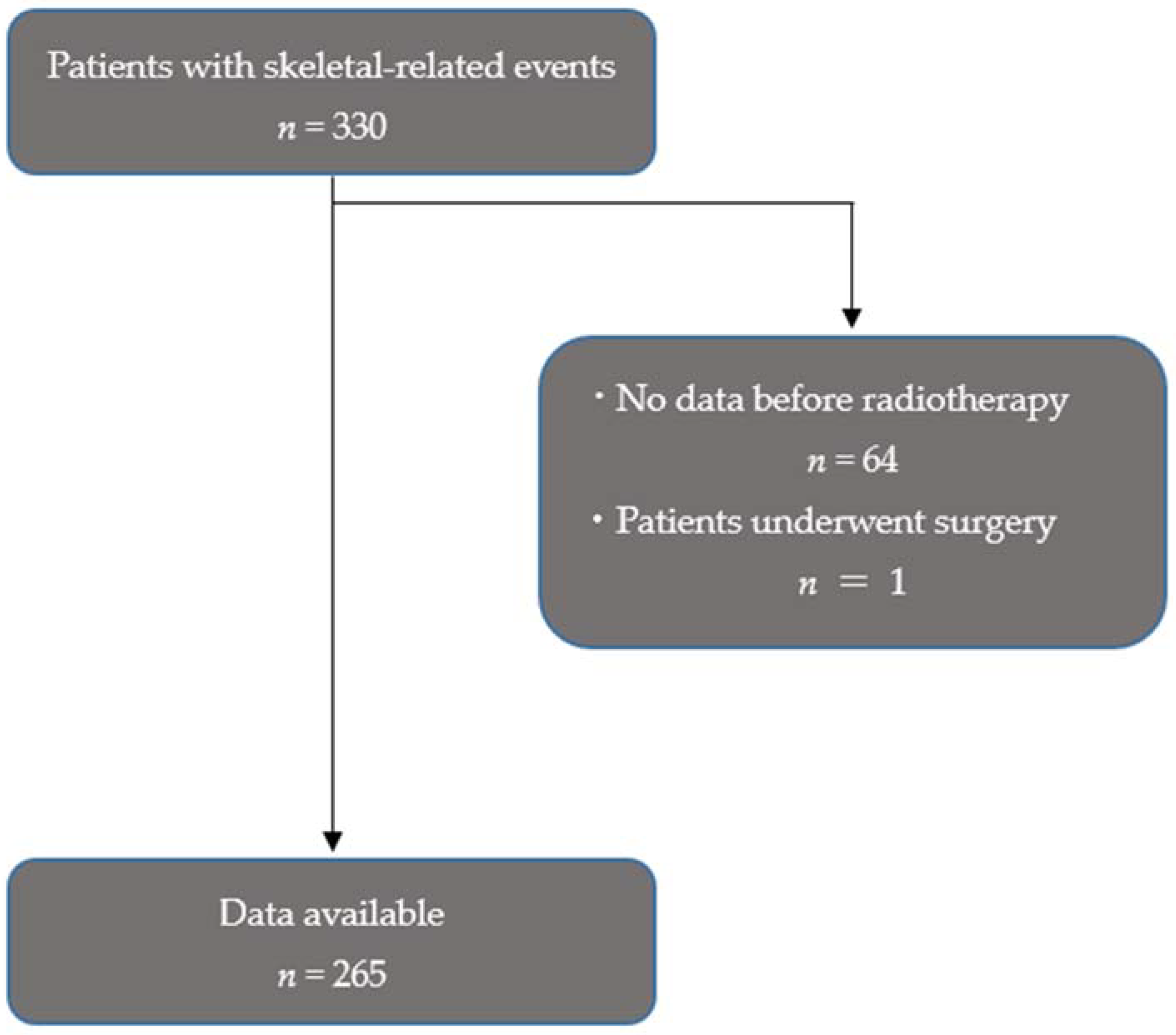
2.2. Patients
2.3. Clinical Parameters
2.4. Measurement of ADL
2.5. Measurement of Pain
2.6. The Primary Site and Spinal Level of Bone Metastases
2.7. Measurement of Spinal Instability
2.8. Treatment Strategy
2.9. OS
2.10. Statistical Analyses
3. Results
3.1. Characteristics of the Patients
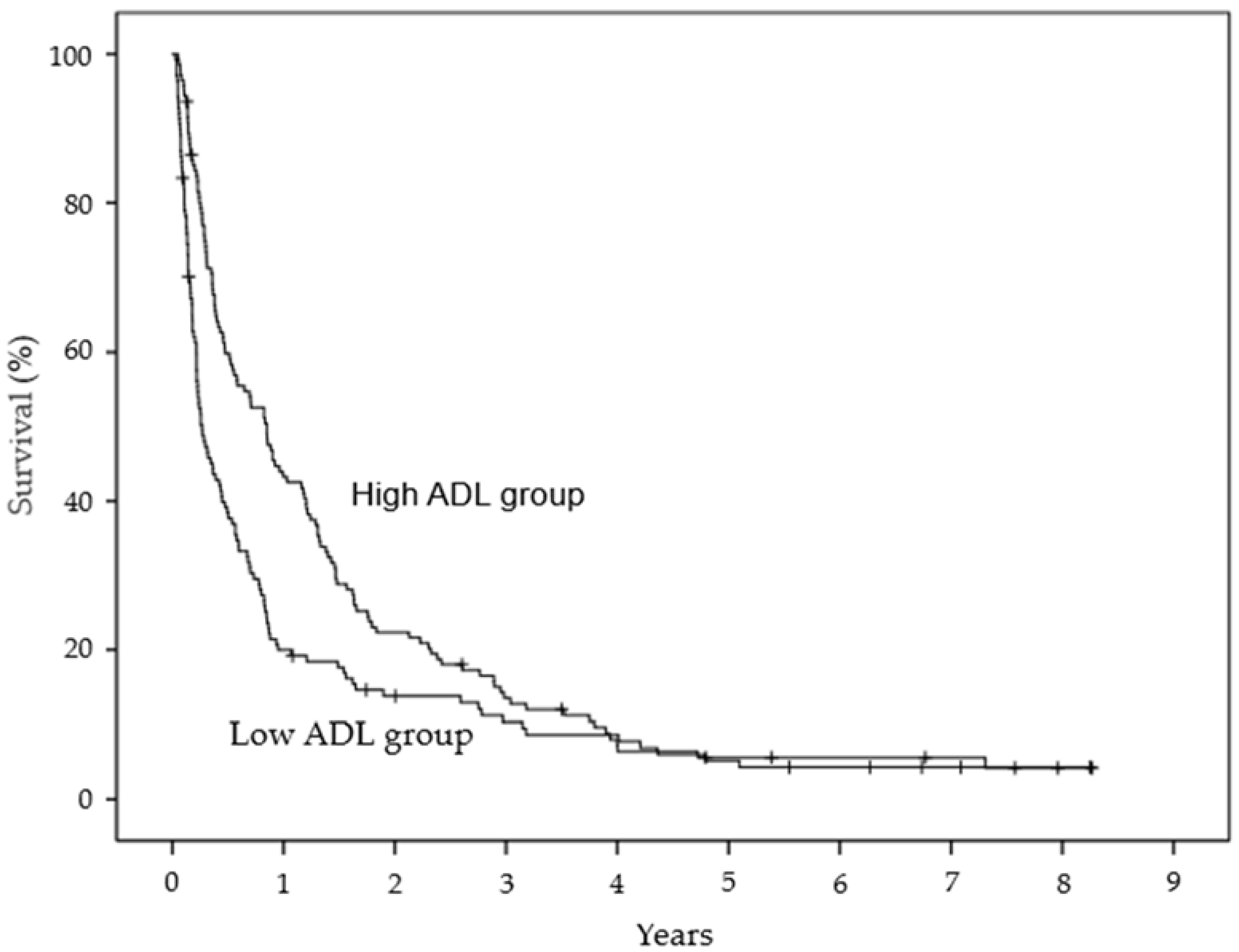
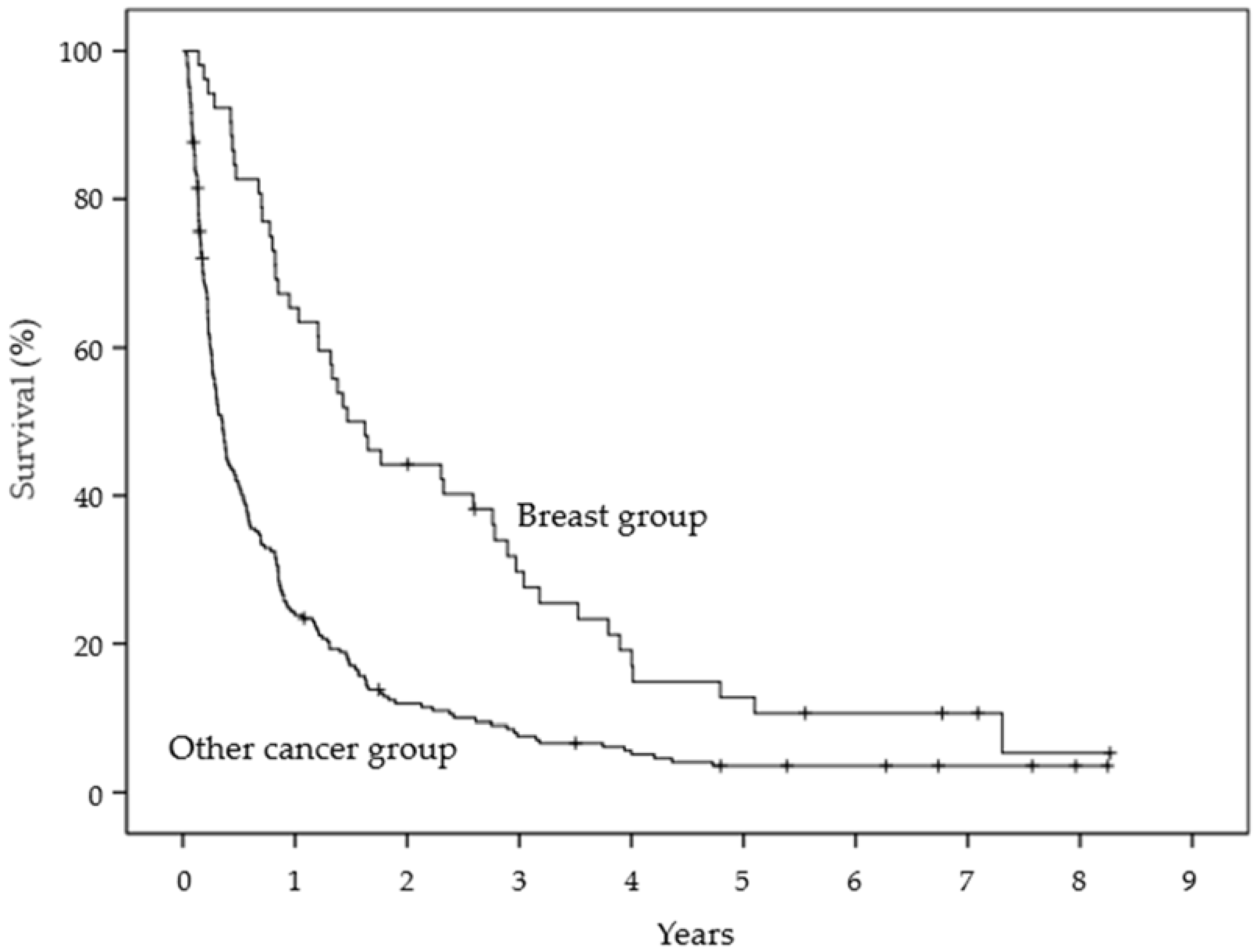
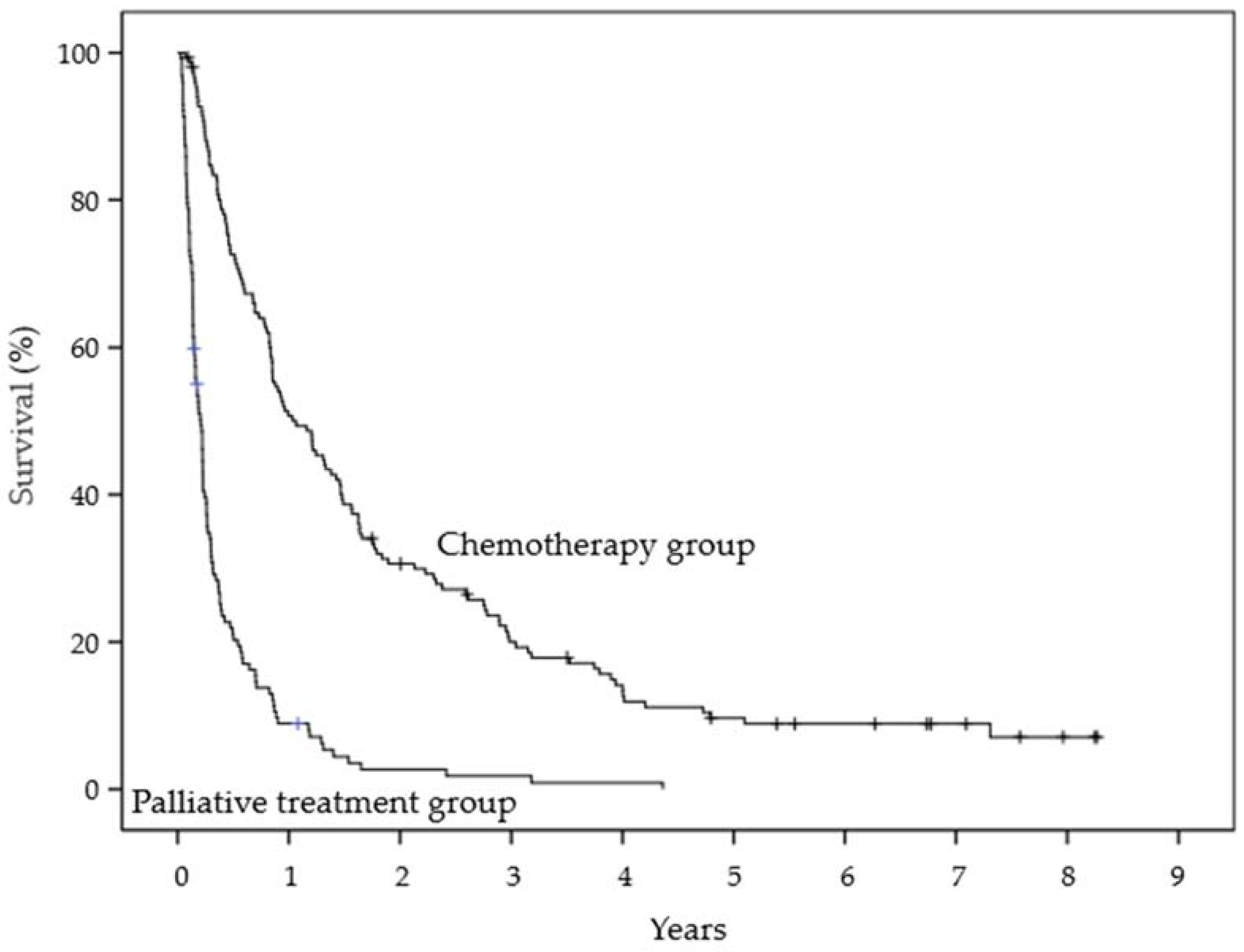
3.2. Univariate Analysis
3.3. Factors Affecting OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coleman, R.E. Clinical Features of Metastatic Bone Disease and Risk of Skeletal Morbidity. Clin. Cancer Res. 2006, 12, 6243s–6249s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Oorschot, B.; Rades, D.; Schulze, W.; Beckmann, G.; Feyer, P. Palliative radiotherapy—New approaches. Semin. Oncol. 2011, 38, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, R.E. Skeletal complications of malignancy. Cancer 1997, 80, 1588–1594. [Google Scholar] [CrossRef]
- Hatoum, H.T.; Lin, S.J.; Smith, M.R.; Barghout, V.; Lipton, A. Zoledronic acid and skeletal complications in patients with solid tumors and bone metastases: Analysis of a national medical claims database. Cancer 2008, 113, 1438–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, P.S.; Buchowski, J.M. Metastatic disease in the thoracic and lumbar spine: Evaluation and management. J. Am. Acad. Orthop. Surg. 2011, 19, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janjan, N.; Lutz, S.T.; Bedwinek, J.M.; Hartsell, W.F.; Ng, A.; Pieters, R.S., Jr.; Ratanatharathorn, V.; Silberstein, E.B.; Taub, R.J.; Yasko, A.W.; et al. Therapeutic guidelines for the treatment of bone metastasis: A report from the American College of Radiology Appropriateness Criteria Expert Panel on Radiation Oncology. J. Palliat. Med. 2009, 12, 417–426. [Google Scholar] [CrossRef]
- Mitera, G.; Probyn, L.; Ford, M.; Donovan, A.; Rubenstein, J.; Finkelstein, J.; Christakis, M.; Zhang, L.; Campos, S.; Culleton, S.; et al. Correlation of computed tomography imaging features with pain response in patients with spine metastases after radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 827–830. [Google Scholar] [CrossRef]
- Wu, J.S.; Monk, G.; Clark, T.; Robinson, J.; Eigl, B.J.; Hagen, N. Palliative radiotherapy improves pain and reduces functional interference in patients with painful bone metastases: A quality assurance study. Clin. Oncol. 2006, 18, 539–544. [Google Scholar] [CrossRef]
- Van Oorschot, B.; Schuler, M.; Simon, A.; Schleicher, U.; Geinitz, H. Patterns of care and course of symptoms in palliative radiotherapy: A multicenter pilot study analysis. Strahlenther. Onkol. 2011, 187, 461–466. [Google Scholar] [CrossRef]
- Kang, E.J.; Lee, S.Y.; Kim, H.J.; Min, K.H.; Hur, G.Y.; Shim, J.J.; Kang, K.H.; Oh, S.C.; Seo, J.H.; Lee, S.Y.; et al. Prognostic Factors and Skeletal-Related Events in Patients with Small Cell Lung Cancer with Bone Metastases at the Time of Diagnosis. Oncology 2016, 90, 103–111. [Google Scholar] [CrossRef]
- Mizumoto, M.; Harada, H.; Asakura, H.; Hashimoto, T.; Furutani, K.; Hashii, H.; Murata, H.; Takagi, T.; Katagiri, H.; Takahashi, M.; et al. Radiotherapy for patients with metastases to the spinal column: A review of 603 patients at Shizuoka Cancer Center Hospital. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Rief, H.; Muley, T.; Bruckner, T.; Welzel, T.; Rieken, S.; Bischof, M.; Lindel, K.; Combs, S.E.; Debus, J. Survival and prognostic factors in non-small cell lung cancer patients with spinal bone metastases: A retrospective analysis of 303 patients. Strahlenther. Onkol. 2014, 190, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Palacios-Ceña, D.; Gómez-Calero, C.; Cachón-Pérez, J.M.; Brea-Rivero, M.; Gómez-Pérez, D.; Fernández-de-las-Peñas, C. Non-capable residents: Is the experience of dependence understood in nursing homes? A qualitative study. Geriatr. Gerontol. Int. 2014, 14, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Gastelurrutia, P.; Lupón, J.; Altimir, S.; de Antonio, M.; González, B.; Cabanes, R.; Rodríguez, M.; Urrutia, A.; Domingo, M.; Zamora, E.; et al. Fragility is a key determinant of survival in heart failure patients. Int. J. Cardiol. 2014, 175, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Foerster, R.; Bruckner, T.; Bostel, T.; Schlampp, I.; Debus, J.; Rief, H. Prognostic factors for survival of women with unstable spinal bone metastases from breast cancer. Radiat. Oncol. 2015, 10, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, C.G.; DiPaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; Chou, D.; et al. A novel classification system for spinal instability in neoplastic disease: An evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef] [Green Version]
- Van der Linden, Y.M.; Dijkstra, S.P.; Vonk, E.J.; Marijnen, C.A.; Leer, J.W. Prediction of survival in patients with metastases in the spinal column: Results based on a randomized trial of radiotherapy. Cancer 2005, 103, 320–328. [Google Scholar] [CrossRef]
- Ito, I.; Ito, K.; Takahashi, S.; Horibe, M.; Karita, R.; Nishizaka, C.; Nagai, T.; Hamada, K.; Sato, H.; Shindo, N. Association between bone scan index and activities of daily living in patients with advanced non-small cell lung cancer. Support. Care Cancer 2017, 25, 1779–1785. [Google Scholar] [CrossRef]
- Morishima, T.; Sato, A.; Nakata, K.; Matsumoto, Y.; Koeda, N.; Shimada, H.; Maruhama, T.; Matsuki, D.; Miyashiro, I. Barthel Index-based functional status as a prognostic factor in young and middle-aged adults with newly diagnosed gastric, colorectal and lung cancer: A multicentre retrospective cohort study. BMJ Open 2021, 11, e046681. [Google Scholar] [CrossRef]
- Nakata, E.; Sugihara, S.; Sugawara, Y.; Nakahara, R.; Furumatsu, T.; Tetsunaga, T.; Kunisada, T.; Nakanishi, K.; Akezaki, Y.; Ozaki, T. Multidisciplinary treatment system for bone metastases for early diagnosis, treatment and prevention of malignant spinal cord compression. Oncol. Lett. 2020, 19, 3137–3144. [Google Scholar] [CrossRef] [Green Version]
- Rief, H.; Omlor, G.; Akbar, M.; Welzel, T.; Bruckner, T.; Rieken, S.; Haefner, M.F.; Schlampp, I.; Gioules, A.; Habermehl, D.; et al. Feasibility of isometric spinal muscle training in patients with bone metastases under radiation therapy—First results of a randomized pilot trial. BMC Cancer 2014, 14, 67. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.Q.; Huang, J.F.; Lin, J.L.; Chen, L.; Zhou, T.T.; Chen, D.; Lin, D.D.; Shen, J.F.; Wu, A.M. Incidence, prognostic factors, and a nomogram of lung cancer with bone metastasis at initial diagnosis: A population-based study. Transl. Lung Cancer Res. 2019, 8, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Kong, P.; Yan, J.; Liu, D.; Ji, Y.; Wang, Y.; Zhuang, J.; Wang, J.; Hu, X.; Yue, X. Skeletal-related events and overall survival of patients with bone metastasis from nonsmall cell lung cancer—A retrospective analysis. Medicine 2017, 96, e9327. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnipper, L.E.; Smith, T.J.; Raghavan, D.; Blayney, D.W.; Ganz, P.A.; Mulvey, T.M.; Wollins, D.S. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: The top five list for oncology. J. Clin. Oncol. 2012, 30, 1715–1724. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Muñoz, A.; Pérez-Ruiz, E.; Sáez, M.I.; Trigo, J.M.; Galindo, M.M.; Manzaneque, L.; Jiménez, B.; Muros, B.; Alba, E. Limited impact of palliative chemotherapy on survival in advanced solid tumours in patients with poor performance status. Clin. Transl. Oncol. 2011, 13, 426–429. [Google Scholar] [CrossRef]
- Stanley, K.E. Prognostic factors for survival in patients with inoperable lung cancer. J. Natl. Cancer Inst. 1980, 65, 25–32. [Google Scholar] [PubMed]
- Pater, J.L.; Loeb, M. Nonanatomic prognostic factors in carcinoma of the lung: A multivariate analysis. Cancer 1982, 50, 326–331. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number |
|---|---|
| Primary cancer site | |
| Lung | 94 |
| Breast | 48 |
| Prostate | 30 |
| Colorectal | 23 |
| Stomach | 15 |
| Liver | 12 |
| Pancreatic | 8 |
| Others | 35 |
| ECOG PS | |
| 0 | 3 |
| 1 | 90 |
| 2 | 68 |
| 3 | 67 |
| 4 | 37 |
| Radiotherapy dose | |
| 8 Gy | 5 |
| 20 Gy | 47 |
| 24 Gy | 1 |
| 25 Gy | 2 |
| 25.2 Gy | 1 |
| 27 Gy | 1 |
| 29 Gy | 1 |
| 30 Gy | 179 |
| 32.5 Gy | 1 |
| 36 Gy | 1 |
| 37.5 Gy | 1 |
| 39 Gy | 1 |
| 40 Gy | 23 |
| 50 Gy | 1 |
| Skeletal-related events | |
| Vertebral bone fracture | 194 |
| Painful spinal bone metastases | 52 |
| Spinal cord compression | 19 |
| Variable | Non-Poor Prognosis Group | Poor Prognosis Group | p-Value |
|---|---|---|---|
| Age (y) | 66.0 ± 9.2 | 68.4 ± 11.8 | 0.051 |
| Sex (n) | 0.014 | ||
| Male | 61 (46%) | 82 (62%) | |
| Female | 71 (54%) | 51 (38%) | |
| Comorbidities (n) | 0.220 | ||
| Yes | 59 | 70 | |
| No | 73 | 63 | |
| ADL (n) | 0.002 | ||
| High ADL group | 78 (59%) | 53 (40%) | |
| Low ADL group | 54 (41%) | 80 (60%) | |
| Pain (scores) | 2.7 ± 3.2 | 3.8 ± 3.7 | 0.023 |
| Primary site (n) | p < 0.0001 | ||
| Breast cancer group | 42 (32%) | 6 (5%) | |
| Other cancer group | 90 (68%) | 127 (95%) | |
| Brain or visceral metastases (n) | 0.110 | ||
| Yes | 56 | 70 | |
| No | 76 | 63 | |
| Bone metastases other than the spine (n) | 0.388 | ||
| Yes | 56 | 64 | |
| No | 76 | 69 | |
| Spinal level of bone metastases (n) | 0.320 | ||
| Cervical and thoracic vertebrae group | 73 (55%) | 82 (62%) | |
| Lumbar vertebrae group | 59 (45%) | 51 (38%) | |
| Spinal instability (n) | 0.175 | ||
| Stable group | 65 (49%) | 54 (41%) | |
| Unstable group | 67 (51%) | 79 (59%) | |
| Treatment strategy (n) | p < 0.0001 | ||
| Chemotherapy group | 104 (79%) | 35 (26%) | |
| Palliative treatment group | 28 (21%) | 98 (74%) |
| Variable | B | Standard Error | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 0.017 | 0.015 | 1.017 (0.987–1.048) | 0.272 |
| Sex | −0.093 | 0.342 | 0.911 (0.466–1.780) | 0.785 |
| ADL | 0.635 | 0.321 | 1.887 (1.005–3.543) | 0.048 |
| Pain | −0.046 | 0.045 | 0.955 (0.874–1.044) | 0.313 |
| Primary site | 1.743 | 0.558 | 5.714 (1.914–17.062) | 0.002 |
| Treatment strategy | 2.115 | 0.321 | 8.286 (4.421–15.531) | p < 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akezaki, Y.; Nakata, E.; Kikuuchi, M.; Sugihara, S.; Katayama, Y.; Katayama, H.; Hamada, M.; Ozaki, T. Association between Overall Survival and Activities of Daily Living in Patients with Spinal Bone Metastases. Healthcare 2022, 10, 350. https://doi.org/10.3390/healthcare10020350
Akezaki Y, Nakata E, Kikuuchi M, Sugihara S, Katayama Y, Katayama H, Hamada M, Ozaki T. Association between Overall Survival and Activities of Daily Living in Patients with Spinal Bone Metastases. Healthcare. 2022; 10(2):350. https://doi.org/10.3390/healthcare10020350
Chicago/Turabian StyleAkezaki, Yoshiteru, Eiji Nakata, Masato Kikuuchi, Shinsuke Sugihara, Yoshimi Katayama, Haruyoshi Katayama, Masanori Hamada, and Toshifumi Ozaki. 2022. "Association between Overall Survival and Activities of Daily Living in Patients with Spinal Bone Metastases" Healthcare 10, no. 2: 350. https://doi.org/10.3390/healthcare10020350
APA StyleAkezaki, Y., Nakata, E., Kikuuchi, M., Sugihara, S., Katayama, Y., Katayama, H., Hamada, M., & Ozaki, T. (2022). Association between Overall Survival and Activities of Daily Living in Patients with Spinal Bone Metastases. Healthcare, 10(2), 350. https://doi.org/10.3390/healthcare10020350