
Effects of Aquatic Exercises for Patients with Osteoarthritis: Systematic Review with Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Eligibility Criteria
2.2.1. Patients
2.2.2. Intervention
2.2.3. Comparator
2.2.4. Outcome
2.2.5. Inclusion and Exclusion Criteria
2.3. Information Sources, Search Strategy and Selection Process
2.3.1. Information Sources
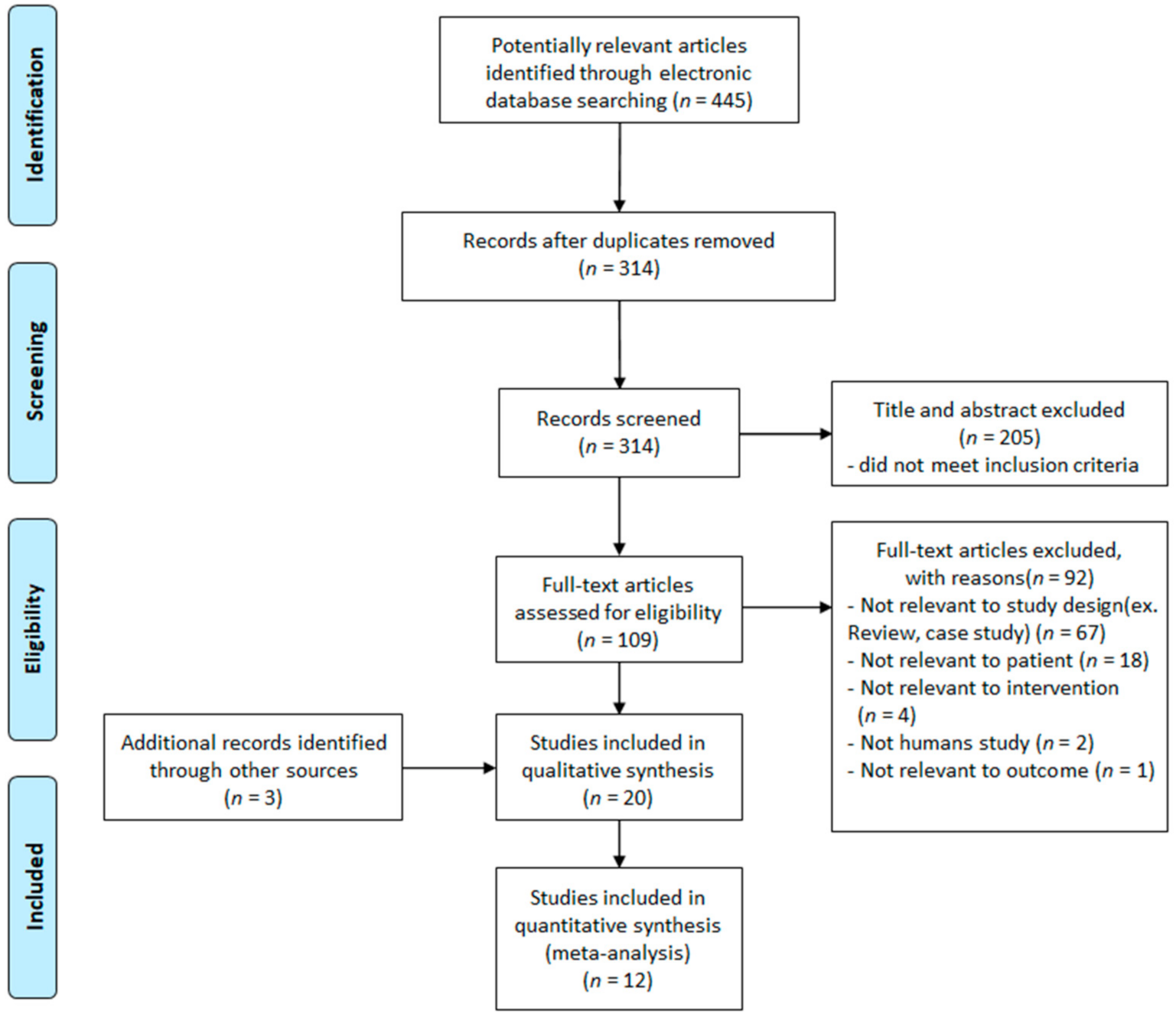
2.3.2. Search Strategy and Selection Process
2.4. Quality Assessment of Articles
2.5. Data Analysis
2.5.1. Data Extraction
2.5.2. Selection of the Analysis Model
2.5.3. Effect Size Calculation
2.5.4. Heterogeneity Test
3. Results
3.1. General Characteristics of the Systemically Reviewed Articles
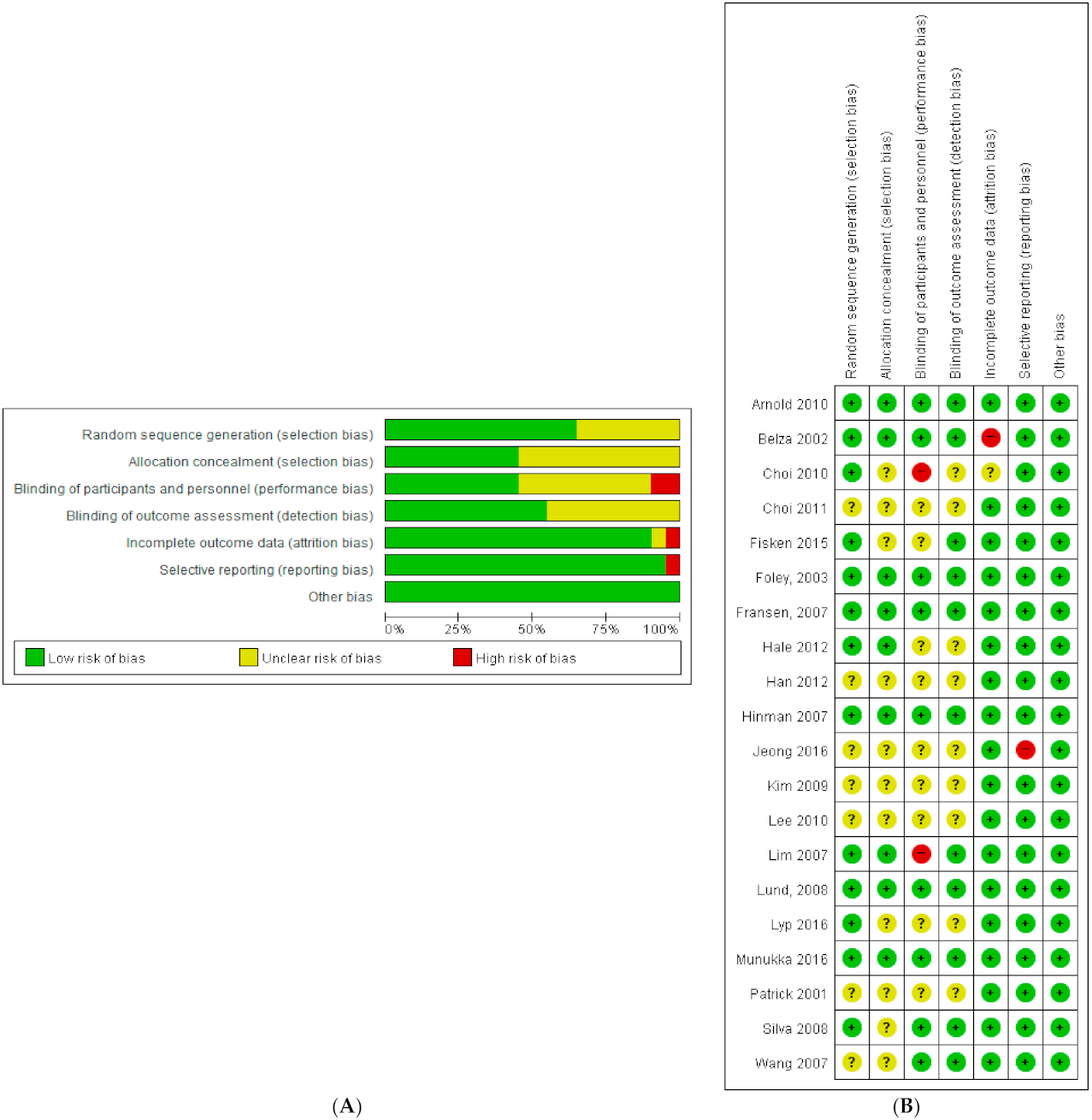
3.2. Quality Assessment of Articles
3.3. Effect Size Estimation
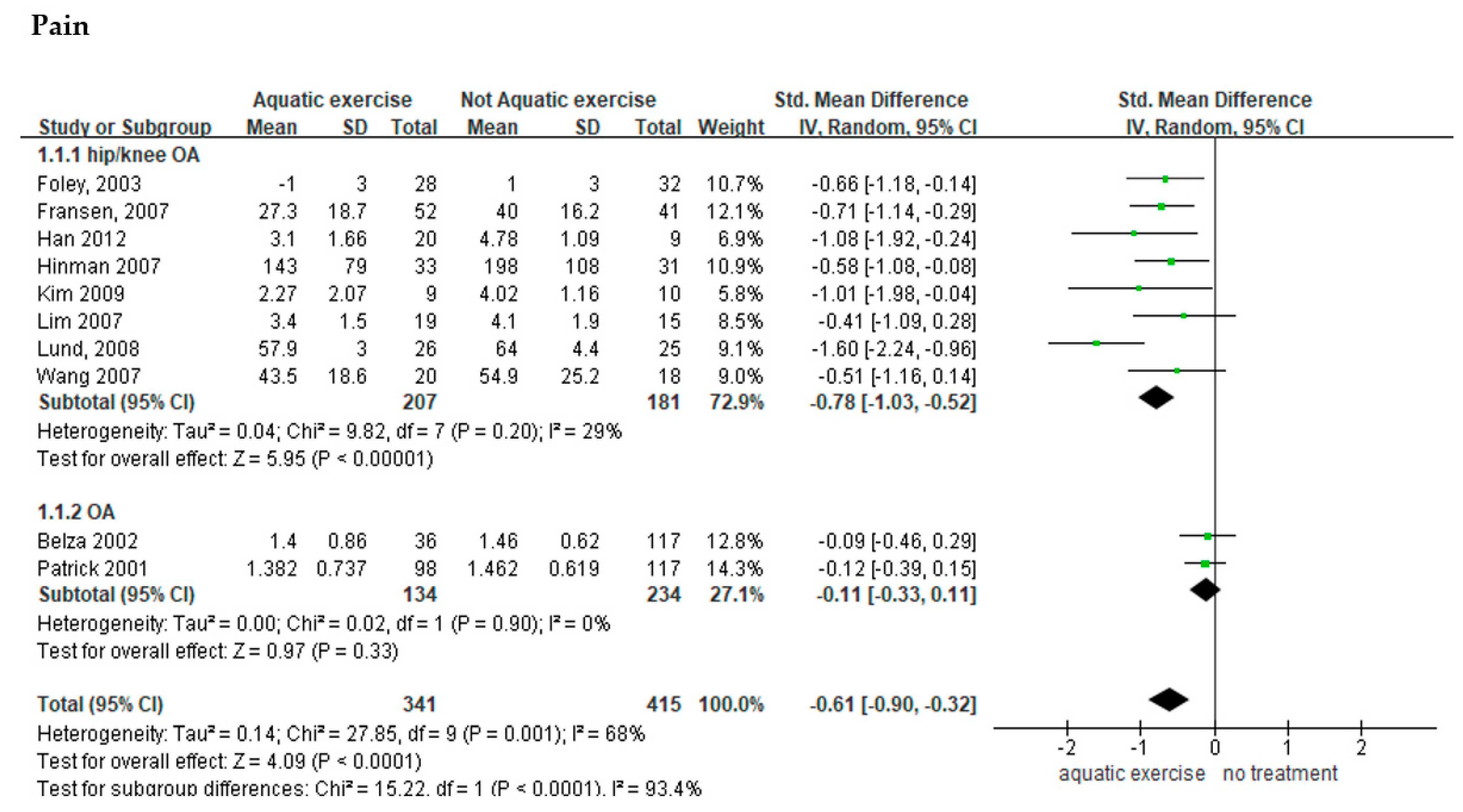
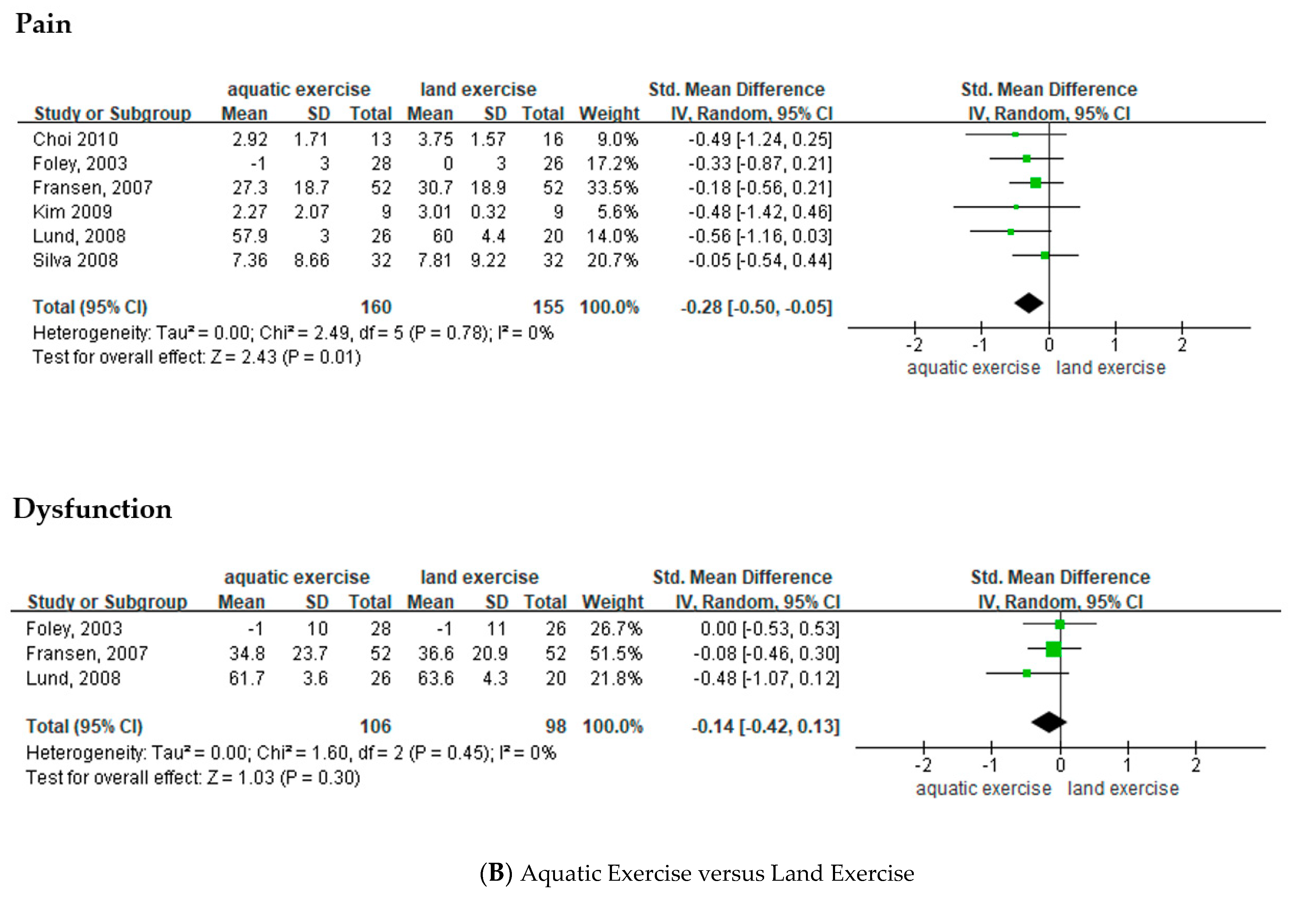
3.3.1. Effects of Aquatic Exercise on Pain among Patients with Osteoarthritis
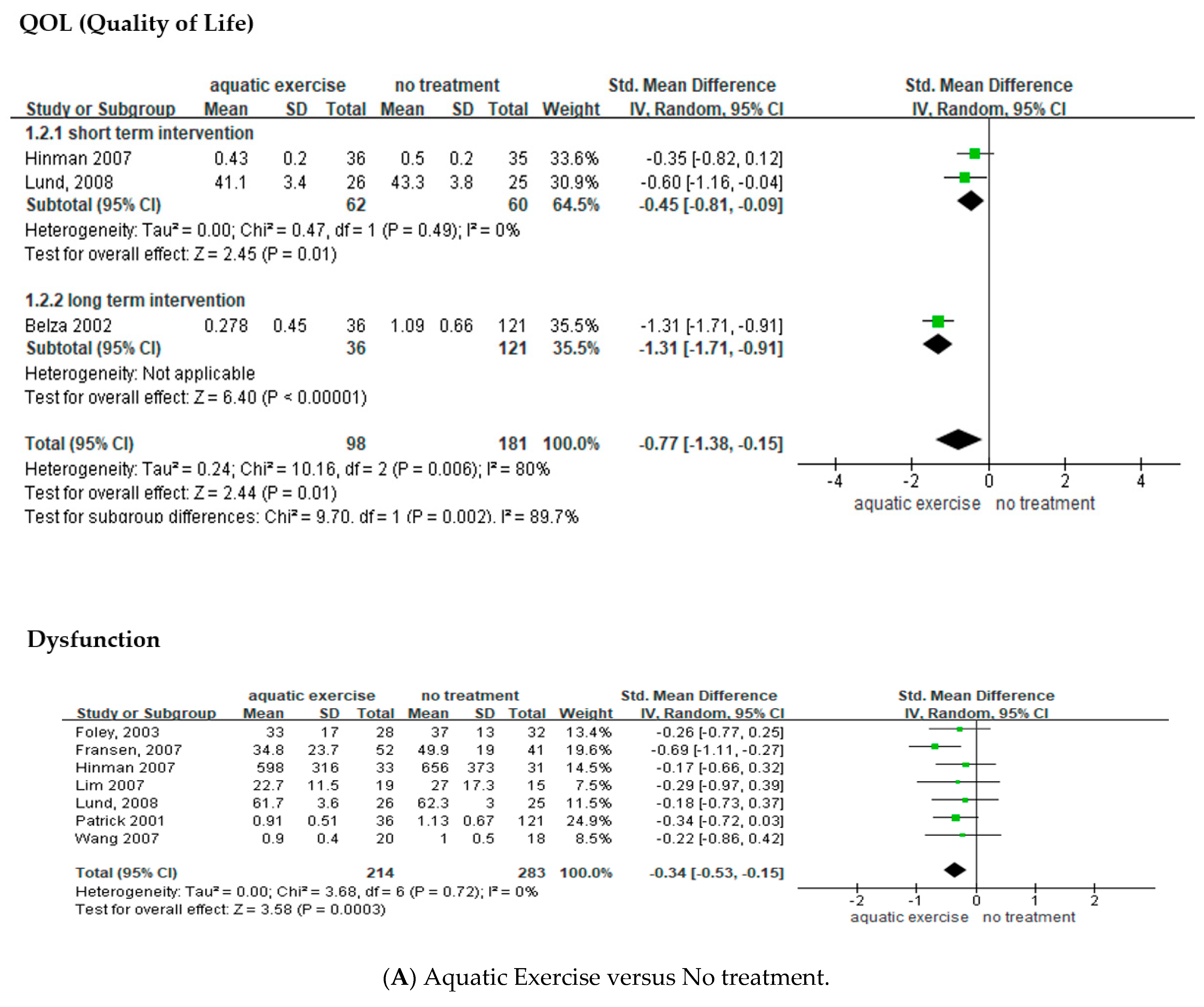
3.3.2. Effects of Aquatic Exercise on the Quality of Life of Patients with Osteoarthritis
3.3.3. Effects of Aquatic Exercise on Joint Dysfunction among Patients with Osteoarthritis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arden, N.; Nevitt, M.C. Osteoarthritis: Epidemiology. Best Pract. Res. Clin. Rheumatol. 2006, 20, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Woo, G.J.; Oh, K.W. Prevalence of osteoarthritis among adults over 50 years old in Korea, 2010–2013. Public Health Weekly Rep. 2015, 8, 82–84. [Google Scholar]
- Bennell, K.L.; Hinman, R.S. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J. Sci. Med. Sport 2011, 14, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Cudejko, T.; van der Esch, M.; van der Leeden, M.; Holla, J.; Roorda, L.D.; Lems, W.; Waddington, G.; Harlaar, J.; Dekker, J. Proprioception mediates the association between systemic inflammation and muscle weakness in patients with knee osteoarthritis: Results from the Amsterdam Osteoarthritis cohort. J. Rehabil. Med. 2018, 50, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F. The C-reactive protein but not erythrocyte sedimentation rate is associated with clinical severity in patients with osteoarthritis of the knee or hip. J. Rheumatol. 1997, 24, 1486–1488. [Google Scholar] [PubMed]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [Green Version]
- Nelson, A.E.; Allen, K.D.; Golightly, Y.M.; Goode, A.P.; Jordan, J.M. A systematic review of recommendations and guidelines for the management of osteoarthritis: The chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin. Arthritis Rheum. 2014, 43, 701–712. [Google Scholar] [CrossRef]
- Beckwée, D.; Vaes, P.; Cnudde, M.; Swinnen, E.; Bautmans, I. Osteoarthritis of the knee: Why does exercise work? A qualitative study of the literature. Ageing Res. Rev. 2013, 12, 226–236. [Google Scholar] [CrossRef]
- Hinman, R.S.; Hunt, M.A.; Creaby, M.W.; Wrigley, T.V.; McManus, F.J.; Bennell, K.L. Hip muscle weakness in individuals with medial knee osteoarthritis. Arthritis Care Res. 2010, 62, 1190–1193. [Google Scholar] [CrossRef]
- Knoop, J.; Dekker, J.; van der Leeden, M.; van der Esch, M.; Thorstensson, C.; Gerritsen, M.; Voorneman, R.E.; Peter, W.F.; de Rooij, M.; Romviel, S.; et al. Knee joint stabilization therapy in patients with osteoarthritis of the knee: A randomized, controlled trial. Osteoarthr. Cartil. 2013, 21, 1025–1034. [Google Scholar] [CrossRef] [Green Version]
- Yázigi, F.; Espanha, M.; Vieira, F.; Messier, S.P.; Monteiro, C.; Veloso, A.P. The PICO project: Aquatic exercise for knee osteoarthritis in overweight and obese individuals. BMC Musculoskelet. Disord. 2013, 14, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosini, A.B.; Brentano, M.A.; Coertjens, M.; Kruel, L.F. The effects of strength training in hydrogymnastics for middle-age women. Int. J. Aquatic. Res. Educ. 2010, 4, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Barker, A.L.; Talevski, J.; Morello, R.T.; Brand, C.A.; Rahmann, A.E.; Urquhart, D.M. Effectiveness of aquatic exercise for musculoskeletal conditions: A meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 1776–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinman, R.S.; Heywood, S.E.; Day, A.R. Aquatic physical therapy for hip and knee osteoarthritis: Results of a single-blind randomized controlled trial. Phys. Ther. 2007, 87, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Bento, P.C.B.; Pereira, G.; Ugrinowitsch, C.; Rodacki, A.L.F. The effects of a water-based exercise program on strength and functionality of older adults. J. Aging Phys. Act. 2012, 20, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Batterham, S.I.; Heywood, S.; Keating, J.L. Systematic review and meta-analysis comparing land and aquatic exercise for people with hip or knee arthritis on function, mobility and other health outcomes. BMC Musculoskelet. Disord. 2011, 12, 123. [Google Scholar] [CrossRef] [Green Version]
- Mattos, F.; Leite, N.; Pitta, A.; Bento, P.C. Effects of aquatic exercise on muscle strength and functional performance of individuals with osteoarthritis: A systematic review. Rev. Bras. Reumatol. Engl. Ed. 2016, 56, 530–542. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2011. [Google Scholar]
- Becker, B.E. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM&R 2009, 1, 859–872. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, J.E.; Seo, H.J.; Lee, Y.J.; Jang, B.H.; Son, H.J.; Suh, H.S.; Shin, C.M. NECA’s Guidance for Undertaking Systematic Reviews and Meta-Analyses for Intervention; National Evidence-Based Healthcare Collaborating Agency: Seoul, Korea, 2011. [Google Scholar]
- Arnold, C.M.; Faulkner, R.A. The effect of aquatic exercise and education on lowering fall risk in older adults with hip osteoarthritis. J. Aging Phys. Act. 2010, 18, 245–260. [Google Scholar] [CrossRef]
- Belza, B.; Topolski, T.; Kinne, S.; Patrick, D.L.; Ramsey, S.D. Does adherence make a difference? Results from a community-based aquatic exercise program. Nurs. Res. 2002, 51, 285–291. [Google Scholar] [CrossRef]
- Choi, H.K.; Cho, K.S.; Kim, J.I. Comparative study of the effects of stretching exercise and aquatic exercise program. J. Muscle Joint Health 2010, 17, 5–13. [Google Scholar] [CrossRef]
- Choi, P.B. Effects of aquatic exercise program on leg muscle functions and T-score as well as depression in elderly women with knee osteoarthritis for 24 weeks. Korean J. Sports Sci. 2011, 20, 1289–1299. [Google Scholar]
- Fisken, A.L.; Waters, D.L.; Hing, W.A.; Steele, M.; Keogh, J.W. Comparative effects of 2 aqua exercise programs on physical function, balance, and perceived quality of life in older adults with osteoarthritis. J. Geriatr. Phys. Ther. 2015, 38, 17–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, A.; Halbert, J.; Hewitt, T.; Crotty, M. Does hydrotherapy improve strength and physical function in patients with osteoarthritis--A randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme. Ann. Rheum. Dis. 2003, 62, 1162–1167. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; Nairn, L.; Winstanley, J.; Lam, P.; Edmonds, J. Physical activity for osteoarthritis management: A randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Rheum. 2007, 57, 407–414. [Google Scholar] [CrossRef]
- Hale, L.A.; Waters, D.; Herbison, P. A randomized controlled trial to investigate the effects of water-based exercise to improve falls risk and physical function in older adults with lower-extremity osteoarthritis. Arch. Phys. Med. Rehabil. 2012, 93, 27–34. [Google Scholar] [CrossRef]
- Han, S.W.; Kim, K.T. The effect of aquarobic and swimming exercise for female elderly suffering from degenerative arthritis on body composition, gait function and pain. Korean J. Sports Sci. 2012, 21, 1077–1089. [Google Scholar] [CrossRef]
- Jeong, T.W.; Choi, Y.C.; Lee, J.W. Effects of land-based and water-based walking exercise on WOMAC and activity fitness in female elderly with knee osteoarthritis. Korean J. Sports Sci. 2016, 25, 1409–1421. [Google Scholar]
- Kim, J.K.; Roh, S.K. Effect of Nordic walking and aquatic exercise on oxidative stress and pain in women with degenerative arthritis. Exerc. Sci. 2009, 18, 549–558. [Google Scholar] [CrossRef]
- Lee, H.D.; Han, S.W. The effects of swimming and aquarobics exercise programs for female elderly suffering from degenerative arthritis on leg muscular function and knee joint ROM. Korean J. Sports Sci. 2010, 19, 1129–1139. [Google Scholar]
- Lim, J.Y.; Kim, B.H.; Chae, E.; Kim, Y.D.; Hong, H.J. The effectiveness of aquatic exercise for obese patients with knee osteoarthritis: Preliminary study. Korean J. Sports Med. 2007, 25, 98–105. [Google Scholar]
- Lund, H.; Weile, U.; Christensen, R.; Rostock, B.; Downey, A.; Bartels, E.M.; Danneskiold-Samsøe, B.; Bliddal, H. A randomized controlled trial of aquatic and land-based exercise in patients with knee osteoarthritis. J. Rehabil. Med. 2008, 40, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyp, M.; Kaczor, R.; Cabak, A.; Tederko, P.; Włostowska, E.; Stanisławska, I.; Szypuła, J.; Tomaszewski, W. A water rehabilitation program in patients with hip osteoarthritis before and after total hip replacement. Med. Sci. Monit. 2016, 22, 2635–2642. [Google Scholar] [CrossRef]
- Munukka, M.; Waller, B.; Rantalainen, T.; Häkkinen, A.; Nieminen, M.T.; Lammentausta, E.; Kujala, U.M.; Paloneva, J.; Sipilä, S.; Peuna, A.; et al. Efficacy of progressive aquatic resistance training for tibiofemoral cartilage in postmenopausal women with mild knee osteoarthritis: A randomised controlled trial. Osteoarthr. Cartil. 2016, 24, 1708–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, D.L.; Ramsey, S.D.; Spencer, A.C.; Kinne, S.; Belza, B.; Topolski, T.D. Economic evaluation of aquatic exercise for persons with osteoarthritis. Med. Care 2001, 39, 413–424. [Google Scholar] [CrossRef]
- Silva, L.E.; Valim, V.; Pessanha, A.P.; Oliveira, L.M.; Myamoto, S.; Jones, A.; Natour, J. Hydrotherapy versus conventional land-based exercise for the management of patients with osteoarthritis of the knee: A randomized clinical trial. Phys. Ther. 2008, 88, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Belza, B.; Elaine Thompson, F.; Whitney, J.D.; Bennett, K. Effects of aquatic exercise on flexibility, strength and aerobic fitness in adults with osteoarthritis of the hip or knee. J. Adv. Nurs. 2007, 57, 141–152. [Google Scholar] [CrossRef]
- Bender, T.; Karagülle, Z.; Bálint, G.P.; Gutenbrunner, C.; Bálint, P.V.; Sukenik, S. Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatol. Int. 2005, 25, 220–224. [Google Scholar] [CrossRef]
- Padilla, G.V.; Ferrell, B.; Grant, M.M.; Rhiner, M. Defining the content domain of quality of life for cancer patients with pain. Cancer Nurs. 1990, 13, 108–115. [Google Scholar] [CrossRef]
- Alkan, B.M.; Fidan, F.; Tosun, A.; Ardıçoğlu, O. Quality of life and self-reported disability in patients with knee osteoarthritis. Mod. Rheumatol. 2014, 24, 166–171. [Google Scholar] [CrossRef]
- Ayis, S.; Dieppe, P. The natural history of disability and its determinants in adults with lower limb musculoskeletal pain. J. Rheumatol. 2009, 36, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Marks, R.; Allegrante, J.P. Chronic osteoarthritis and adherence to exercise: A review of the literature. J. Aging Phys. Act. 2005, 13, 434–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, K.R.; Vincent, H.K. Resistance exercise for knee osteoarthritis. PM&R 2012, 4, S45–S52. [Google Scholar] [CrossRef]
- Pollard, H.; Ward, G.; Hoskins, W.; Hardy, K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: A randomised controlled trial. J. Can. Chiropr Assoc. 2008, 52, 229–242. [Google Scholar]
- Cudejko, T.; van der Esch, M.; van den Noort, J.C.; Rijnhart, J.J.M.; van der Leeden, M.; Roorda, L.D.; Lems, W.; Waddington, G.; Harlaar, J.; Dekker, J. Decreased pain and improved dynamic knee Instability mediate the beneficial effect of wearing a soft knee brace on activity limitations in patients with knee osteoarthritis. Arthritis Care Res. 2019, 71, 1036–1043. [Google Scholar] [CrossRef]
- Cherian, J.J.; Kapadia, B.H.; Bhave, A.; McElroy, M.J.; Cherian, C.; Harwin, S.F.; Mont, M.A. Use of transcutaneous electrical nerve stimulation device in early osteoarthritis of the knee. J. Knee Surg. 2015, 28, 321–327. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Years) | Sample Size Age | Intervention Group (Regime) | Control Group (Regime) | Aquatic Exercise | Main Outcome Measures | Intergroup Difference | Author’s Conclusion |
|---|---|---|---|---|---|---|---|
| Arnold (2010) | 79 adults with hip OA, over 65 years | (1) Aquatic exercise, Chest depth (n = 26) (2) Aquatic exercise and Education, Chest depth (n = 28) * walking, stretching, jump, dumbbell | (3) No treatment (n = 25) | (1) Duration 45 min, 2 days/week, 11-week (2) Duration 30-min education + 45-min aquatic exercise 2 days/week, 11-week | (1) BBSm (2) 6-min Walk test (3) 30-s chair stand (4) ABC-Q (5) TUGcog | (1) NS (2) NS (3) p = 0.022 (4) p = 0.047 (5) NS | “The combination of aquatic exercise and education was effective in improving fall risk factors in older adults with arthritis.” |
| Belza (2002) | 222 adults with OA, 55~75 years | (1) Aquatic exercise, adherence, 85~92 °F (n = 36) * upper- and lower-body activities | (2) Aquatic exercise, non-adherence, 85~92 °F (n = 65) (3) No treatment (n = 121) | (1) Duration 1 h, ≥2 days/week, 20-week (2) Duration 1 h < 2 days/week, 20-week | (1) QWB (2) HAQ (3) Pain-VAS (4) CES-D (5) QOL | (1) p = 0.02 (2) p = 0.02 (3) NS (4) p =0.035 (5) p < 0.01 | “When analyzed for level of participation, exercise benefits adults with osteoarthritis. Improved methods are needed to enhance adherence, with increased attention…” |
| Chi (2010) | 29 women with OA, Avg. age 61 years | (1) Aquatic exercise, Chest depth (n = 13) * walking, stretching, running | (2) Stretching exercise (n = 16) | (1), (2) Duration 50 min, 2 days/week, 8-week | (1) Flexibility (2) Pain-VAS (3) QOL | (1) NS (2) NS (3) NS | “The 8-week stretching exercise program would significantly improve flexibility, pain control and QOL in patients with osteoarthritis.” |
| Choi (2011) | 30 women with knee OA, over 65 years | (1) Aquatic exercise, Chest depth, 28~30 °C (n = 15) * walking, stretching, jump | (2) No treatment (n = 15) | (1) Duration 50 min, 5 days/week, 24-week | (1) Muscle function (2) T-score(pelvic) (3) GDS-K | (1) p < 0.05 (2) p < 0.001 (3) p < 0.001 | “Aquatic exercise very effective on improving leg muscle function and T-score as well as depression.” |
| Fisken (2015) | 25 adults with OA, over 60 years | (1) Aquatic exercise, Chest depth, 87 °F (n = 13) * aerobic, strength | (2) Seated-aquatic DVD exercise, 97.7 °F (n = 12) | (1) Duration 60 min, 2 days/week, 12-week (2) Duration 40 min, once/week, 12-week | (1) TUG (2) Step test (3) Sit-to-stand test (4) Handgrip (5) 400-m walk test (6) AIMS2-SF (7) FES-I | (1) NS (2) NS (3) NS (4) NS (5) NS (6) NS (7) p < 0.05 | “Aqua fitness may offer a number of positive functional and psychosocial benefits for older adults with OA...” |
| Foley (2003) | 35 adults with hip and knee OA, over 50 years | (1) Aquatic exercise, no information (n = 28) (2) Land-based exercise (n = 26) * walking, strength | (3) No treatment (n = 32) | (1), (2) Duration 30 min, 3 days/week, 6-week | (1) Walk speed (2) Muscle strength (3) WOMAC-pain (4) WOMAC-stiff. (5) WOMAC-func. (6) SF-12 PCS (7) SF-12 MCS | (1) B/C p = 0.009 (2) A/B, B/C p < 0.05 (3) NS (4) NS (5) NS (6) A/C p < 0.05 (7) NS | “Functional gains were achieved with both exercise programs compared with the control group.” |
| Fransen (2007) | 145 adults with hip and knee OA, 59~85 years | (1) Aquatic exercise, Waist depth, 34 °C (n = 52) (2) Tai Chi (n = 52) * walking, stretching, strength, raise | (3) No treatment (n = 41) | (1), (2) Duration 60 min, 2 days/week, 12-week | (1) WOMAC-pain (2) WOMAC-func. (3) SF-12 PCS (4) SF-12 MCS (5) Depression (6) Anxiety (7) Stress (8) Up-and-Go (9) 50-foot walk time (10) Stair climb | (1) A/C p < 0.05 (2) A/C, B/C p < 0.05 (3) A/C, B/C p < 0.05 (4) NS (5) NS (6) NS (7) NS (8) A/C, B/C p < 0.05 (9) A/C p < 0.05 (10) A/C, B/C p < 0.05 | “Access to either hydrotherapy or Tai Chi classes can provide large and sustained improvements in physical function for many older, sedentary individuals with chronic hip or knee OA.” |
| Hale (2012) | 35 adults with hip and knee OA, over 65 years | (1) Aquatic exercise, Chest depth, 28 °C (n = 20) * walking, stretching, jump, dumbbell | (2) No treatment, time-matched computer training program (n = 15) | (1), (2) Duration 60 min, 2 days/week, 12-week | (1) PPA (2) Step test (3) TUG (4) WOMAC (5) AIMS2-SF (6) ABC-Q | (1) NS (2) NS (3) NS (4) NS (5) NS (6) NS | “Water-based exercise did not reduce falls risk in our sample compared with attending a computer skills training class.” |
| Han (2012) | 29 women with hip and knee OA, 65~70 years | (1) Aquatic exercise (n = 10) (2) Swimming exercise (n = 10) * walking, stretching, jump | (3) No treatment (n = 9) | (1), (2) Duration 50 min, 3 days/week, 12-week | (1) In body (2) Step length (3) Gait cadence (4) Speed (5) Pain-VAS | (1) NS (2) NS (3) NS (4) p < 0.01 (5) p < 0.05 | “Aquarobic group showed significant increase of lean body mass, and significant decrease body fat, BMI, pain…” |
| Hinman (2007) | 64 adults with hip and knee OA, over 60 years | (1) Aquatic exercise, Chest depth, 34 °C (n = 33) * walking, stretching, hitching, raise | (2) No treatment (n = 31) | (1) Duration 45~60 min, 2 days/week, 6-week | (1) Pain-VAS (2) WOMAC-pain (3) WOMAC-stiff. (4) WOMAC-func. (5) QOL (6) PASE (7) Muscle strength (8) Step test (9) TUG (10) 6-min Walk test | (1) p < 0.05 (2) p < 0.001 (3) p < 0.01 (4) p < 0.001 (5) p < 0.05 (6) NS (7) p < 0.05 (8) NS (9) NS (10) p < 0.01 | “Compared with no intervention, a 6-week program of aquatic physical therapy resulted in significantly less pain and improved physical function, strength, and quality of life.” |
| Jeong (2016) | 30 women with knee OA, over 65 years | (1) Aquatic exercise, Chest depth, 29~30 °C (n = 10) (2) Land-based exercise, Nordic walking (n = 10) * walking, stretching, raise | (3) No treatment (n = 10) | (1), (2) Duration 60 min, 4 days/week, 8-week | (1) WOMAC (2) Arm curl test (3) 30-s chair stand (4) Back scratch (5) Chair sit-reach (6) 2.44-m-TUG (7) 6-min Walk test | (1) p < 0.001 (2) p < 0.001 (3) NS (4) p < 0.001 (5) p < 0.001 (6) p < 0.001 (7) NS | “Walking exercise in the water and walking exercise on the ground are positive exercises that can promote health for the elderly women with degenerative arthritis….” |
| Kim (2009) | 28 women with knee OA, over 65 years | (1) Aquatic exercise, Chest depth, 28 °C (n = 9) (2) Land-based exercise, Nordic walking (n = 9) * walking, stretching, jump, raise | (3) No treatment (n = 10) | (1), (2) Duration 60 min, 4 days/week, 8-week | (1) Pain-VAS (2) Free Oxygen Radical (3) TAC | (1) p < 0.01 (2) p < 0.01 (3) p < 0.01 | “…aquatic exercise in combination including decreases of ROS, are safe and moderately effective…” |
| Lee (2010) | 29 women with knee OA, 60~70 years | (1) Aquatic exercise (n = 10) (2) Swimming exercise (n = 10) * walking, stretching, running, jump, raise | (3) No treatment (n = 9) | (1), (2) Duration 50 min, 3 days/week, 12-week | (1) Power (2) Isometric (3) Leg length (4) Knee joint distance (5) ROM | (1) NS (2) NS (3) NS (4) NS (5) NS | “Aquarobic exercise more effective than swimming on leg muscular strength and ROM for degenerative arthritis.” |
| Lim (2007) | 34 adults with knee OA, Avg. 65.9(A)/62.1(B) years | (1) Aquatic exercise, Chest depth, 32 °C (n = 19) * no information | (2) No treatment (n = 15) | (A) Duration 30 min, 3 days/week, 8-week | (1) Pain-BPI (2) Interference-BPI (3) WOMAC (4) SF-36 PCS (5) SF-36 MCS (6) body mass (7) Body fat mass (8) Waist-hip ratio | (1) p < 0.05 (2) p < 0.05 (3) p = 0.001 (4) NS (5) NS (6) NS (7) NS (8) NS | “Aquatic exercise is an effective tool for obese patients who have a difficulty in active exercise due to combined knee osteoarthritis.” |
| Lund (2008) | 192 adults with knee OA, Avg. 65.0(A)/70.0(B)/ 68.0(C) years | (1) Aquatic exercise, Chest depth, 33.5 °C (n = 26) (2) Land-based exercise (n = 20) * walking, stretching, running | (3) No treatment (n = 25) | (1) Duration 50 min, 2 days/week, 8-week | (1) Pain-VAS (2) KOOS-symp. (3) KOOS-pain (4) KOOS-ADL (5) KOOS-sport (6) KOOS-QOL (7) Muscle strength (8) Balance | (1) NS (2) NS (3) NS (4) NS (5) NS (6) NS (7) NS (8) NS | “Only land-based exercise showed some improvement in pain and muscle strength compared with the control group…” |
| Lyp (2016) | 192 adults with hip OA, 48~82 years | (1) After THR, Aquatic exercise + Kinesitherapy + low-frequency magnetic field, Chest depth, 34 °C (n = 32) (2) Aquatic exercise + Kinesitherapy + low-frequency magnetic field, Chest depth, 34 °C (n = 32) * walking, stretching | (3) After THR, Kinesitherapy + low-frequency magnetic field (n = 32) (D) Kinesitherapy + low-frequency magnetic field (n = 32) (E) After THR, No treatment (n = 32) (F) No treatment (n = 32) | (1), (3) Duration 30 min, 5 days/week, 4-week | (1) Pain-VAS (2) Pain-Laitinen scale (3) HAROM (4) Strength of hip joint | (1) p < 0.001 (2) p < 0.01 (3) −1. A/B/E NS (3) −2. C/D/F NS (4) −1. A/B/E NS (4) −2. C/D/F NS | “Inclusion of water exercises in a rehabilitation program can reduce the use of medicines in patient with OA and after THR.” |
| Munukka (2016) | 84 women with knee OA, 60~68 years | (1) Aquatic exercise, Chest depth, 30~32 °C (n = 42) * resistance ROM | (2) No treatment (n = 42) | (1) Duration 60 min, 3 days/week, 16-week | (1) T2 relaxation time (2) dGEMRIC (3) VO2 peak (4) KOOS | (1) p < 0.05 (2) p < 0.05 (3) p = 0.01 (4) NS | “Additionally, aquatic resistance training of sufficient intensity low risk of harm amongst women with mild knee OA.” |
| Patrick (2001) | 225 adults with OA, 55~75 years | (1) Aquatic exercise: adherence, Chest depth, 85~92 °F (n = 36) (2) Aquatic exercise: non-adherence, Chest depth, 85~92 °F (n = 68) * upper- and lower-body activities | (3) No treatment (n = 121) | (1) Duration 45~60 min, 2 days/week, 20-week (2) Duration 45~60 min, <2 days/week, 20-week | (1) QWB (2) Health desirability (3) HAQ-disability (4) HAQ-pain (5) PQOL-physical (6) CES-D | (1) NS (2) p < 0.05 (3) p < 0.05 (4) NS (5) p < 0.01 (6) NS | “Aquatic exercisers reported equal (QWB) or better (CHDR, HAQ, PQOL) health-related quality of life compared with controls.” |
| Silva (2008) | 64 adults with knee OA, Avg. age 59 years | (1) Aquatic exercise, Chest depth, 32 °C (n = 32) * stretching, strengthening | (2) Land-based exercise (n = 32) | (1), (2) Duration 50 min, 3 days/week, 18-week | (1) Pain-VAS (2) Lequesne index (3) WOMAC (4) After 50FWT Pain-VAS (5) Walking time-fast (6) Walking time | (1) NS (2) NS (3) NS (4) p < 0.01 (5) NS (6) NS | “Water-based exercises are a suitable and effective alternative for the management of OA of the knee.” |
| Wang (2007) | 38 adults with hip and knee OA, Avg. age 69.3(I)/62.7(C) years | (1) Aquatic exercise, Chest depth, 30~32 °C (n = 20) * walking, stretching, lift | (2) No treatment (n = 18) | (1) Duration 50 min, 3 days/week, 12-week | (1) Flexibility (2) Strength-knee (3) Strength-hip (4) Physical function (5) Pain-VAS | (1) p < 0.05 (2) p < 0.05 (3) p < 0.05 (4) NS (5) NS | “Beneficial short-term effects of aquatic exercise were found in adults with osteoarthritis of the hip or knee.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.-A.; Oh, J.W. Effects of Aquatic Exercises for Patients with Osteoarthritis: Systematic Review with Meta-Analysis. Healthcare 2022, 10, 560. https://doi.org/10.3390/healthcare10030560
Song J-A, Oh JW. Effects of Aquatic Exercises for Patients with Osteoarthritis: Systematic Review with Meta-Analysis. Healthcare. 2022; 10(3):560. https://doi.org/10.3390/healthcare10030560
Chicago/Turabian StyleSong, Ji-Ah, and Jae Woo Oh. 2022. "Effects of Aquatic Exercises for Patients with Osteoarthritis: Systematic Review with Meta-Analysis" Healthcare 10, no. 3: 560. https://doi.org/10.3390/healthcare10030560
APA StyleSong, J. -A., & Oh, J. W. (2022). Effects of Aquatic Exercises for Patients with Osteoarthritis: Systematic Review with Meta-Analysis. Healthcare, 10(3), 560. https://doi.org/10.3390/healthcare10030560