Patient Profile and Management of Delirium in Older Adults Hospitalized Due to COVID-19

 ,
,  ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ticinesi, A.; Cerundolo, N.; Parise, A.; Nouvenne, A.; Prati, B.; Guerra, A.; Lauretani, F.; Maggio, M.; Meschi, T. Delirium in COVID-19: Epidemiology and clinical correlations in a large group of patients admitted to an academic hospital. Aging Clin. Exp. Res. 2020, 32, 2159–2166. [Google Scholar] [CrossRef] [PubMed]
- Poloni, T.E.; Carlos, A.F.; Cairati, M.; Cutaia, C.; Medici, V.; Marelli, E.; Ferrari, D.; Galli, A.; Bognetti, P.; Davin, A.; et al. Prevalence and prognostic value of Delirium as the initial presentation of COVID-19 in the elderly with dementia: An Italian retrospective study. EClinicalMedicine 2020, 26, 100490. [Google Scholar] [CrossRef] [PubMed]
- Carlos III Health Institute, Epidemiological Surveillance Network. [Covid- I. Informe no 81. Situación de COVID-19 en España]. ISCIII-CNE 2021. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/INFORMES/Informes%20COVID-19/INFORMES%20COVID-19%202021/Informe%20n%C2%BA%2081.%20Situaci%C3%B3n%20de%20COVID-19%20en%20Espa%C3%B1a%20a%202%20de%20junio%20de%202021.pdf (accessed on 3 January 2022).
- Epidemiological Surveillance Network. Carlos III Health Institute [Covid- I. Informe sobre la situación de COVID-19 en España]. Guía COVID-19. Información para profesionales sanitarios. ISCIII -CNE. 2020. Available online: https://repisalud.isciii.es/bitstream/handle/20.500.12105/11012/14%20-%20Profesionales%2028%20Septiembre.pdf?sequence=65&isAllowed=y (accessed on 3 January 2022).
- Fisicaro, F.; Di Napoli, M.; Liberto, A.; Fanella, M.; Di Stasio, F.; Pennisi, M.; Bella, R.; Lanza, G.; Mansueto, G. Neurological Sequelae in Patients with COVID-19: A Histopathological Perspective. Int. J. Environ. Res. Public Health 2021, 18, 1415. [Google Scholar] [CrossRef] [PubMed]
- Antón Jimenez, M.; Giner Santeodoro, A.; Villalba Lancho, E. Tratado de Geriatría Para Residentes; Sociedad Española de Enfermería Geriátrica: Madrid, Spain, 2006; pp. 189–198. [Google Scholar]
- Merino Vaca, C. Prevalencia del delirium en el paciente anciano ingresado en una unidad de convalescencia: Plan de cuidados y protocolo de prevención. Inf. Psiquiátricas 2018, 232, 131–138. [Google Scholar]
- Vazquez, F.; Flaherty, M.; Michelangelo, H.; Quiros, R.; Garfi, L.; Janson, J.; Camera, L. Epidemiología del delirio en ancianos hospitalizados. Medicina 2000, 60, 555–560. [Google Scholar]
- Vreeswijk, R.; Kalisvaart, I.; Maier, A.B.; Kalisvaart, K.J. Development and validation of the delirium risk assessment score (DRAS). Eur. Geriatr. Med. 2020, 11, 307–314. [Google Scholar] [CrossRef]
- Young, J.; Cheater, F.; Collinson, M.; Fletcher, M.; Forster, A.; Godfrey, M.; Green, J.; Anwar, S.; Hartley, S.; Hulme, C.; et al. Prevention of delirium (POD) for older people in hospital: Study protocol for a randomised controlled feasibility trial. Trials 2015, 16, 340. [Google Scholar] [CrossRef] [Green Version]
- Sánchez García, E. Prevención del Delirium en el Paciente Anciano: Diseño y Evaluación de Una Intervención no Farmacológica en el Ámbito Hospitalario; Universidad Complutense de Madrid: Madrid, Spain, 2015. [Google Scholar]
- Mcloughlin, B.C.; Miles, A.; Webb, T.E.; Knopp, P.; Eyres, C.; Fabbri, A.; Humphries, F.; Davis, D. Functional and cognitive outcomes after COVID-19 delirium. Eur. Geriatr. Med. 2020, 11, 857–862. [Google Scholar] [CrossRef]
- Perelló Campaner, C. Valoración del riesgo de delirium en pacientes mayores hospitalizados. Rev. Esp. Geriatr. Gerontol. 2010, 45, 285–290. [Google Scholar] [CrossRef]
- Schmitt, E.M.; Gallagher, J.; Albuquerque, A.; Tabloski, P.; Lee, H.J.; Gleason, L.; Schulman-Green, D. Perspectives on the Delirium Experience and Its Burden: Common Themes among Older Patients, Their Family Caregivers, and Nurses. Gerontologist 2019, 59, 327–337. [Google Scholar] [CrossRef]
- González Tugas, M.; Uslar Nawrath, W.; Villarroel del Pino, L.; Calderón Pinto, J.; Palma Onetto, C.; Carrasco Gorman, M. Coste hospitalario asociado al delirium en pacientes mayores. Rev. Esp. Geriatr. Gerontol. 2012, 47, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Bogardus, S.T.; Charpentier, P.A.; Leo-Summers, L.; Acampora, D.; Holford, T.R.; Cooney, L.M. A Multicomponent Intervention to Prevent Delirium in Hospitalized Older Patients. N. Engl. J. Med. 1999, 340, 669–676. [Google Scholar] [CrossRef] [PubMed]
- O’Hanlon, S.; Inouye, S.K. Delirium: A missing piece in the COVID-19 pandemic puzzle. Age Ageing 2020, 49, 497–498. [Google Scholar] [CrossRef] [PubMed]
- Rubin, F.H.; Bellon, J.; Bilderback, A.; Urda, K.; Inouye, S.K. Effect of the Hospital Elder Life Program on Risk of 30-Day Readmission. J. Am. Geriatr. Soc. 2018, 66, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radhakrishnan, N.S.; Mufti, M.; Ortiz, D.; Maye, S.; Melara, J.; Lim, D.; Price, C.C. Implementing Delirium Prevention in the Era of COVID-19. J. Alzheimer’s Dis. 2021, 79, 31–36. [Google Scholar] [CrossRef] [PubMed]
- De Castro, R.E.V.; Garcez, F.B.; Avelino-Silva, T.J. Patient care during the covid-19 pandemic: Do not leave delirium behind. Braz. J. Psychiatry 2021, 43, 127–128. [Google Scholar] [CrossRef]
- Garcez, F.B.; Aliberti, M.J.R.; Poco, P.C.E.; Hiratsuka, M.; de Takahashi, S.F.; Coelho, V.A.; Salotto, D.B.; Moreira, M.L.V.; Jacob-Filho, W.; Avelino-Silva, T.J. Delirium and Adverse Outcomes in Hospitalized Patients with COVID-19. J. Am. Geriatr. Soc. 2020, 68, 2440–2446. [Google Scholar] [CrossRef]
- Mendes, A.; Herrmann, F.R.; Périvier, S.; Gold, G.; Graf, C.E.; Zekry, D. Delirium in Older Patients With COVID-19: Prevalence, Risk Factors, and Clinical Relevance. J. Gerontol. Ser. A 2021, 76, e142–e146. [Google Scholar] [CrossRef]
- Zazzara, M.B.; Penfold, R.S.; Roberts, A.L.; Lee, K.A.; Dooley, H.; Sudre, C.H.; Lochlainn, M.N. Probable delirium is a presenting sympton of COVID-19 in frail, older adults: A cohort study of 322 hospitalized and 535 comunity-based older adults. Age Ageing 2021, 50, 40–48. [Google Scholar] [CrossRef]
- [Desarrollo De Guías De Práctica Clínica En Pacientes Con Comorbilidad Y Pluripatología]. SEMI-semFYC-FAECAP. Madrid. 2013. Available online: https://www.faecap.com/publicaciones/show/desarrollo-de-guias-de-practica-clinica-en-pacientes-con-comorbilidad-y-pluripatologia (accessed on 3 January 2022).
- Buzzini, D.M.; Secundini, R.; Gazzotti, A.; Giraldes, R.L.; Alejandro, R.; Castro, A.; Druetta, S.; Se-, S.; Rodríguez, A.; Li, L. Validación del Índice de Barthel. Boletín Del Dep. De Docencia E Investig. IREP 2002, 6, 9–12. [Google Scholar]
- Martínez de la Iglesiaa, J.; DueñasHerrero, R.; Carmen Onís Vilchesa, M.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Adaptación y validación al castellano del cuestionario de Pfeiffer (SPMSQ) para detectar la existencia de deterioro cognitivo en personas mayores e 65 años. Med. Clin. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Pancorbo, P.; García, F.; Soldevilla, J.; Blasco, C. Documento Técnico Gneaupp no xi “Escalas e instrumentos de valoración del riesgo de desarrollar úlceras por presión”. Gerocomos 2009, 19, 136–144. Available online: http://gneaupp.es/app/adm/documentos-guias/archivos/81_pdf.pdf (accessed on 3 January 2022).
- Alonso Ganuza, Z.; González-Torres, M.Á.; Gaviria, M. El Delirium: Una revisión orientada a la práctica clínica. Rev. La Asoc. Esp. Neuropsiquiatr. 2012, 32, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Navarro, S.G.; Duarte-Flores, J.O.; Granados-Valdéz, M.C.; Suing-Ortega, M.J.; Mimenza-Alvarado, A.J. Prevention, diagnosis, and treatment of delirium in older adults with COVID-19. Literature review. Salud Ment. 2020, 43, 319–327. [Google Scholar] [CrossRef]
- Inouye, S.K. The Short Confusion Assessment Method (Short CAM): Training Manual and Coding Guide. In Hosp Elder Life Program; Harvard Medical School: Boston, MA, USA, 2014; pp. 526–533. [Google Scholar]
- Carrera Castro, C. Un análisis cualitativo del rendimiento del Método de Evaluación de la Confusión. Investig en Enfermería Imagen y Desarro. Investig. En Enferm. Imagen Desarro. 2015, 17, 95–110. [Google Scholar] [CrossRef]
- Duaso, E.; Formiga, F.; Rodríguez, D. Tratamiento farmacológico del delirium. Rev. Esp. De Geriatría Gerontol. 2008, 43, 33–38. [Google Scholar]
- Nogal, M.L. Síndrome confusional. Psicogeriatría 2009, 1, 209–221. [Google Scholar]
- Woodhouse, R.; Burton, J.K.; Rana, N.; Pang, Y.L.; Lister, J.E.; Siddiqi, N. Interventions for preventing delirium in older people in institutional long-term care. Cochrane Database Syst. Rev. 2019, 4, CD009537 . [Google Scholar] [CrossRef]
- Britton, A.M.; Russell, R. Multidisciplinary team interventions for delirium in patients with chronic cognitive impairment. Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef]
- Inouye, S.K.; Zhang, Y.; Jones, R.N.; Kiely, D.K.; Yang, F.; Marcantonio, E.R. Risk Factors for Delirium at Discharge. Arch. Int. Med. 2007, 167, 1406. [Google Scholar] [CrossRef] [Green Version]
- Carignan, C.C.; Punshon, T.; Karagas, M.R.; Cottingham, K.L.; Hanover, N. HHS Public Access. Ann. Glob. Health Author Manuscr. 2018, 318, 1161–1174. [Google Scholar]
- Claver Martín, M.D. Actualización en la evaluación y tratamiento del delirium. Rev. Esp. Geriatr. Gerontol. 2008, 34. Available online: http://www.elsevier.es/es-revista-revista-espanola-geriatria-gerontologia-124-articulo-actualizacion-evaluacion-tratamiento-del-delirium-13011650 (accessed on 3 January 2022).
- Heaven, A.; Cheater, F.; Clegg, A.; Collinson, M.; Farrin, A.; Forster, A.; Siddiqi, N. Pilot trial of Stop Delirium! (PiTStop)-a complex intervention to prevent delirium in care homes for older people: Study protocol for a cluster randomised controlled trial. Trials 2014, 15, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | Items | N (%) or Mean ± SD 1 |
|---|---|---|
| Age range (65–95) | 77.29 ± 7.7 | |
| 65–74 | 42 (38.9) | |
| 75–85 | 44 (40.7) | |
| >85 | 22 (20.4) | |
| Sex | Male | 63 (58.3) |
| Female | 45 (41.7) | |
| Place of residence | Urban | 62 (57.4) |
| Rural | 46 (42.6) | |
| Cohabitants | Partner or spouse | 60 (55.6) |
| Other relative | 10 (9.3) | |
| Living alone | 18 (16.7) | |
| Paid carer | 5 (4.6) | |
| Nursing home | 15 (13.9) | |
| Clinical history Comorbidities 2 | <2 | 36 (32.4) |
| x > 2 | 56 (52.8) | |
| No comorbidities | 16 (14.8) |
| Variable | N (%) | No ADOP n (%) | ADOP n (%) | Chi2/Fisher (p) |
|---|---|---|---|---|
| Age | ||||
| 65–75 | 50 (46.3) | 42 (55.3) | 8 (25) | 0.001 |
| 76–85 | 38 (35.2) | 26 (34.2) | 12 (37.5) | |
| >86 | 22 (18.5) | 8 (10.5) | 12 (37.5) | |
| Male sex | 45 (41.7) | 33 (43.5) | 12 (37.5) | 0.569 |
| Comorbidity | 57 (52.8) | 38 (50) | 19 (59.4) | 0.021 |
| Medical diagnosis of dementia | 15 (13.8) | 6 (7.9) | 9 (28.2) | 0.021 |
| Severe dependent (Barthel < 35) | 3 (2.8) | 0 | 3 (9.4) | 0.000 |
| Moderate dependent (Barthel 35–65) | 27 (25) | 13 (17.1) | 14 (43.8) | |
| Slight dependent or independent | 78 (72.2) | 63 (82.9) | 15 (46.9) | |
| Severe cognitive impairment (Pfeiffer 7–10) | 6 (5.6) | 2 (2.6) | 4 (12.5) | 0.000 |
| Moderate cognitive impartment (Pfeiffer 3–7) | 16 (14.8) | 2 (2.6) | 14 (43.8) | |
| No cognitive impairment | 86 (79.6) | 72 (94.7) | 14 (43.8) | |
| Auditive sensorial deterioration | 19 (17.6) | 10 (13.2) | 9 (28.1) | 0.021 |
| Visual sensorial deterioration | 8 (7.4) | 4 (5.3) | 4 (12.5) | |
| Auditive and visual sensorial deterioration | 3 (2.8) | 1 (1.3) | 2 (6.3) | |
| Average nutritional status | 47 (43.5) | 34 (44.7) | 13 (40.6) | 0.407 |
| Mediocre nutritional status | 28 (25.9) | 17 (22.4) | 11 (34.4) | |
| Dehydrated | 2 (1.9) | 0 | 2 (6.3) | 0.086 |
| Daily use of hypnotics | 35 (32.4) | 22 (28.9) | 13 (40.6) | 0.477 |
| Previous ADOP | 8 (7.4) | 3 (3.9) | 5 (15.6) | 0.048 |
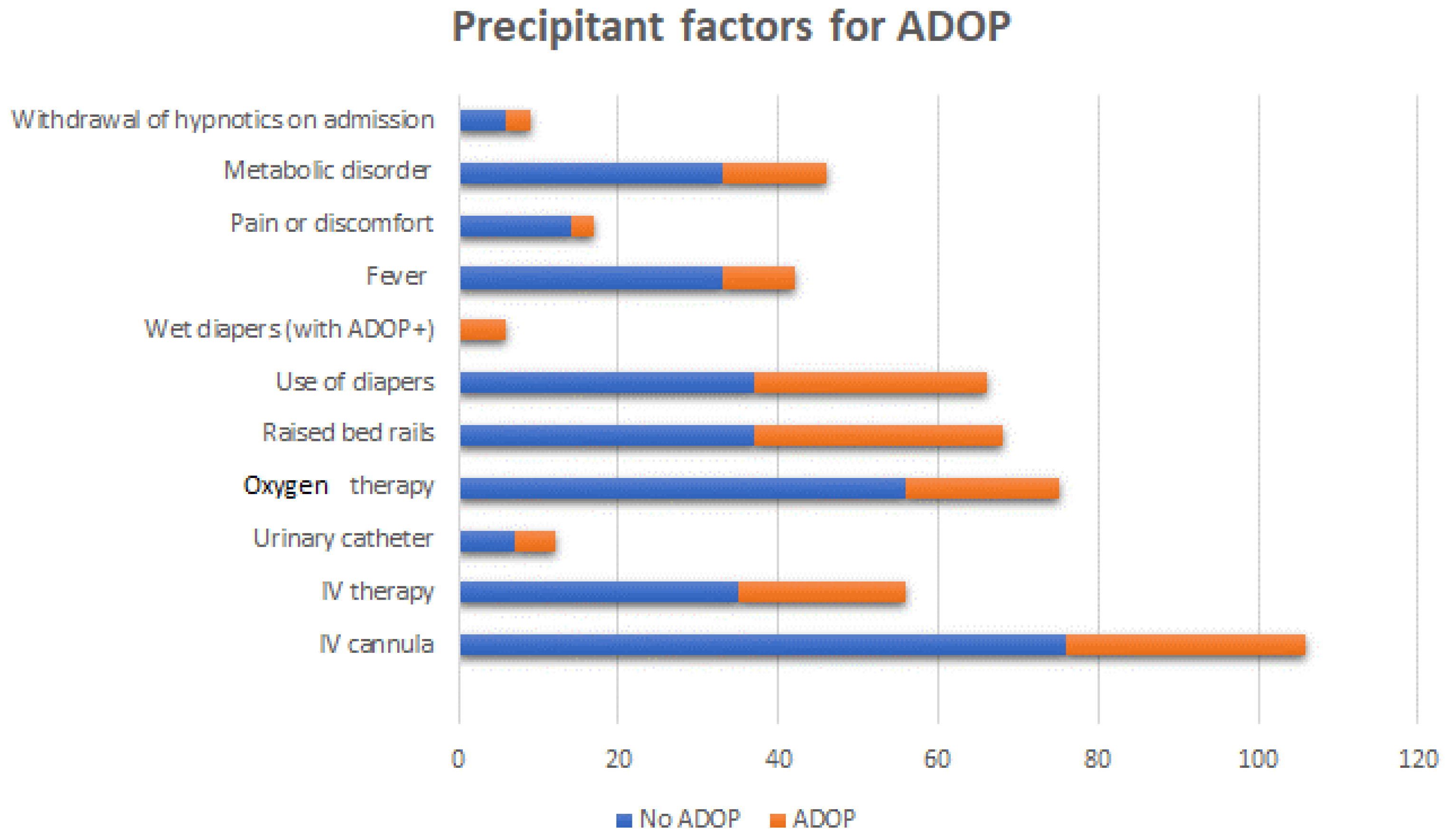
| Variable | Total (%) | No ADOP (%) | ADOP (%) | Chi2/Fisher (p) |
|---|---|---|---|---|
| IV cannula | 106 (98.1) | 76 (100) | 30 (96.8) | 0.116 |
| IV therapy | 56 (51.9) | 35 (47.3) | 21 (70) | 0.035 |
| Urinary catheter | 12 (11.1) | 7 (9.2) | 5 (16.1) | 0.323 |
| Oxygen therapy | 92 (85.2) | 56 (88.9) | 19 (65.5) | 0.021 |
| Raised bed rails | 68 (63) | 37 (48.7) | 31 (100) | 0.000 |
| Use of diapers | 66 (61.1) | 37 (48.7) | 29 (93.5) | 0.000 |
| Wet diapers (with ADOP+) | 6 (5.6) | 0 | 6 (21.4) | 0.557 |
| Fever | 42 (38.9) | 33 (44) | 9 (28.1) | 0.124 |
| Pain or discomfort | 17 (15.7) | 14 (18.9) | 3 (9.7) | 0.241 |
| Metabolic disorder | 51 (47.2) | 33 (43.4) | 13 (62.5) | 0.135 |
| Withdrawal of hypnotics on admission | 9 (8.3) | 6 (27.3) | 3 (9.4) | 1.0 |
| Variable | Verbal n (%) | Verbal and Pharmacologic n (%) | Pharmacologic and Physical n (%) | p | |
|---|---|---|---|---|---|
| Barthel Index | Severe dependent | 0 | 2 (10.5) | 0 | 0.511 |
| Moderate dependent | 4 (50) | 8 (42.1) | 2 (100) | ||
| Independent | 4 (50) | 9 (47.4) | 0 | ||
| Pfeiffer’s SPMSQ | Normal | 3 (37.5) | 9 (47.4) | 1 (50) | 0.976 |
| Slight–moderate | 4 (50) | 8 (42.1) | 1 (50) | ||
| Severe | 1 (12.5) | 2 (10.5) | 0 | ||
| Age | 65–75 | 3 (37.5) | 4 (21.1) | 1 (50) | 0.266 |
| 76–85 | 4 (50) | 5 (26.3) | 1 (50) | ||
| >86 | 1 (12.5) | 10 (52.6) | 0 | ||
| Sex | Male | 2 (25) | 9 (47.4) | 1 (50) | 0.541 |
| Female | 6 (75) | 10 (52.6) | 1 (50) | ||
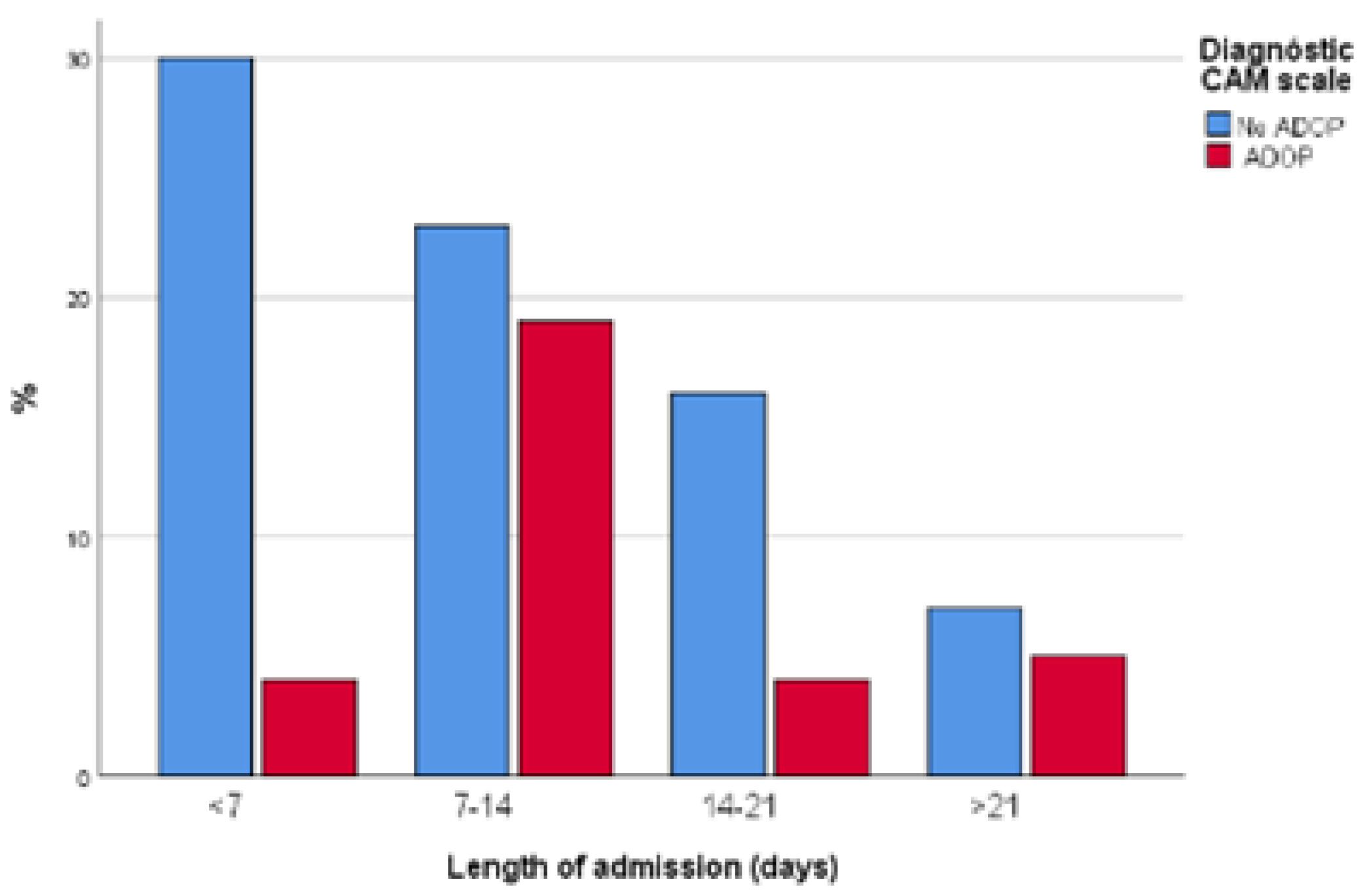
| Variable | NO ADOP n (%) | ADOP n (%) | (p) | ||||
| Length of admission | <7 days | 30 (39.5) | 4 (12.5) | 0.006 | |||
| 7–14 days | 23 (30.3) | 19 (59.4) | |||||
| 14–21 days | 16 (21.1) | 4 (12.5) | |||||
| >21 days | 7 (9.2) | 5 (15.6) | |||||
| Early mobilization | First week | 49 (64.5) | 5 (15.6) | 0.000 | |||
| Second week | 8 (10.5) | 4 (12.5) | |||||
| Third week | 0 | 2 (6.3) | |||||
| No early mobilization | 19 (25) | 21 (65.6) | |||||
|
Barthel Index (on discharge) | Severe dependent (<35) | 4 (5.5) | 12 (37.9) | 0.000 | |||
| Moderate dependent (40–80) | 19 (26) | 14 (48.3) | |||||
| Independent (>85) | 50 (68.6) | 3 (10.3) | |||||
| Pfeiffer’s SPMSQ (on discharge) | Severe impairment (8–10) | 2 (2.6) | 8 (27.6) | 0.000 | |||
| Moderate impairment (4–7) | 4 (5.2) | 14 (48.3) | |||||
| No impairment (0–3) | 67 (91.8) | 7 (24.1) | |||||
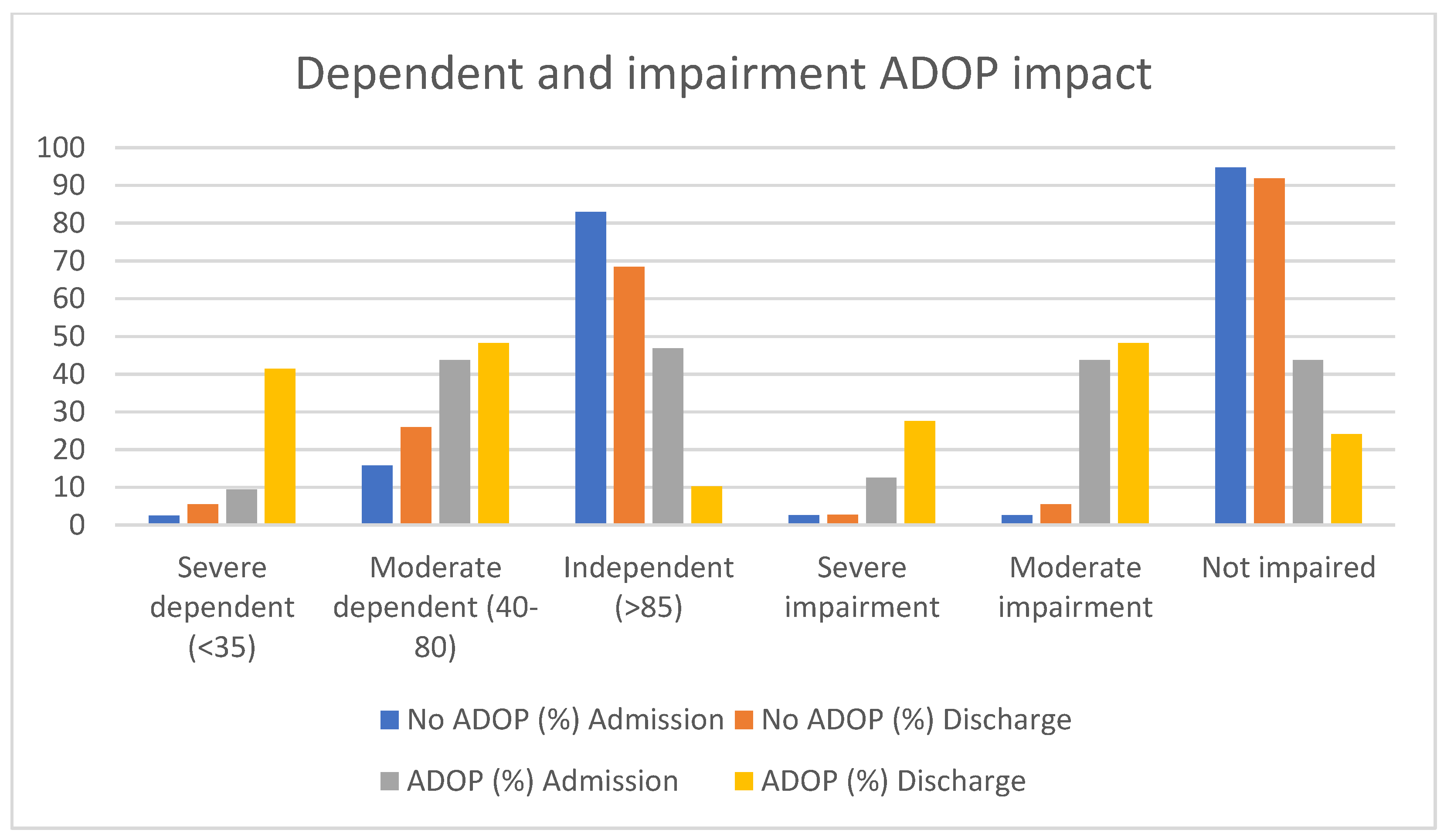
| No ADOP n/(%) | (p) | ADOP n/(%) | (p) | ||||
| Admission | Discharge | Admission | Discharge | ||||
| Barthel Index | Severe dependent (<35) | 1/2.5 | 4/5.5 | 3/9.4 | 12/41.4 | ||
| Moderate dependent (40–80) | 12/15.8 | 19/26 | 14/43.8 | 14/48.3 | |||
| Independent (>85) | 63/82.9 | 50/68.5 | 0.112 | 15/46.9 | 3/10.3 | 0.01 | |
| Pfeiffer’s SPMSQ | Severe impairment | 2/2.6 | 2/2.7 | 4/12.5 | 8/27.6 | ||
| Moderate impairment | 2/2.6 | 14/5.5 | 14/43.8 | 14/48.3 | |||
| Not impaired | 72/94.7 | 67/91.8 | 0.00 | 14/43.8 | 7/24.1 | 0.17 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jorge-Samitier, P.; Juárez-Vela, R.; Santolalla-Arnedo, I.; Antón-Solanas, I.; Gea-Caballero, V.; Sánchez-González, J.L.; Fernández-Rodrigo, M.T. Patient Profile and Management of Delirium in Older Adults Hospitalized Due to COVID-19. Healthcare 2022, 10, 724. https://doi.org/10.3390/healthcare10040724
Jorge-Samitier P, Juárez-Vela R, Santolalla-Arnedo I, Antón-Solanas I, Gea-Caballero V, Sánchez-González JL, Fernández-Rodrigo MT. Patient Profile and Management of Delirium in Older Adults Hospitalized Due to COVID-19. Healthcare. 2022; 10(4):724. https://doi.org/10.3390/healthcare10040724
Chicago/Turabian StyleJorge-Samitier, Pablo, Raúl Juárez-Vela, Iván Santolalla-Arnedo, Isabel Antón-Solanas, Vicente Gea-Caballero, Juan Luis Sánchez-González, and María Teresa Fernández-Rodrigo. 2022. "Patient Profile and Management of Delirium in Older Adults Hospitalized Due to COVID-19" Healthcare 10, no. 4: 724. https://doi.org/10.3390/healthcare10040724
APA StyleJorge-Samitier, P., Juárez-Vela, R., Santolalla-Arnedo, I., Antón-Solanas, I., Gea-Caballero, V., Sánchez-González, J. L., & Fernández-Rodrigo, M. T. (2022). Patient Profile and Management of Delirium in Older Adults Hospitalized Due to COVID-19. Healthcare, 10(4), 724. https://doi.org/10.3390/healthcare10040724