
Effect of a Community Gerontology Program on the Control of Metabolic Syndrome in Mexican Older Adults

 ,
,
Abstract
:1. Introduction
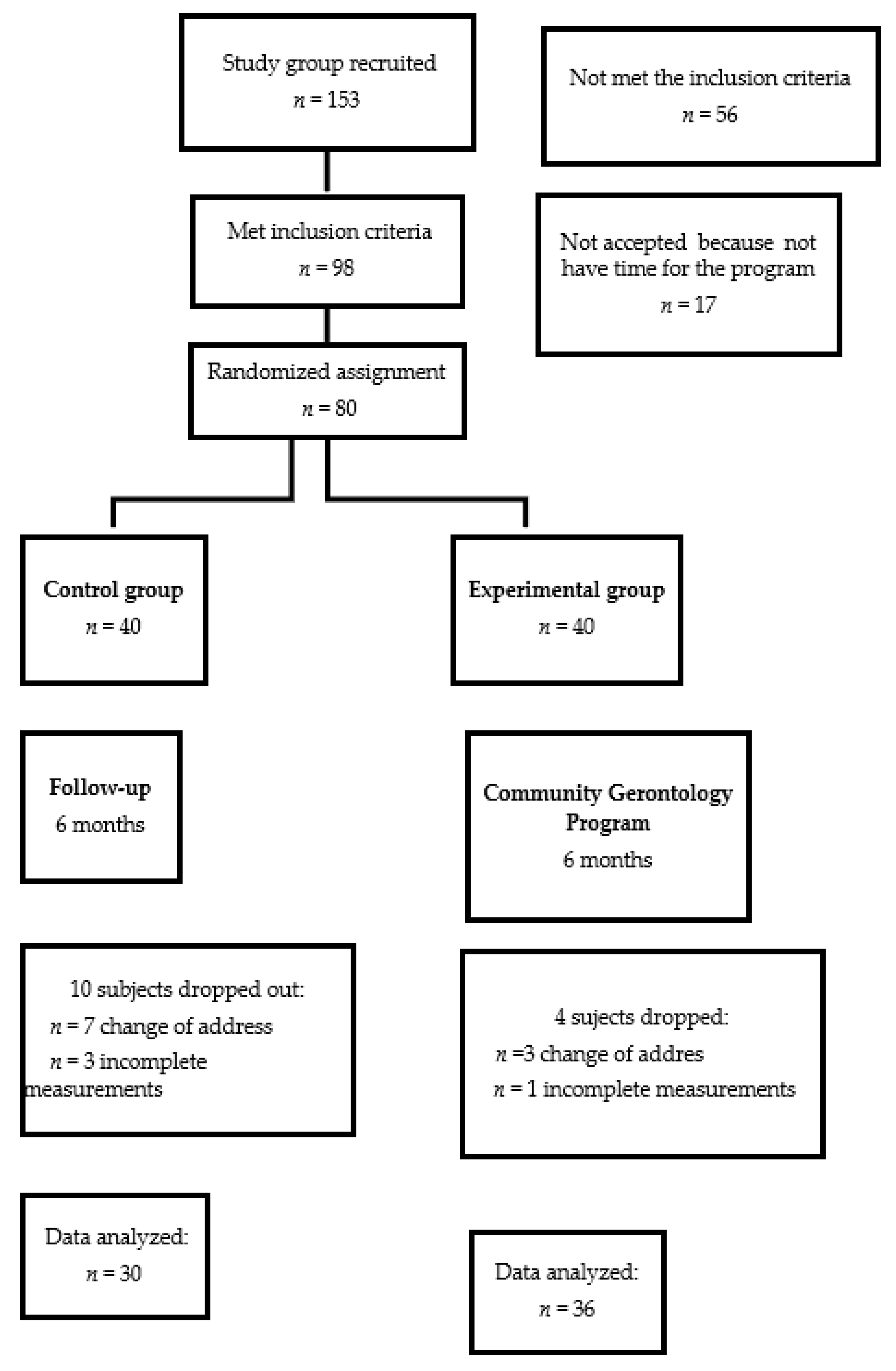
2. Materials and Methods
2.1. Clinical Assessment
2.2. Metabolic Syndrome Diagnosis
2.3. Biochemical Measurements
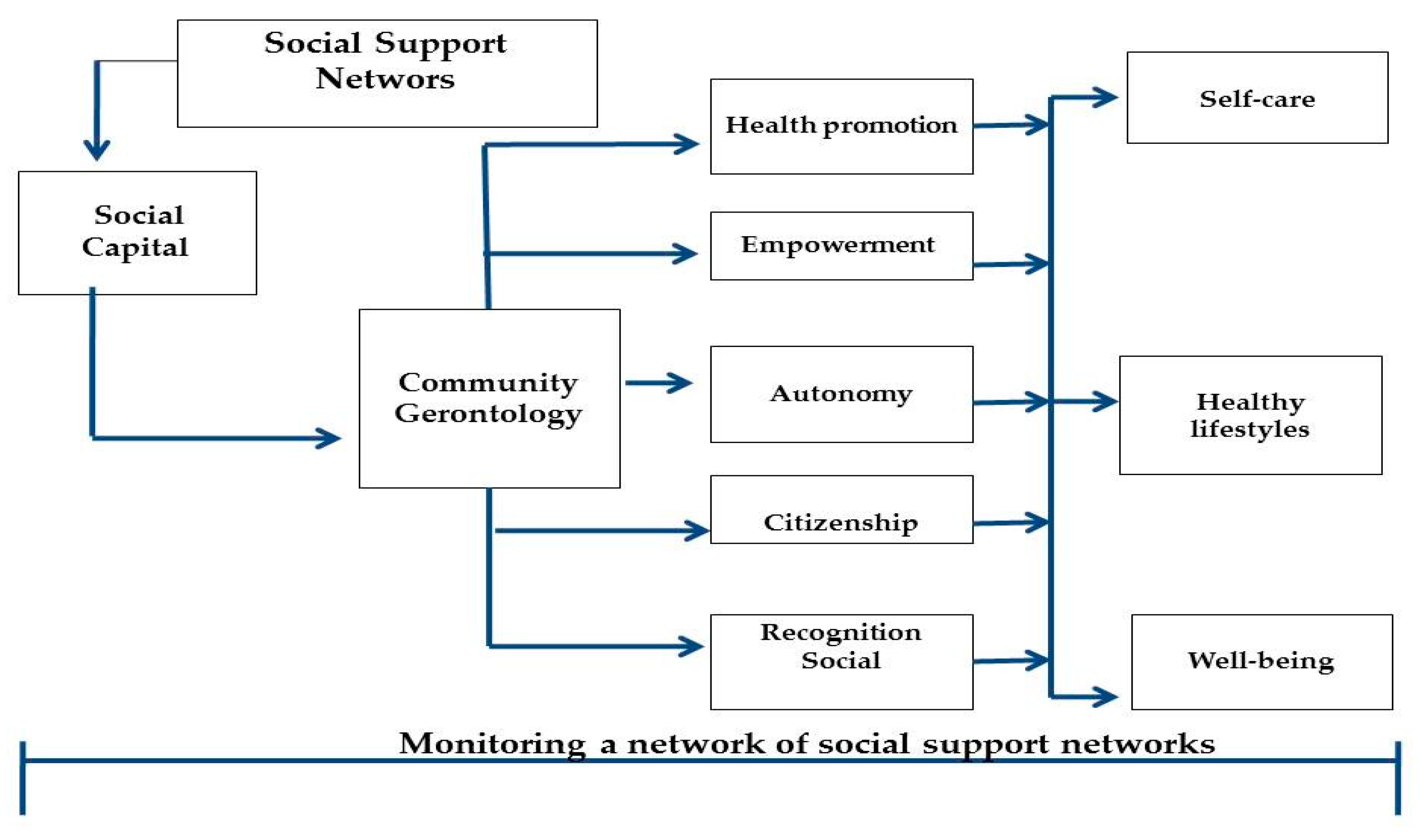
2.4. Community Gerontology Program (CGP)
2.5. Statistical Analysis
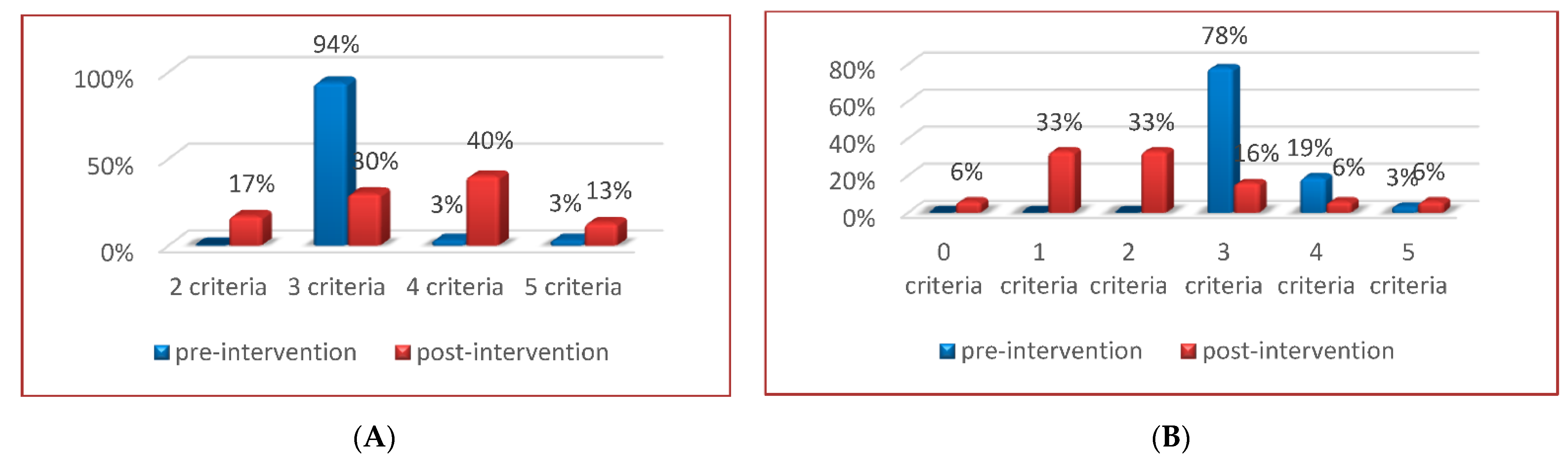
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, D.W.; LeRoith, D. Metabolic syndrome. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK278936/ (accessed on 20 October 2021).
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Solis, A.L.; Datta Banik, S.; Méndez-González, R.M. Prevalence of metabolic syndrome in Mexico: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2018, 16, 395–405. [Google Scholar] [CrossRef]
- Solano Jaurrieta, J.J. Síndrome metabólico y envejecimiento. Rev. Esp. Geriatr. Gerontol. 2009, 44, 335–341. [Google Scholar] [CrossRef]
- Cankurtaran, M.; Halil, M.; Yavuz, B.B.; Dagli, N.; Oyan, B.; Ariogul, S. Prevalence and correlates of metabolic syndrome (MS) in older adults. Arch. Gerontol. Geriatr. 2006, 42, 35–45. [Google Scholar] [CrossRef]
- Aguilar-Salinas, C.A.; Rojas, R.; Gómez-Pérez, F.J.; Valles, V.; Ríos-Torres, J.M.; Franco, A.; Olaiz, G.; Rull, J.A.; Sepúlveda, J. High prevalence of metabolic syndrome in Mexico. Arch. Med. Res. 2004, 35, 76–81. [Google Scholar] [CrossRef]
- Ortiz-Rodríguez, M.A.; Yáñez-Velasco, L.; Carnevale, A.; Romero-Hidalgo, S.; Bernal, D.; Aguilar-Salinas, C.; Rojas, R.; Villa, A.; Tur, J.A. Prevalence of metabolic syndrome among elderly Mexicans. Arch. Gerontol. Geriatr. 2017, 73, 288–293. [Google Scholar] [CrossRef]
- Zhang, W.; Zhao, Z.; Sun, X.; Tian, X. Prevalence of metabolic syndrome according to absolute and relative values of muscle strength in middle-aged and elderly women. Int. J. Environ. Res. Public Health 2021, 18, 9073. [Google Scholar] [CrossRef]
- Lee, D.-Y.; Shin, S. Sarcopenia Is Associated with Metabolic Syndrome in Korean Adults Aged over 50 Years: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1330. [Google Scholar] [CrossRef]
- Dao, H.H.H.; Nguyen, A.T.; Vu, H.T.T.; Nguyen, T.N. Examine the association between metabolic syndrome and frailty in an older asian population. Diabetology 2022, 3, 108–116. [Google Scholar] [CrossRef]
- Bahchevanov, K.M.; Dzhambov, A.M.; Chompalov, K.A.; Massaldjieva, R.I.; Atanassova, P.A.; Mitkov, M.D. Contribution of components of metabolic syndrome to cognitive performance in middle-aged adults. Arch. Clin. Neuropsychol. 2021, 36, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Smiley, A.; King, D.; Bidulescu, A. The association between sleep duration and metabolic syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef] [Green Version]
- Terschüren, C.; Damerau, L.; Petersen, E.L.; Harth, V.; Augustin, M.; Zyriax, B.C. Association of dietary pattern, lifestyle and chronotype with metabolic syndrome in elderly-lessons from the population-based Hamburg City Health Study. Int. J. Environ. Res. Public Health 2021, 19, 377. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, A.A.; Petersen, M.W.; Gormsen, L.K.; Skovbjerg, S.; Jørgensen, N.R.; Linneberg, A.; Cedeño-Laurent, J.G.; Jørgensen, T.; Dantoft, T.M. Insulin resistance is associated with multiple chemical sensitivity in a Danish population-based Study-Danfund. Int. J. Environ. Res. Public Health 2021, 18, 12654. [Google Scholar] [CrossRef] [PubMed]
- Rim, H.S.; Kim, M.G.; Park, D.C.; Kim, S.S.; Kang, D.W.; Kim, S.H.; Yeo, S.G. Association of metabolic syndrome with sensorineural hearing loss. J. Clin. Med. 2021, 10, 4866. [Google Scholar] [CrossRef]
- Chang, C.W.; Ke, H.L.; Lee, J.I.; Lee, Y.C.; Jhan, J.H.; Wang, H.S.; Shen, J.T.; Tsao, Y.H.; Huang, S.P.; Geng, J.H. Metabolic syndrome increases the risk of kidney stone disease: A cross-sectional and longitudinal cohort study. J. Pers. Med. 2021, 11, 1154. [Google Scholar] [CrossRef]
- Dunkley, A.J.; Charles, K.; Gray, L.J.; Camosso-Stefinovic, J.; Davies, M.J.; Khunti, K. Effectiveness of interventions for reducing diabetes and cardiovascular disease risk in people with metabolic syndrome: Systematic review and mixed treatment comparison meta-analysis. Diabetes Obes. Metab. 2012, 14, 616–625. [Google Scholar] [CrossRef]
- Guzmán, A.; Navarro, E.; Obando, L.; Pacheco, J.; Quirós, K.; Vásquez, L.; Castro, M.; Ramírez, F. Efectividad de las intervenciones para revertir el diagnóstico del síndrome metabólico: Actualización de un metaanálisis de comparación mixta de tratamientos. Biomedica 2019, 39, 647–662. [Google Scholar] [CrossRef]
- Martínez-Maldonado, M.L.; Correa-Muñoz, E.; Mendoza-Núñez, V.M. Program of active aging in a rural Mexican community: A qualitative approach. BMC Public Health 2007, 7, 276. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Rodríguez, M.A.; Arronte-Rosales, A.; Mendoza-Núñez, V.M. Effect of a self-care program on oxidative stress and cognitive function in an older Mexican urban-dwelling population. J. Nutr. Health Aging 2009, 13, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.M.; Sarmiento-Salmorán, E.; Marín-Cortés, R.; Martínez-Maldonado, M.L.; Ruiz-Ramos, M. Influence of the self-perception of old age on the effect of a healthy aging program. J. Clin. Med. 2018, 7, 106. [Google Scholar] [CrossRef] [Green Version]
- Arronte-Rosales, A.; Beltrán-Castillo, N.; Correa-Muñoz, E.; Martínez-Maldonado, M.L.; Mendoza-Núñez, V.M.; Rosado-Pérez, J.; Sánchez-Rodríguez, M.A.; Vargas-Guadarrama, L.A.; Vélez-Sagahón, F. Manual para la Evaluación Gerontológica Integral en la Comunidad, 2nd ed.; FES Zaragoza UNAM: Mexico City, Mexico, 2007. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.M.; Vivaldo-Martínez, M. Community gerontology model for healthy aging developed in Mexico framed in resilience and generativity. J. Cross. Cult. Gerontol. 2019, 34, 439–459. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.M.; Martínez-Maldonado, M.L.; Vargas-Guadarrama, L.A. Envejecimiento activo y saludable. In Fundamentos y Estrategias Desde la Gerontología Comunitaria; FES Zaragoza UNAM: Mexico City, Mexico, 2013. [Google Scholar]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition management in older adults with diabetes: A review on the importance of shifting prevention strategies from metabolic syndrome to frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Komleva, Y.; Chernykh, A.; Lopatina, O.; Gorina, Y.; Lokteva, I.; Salmina, A.; Gollasch, M. Inflamm-aging and brain insulin resistance: New insights and role of life-style strategies on cognitive and social determinants in aging and neurodegeneration. Front. Neurosci. 2021, 14, 618395. [Google Scholar] [CrossRef]
- Nisar, O.; Pervez, H.; Mandalia, B.; Waqas, M.; Sra, H.K. Type 3 diabetes mellitus: A link between Alzheimer’s disease and type 2 diabetes mellitus. Cureus 2020, 12, e11703. [Google Scholar] [CrossRef]
- Boothroyd, R.I.; Fisher, E.B. Peers for progress: Promoting peer support for health around the world. Fam. Pract. 2010, 27 (Suppl. 1), i62–i68. [Google Scholar] [CrossRef] [Green Version]
- Joensen, L.E.; Filges, T.; Willaing, I. Patient perspectives on peer support for adults with type 1 diabetes: A need for diabetes-specific social capital. Patient Prefer. Adherence 2016, 10, 1443–1451. [Google Scholar] [CrossRef] [Green Version]
- Joensen, L.E.; Meldgaard Andersen, M.; Jensen, S.; Nørgaard, K.; Willaing, I. The effect of peer support in adults with insulin pump-treated type 1 diabetes: A pilot study of a flexible and participatory intervention. Patient Prefer. Adherence 2017, 11, 1879–1890. [Google Scholar] [CrossRef] [Green Version]
- Mendoza-Núñez, V.M.; Martínez-Maldonado, M.L. Promoting successful aging in the community. In Cambridge Handbook of Successful Aging; Fernández-Ballesteros, R., Benetos, A., Robine, J.-M., Eds.; Cambridge University Press: Cambridge, UK, 2019; pp. 534–554. [Google Scholar]
- World Health Organization. Active Aging: A Policy Framework; WHO: Geneva, Switzerland, 2002; Available online: http://www.who.int/hpr/ageing/publications.htm (accessed on 22 July 2021).
- World Health Organization. World Report on Ageing and Health; WHO: Geneva, Switzerland, 2015; Available online: http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf1 (accessed on 22 July 2021).
- Wang, X.; Hsu, F.C.; Isom, S.; Walkup, M.P.; Kritchevsky, S.B.; Goodpaster, B.H.; Church, T.S.; Pahor, M.; Stafford, R.S.; Nicklas, B.J. Effects of a 12-month physical activity intervention on prevalence of metabolic syndrome in elderly men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Ballesteros, R.; Caprara, M.G.; Iñiguez, J.; García, L.F. Promoción del envejecimiento activo: Efectos del programa «Vivir con vitalidad»®. Rev. Esp. Geriatr. Gerontol. 2005, 40, 92–102. [Google Scholar] [CrossRef]
- Caprara, M.; Molina, M.Á.; Schettini, R.; Santacreu, M.; Orosa, T.; Mendoza-Núñez, V.M.; Rojas, M.; Fernández-Ballesteros, R. Active aging promotion: Results from the vital aging program. Curr. Gerontol. Geriatr. Res. 2013, 2013, 817813. [Google Scholar] [CrossRef] [Green Version]
- Caprara, M.; Fernández-Ballesteros, R.; Alessandri, G. Promoting aging well: Evaluation of Vital-Aging-Multimedia Program in Madrid, Spain. Health Promot. Int. 2016, 31, 515–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendoza-Ruvalcaba, N.M.; Fernández-Ballesteros, R. Effectiveness of the Vital Aging program to promote active aging in Mexican older adults. Clin. Interv. Aging 2016, 11, 1631–1644. [Google Scholar] [CrossRef] [Green Version]
- Jahangiry, L.; Shojaeizadeh, D.; Abbasalizad-Farhangi, M.; Yaseri, M.; Mohammad, K.; Najafi, M.; Montazeri, A. Interactive web-based lifestyle intervention and metabolic syndrome: Findings from the Red Ruby (a randomized controlled trial). Trials 2015, 16, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.H.; Chu, L.L.; Kao, C.C.; Chen, T.B.; Lee, I.; Li, H.C. The effects of a diet and exercise program for older adults with metabolic syndrome. J. Nurs. Res. 2015, 23, 197–205. [Google Scholar] [CrossRef]
- Martínez, M.I.; Ferri, A.; Mateos, A.M.; Alegre, A. Mejora de los parámetros clínicos en un paciente con síndrome metabólico mediante intervención en educación nutricional y mejora del estilo de vida. Nutr. Hosp. 2015, 31, 1444–1448. [Google Scholar]
- Papaioannou, K.G.; Kadi, F.; Nilsson, A. Benefits of fruit and vegetable consumption on prevalence of metabolic syndrome are independent of physical activity behaviors in older adults. Nutrients 2022, 14, 263. [Google Scholar] [CrossRef]
- Hermenegildo-López, Y.; Donat-Vargas, C.; Sandoval-Insausti, H.; Moreno-Franco, B.; Rodríguez-Ayala, M.; Rey-García, J.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. A higher intake of energy at dinner is associated with incident metabolic syndrome: A prospective cohort study in older adults. Nutrients 2021, 13, 3035. [Google Scholar] [CrossRef]
- Kim, K.; Jung, S.J.; Baek, J.M.; Yim, H.W.; Jeong, H.; Kim, D.J.; Park, S.; Youm, Y.; Kim, H.C. Associations between social network properties and metabolic syndrome and the mediating effect of physical activity: Findings from the Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) Cohort. BMJ Open Diabetes Res. Care 2020, 8, e001272. [Google Scholar] [CrossRef] [PubMed]
- Abbate, M.; Pericas, J.; Yañez, A.M.; López-González, A.A.; De Pedro-Gómez, J.; Aguilo, A.; Morales-Asencio, J.M.; Bennasar-Veny, M. Socioeconomic inequalities in metabolic syndrome by age and gender in a Spanish working population. Int. J. Environ. Res Public Health 2021, 18, 10333. [Google Scholar] [CrossRef] [PubMed]
- Atzeni, A.; Galié, S.; Muralidharan, J.; Babio, N.; Tinahones, F.J.; Vioque, J.; Corella, D.; Castañer, O.; Vidal, J.; Moreno-Indias, I.; et al. Gut microbiota profile and changes in body weight in elderly subjects with overweight/obesity and metabolic syndrome. Microorganisms 2021, 9, 346. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Chiou, J.M.; Chen, T.F.; Lai, L.C.; Chen, J.H.; Chen, Y.C. The association between metabolic syndrome and successful aging- using an extended definition of successful aging. PLoS ONE 2021, 16, e0260550. [Google Scholar] [CrossRef] [PubMed]
- Koutsogeorgou, E.; Kenneth Davies, J.; Aranda, K.; Zissi, A.; Chatzikou, M.; Cerniauskaite, M.; Quintas, R.; Raggi, A.; Matilde Leonardi, M. Healthy and active ageing: Social capital in health promotion. Health Educ. J. 2014, 73, 627–641. [Google Scholar] [CrossRef] [Green Version]
- Nyqvist, F.; Forsman, A.K. Healthy ageing: Focus on social capital. In Social Capital as a Health Resource in Later Life: The Relevance of Context; Springer: Dordrecht, The Netherlands, 2015. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Topic | Activity | Sessions per Week | Hours per Session | Total Sessions | Total Hours | |
|---|---|---|---|---|---|---|
| 1 | Active and healthy aging | Theoretical/debate | 1 | 2 | 3 | 6 |
| 2 | Healthy eating | Theoretical/practical | 1 | 2 | 3 | 6 |
| 3 | Safe physical exercise | Theoretical/practical | 1 | 2 | 3 | 6 |
| 4 | Personal and environmental hygiene | Theoretical/practical | 1 | 2 | 2 | 4 |
| 5 | Sleep hygiene | Theoretical/debate | 1 | 2 | 2 | 4 |
| 6 | Self-esteem vs. ageism | Theoretical/debate | 1 | 2 | 2 | 4 |
| 7 | Leisure and recreation | Theoretical/practical | 1 | 2 | 2 | 4 |
| 8 | Self-care for healthy aging | Theoretical/practical | 1 | 2 | 3 | 6 |
| 20 | 40 |
| Control Group n = 30 | Experimental Group n = 36 | |
|---|---|---|
| Age (mean ± SD) | 71 ± 9 | 69 ± 8 |
| Sex (%) | ||
| Men | 10 (33) | 8 (22) |
| Women | 20 (67) | 28 (78) |
| Civil status (%) | ||
| With couple | 9 (30) | 12 (33) |
| Without couple | 21 (70) | 24 (67) |
| Scholarship (years) | 7 ± 3 | 6 ± 3 |
| Socioeconomic level (%) | ||
| Low | 19 (63) | 25 (70) |
| Medium | 7 (23) | 8 (22) |
| High | 4 (14) | 3 (8) |
| Measurement | Control Group n = 30 (%) | Experimental Group n = 36 (%) | p Value |
|---|---|---|---|
| Pre-intervention | 3.1 ± 0.4 | 3.2 ± 0.5 | |
| Post-intervention | 3.5 ± 0.9 | 2.0 ± 1.2 | <0.001 |
| Control Group n = 30 | Experimental Group n = 36 | p Value | |
|---|---|---|---|
| Weight (kg) | |||
| Pre-intervention | 68 ± 12 | 71 ± 20 | |
| Post-intervention | 71 ± 10 | 66 ± 11 | 0.792 |
| Height (cm) | |||
| Pre-intervention | 158 ± 11 | 148 ± 8 | |
| Post-intervention | 157 ± 10 | 148 ± 7 | 0.997 |
| BMI (weight/height2) | |||
| Pre-intervention | 28 ± 5 | 32 ± 6 | |
| Post-intervention | 29 ± 3 | 30 ± 5 | 0.009 |
| Waist (cm) | |||
| Pre-intervention | 99 ± 10 | 104 ± 12 | |
| Post-intervention | 98 ± 9 | 102 ± 15 | 0.142 |
| Hip (cm) | |||
| Pre-intervention | 103 ± 10 | 108 ± 14 | |
| Post-intervention | 104 ± 10 | 105 ± 13 | 0.190 |
| SBP (mm Hg) | |||
| Pre-intervention | 128 ± 16 | 129 ± 14 | |
| Post-intervention | 132 ± 10 | 126 ± 20 | 0.047 |
| DBP (mm Hg) | |||
| Pre-intervention | 82 ± 8 | 85 ± 11 | |
| Post-intervention | 85 ± 9 | 81 ± 13 | 0.048 |
| Control Group n = 30 | Experimental Group n = 36 | p Value | |
|---|---|---|---|
| Glucose (mg/dL) | |||
| Pre-intervention | 118 ± 31 | 111 ± 20 | |
| Post-intervention | 124 ± 45 | 112 ± 32 | 0.164 |
| Urea (mg/dL) | |||
| Pre-intervention | 35 ± 7 | 35 ± 9 | |
| Post-intervention | 33 ± 8 | 37 ± 10 | 0.246 |
| Urate (mg/dL) | |||
| Pre-intervention | 5 ± 1 | 5 ± 2 | |
| Post-intervention | 6 ± 2 | 4 ± 1 | 0.080 |
| Cholesterol (mg/dL) | |||
| Pre-intervention | 206 ± 57 | 207 ± 44 | |
| Post-intervention | 211 ± 38 | 185 ± 19 | 0.140 |
| HDL (mg/dL) | |||
| Pre-intervention | 52 ± 12 | 56 ± 16 | |
| Post-intervention | 46 ± 9 | 63 ± 17 | 0.001 |
| Triglycerides (mg/dL) | |||
| Pre-intervention | 192 ± 78 | 177 ± 61 | |
| Post-intervention | 200 ± 90 | 139 ± 43 | 0.004 |
| Albumin (mg/dL) | |||
| Pre-intervention | 4.5 ± 0.23 | 4.5 ± 0.52 | |
| Post-intervention | 4.3 ± 0.51 | 4.3 ± 0.52 | 0.835 |
| Creatinine (mg/dL) | |||
| Pre-intervention | 0.91 ± 0.48 | 0.78 ± 0.20 | |
| Post-intervention | 0.78 ± 0.25 | 0.76 ± 0.32 | 0.207 |
| CRP (mg/dL) | |||
| Pre-intervention | 0.28 ± 0.39 | 0.47 ± 0.38 | |
| Post-intervention | 0.30 ± 0.47 | 0.41 ± 0.31 | 0.057 |
| MS Criteria | Control Group n = 30 (%) | Difference | Experimental Group n = 36 (%) | Difference | p Value |
|---|---|---|---|---|---|
| Abdominal circumference * | (5) | (−9) | |||
| Pre-intervention | 23 (78) | 33 (92) | |||
| Post-intervention | 25 (83) | 29 (81) | 0.125 | ||
| Glucose ≥ 110 mg/dL | (0) | (−9) | |||
| Pre-intervention | 17 (57) | 19 (53) | |||
| Post-intervention | 17 (57) | 15 (42) | 0.267 | ||
| SBP ≥ 130 mm Hg | (13) | (−33) | |||
| Pre-intervention | 14 (47) | 22 (61) | |||
| Post-intervention | 18 (60) | 10 (28) | 0.004 | ||
| DBP ≥ 85 mm Hg | (7) | (−34) | |||
| Pre-intervention | 18 (60) | 20 (56) | |||
| Post-intervention | 20 (67) | 8 (22) | 0.006 | ||
| Triglycerides ≥ 150 mg/dL | (−7) | (−11) | |||
| Pre-intervention | 26 (87) | 27 (75) | |||
| Post-intervention | 24 (80) | 13 (64) | 0.002 | ||
| HDL * | (27) | (−27) | |||
| Pre-intervention | 13 (43) | 16 (44) | |||
| Post-intervention | 21 (70) | 6 (17) | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza-Núñez, V.M.; Pulido-Castillo, G.; Correa-Muñoz, E.; Rosado-Pérez, J. Effect of a Community Gerontology Program on the Control of Metabolic Syndrome in Mexican Older Adults. Healthcare 2022, 10, 466. https://doi.org/10.3390/healthcare10030466
Mendoza-Núñez VM, Pulido-Castillo G, Correa-Muñoz E, Rosado-Pérez J. Effect of a Community Gerontology Program on the Control of Metabolic Syndrome in Mexican Older Adults. Healthcare. 2022; 10(3):466. https://doi.org/10.3390/healthcare10030466
Chicago/Turabian StyleMendoza-Núñez, Víctor Manuel, Gabriela Pulido-Castillo, Elsa Correa-Muñoz, and Juana Rosado-Pérez. 2022. "Effect of a Community Gerontology Program on the Control of Metabolic Syndrome in Mexican Older Adults" Healthcare 10, no. 3: 466. https://doi.org/10.3390/healthcare10030466
APA StyleMendoza-Núñez, V. M., Pulido-Castillo, G., Correa-Muñoz, E., & Rosado-Pérez, J. (2022). Effect of a Community Gerontology Program on the Control of Metabolic Syndrome in Mexican Older Adults. Healthcare, 10(3), 466. https://doi.org/10.3390/healthcare10030466