
True Brachial Artery Aneurysm in Patients with Previous Arterio-Venous Fistula Ligation and Immunosuppressant Therapy for Renal Transplantation: Case Report and Literature Review

 ,
,  and
and
Abstract
:1. Introduction
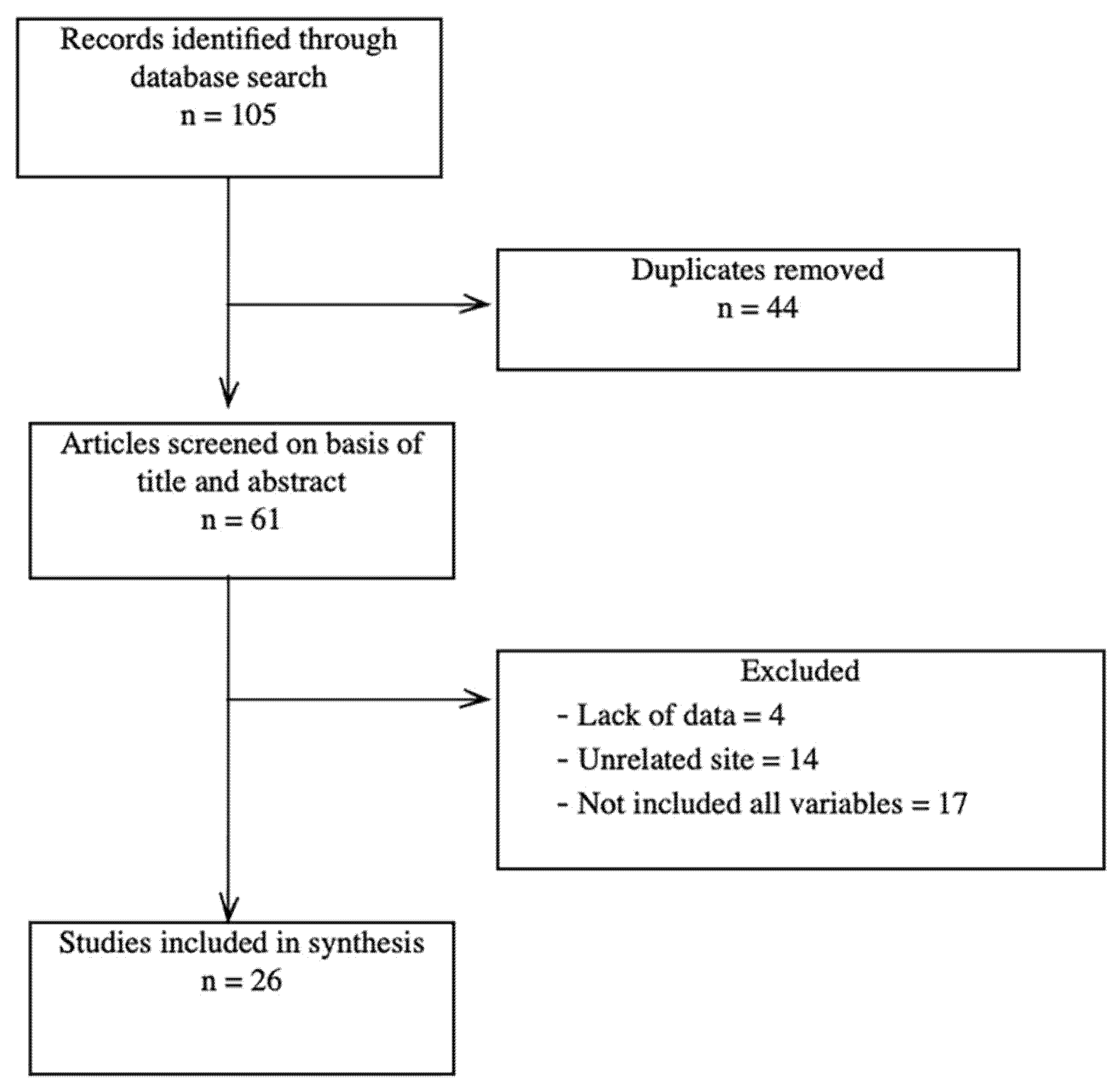
2. Materials and Methods
3. Results
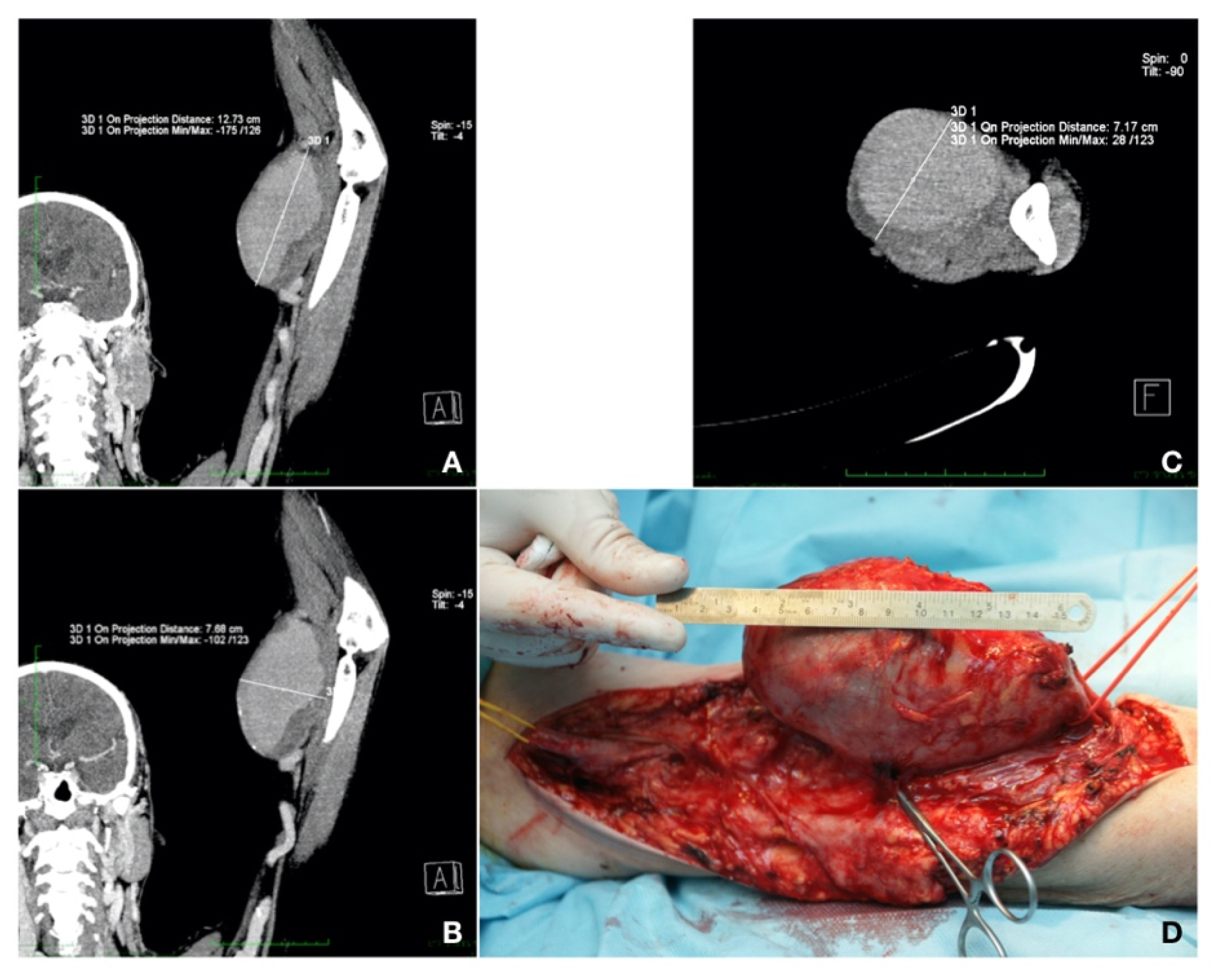
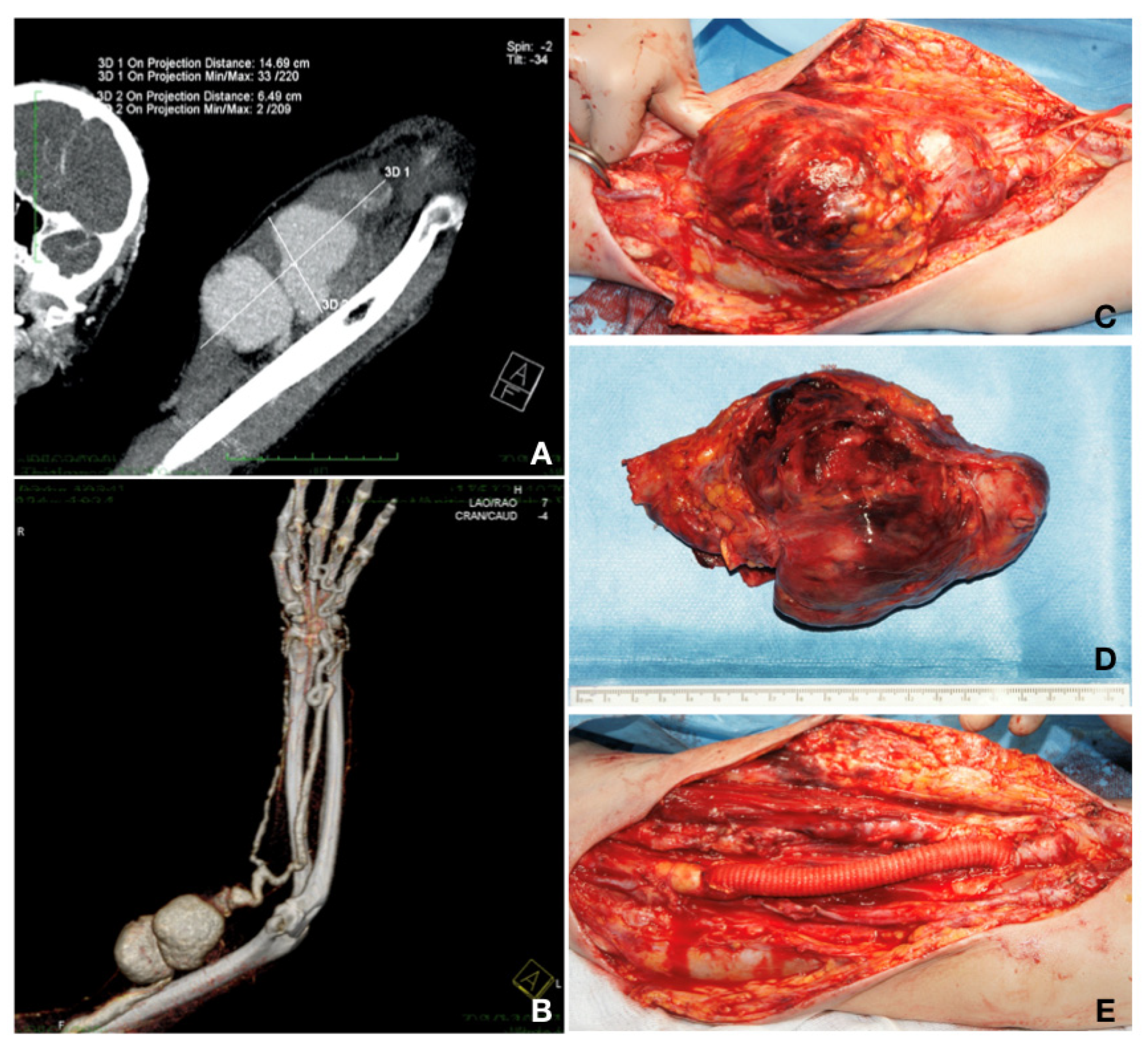
3.1. Case Reports
3.2. Evidence from the Literature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schunn, C.D.; Sullivan, T.M.B. Brachial arteriomegaly and true aneurysmal degeneration: Case report an litearture review. Vasc. Med. 2002, 7, 25–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyota, S.; Inoue, K.; Kurose, S.; Yoshino, S.; Nakayama, K.; Yamashita, S.; Morisaki, K.; Furuyama, T.; Mori, M. True brachial artery aneurysm after arteriovenous fistula closure following renal transplantation: A case report and literature review. Surg Case Rep. 2019, 5, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Report on Organ Donation and Transplantation Activities. Executive Summary. Available online: http://www.transplant-observatory.org/wpcontent/uploads/2019/11/glorep2017.pdf (accessed on 17 March 2020).
- Ferrara, D.; Di Filippo, M.; Spalla, F.; Giribono, A.M.; Viviani, E.; Santagata, A.; Bracale, U.; Santangelo, M.; del Guercio, L.; Bracale, U.M. Giant true brachial artery aneurysm after hemodialysis fistula closure in a renal transplant patient. Case Rep. Nephrol. Dial. 2016, 6, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Dinoto, E.; Bracale, U.M.; Vitale, G.; Cacciatore, M.; Pecoraro, F.; Cassaro, L.; Lo Momte, A.l.; Bajardi, G. Late giant brachial artery aneurysm following hemodialysis fistula ligation in a renal transplant patient: Case report and literature review. Gen. Thorac. Cardiovasc. Surg. 2012, 60, 768–770. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.J.; Stone, W.M.; Fowl, R.J.; Cherry, K.J.; Bower, T.C. Management of true aneurysms distal to the axillary artery. J. Vasc. Surg. 1998, 28, 606–610. [Google Scholar] [CrossRef] [Green Version]
- Barac, S.; Jiga, L.P.; Rata, A.; Sas, I.; Onofrei, R.R.; Ionac, M. Role of reconstructive microsurgery in tubal infertility in young women. J. Clin. Med. 2020, 9, 1300. [Google Scholar] [CrossRef] [PubMed]
- KDIGO Clinical Practice Guideline for Acute Kidney Injury. 2012. Available online: https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf (accessed on 17 March 2020).
- Lewington, A.; MacTier, R.; Hoefield, R.; Sutton, A.; Smith, D.; Downes, M. Clinical Practice Guideline. Available online: https://renal.org/wp-content/uploads/2017/06/Prevention_of_Contrast_Induced_Acute_Kidney_Injury_CI-AKI_In_Adult_Patients-1.pdf (accessed on 17 March 2020).
- Johnston, K.W.; Rutherford, R.B.; Tilson, M.D.; Shah, D.M.; Hollier, L.; Stanley, J.C. Suggested standards for reporting on arterial aneurysms. Sub- committee on Reporting Standards for Arterial Aneurysms Ad Hoc Committee on Reporting Standards Society for Vascular Surgery and North American Chapter International Society for Cardiovascular Surgery. J. Vasc. Surg. 1991, 13, 452–458. [Google Scholar] [PubMed] [Green Version]
- Nguyen, D.Q.A.; Ruddle, A.C.; Thompson, J.F. Late axillo-brachial arterial aneurysm following ligated Brescia-Cimino haemodialysis fistula. Eur. J. Vasc. Endovasc. Surg. 2001, 22, 381–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maynar, M.; Sanchez-Alvarez, E.; Qian, Z.; Lopez-Benitez, R.; Long, D.; Zerolo-Saez, I. Percutaneous Endovascular Treatment of a Brachial Artery Aneurysm. EJVES Extra 2003, 6, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, L.; Bucci, F.; Battaglia, M.; Reddler, A. Late occurrence of a large brachial artery aneurysm following closure of a hemodialysis arteriovenous fistula. Ann. Vasc. Surg. 2006, 20, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Ventura, M.; Perilli, L.; Pisani, F.; Cucciolillo, L.; Franceschini, E. True aneurysm of the brachial artery in a kidney transplant patient. J. Vasc. Endovasc. Surg. 2006, 13, 15–19. [Google Scholar]
- Murphy, J.; Bakran, A. Late acute presentation of a large brachial artery aneurysm following ligation of a Brescia-Cimino arteriovenous fistula. EJVES Extra 2009, 18, 73–75. [Google Scholar] [CrossRef] [Green Version]
- Chemla, E.; Nortley, M.; Morsy, M. Brachial Artery Aneurysms Associated with Arteriovenous Access for Hemodialysis. Semin. Dial. 2010, 23, 440–444. [Google Scholar] [CrossRef]
- Basile, C.; Antonelli, M.; Libutti, P.; Teutonico, A.; Casucci, F.; Lomonte, C. Is there a link between the late occurrence of a brachial artery aneurysm and the ligation of an arteriovenous fistula? Semin. Dial. 2010, 24, 341–342. [Google Scholar] [CrossRef] [PubMed]
- Marzelle, J.; Gashi, V.; Nguyen, H.D.; Mouton, A.; Becquemin, J.P.; Bourquelot, P. Aneurysmal degeneration of the donor artery after vascular access. J. Vasc. Surg. 2012, 55, 1052–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garza, R., 3rd; Dangleben, D.A.; Welkie, J.F. Brachial artery aneurysm with “blue finger syndrome” after ligation of a remote brachial artery-cephalic vein fistula. Vasc. Endovascular. Surg. 2013, 47, 479–481. [Google Scholar] [CrossRef]
- Bahia, S.S.; Tomei, F.; Ozdemir, B.A.; Chemla, E.S. Acute limb ischaemia due to focal brachial artery aneurysms complicating brachiocephalic arteriovenous fistula ligation: Two recent case reports. J. Vasc. Access 2014, 15, 427–430. [Google Scholar] [CrossRef]
- De Santis, F.; Martini, G.; Mani, G.; Bernhard, O. Diffuse Aneurysmal Degeneration of the Brachial Artery after Long-Standing High-Flow Arteriovenous Fistula Closure for Hemodialysis at Elbow Level. Ann. Vasc. Surg. 2014, 28, 1315.e11–1315.e15. [Google Scholar] [CrossRef]
- Kordzadeh, A.; Raquel, M.; D’Espiney, B.; Ahmad, A.S.; Hanif, M.A.; Panayiotopoulos, Y.P. Donor artery aneurysm formation following the ligation of haemodialysis arteriovenous fistula: A systematic review and case reports. J. Vasc. Access 2015, 16, 5–12. [Google Scholar] [CrossRef]
- Khalid, U.; Parkinson, F.; Mohiuddin, K.; Davies, P.; Woolgar, J. Brachial artery aneurysms following brachio-cephalic AV fistula ligation. J. Vasc. Access 2014, 15, 22–24. [Google Scholar] [CrossRef]
- Cleveland, E.C.; Sinno, S.; Sheth, S.; Sharma, S.; Mussa, F.F. Neurovascular compromise due to true brachial artery aneurysm at the site of a previously ligated arteriovenous fistula: Case report and review of literature. Vascular 2015, 23, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Fendri, J.; Palcau, L.; Cameliere, L.; Coffin, O.; Felisaz, A.; Gouicem, D.; Dufranc, J.; Laneelle, D.; Berger, L. True Brachial Artery Aneurysm after Arteriovenous Fistula for Hemodialysis: Five Cases and Literature Review. Ann. Vasc. Surg. 2017, 39, 228–235. [Google Scholar] [CrossRef]
- Gardiner, J.; Smout, J.; Torella, F. Repair of Access-Related Brachial Artery Aneurysm with Cadaveric Homograft: Mid-Term Follow-up. J. Vasc. Access 2016, 17, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Fernández, P.C.; Al-Sibbai, A.A.Z.; González, G.M.; Morrondo, J.A.C.; Alonso, P.M. Aneurisma humeral verdadero en relación con acceso vascular en paciente trasplantado renal: A propósito de 2 casos clínicos. Nefrologia 2017, 37, 96–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correia, M.; Marinho, A.; Mendes, C.; Antunes, L.; Gonçalves, Ó. True Brachial Artery Aneurysm in a Patient with Vascular Access for Haemodialysis and Kidney Graft. Rev. Port. Cir. Cardiotorac. Vasc. 2017, 24, 184. [Google Scholar] [PubMed]
- Soares, T.; Ferreira-Castro, R.; Neves, J.R.; Neto, M.; Sousa, J.; Pinto, J.P.; Gamas, L.; Cerquiera, A.; Sampaio, S.; Teixeira, J.G. True brachial artery aneurysm after arteriovenous fistula for hemodialysis—Case report. Rev. Port. Cir. Cadiotorac. Vasc. 2017, 24, 182. [Google Scholar]
- Giordano, G.; Giannikouris, I.E.; Vigano, S.; Bacchini, G. Vascular access donor artery dilatation: Considerations about the formation mechanism in immunosuppressed patient. J. Vasc. Access 2018, 19, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Aacleto, F.; Lima, P.; Gonçalves, A.; Gonçalves, O. Rupture of a true brachial artery aneurysm in a kidney transplant patient after arteriovenous fistula ligation: A rare presentation of an unusual disease. J. Vasc. Access 2019, 20, 107. [Google Scholar] [CrossRef]
- Anastasiadou, C.; Megalopoulos, A.; Tasiopoulou, K.; Intzos, V. A Rare Case of Brachial Artery Aneurysm Following Hemodialysis Fistula Ligation in a Transplanted Patient. Vasc. Endovasc. Surg. 2019, 53, 71–74. [Google Scholar] [CrossRef]
- Lee, H.Y.; Roh, Y.N.; Kim, H.T.; Park, U.J. Arterial Aneurysmal Degeneration with Venous Varicosity Following Ligation of an Arteriovenous Fistula in a Kidney Transplant Recipient. Vasc. Endovasc. Surg. 2019, 53, 242–245. [Google Scholar] [CrossRef]
- Fuente, R.G.; Brizuela, J.A.S.; Santiago, A.F.S.; Gutierrez, D.C.; San Norberto Garcia, E.M.; Puerta Vaquero, C. Aneurysmal degeneration of brachial artery in kidney transplant receptors after arteriovenous fistula ligation. Rev. Port. Cir. Cardiotorac. Vasc. 2015, 22, 109–113. [Google Scholar]
- Diwan, A.; Sarkar, R.; Stanley, J.C.; Zelenock, G.B.; Wakefield, T.W. Incidence of femoral and popliteal artery aneurysms in patients with abdominal aortic aneurysms. J. Vasc. Surg. 2000, 31, 863–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, W. The history of an aneurysm of the aorta with some remarks on aneurysms in general. Trans. Med. Obstet. Soc. Phys. Lond. 1757, 1, 323. [Google Scholar]
- Carroll, G.T.; McGloughlin, T.M.; Burke, P.E.; Egan, M.; Wallis, F.; Walsh, M.T. Wall shear stresses remain elevated in mature arteriovenous fistulas: A case study. J. Biomech. Eng. 2011, 133, 021003. [Google Scholar] [CrossRef]
- Buus, C.L.; Pourageaud, F.; Fazzi, G.E.; Janssen, M.J.; Mulvany, M.J.; De Mey, J.G.R. Smooth muscle cell changes during flow-related remodelling of rat mesenteric resistance arteries. Circ. Res. 2001, 89, 180–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, A.W.Y.; Yang, H.H.; Kim, J.M.; Sigrist, M.K.; Chum, E.; Gourlay, W.A.; Levin, A. Upregulation of matrix metalloproteinase-2 in the arterial vasculature contributes to stiffening and vasomotor dysfunction in patients with chronic kidney disease. Circulation 2009, 120, 792–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, J.M.; Savage, E.B.; Brophy, C.M.; Tilson, M.D. Hydrocortisone rapidly induces aortic rupture in a genetically susceptible mouse. Arch. Surg. 1990, 125, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Sato, O.; Takagi, A.; Miyata, T.; Takayama, Y. Aortic aneurysms in patients with autoimmune disorders treated with corticosteroids. Eur. J. Vasc. Endovasc. Surg. 1995, 10, 366–369. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Type of Fistula | No of Patients | % |
|---|---|---|
| Brachio-basilic | 1 | 1.78 |
| Brachio-cephalic | 24 | 42.85 |
| Radio-cephalic | 20 | 35.71 |
| Brachio-/Radio-cephalic | 1 | 1.78 |
| Not mentioned | 10 | 17.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barac, S.; Rata, A.L.; Popescu, A.I.; Onofrei, R.R.; Chiriac, S.D. True Brachial Artery Aneurysm in Patients with Previous Arterio-Venous Fistula Ligation and Immunosuppressant Therapy for Renal Transplantation: Case Report and Literature Review. Healthcare 2022, 10, 470. https://doi.org/10.3390/healthcare10030470
Barac S, Rata AL, Popescu AI, Onofrei RR, Chiriac SD. True Brachial Artery Aneurysm in Patients with Previous Arterio-Venous Fistula Ligation and Immunosuppressant Therapy for Renal Transplantation: Case Report and Literature Review. Healthcare. 2022; 10(3):470. https://doi.org/10.3390/healthcare10030470
Chicago/Turabian StyleBarac, Sorin, Andreea Luciana Rata, Alexandra Ioana Popescu, Roxana Ramona Onofrei, and Sorin Dan Chiriac. 2022. "True Brachial Artery Aneurysm in Patients with Previous Arterio-Venous Fistula Ligation and Immunosuppressant Therapy for Renal Transplantation: Case Report and Literature Review" Healthcare 10, no. 3: 470. https://doi.org/10.3390/healthcare10030470
APA StyleBarac, S., Rata, A. L., Popescu, A. I., Onofrei, R. R., & Chiriac, S. D. (2022). True Brachial Artery Aneurysm in Patients with Previous Arterio-Venous Fistula Ligation and Immunosuppressant Therapy for Renal Transplantation: Case Report and Literature Review. Healthcare, 10(3), 470. https://doi.org/10.3390/healthcare10030470