The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
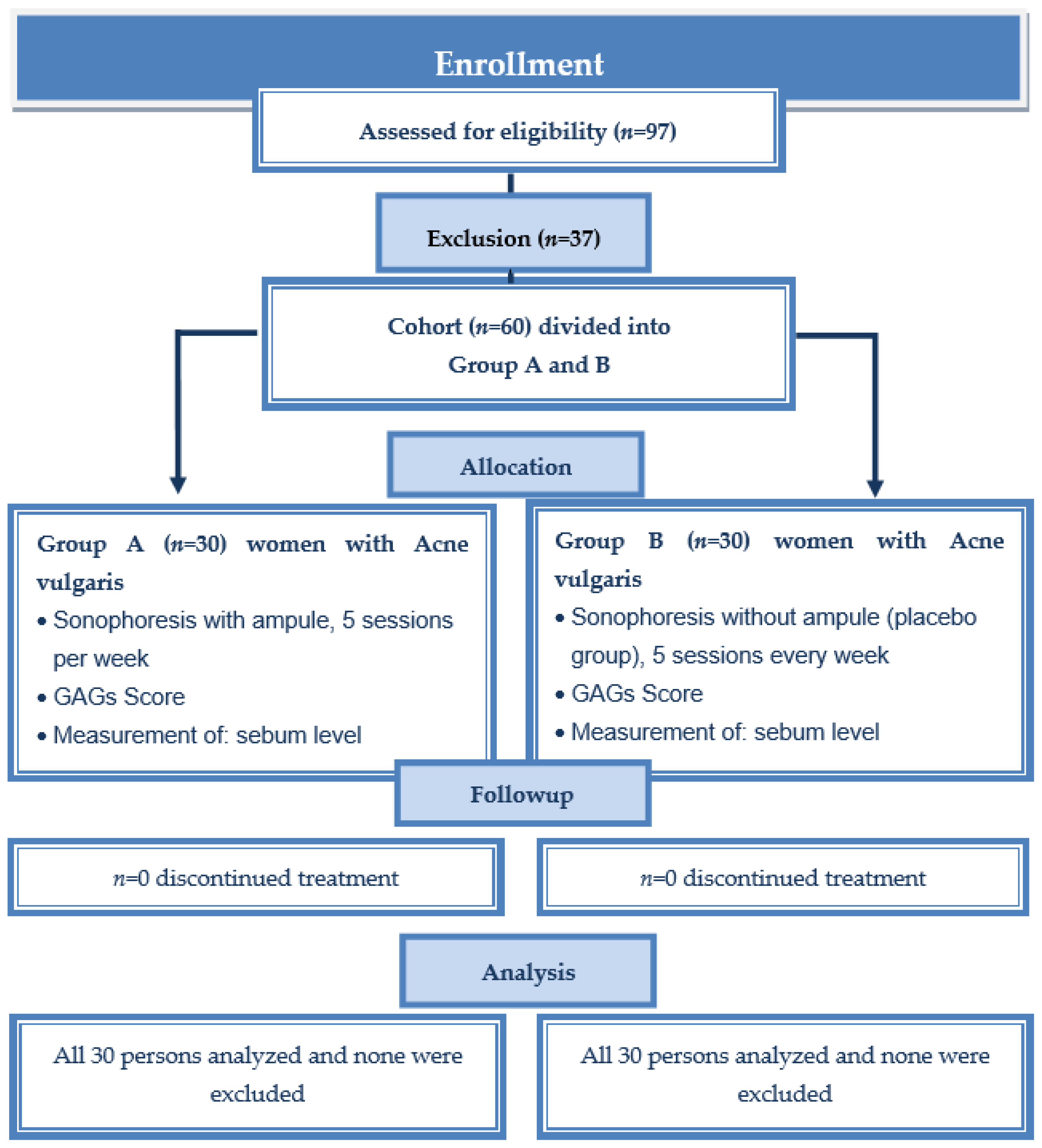
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Acne Vulgaris
2.3.2. Skin Parameters
2.3.3. Demographic Survey
- How old are you?
- What is your height (in cm)?
- How much do you weigh (in kg)?
- How many years have you been suffering from acne?
- Have you ever been treated with antibiotics meant to reduce acne (for example, tetracycline)?
- Have you ever been treated with isotretinoin?
- Have you smoked cigarettes in the last week?
- Have you drinking alcohol in the past week?
- Have you eaten sweets in the last week?
2.4. Treatment Procedure (Intervention)
2.5. Statistical Analysis
3. Results
3.1. Changes in Acne Severity after Sonophoresis Treatment
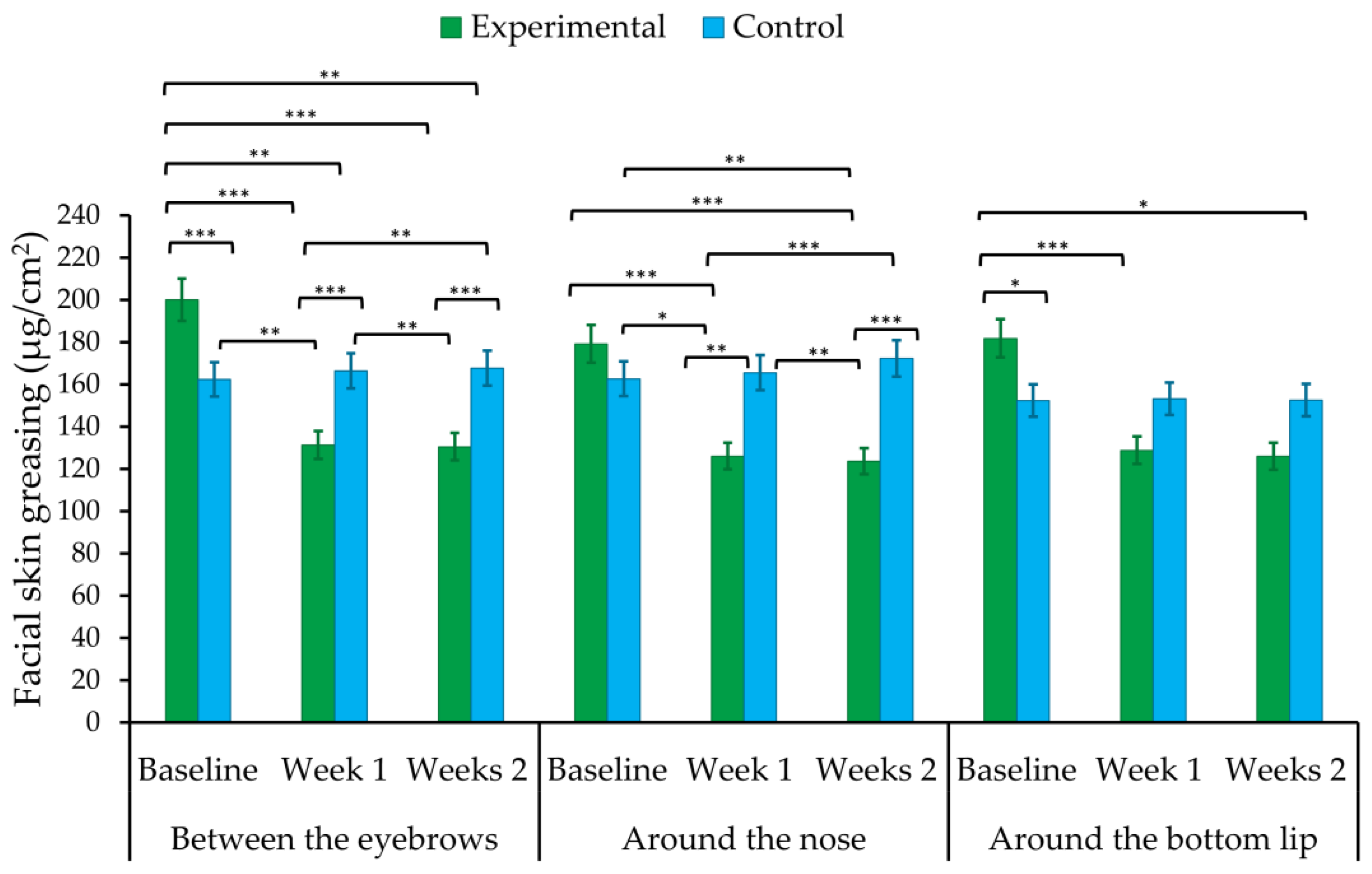
3.2. Changes in Facial Skin Greasing after Sonophoresis
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, S.-Y.; Kim, H.S.; Lee, S.H.; Kim, S. Characterization and Analysis of the Skin Microbiota in Acne: Impact of Systemic Antibiotics. J. Clin. Med. 2020, 9, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.B.; Byun, E.J.; Kim, H.S. Potential Role of the Microbiome in Acne: A Comprehensive Review. J. Clin. Med. 2019, 8, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.-S.; Lu, N.-H.; Shieh, P.-C.; Sun, C.-K. Combination of a Self-Regulation Module and Mobile Application to Enhance Treatment Outcome for Patients with Acne. Medicina 2020, 56, 276. [Google Scholar] [CrossRef] [PubMed]
- Rocha, M.A.; Bagatin, E. Adult-onset acne: Prevalence, impact, and management challenges. Clin. Cosmet. Investig. Dermatol. 2018, 11, 59–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skroza, N.; Tolino, E.; Mambrin, A.; Zuber, S.; Balduzzi, V.; Marchesiello, A.; Bernardini, N.; Proietti, I.; Potenza, C. Adult Acne Versus Adolescent Acne: A Retrospective Study of 1,167 Patients. J. Clin. Aesthetic Dermatol. 2018, 11, 21–25. [Google Scholar]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Taradaj, J. Examining Quality of Life After Treatment with Azelaic and Pyruvic Acid Peels in Women with Acne Vulgaris. Clin. Cosmet. Investig. Dermatol. 2020, 13, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Saric, S.; Notay, M.; Sivamani, R.K. Green Tea and Other Tea Polyphenols: Effects on Sebum Production and Acne Vulgaris. Antioxidants 2017, 6, 2. [Google Scholar] [CrossRef]
- Tsao, R. Chemistry and Biochemistry of Dietary Polyphenols. Nutrients 2010, 2, 1231–1246. [Google Scholar] [CrossRef]
- Melnik, B.C. Western Diet-Mediated mTORC1-Signaling in Acne, Psoriasis, Atopic Dermatitis, and Related Diseases of Civilization: Therapeutic Role of Plant-Derived Natural mTORC1 Inhibitors. In Bioactive Dietary Factors and Plant Extracts in Dermatology; Humana Press: Totowa, NJ, USA, 2013; pp. 397–419. [Google Scholar]
- Melnik, B.C.; Zouboulis, C.C. Potential role of FoxO1 and mTORC1 in the pathogenesis of western diet-induced acne. Exp. Dermatol. 2013, 22, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Monfrecola, G.; Lembo, S.; Caiazzo, G.; De Vita, V.; Di Caprio, R.; Balato, A.; Fabbrocini, G. Mechanistic target of rapamycin (mTOR) expression is increased in acne patients’ skin. Exp. Dermatol. 2016, 25, 153–155. [Google Scholar] [CrossRef] [Green Version]
- Agamia, N.F.; Abdallah, D.M.; Sorour, O.; Mourad, B.; Younan, D.N. Skin expression of mammalian target of rapamycin and forkhead box transcription factor O1, and serum insulin-like growth factor-1 in patients with acne vulgaris and their rela-tionship with diet. Br. J. Dermatol. 2016, 174, 1299–1307. [Google Scholar] [CrossRef]
- Im, M.; Kim, S.Y.; Sohn, K.C.; Choi, D.K.; Lee, Y.; Seo, Y.J.; Kim, C.D.; Hwang, Y.L.; Zouboulis, C.C.; Lee, J.H. Epigallocatechin-3-gallate suppresses IGF-I-induced lipogenesis and cytokine expression in SZ95 sebocytes. J. Investig. Dermatol. 2012, 132, 2700–2708. [Google Scholar] [CrossRef] [Green Version]
- Gong, J.; Huang, J.; Xiao, G.; Chen, F.; Lee, B.; Ge, Q.; You, Y.; Liu, S.; Zhang, Y. Antioxidant Capacities of Fractions of Bamboo Shaving Extract and Their Antioxidant Components. Molecules 2016, 21, 996. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.-C.; Yang, J.-H. Dual Effects of Alpha-Hydroxy Acids on the Skin. Molecules 2018, 23, 863. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Baek, J.H.; Koh, J.S.; Bae, M.I.; Lee, S.J.; Shin, M.K. The effect of physically applied alpha hydroxyl acids on the skin pore and comedone. Int. J. Cosmet. Sci. 2015, 37, 519–525. [Google Scholar] [CrossRef]
- Sharquie, K.E.; Al-Tikreety, M.M.; Al-Mashhadani, S.A. Lactic acid chemical peels as a new therapeutic modality in melasma in comparison to Jessner’s solution chemical peels. Dermatol. Surg. 2006, 32, 1429–1436. [Google Scholar] [CrossRef]
- Polat, B.E.; Blankschtein, D.; Langer, R. Low-frequency sonophoresis: Application to the transdermal delivery of macromolecules and hydrophilic drugs. Expert Opin. Drug Deliv. 2010, 7, 1415–1432. [Google Scholar] [CrossRef] [Green Version]
- Pahade, A.; Jadhav, V.M.; Kadam, V.J. Sonophoresis: An overview. Int. J. Pharm. Sci. Rev. Res. 2010, 3, 24–32. [Google Scholar]
- Wesołowska, J.; Iwan-Ziętek, I.; Mosiejczuk, H.; Kemicer-Chmielewska, E.; Marchlewicz, M. The use of selected physical stimuli during professional cosmetology treatments. Part II. Ultrasonic waves. Pomeranian J. Life Sci. 2017, 63, 44–48. [Google Scholar]
- Vranic, E. Sonophoresis—Mechanizm and application. Bosn. J. Basic Med. Sci. 2004, 4, 25–32. [Google Scholar] [CrossRef]
- Zasada, M.; Drożdż, Z.; Erkiert-Polguj, A.; Budzisz, E. A blinded study assessment of the efficacy of an original formula with retinol in combination with sonophoresis. Dermatol. Ther. 2020, 33, e13163. [Google Scholar] [CrossRef]
- Park, J.; Lee, H.; Lim, G.-S.; Kim, N.; Kim, D.; Kim, Y.-C. Enhanced Transdermal Drug Delivery by Sonophoresis and Simultaneous Application of Sonophoresis and Iontophoresis. AAPS PharmSciTech 2019, 20, 96. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Jeong, K.-H.; Bae, M.I.; Lee, S.-J.; Kim, N.-I.; Shin, M.K. Fractional radiofrequency combined with sonophoresis to facilitate skin penetration of 5-aminolevulinic acid. Lasers Med. Sci. 2016, 31, 113–118. [Google Scholar] [CrossRef]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Dzieńdziora-Urbińska, I.; Taradaj, J. A comparison of the effectiveness of azelaic and pyruvic acid peels in the treatment of female adult acne: A randomized controlled trial. Sci. Rep. 2020, 10, 12612. [Google Scholar] [CrossRef]
- Fąk, M.; Rotsztejn, H.; Erkiert-Polguj, A. The early effect of microdermabrasion on hydration and sebum level. Skin Res. Technol. 2018, 24, 650–655. [Google Scholar] [CrossRef]
- Dastoli, S.; Nisticò, S.P.; Morrone, P.; Patruno, C.; Leo, A.; Citraro, R.; Gallelli, L.; Russo, E.; De Sarro, G.; Bennardo, L. Colchicine in Managing Skin Conditions: A Systematic Review. Pharmaceutics 2022, 14, 294. [Google Scholar] [CrossRef]
- Cannarozzo, G.; Silvestri, M.; Tamburi, F.; Sicilia, C.; Del Duca, E.; Scali, E.; Bennardo, L.; Nisticò, S.P. A new 675-nm laser device in the treatment of acne scars: An observational study. Lasers Med. Sci. 2021, 36, 227–231. [Google Scholar] [CrossRef]
- Monib, K.M.E.-D.; Hussein, M.S. Nd:YAG laser vs IPL in inflammatory and noninflammatory acne lesion treatment. J. Cosmet. Dermatol. 2019, 19, 2325–2332. [Google Scholar] [CrossRef]
- Doshi, A.; Zaheer, A.; Stiller, M.J. A comparison of current acne trading systems and proposal of a novel system. Int. J. Dermatol. 1997, 36, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Thappa, D.; Adityan, B.; Kumari, R. Scoring systems in acne vulgaris. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 323–326. [Google Scholar] [CrossRef]
- Kołodziejczak, A.; Wieczorek, A.; Rotsztejn, H. The assessment of the effects of the combination of microdermabrasion and cavitation peeling in the therapy of seborrhoeic skin with visible symptoms of acne punctata. J. Cosmet. Laser Ther. 2019, 21, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, T.; Akhtar, N.; Moldovan, C. A comparison of the effects of topical green tea and lotus on facial sebum control in healthy humans. Hippokratia 2013, 17, 64–67. [Google Scholar] [PubMed]
- Lu, P.H.; Hsu, C.H. Does supplementation with green tea extract improve acne in post-adolescent women? A randomized, double-blind, and placebo-controlled clinical trial. Complement. Ther. Med. 2016, 25, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.K.; Ha, S.; Son, J.-A.; Song, J.H.; Houh, Y.; Cho, E.; Chun, J.H.; Yoon, S.R.; Yang, Y.; Bang, S.I.; et al. Polyphenon-60 displays a therapeutic effect on acne by suppression of TLR2 and IL-8 expression via down-regulating the ERK1/2 pathway. Arch. Dermatol. Res. 2012, 304, 655–663. [Google Scholar] [CrossRef]
- Sharquie, K.E.; Al-Turfi, I.A.; Al-Shimary, W.M. Treatment of acne vulgaris with 2% topical tea lotion. Saudi Med. J. 2006, 27, 83–85. [Google Scholar]
- Elsaie, M.L.; Abdelhamid, M.F.; Elsaaiee, L.T.; Emam, H.M. The efficacy of topical 2% green tea lotion in mild-to-moderate acne vulgaris. J. Drugs Dermatol. 2009, 8, 358–364. [Google Scholar]
- Mahmood, T.; Akhtar, N.; Khan, B.A.; Khan, H.M.S.; Saeed, T. Outcomes of 3% Green Tea Emulsion on Skin Sebum Production in Male Volunteers. Bosn. J. Basic Med. Sci. 2010, 10, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.-T.; Liu, W.-S.; Wu, Y.-C.; Lai, Y.-W.; Wen, Z.-H.; Wang, H.-M.; Lee, S.-S. The Effect in Topical Use of Lycogen(TM) via Sonophoresis for Anti-aging on Facial Skin. Curr. Pharm. Biotechnol. 2015, 16, 1063–1069. [Google Scholar] [CrossRef]
- Choi, J.H.; Shin, E.J.; Jeong, K.-H.; Shin, M.K. Comparative analysis of the effects of CO2 fractional laser and sonophoresis on human skin penetration with 5-aminolevulinic acid. Lasers Med. Sci. 2017, 32, 1895–1900. [Google Scholar] [CrossRef]
- Jung, E.C.; Zhu, H.; Zou, Y.; Elmahdy, A.; Cao, Y.; Hui, X.; Maibach, H.I. Effect of ultrasound and heat on percutaneous absorption of l-ascorbic acid: Human in vitro studies on Franz cell and Petri dish systems. Int. J. Cosmet. Sci. 2016, 38, 646–650. [Google Scholar] [CrossRef]
- Lodhi, S.; Jain, A.P.; Rai, G.; Yadav, A.K. Preliminary investigation for wound healing and anti-inflammatory effects of Bambusa vulgaris leaves in rats. J. Ayurveda Integr. Med. 2016, 7, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Davane, M.; Nagoba, B. Wound healing effects of Bambusa vulgaris leaves. J. Ayurveda Integr. Med. 2016, 7, 185. [Google Scholar] [CrossRef] [Green Version]
- Greydanus, D.E.; Azmeh, R.; Cabral, M.D.; Dickson, C.A.; Patel, D.R. Acne in the first three decades of life: An update of a disorder with profound implications for all decades of life. Dis. Mon. 2021, 67, 101103. [Google Scholar] [CrossRef]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R. Effects of Topical Hydrogen Purification on Skin Parameters and Acne Vulgaris in Adult Women. Healthcare 2021, 9, 144. [Google Scholar] [CrossRef]
- Tallei, T.E.; Fatimawali; Niode, N.J.; Idroes, R.; Zidan, B.M.R.M.; Mitra, S.; Celik, I.; Nainu, F.; Ağagündüz, D.; Emran, T.B.; et al. A Comprehensive Review of the Potential Use of Green Tea Polyphenols in the Management of COVID-19. Evid.-Based Complement. Altern. Med. 2021, 2021, 7170736. [Google Scholar] [CrossRef]
- Mathew, T.C.; Abdeen, S.M.; Dashti, H.; Asfar, S. Green Tea Induced Cellular Proliferation and the Expression of Transforming Growth Factor-β1 in the Jejunal Mucosa of Fasting Rats. Med. Princ. Pract. 2017, 26, 343–350. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Sample | Experimental Group | Control Group | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Range | n | % | n | % | n | % | χ2 | p | φ | |
| Age (years) (M, SD) | 19–23 | 21.45 | 0.91 | 21.17 | 0.99 | 21.73 | 0.74 | 330.50 U | 0.059 | −0.27 d |
| Height (cm) (M, SD) | 153–187 | 164.77 | 5.44 | 163.83 | 5.51 | 165.70 | 5.29 | 373.00 U | 0.257 | −0.1 d |
| Weight (kg) (M, SD) | 44–87 | 61.22 | 8.40 | 61.83 | 7.61 | 60.60 | 9.21 | 520.50 U | 0.300 | 0.16 d |
| Body mass index (BMI) (M, SD) | 17.40–31.96 | 22.54 | 2.81 | 23.01 | 2.38 | 22.06 | 3.15 | 584.50 U | 0.048 | 0.30 d |
| Normal | 18.51–24.99 | 51 | 85.00 | 26 | 86.67 | 25 | 83.33 | 1.52 | 0.468 | 0.16 V |
| Overweight | 25.00–29.99 | 8 | 13.33 | 3 | 10.00 | 5 | 16.67 | |||
| Obese | 30.00< | 1 | 1.67 | 1 | 3.33 | 0 | 0.00 | |||
| Acne duration (years) (M, SD) | 2–12 | 6.20 | 2.15 | 6.57 | 1.14 | 5.83 | 2.81 | 558.00 U | 0.106 | 0.24 d |
| Acne severity (GAG) (M, SD) | 17–25 | 21.10 | 1.68 | 21.50 | 1.64 | 20.70 | 1.66 | 562.50 U | 0.092 | 0.25 d |
| Mild | 1–18 | 2 | 3.33 | 0 | 0.00 | 2 | 6.67 | 2.07 | 0.150 | −0.19 |
| Moderate | 19–30 | 58 | 96.67 | 30 | 100.00 | 28 | 93.33 | |||
| Antibiotics use (ever) | ||||||||||
| Yes | 43 | 71.67 | 26 | 86.67 | 17 | 56.67 | 6.65 | 0.010 | −0.33 | |
| No | 17 | 28.33 | 4 | 13.33 | 13 | 43.33 | ||||
| Isotretinoin use (ever) | ||||||||||
| Yes | 16 | 26.67 | 11 | 36.67 | 5 | 16.67 | 3.07 | 0.080 | −0.23 | |
| No | 44 | 73.33 | 19 | 63.33 | 25 | 83.33 | ||||
| Smoking cigarettes last week | ||||||||||
| Yes | 21 | 35.00 | 10 | 33.33 | 11 | 36.67 | 0.07 | 0.787 | 0.04 | |
| No | 39 | 65.00 | 20 | 66.67 | 19 | 63.33 | ||||
| Drinking alcohol last week | ||||||||||
| Yes | 35 | 58.33 | 18 | 60.00 | 7 | 23.33 | 8.297 | 0.004 | 0.37 | |
| No | 25 | 41.67 | 12 | 40.00 | 23 | 76.67 | ||||
| Eating sweets last week | ||||||||||
| Yes | 57 | 95.00 | 30 | 100.00 | 27 | 90.00 | 3.16 | 0.076 | −0.23 | |
| No | 3 | 5.00 | 0 | 0.00 | 3 | 10.00 | ||||
| Experimental Group | Control Group | |||||
|---|---|---|---|---|---|---|
| Condition | Range | M | SD | Range | M | SD |
| Before treatment | 19–25 | 21.50 | 1.63 | 17–24 | 20.70 | 1.66 |
| After treatment | 9–19 | 14.73 | 3.04 | 17–24 | 20.70 | 1.62 |
| Experimental | Control | |||||||
|---|---|---|---|---|---|---|---|---|
| Facial Skin Greasing | M | SD | M | SD | Effect | F ratio | df | ηp2 |
| Between the eyebrows | ||||||||
| Baseline | 199.98 | 30.82 | 162.43 | 53.79 | G | 2.20 | 1.58 | 0.04 |
| Week 1 after treatment | 131.35 | 25.22 | 166.40 | 34.01 | T | 49.08 *** | 2.116 | 0.46 |
| Weeks 2 after treatment | 130.52 | 23.31 | 167.70 | 31.35 | G × T | 64.20 *** | 2.116 | 0.53 |
| Around the nose | ||||||||
| Baseline | 179.23 | 44.53 | 162.67 | 51.98 | G | 6.15 * | 1.58 | 0.10 |
| Week 1 after treatment | 126.03 | 27.01 | 165.67 | 45.57 | T | 24.92 *** | 2.116 | 0.30 |
| Weeks 2 after treatment | 123.69 | 25.37 | 172.30 | 45.65 | G × T | 40.15 *** | 2.116 | 0.41 |
| Around the bottom lip | ||||||||
| Baseline | 181.83 | 40.33 | 152.33 | 50.76 | G | 0.65 | 1.58 | 0.01 |
| Week 1 after treatment | 128.83 | 27.33 | 153.30 | 48.64 | T | 29.64 *** | 2.116 | 0.34 |
| Weeks 2 after treatment | 126.00 | 23.26 | 152.53 | 34.48 | G × T | 30.87 *** | 2.116 | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chilicka, K.; Rogowska, A.M.; Rusztowicz, M.; Szyguła, R.; Yanakieva, A.; Asanova, B.; Wilczyński, S. The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment. Healthcare 2022, 10, 684. https://doi.org/10.3390/healthcare10040684
Chilicka K, Rogowska AM, Rusztowicz M, Szyguła R, Yanakieva A, Asanova B, Wilczyński S. The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment. Healthcare. 2022; 10(4):684. https://doi.org/10.3390/healthcare10040684
Chicago/Turabian StyleChilicka, Karolina, Aleksandra M. Rogowska, Monika Rusztowicz, Renata Szyguła, Antoniya Yanakieva, Binnaz Asanova, and Sławomir Wilczyński. 2022. "The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment" Healthcare 10, no. 4: 684. https://doi.org/10.3390/healthcare10040684
APA StyleChilicka, K., Rogowska, A. M., Rusztowicz, M., Szyguła, R., Yanakieva, A., Asanova, B., & Wilczyński, S. (2022). The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment. Healthcare, 10(4), 684. https://doi.org/10.3390/healthcare10040684