
Risk Assessment-Oriented Design of a Needle Insertion Robotic System for Non-Resectable Liver Tumors

 ,
,  , ,
, , 
Abstract
:1. Introduction
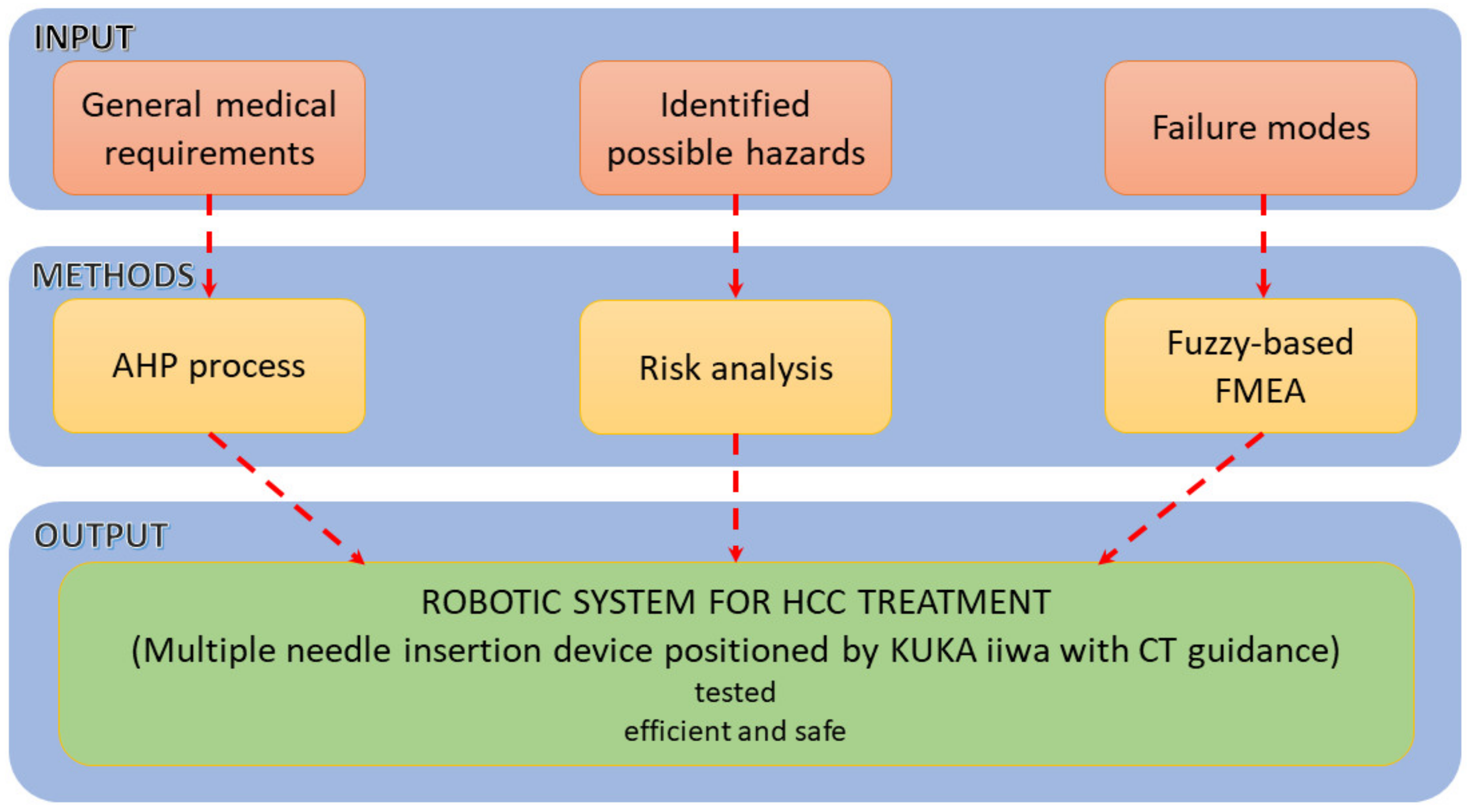
2. Materials and Methods
2.1. General Requirements
- The robotic system should be able to position the needle within a very tight space in the CT bore, above the patient’s abdominal cavity (functional requirement Func-01).
- 2.
- The robotic system should be able to provide a very accurate orientation of the needle inside the CT bore (functional requirement Func-02).
- 3.
- The robotic system should be able to position accurately the needles in a predetermined array (functional requirement Func-03).
- 4.
- The robotic system should be stiff enough to ensure a high precision (design requirement Des-01).
- 5.
- The robotic system should have a modular architecture for a broad variety of clinical applications (design requirement Des-02).
- 6.
- The needle insertion device should be sterilizable (design requirement Des-03).
- remove all electronics (including actuation motors) by designing it in such a way that it allows an easy connection/disconnection and removal.
- use sterilizable electronic equipment.
- 7.
- The robotic system should account for patient breathing (control requirement—Con-01).
- 8.
- The robotic system should account for the needle deflection (control requirement—Con-02).
- 9.
- Seamless integration within the clinical workflow (control requirement—Con-03).
2.2. The Solution
- Component 1 (A—CT scanner and B—external axis with 1 translational DoF)
- Component 2 (C—robotic system and D—MNID)
- Component 3 (E—stand and F—mobile platform that moves on a trajectory parallel with the moving table (couch) of the CT)
2.3. Risk Analysis
- Preplanning. Before performing the insertion procedure, based on an initial scan, a preplanning procedure is required, to define the safe needle insertion trajectories.
- Tumor’s registration. The patient, CT and the robotic system must run a registration procedure, where the position of the tumors is exactly defined within the robotic system coordinates. This is achieved using a set of metal markers (steel balls) fixed placed on the patient’s body.
- Needle trajectory definition. Based on the preplanning results and the final tumor’s position relative to the robotic system’s coordinates, each needle trajectory is defined.
- Needle insertion. The first needle in partially inserted up to a safe depth. A visual confirmation is required, using local CT scans, and thus, the needle trajectory is validated. In case the needle’s actual trajectory does not fit the predetermined one, the trajectory needs corrections. This means that the needle needs to be retracted and re-inserted using a new trajectory using the same target point into the tumor. If the needle trajectory is validated, another insertion depth is defined, and a second needle is taken from the needles rack and the entire procedure is repeated for each needle.
- Expected: 100;
- Quite possible: 80–99;
- Unusual, but possible: 50–79;
- Possible but unlikely: 30–49;
- Minor: 0–29.
- Catastrophic: 100;
- Critical: 80–99;
- Serious: 60–79;
- Moderate: 30–59;
- Negligible: 0–29.
- Critical >180;
- High: 150–179;
- Moderate: 120–149;
- Minor: 50–119;
- Negligible: 0–49.
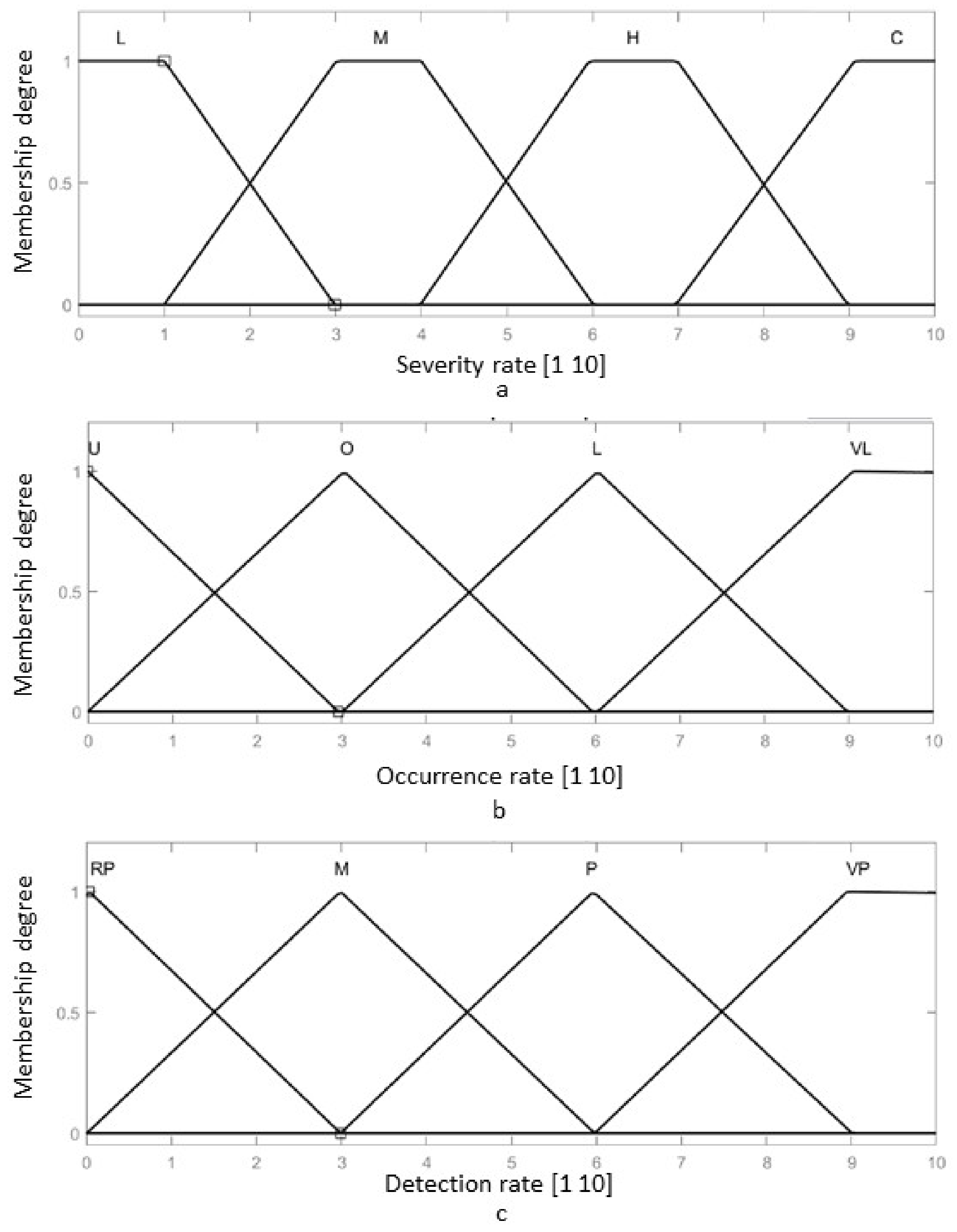
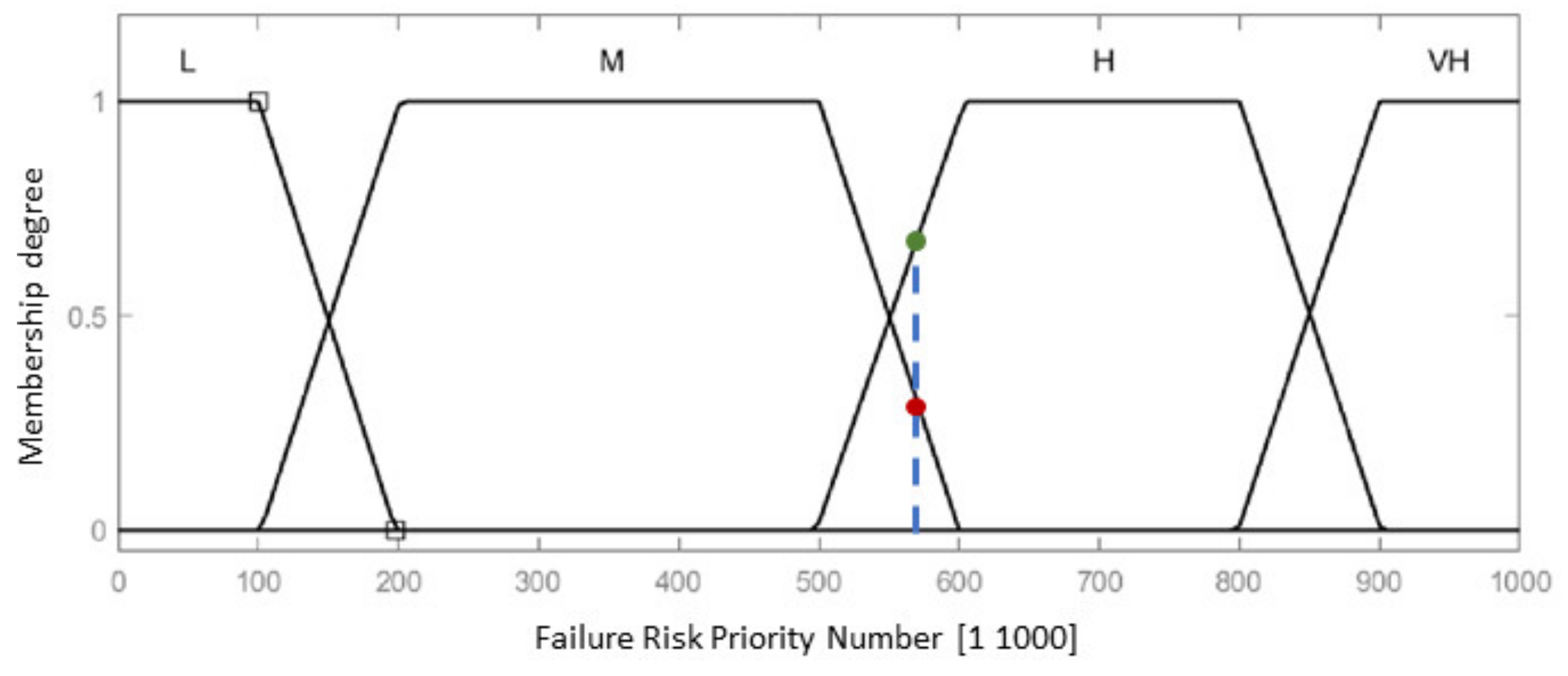
2.4. Failure Mode and Effect Analysis of the MNID
- Identify the subsystems of the selected system (if the case);
- Analyze the main functions of the components;
- Identify the breakdown modes of each element performing the MNID functions, their potential effect, cause and the means to resolve the issues and avoid the negative results;
- Assess the identified hazards in terms of severity, occurrence and detection and calculate the Risk Priority Number (RPN = severity × occurrence × detection scores).
- I.
- IF Severity is H AND Occurrence is O AND Detection is M THEN RPN is H
- II.
- IF Severity is H AND Occurrence is O AND Detection is VP THEN RPN is M
- III.
- IF Severity is H AND Occurrence is L AND Detection is VP THEN RPN is M
- IV.
- IF Severity is C AND Occurrence is L AND Detection is P THEN RPN is H
- V.
- IF Severity is H AND Occurrence is VL AND Detection is P THEN RPN is H
- VI.
- IF Severity is H AND Occurrence is O AND Detection is VP THEN RPN is L
- VII.
- IF Severity is H AND Occurrence is O AND Detection is RP THEN RPN is VH
- VIII.
- IF Severity is H AND Occurrence is VL AND Detection is VP THEN RPN is M
- IX.
- IF Severity is M AND Occurrence is L AND Detection is RP THEN RPN is VH
- X.
- IF Severity is M AND Occurrence is L AND Detection is VP THEN RPN is L
- XI.
- IF Severity is L AND Occurrence is VL AND Detection is VP THEN RPN is L
- XII.
- IF Severity is L AND Occurrence is L AND Detection is RP THEN RPN is VH
- XIII.
- IF Severity is L AND Occurrence is L AND Detection is M THEN RPN is H
- XIV.
- IF Severity is L AND Occurrence is L AND Detection is P THEN RPN is M
- XV.
- IF Severity is L AND Occurrence is VL AND Detection is VP THEN RPN is L
- XVI.
- IF Severity is M AND Occurrence is L AND Detection is RP THEN RPN is VH
- XVII.
- IF Severity is M AND Occurrence is L AND Detection is M THEN RPN is VH
- XVIII.
- IF Severity is M AND Occurrence is L AND Detection is P THEN RPN is H
- XIX.
- IF Severity is M AND Occurrence is L AND Detection is VP THEN RPN is L
- XX.
- IF Severity is C AND Occurrence is L AND Detection is VP THEN RPN is M
- XXI.
- IF Severity is C AND Occurrence is L AND Detection is P THEN RPN is VH
- XXII.
- IF Severity is C AND Occurrence is L AND Detection is VP THEN RPN is M
- XXIII.
- IF Severity is C AND Occurrence is VL AND Detection is P THEN RPN is H
- XXIV.
- IF Severity is C AND Occurrence is L AND Detection is RP THEN RPN is VH
- XXV.
- IF Severity is L AND Occurrence is O AND Detection is VP THEN RPN is L
- XXVI.
- IF Severity is H AND Occurrence is O AND Detection is P THEN RPN is H
- XXVII.
- IF Severity is M AND Occurrence is VL AND Detection is RP THEN RPN is VH
- XXVIII.
- IF Severity is H AND Occurrence is U AND Detection is VP THEN RPN is M
- XXIX.
- IF Severity is H AND Occurrence is U AND Detection is VP THEN RPN is M
- XXX.
- IF Severity is H AND Occurrence is O AND Detection is RP THEN RPN is H
3. Results
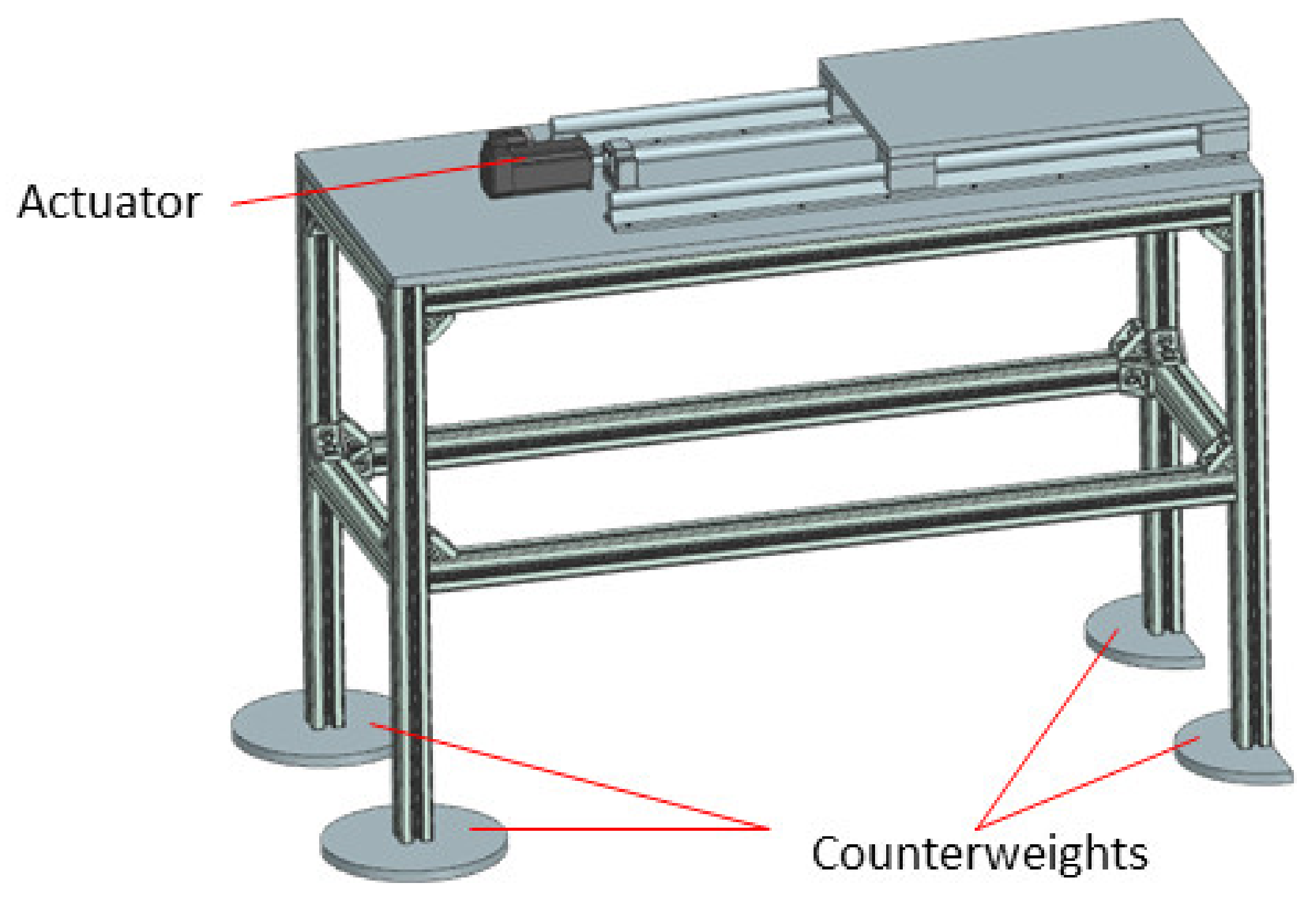
3.1. The Robotic System Design
3.2. The Control System
- User level, consisting of the KUKA smartPAD and the User Interface (PC);
- Control level, consisting of the KUKA Sunrise Cabinet and the PLC. The drivers used for the Nanotec stepper motors are also from B&R Automation, namely 80SD100XD.C011-01, each one being able to drive 2 motors;
- Physical level, consisting of the KUKA iiwa robot, the MNID and the 1 DoF axis, their actuators, and the sensory system. The latter consists of the proximity sensors used for the initialization procedure of each motion axis (and as stroke limiters) and the distance sensor from IFM.
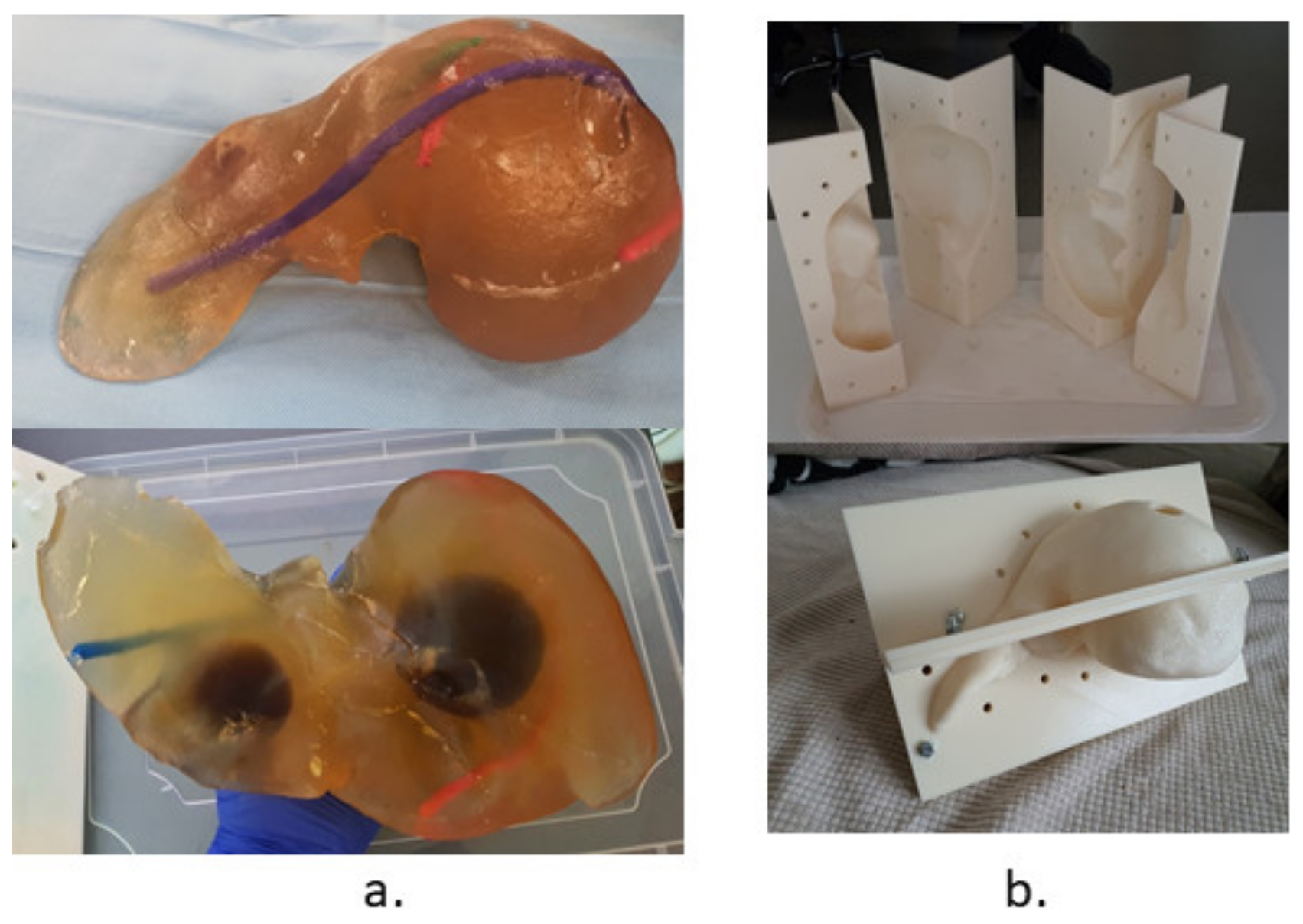
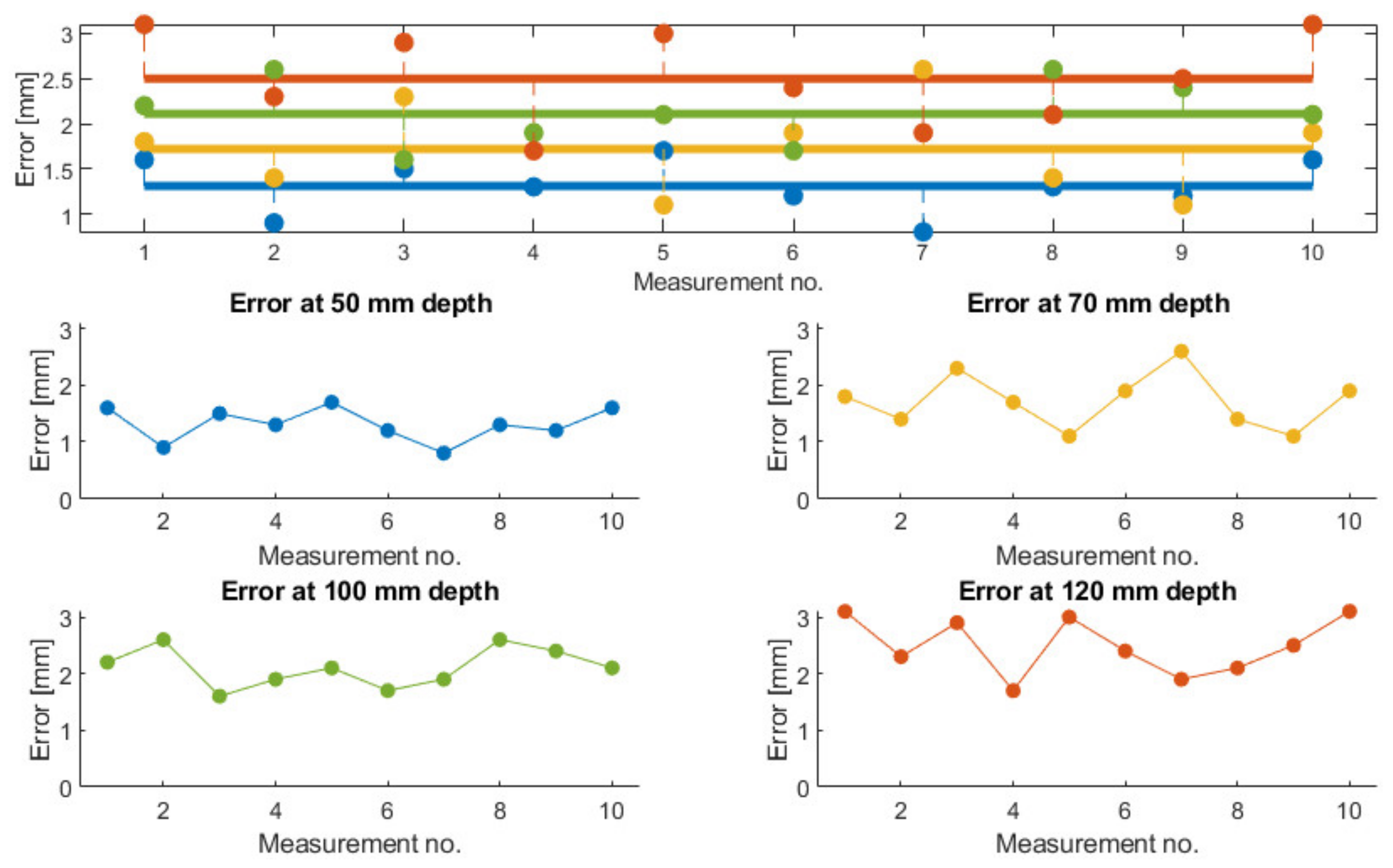
3.3. Validation Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, B. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level. JAMA Oncol. 2017, 3, 1683. [Google Scholar]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Wan, S.; Yang, Z.; Teschendorff, A.; Zou, Q. Tumor origin detection with tissue-specific miRNA and DNA methylation markers. Bioinformatics 2018, 34, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Zou, Q.; Xing, P.; Wei, L.; Liu, B. Gene2vec: Gene Subsequence Embedding for Prediction of Mammalian N6-Methyladenosine Sites from mRNA. RNA 2019, 25, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.; Yan, J.; Liu, D.; Li, X.; Kang, Q.; You, W.; Zhang, J.; Wang, L.; Tian, Z.; Lu, W.; et al. A nano-predator of pathological MDMX construct by clearable supramolecular gold(I)-thiol-peptide complexes achieves safe and potent anti-tumor activity. Theranostics 2021, 11, 6833–6846. [Google Scholar] [CrossRef]
- Xu, Q.; Guo, Q.; Wang, C.X.; Zhang, S.; Wen, C.B.; Sun, T.; Peng, W.; Chen, J.; Li, W.H. Network differentiation: A computational method of pathogenesis diagnosis in traditional Chinese medicine based on systems science. Artif. Intell. Med. 2021, 118, 102134. [Google Scholar] [CrossRef]
- Pisla, D.; Gherman, B.; Plitea, N.; Gyurka, B.; Vaida, C.; Vlad, L.; Graur, F.; Radu, C.; Suciu, M.; Szilaghi, A.; et al. PARASURG hybrid parallel robot for minimally invasive surgery. Chirurgia 2011, 106, 619–625. [Google Scholar] [PubMed]
- Zhou, J.; Sun, H.; Wang, Z.; Cong, W.; Wang, J.; Zeng, M.; Zhou, W.; Bie, P.; Liu, L.; Wen, T.; et al. Guidelines for the Diagnosis and Treatment of Hepatocellular Carcinoma (2019 Edition). Liver Cancer 2020, 9, 682–720. [Google Scholar] [CrossRef]
- Feldbrügge, L.; Langenscheidt, A.; Krenzien, F.; Schulz, M.; Krezdorn, N.; Kamali, K.; Hinz, A.; Bartels, M.; Fikatas, P.; Schmelzle, M.; et al. Health-Related Quality of Life and Mental Health after Surgical Treatment of Hepatocellular Carcinoma in the Era of Minimal-Invasive Surgery: Resection versus Transplantation. Healthcare 2021, 9, 694. [Google Scholar] [CrossRef]
- Millson, C.; Considine, A.; Cramp, M.E.; Holt, A.; Hubscher, S.; Hutchinson, J.; Jones, K.; Leithead, J.; Masson, S.; Menon, K.; et al. Adult liver transplantation: A UK clinical guideline-part 1: Pre-operation. Frontline Gastroenterol. 2020, 11, 375–384. [Google Scholar] [CrossRef] [Green Version]
- Nadim, M. Selection for Liver Transplantation: Indications and Evaluation. Curr. Hepatol. Rep. 2020, 19, 203–212. [Google Scholar]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fábrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepat. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Raoul, J.L.; Forner, A.; Bolondi, L.; Cheung, T.T.; Kloeckner, R.; de Baere, T. Updated use of TACE for hepatocellular carcinoma treatment: How and when to use it based on clinical evidence. Cancer Treat Rev. 2019, 72, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Bang, A.; Dawson, L.A. Radiotherapy for HCC: Ready for prime time? JHEP Rep. 2019, 1, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraki, T.; Kamegawa, T.; Matsuno, T.; Sakurai, J.; Kirita, Y.; Matsuura, R.; Yamaguchi, T.; Sasaki, T.; Mitsuhashi, T.; Komaki, T.; et al. Robotically Driven CT-guided Needle Insertion: Preliminary Results in Phantom and Animal Experiments. Radiology 2017, 285, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unger, M.; Berger, J.; Melzer, A. Robot-Assisted Image-Guided Interventions. Front. Robot. AI 2021, 8, 664622. [Google Scholar] [CrossRef]
- Kettenbach, J.; Kronreif, G. Robotic systems for percutaneous needle-guided interventions. Minim Invasive Ther. Allied Technol. 2015, 24, 45–53. [Google Scholar] [CrossRef]
- Taylor, A.J.; Xu, S.; Wood, B.J.; Tse, Z.T.H. Origami Lesion-Targeting Device for CT-Guided Interventions. J. Imaging 2019, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Cornelis, F.; Takaki, H.; Laskhmanan, M.; Durack, J.C.; Erinjeri, J.P.; Getrajdman, G.I.; Maybody, M.; Sofocleous, C.T.; Solomon, S.B.; Srimathveeravalli, G. Comparison of CT Fluoroscopy-Guided Manual and CT-Guided Robotic Positioning System for In Vivo Needle Placements in Swine Liver. Cardiovasc. Interv. Radiol. 2015, 38, 1252–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-David, E.; Shochat, M.; Roth, I.; Nissenbaum, I.; Sosna, J.; Goldberg, S.N. Evaluation of a CT-Guided Robotic System for Precise Percutaneous Needle Insertion. J. Vasc. Interv. Radiol. 2018, 29, 1440–1446. [Google Scholar] [CrossRef]
- Seitz, P.K.; Baumann, B.; Johnen, W.; Lissek, C.; Seidel, J.; Bendl, R. Development of a Robot-Assisted Ultrasound-Guided Radiation Therapy (USgRT). Int. J. CARS 2020, 15, 491–501. [Google Scholar] [CrossRef]
- Lv, Z.; Chen, D.; Feng, H.; Zhu, H.; Lv, H. Digital Twins in Unmanned Aerial Vehicles for Rapid Medical Resource Delivery in Epidemics. IEEE Trans. Intell. Transp. Syst. 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Meng, Q.; Lai, X.; Yan, Z.; Su, C.Y.; Wu, M. Motion Planning and Adaptive Neural Tracking Control of an Uncertain Two-Link Rigid-Flexible Manipulator with Vibration Amplitude Constraint. IEEE Trans. Neural Netw. Learn Syst. 2021, 32, 1–15. [Google Scholar] [CrossRef]
- Komaki, T.; Hiraki, T.; Kamegawa, T.; Matsuno, T.; Sakurai, J.; Matsuura, R.; Yamaguchi, T.; Sasaki, T.; Mitsuhashi, T.; Okamoto, S.; et al. Robotic CT-guided out-of-plane needle insertion: Comparison of angle accuracy with manual insertion in phantom and measurement of distance accuracy in animals. Eur. Radiol. 2019, 30, 1342–1349. [Google Scholar] [CrossRef] [Green Version]
- Beeksma, B.; Truant, D.; Holloway, L.; Arumugam, S. An assessment of image distortion and CT number accuracy within a wide-bore CT extended field of view. Australas. Phys. Eng. Sci. Med. 2015, 38, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Shibata, T.; Iimuro, Y.; Yamamoto, Y.; Ikai, I.; Itoh, K.; Maetani, Y.; Ametani, F.; Kubo, T.; Konishi, J. CT-guided Transthoracic Percutaneous Ethanol Injection for Hepatocellular Carcinoma Not Detectable with US. Radiology 2002, 223, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Shibata, T.; Maetani, Y.; Kubo, T.; Itoh, K.; Togashi, K.; Hiraoka, M. Transthoracic percutaneous radiofrequency ablation for liver tumors in the hepatic dome. J. Vasc. Interv. Radiol. 2004, 15, 1323–1327. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Waterman, F.; Handler, J.; Gressen, E. Localization of linked 125I seeds in postimplant TRUS images for prostate brachytherapy dosimetry. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Gaponenko, E.V.; Rybak, L.A.; Virabyan, L.G. Analysis of Stiffness and Positioning Accuracy of a Tripod Robot. J. Mach. Manuf. Reliab. 2020, 49, 16–23. [Google Scholar] [CrossRef]
- Thuemmler, C.; Mival, O.; Benyon, D.; Buchanan, W.; Paulin, A.; Fricker, S.; Fiedler, M.; Grottland, A.; Jell, T.; Magedanz, T.; et al. Norms and standards in modular medical architectures. In Proceedings of the 15th International Conference on e-Health Networking, Applications and Services (Healthcom 2013), Lisbon, Portugal, 9–12 October 2013; pp. 382–387. [Google Scholar]
- Nedezki, C.M. Singularities study of the 3rts manipulator. Acta Techn. Nap. Ser. A Math. Mech. Eng. 2021, 64, 389–394. [Google Scholar]
- Pisla, D.; Birlescu, I.; Vaida, C.; Tucan, P.; Pisla, A.; Gherman, B.; Crisan, N.; Plitea, N. Algebraic modeling of kinematics and singularities for a prostate biopsy parallel robot. Proc. Rom. Acad. Ser. A 2019, 19, 489–497. [Google Scholar]
- Antal, T.A.; Antal, A. The Use of Genetic Algorithms for the Design of Mechatronic Transmissions with Improved Operating Conditions. In Proceedings of the 3rd International Conference on Human System Interaction, Rzeszow, Poland, 13–15 May 2010; pp. 63–66. [Google Scholar]
- Gherman, B.; Vaida, C.; Pisla, D.; Plitea, N.; Gyurka, B.; Lese, D.; Glogoveanu, M. Singularities and workspace analysis for a parallel robot for minimally invasive surgery. In Proceedings of the 2010 IEEE International Conference on Automation, Quality and Testing, Robotics (AQTR), Cluj-Napoca, Romania, 28–30 May 2010; pp. 1–6. [Google Scholar] [CrossRef]
- Mohapatra, S. Sterilization and Disinfection. Essent. Neuroanesthesia 2017, 929–944. [Google Scholar] [CrossRef]
- Fahmi, S.; Simonis, F.F.J.; Abayazid, M. Respiratory motion estimation of the liver with abdominal motion as a surrogate. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1940. [Google Scholar]
- Kesner, A.L.; Chung, J.H.; Lind, K.E.; Kwak, J.J.; Lynch, D.; Burckhardt, D.; Koo, J. Validation of Software Gating: A Practical Technology for Respiratory Motion Correction in PET. Radiology 2016, 281, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Che, D.; Pallav, K.; Ehmann, K. Models of the cutting edge geometry of medical needles with applications to needle design. Int. J. Mech. Sci. 2012, 65, 157–167. [Google Scholar] [CrossRef]
- Ilami, M.; Ahmed, R.J.; Petras, A.; Beigzadeh, B.; Marvi, H. Magnetic Needle Steering in Soft Phantom Tissue. Sci. Rep. 2020, 10, 2500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corciova, C.; Andritoi, D.; Luca, C. A Modern approach for maintenance prioritization of medical equipment. In Operations Management-Emerging Trend in the Digital Era; IntechOpen: London, UK, 2020. [Google Scholar] [CrossRef]
- Popescu, S.; Rusu, D.; Dragomir, M.; Popescu, D.; Nedelcu, Ș. Competitive Development Tools in Identifying Efficient Educational Interventions for Improving Pro-Environmental and Recycling Behavior. Int. J. Environ. Res. Public Health 2020, 17, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherman, B.; Birlescu, I.; Burz, A.; Ulinici, I.; Tucan, P.; Pisla, D. Kinematic analysis of two innovative medical instruments for the robotic assisted treatment of non-resectable liver tumors. In European Conference on Mechanism Science; Pisla, D., Corves, B., Vaida, C., Eds.; Springer: Cham, Switzerland, 2020; Volume 89, pp. 189–197. [Google Scholar]
- Vaida, C.; Pisla, D.; Schadlbauer, J.; Husty, M.; Plitea, N. Kinematic Analysis of an Innovative Medical Parallel Robot Using Study Parameters. In New Trends in Medical and Service Robots: Human Centered Analysis, Control and Design; Springer: Cham, Switzerland, 2016; pp. 85–99. [Google Scholar]
- Klodmann, J.; Schlenk, C.; Hellings-Kuß, A.; Bahls, T.; Unterhinninghofen, R.; Albu-Schäffer, A.; Hirzinger, G. An Introduction to Robotically Assisted Surgical Systems: Current Developments and Focus Areas of Research. Curr. Robot Rep. 2021, 2, 321–332. [Google Scholar] [CrossRef]
- Rausand, M.; Hoylan, A. System reliability theory: Models, statistical methods, and applications. In Wiley Series in Probability and Statistics, 2nd ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Skowronek, J. Current status of brachytherapy in cancer treatment-short overview. J. Contemp. Brach. 2017, 9, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Pisla, D.; Cocorean, D.; Vaida, C.; Gherman, B.; Pisla, A.; Plitea, N. Application oriented design and simulation of an innovative parallel robot for brachytherapy. In Proceedings of the American Society of Mechanical Engineers, International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Buffalo, NY, USA, 17–20 August 2014. [Google Scholar] [CrossRef] [Green Version]
- Tucan, P.; Vaida, C.; Plitea, N.; Pisla, A.; Carbone, G.; Pisla, D. Risk-Based Assessment Engineering of a Parallel Robot Used in Post-Stroke Upper Limb Rehabilitation. Sustainability 2019, 11, 2893. [Google Scholar] [CrossRef] [Green Version]
- Fabis-Domagala, J.; Domagala, M.; Momeni, H. A Matrix FMEA Analysis of Variable Delivery Vane Pumps. Energies 2021, 14, 1741. [Google Scholar] [CrossRef]
- Ivančan, J.; Lisjak, D. New FMEA Risks Ranking Approach Utilizing Four Fuzzy Logic Systems. Machines 2021, 9, 292. [Google Scholar] [CrossRef]
- MATLAB. Available online: https://www.mathworks.com/ (accessed on 26 November 2021).
- Schonstein, C. Kinematic control functions for a serial robot structure based on the time derivative Jacobian matrix. Acta Tech. Nap. Ser. A Math. Mech. Eng. 2018, 61, 219–224. [Google Scholar]
- Suikkola, J.; Björninen, T.; Mosallaei, M.; Kankkunen, T.; Iso-Ketola, P.; Ukkonen, L.; Vanhala, J.; Mäntysalo, M. Screen-Printing Fabrication and Characterization of Stretchable Electronics. Sci. Rep. 2016, 6, 25784. [Google Scholar] [CrossRef]
- Gherman, B.; Birlescu, I.; Burz, A.; Pisla, D. Automated Medical Instrument for the Insertion of Brachytherapy Needles on Parallel Trajectories. Patent pending A00806/28, 28 November 2019. [Google Scholar]
- Tang, W.; Ye, X.; Dong, S. Research on site measuring uncertainty of the laser tracker, Proc. SPIE 9282. In Proceedings of the 7th International Symposium on Advanced Optical Manufacturing and Testing Technologies: Optical Test and Measurement Technology and Equipment 92821Q, Harbin, China, 18 September 2014. [Google Scholar] [CrossRef]
- Herbuś, K. Creating an integrated model of a technical system with use of the mechatronic features. In Modelling in Engineering 2020: Applied Mechanics. SMWM 2020. Advances in Intelligent Systems and Computing; Mężyk, A., Kciuk, S., Szewczyk, R., Duda, S., Eds.; Springer: Cham, Switzerland, 2021; Volume 1336, pp. 73–82. [Google Scholar]
- Tucan, P.; Plitea, N.; Gherman, B.; Hajjar, N.A.; Radu, C.; Vaida, C.; Pisla, D. Experimental study regarding needle deflection in robotic assisted brachytherapy of hepatocellular carcinoma. In ROMANSY 23-Robot Design, Dynamics and Control. ROMANSY 2020. CISM International Centre for Mechanical Sciences (Courses and Lectures); Venture, G., Solis, J., Takeda, Y., Konno, A., Eds.; Springer: Cham, Switzerland, 2021; Volume 601. [Google Scholar] [CrossRef]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hazard | En1 | En2 | En3 | En4 | En5 | En6 | En7 | En8 | MD1 | MD2 | Mean Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 | 90 | 95 | 90 | 95 | 85 | 90 | 95 | 90 | 90 | 90 | 91 |
| M2 | 70 | 80 | 90 | 80 | 75 | 65 | 70 | 75 | 65 | 70 | 74 |
| M3 | 65 | 80 | 90 | 80 | 75 | 65 | 70 | 75 | 65 | 70 | 73.5 |
| M4 | 85 | 85 | 90 | 85 | 90 | 95 | 75 | 80 | 70 | 75 | 83 |
| M5 | 90 | 85 | 95 | 80 | 95 | 90 | 80 | 85 | 88 | 92 | 88 |
| M6 | 70 | 75 | 60 | 65 | 60 | 70 | 80 | 75 | 70 | 70 | 69.5 |
| E1 | 50 | 60 | 60 | 70 | 75 | 50 | 55 | 65 | 50 | 50 | 58.5 |
| E2 | 50 | 60 | 65 | 55 | 58 | 65 | 70 | 75 | 55 | 60 | 61.3 |
| E3 | 40 | 45 | 40 | 50 | 40 | 45 | 60 | 55 | 40 | 40 | 45.5 |
| T1 | 45 | 35 | 40 | 45 | 55 | 45 | 50 | 55 | 35 | 40 | 44.5 |
| I1 | 100 | 100 | 95 | 100 | 95 | 90 | 95 | 100 | 100 | 100 | 97.5 |
| V1 | 50 | 55 | 60 | 45 | 50 | 65 | 40 | 35 | 40 | 40 | 48 |
| V2 | 35 | 30 | 40 | 30 | 35 | 30 | 40 | 35 | 30 | 30 | 33.5 |
| ER1 | 30 | 40 | 45 | 40 | 45 | 30 | 35 | 40 | 35 | 35 | 37.5 |
| Hazard | En1 | En2 | En3 | En4 | En5 | En6 | En7 | En8 | MD1 | MD2 | Mean Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 | 90 | 95 | 85 | 90 | 80 | 85 | 80 | 90 | 95 | 95 | 88.5 |
| M2 | 85 | 85 | 90 | 85 | 80 | 90 | 80 | 75 | 75 | 75 | 82 |
| M3 | 85 | 85 | 90 | 85 | 80 | 90 | 80 | 75 | 75 | 75 | 82 |
| M4 | 100 | 100 | 100 | 100 | 100 | 95 | 100 | 100 | 100 | 100 | 99.5 |
| M5 | 100 | 95 | 100 | 95 | 100 | 90 | 100 | 95 | 95 | 95 | 96.5 |
| M6 | 80 | 85 | 75 | 70 | 85 | 70 | 65 | 75 | 75 | 70 | 75 |
| E1 | 80 | 85 | 80 | 70 | 75 | 70 | 65 | 70 | 75 | 70 | 74 |
| E2 | 100 | 95 | 100 | 90 | 95 | 100 | 95 | 90 | 95 | 100 | 96 |
| E3 | 75 | 70 | 75 | 70 | 85 | 80 | 80 | 75 | 70 | 65 | 74.5 |
| T1 | 60 | 55 | 50 | 55 | 55 | 50 | 60 | 55 | 55 | 50 | 54.5 |
| I1 | 70 | 75 | 70 | 80 | 80 | 85 | 70 | 70 | 65 | 70 | 73.5 |
| V1 | 80 | 85 | 80 | 90 | 85 | 70 | 80 | 85 | 70 | 65 | 79 |
| V2 | 50 | 45 | 45 | 40 | 50 | 55 | 40 | 45 | 40 | 40 | 45 |
| ER1 | 90 | 95 | 80 | 95 | 85 | 75 | 85 | 80 | 80 | 80 | 84.5 |
| Hazard | Score | Evaluation |
|---|---|---|
| M1 | 179.5 | High |
| M2 | 156 | High |
| M3 | 155.5 | High |
| M4 | 169.5 | High |
| M5 | 178.5 | High |
| M6 | 144.5 | Moderate |
| E1 | 132.5 | Moderate |
| E2 | 146.3 | Moderate |
| E3 | 119.5 | Minor |
| T1 | 99 | Minor |
| I1 | 153.5 | Moderate |
| V1 | 127 | Moderate |
| V2 | 78.5 | Minor |
| ER1 | 122 | Moderate |
| Hazard | Measure Taken to Reduce the Risk |
|---|---|
| M1 | Needle deflection is almost impossible to avoid but must be kept under certain limits. This is the main reason why the expected accuracy (~2.5 mm) is rather poor within these applications. This hazard is strongly related to the procedure control flow and the only way to avoid the negative effects of deflection is to carefully monitor the needle trajectory between two consecutive scans and decide if it still fits the required outcome in terms of final position within the tumor (if the radiation time or intensity can be adjusted accordingly) or if it hits vital tissue (e.g., important blood vessels), case in which it has to be removed and the trajectory adjusted. |
| M2 | Proximity sensors have been mounted on the MNID and the stroke of each axis is strictly monitored. The torques within the KUKA iiwa are also be monitored. Joint velocities are limited when the MNID approaches the patient. |
| M3 | Since KUKA iiwa is a collaborative robot, the torques are strictly monitored. Limit the ranges of motion of each axis and use proximity sensors. |
| M4 | An additional motion axis has been installed and programmed to use the signal of a distance sensor measuring the real-time displacement of the CT couch within the CT bore. |
| M5 | The needle rack has been designed to firmly hold up to 6 needles using elastic elements. The needle locations are numbered and sufficiently spaced. An artificial ventilation system will be used to strictly monitor the patient’s breathing, which allows the implementation of the motion gating strategy. |
| M6 | The gripper has been custom designed to grip the needles using a large area. Stroke limiters have been installed. |
| E1 | Low voltage components have been used and the proper regulated protection of the system has been installed. |
| E2 | A strict protocol has been developed, in which all functions of the robotic system are tested within the initialization phase. Signal monitoring is strictly monitored. Proper regulated protection has been used. |
| E3 | Use proper regulated protection for the system. |
| T1 | Avoid using parts that would create heat in contact with the patient. Avoid unnecessary contact with the patient in general. |
| I1 | CT scanning implies irradiation with X-rays. The focus here is to avoid unnecessary irradiation (e.g., fewer CT scans) and the strict delimitation of the CT scan range. Nevertheless, irradiation within this kind of procedure cannot be avoided. |
| V1 | Avoid resonance. Check for loose parts. |
| V2 | Check for loose parts. Use low friction materials (e.g., stainless steel screw with brass nut). |
| ER1 | Firmly hold the patient in the right position on the CT couch. Constantly check the tumor position. |
| Code | Function | Potential Failure Mode | Potential Failure Effect | Potential Cause | Recommended Actions |
|---|---|---|---|---|---|
| F1 | Needle gripping | Wrong needle is gripped | The insertion order may be disrupted. Other needles may fall from the rack | Wrong numbering, rack position changed, needle missing from the rack | Before starting the procedure check that all needles are in place, in the correct order. |
| F2 | Needle gripping | Inaccurate positioning | The needle does not reach the target point | The needle may move inside the gripper during insertion | Design the gripper to firmly grip the needles using specific dimension grooves. |
| F3 | Needle positioning | Reach the end of motion range | The needle does not reach the target point | Not enough stroke Lack of stroke limiters | Design properly the stroke lengths. Install stroke limiters |
| F4 | Needle positioning | Inaccurate positioning | The needle does not reach the target point | Play within the screw-nut mechanism | Use preloaded nuts. Check them after each 5 procedures |
| F5 | Needle insertion | Inaccurate positioning | The needle does not reach the target point | Needle slips inside the gripper | Design the gripper to block the slipping tendency |
| F6 | Needle insertion | Patient’s liver hemorrhage | Unexpected blood loss | Needle deflects from the imposed trajectory | Install force sensor to detect out of range insertion forces. |
| F7 | Needle insertion | Inaccurate positioning | Unexpected blood loss. The needle does not reach the target point | Current needle collides with previous inserted needles | Design the gripper to avoid accidental collisions. Use parallel trajectories. Insert first needle in “the middle of the tumor” |
| F8 | Needle insertion | Inaccurate positioning | The needle reaches the tumor, but not the imposed target point | Needle deflects from the imposed trajectory | Choose one of the following: remove and reinsert needle; recalculate the other needles trajectories; recalculate dosimetry |
| F9 | Needle retraction | Inaccurate positioning | After insertion, the needles move from the targeted lesion | The gripper collides with the previous inserted needles | Design the gripper jaws in a slight conical form. Install stroke limiters to control the gripper opening |
| RPN Value | Failure Risk Linguistic Variable |
|---|---|
| 0–200 | Low |
| 100–600 | Moderate |
| 500–900 | High |
| 800–1000 | Very High |
| Failure Mode | Severity | Occurrence | Detection | RPN Value |
|---|---|---|---|---|
| F1 | 6.3 | 3.1 | 6.2 | 648 |
| F2 | 8.1 | 6.4 | 8.1 | 503 |
| F3 | 3.2 | 5.5 | 8.4 | 305 |
| F4 | 7.1 | 5.7 | 4.7 | 739 |
| F5 | 7.9 | 7.2 | 6.4 | 669 |
| F6 | 9.8 | 5.8 | 4.3 | 763 |
| F7 | 9.1 | 7.9 | 7.5 | 578 |
| F8 | 6.2 | 9.1 | 8.3 | 419 |
| F9 | 8.4 | 6.9 | 6.6 | 674 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherman, B.; Hajjar, N.A.; Tucan, P.; Radu, C.; Vaida, C.; Mois, E.; Burz, A.; Pisla, D. Risk Assessment-Oriented Design of a Needle Insertion Robotic System for Non-Resectable Liver Tumors. Healthcare 2022, 10, 389. https://doi.org/10.3390/healthcare10020389
Gherman B, Hajjar NA, Tucan P, Radu C, Vaida C, Mois E, Burz A, Pisla D. Risk Assessment-Oriented Design of a Needle Insertion Robotic System for Non-Resectable Liver Tumors. Healthcare. 2022; 10(2):389. https://doi.org/10.3390/healthcare10020389
Chicago/Turabian StyleGherman, Bogdan, Nadim Al Hajjar, Paul Tucan, Corina Radu, Calin Vaida, Emil Mois, Alin Burz, and Doina Pisla. 2022. "Risk Assessment-Oriented Design of a Needle Insertion Robotic System for Non-Resectable Liver Tumors" Healthcare 10, no. 2: 389. https://doi.org/10.3390/healthcare10020389
APA StyleGherman, B., Hajjar, N. A., Tucan, P., Radu, C., Vaida, C., Mois, E., Burz, A., & Pisla, D. (2022). Risk Assessment-Oriented Design of a Needle Insertion Robotic System for Non-Resectable Liver Tumors. Healthcare, 10(2), 389. https://doi.org/10.3390/healthcare10020389