Decline of Lung Function in Knee and Spine Osteoarthritis in the Korean Population: Cross-Sectional Analysis of Data from the Korea National Health and Nutrition Examination Survey


Abstract
:1. Introduction
2. Subjects and Methods
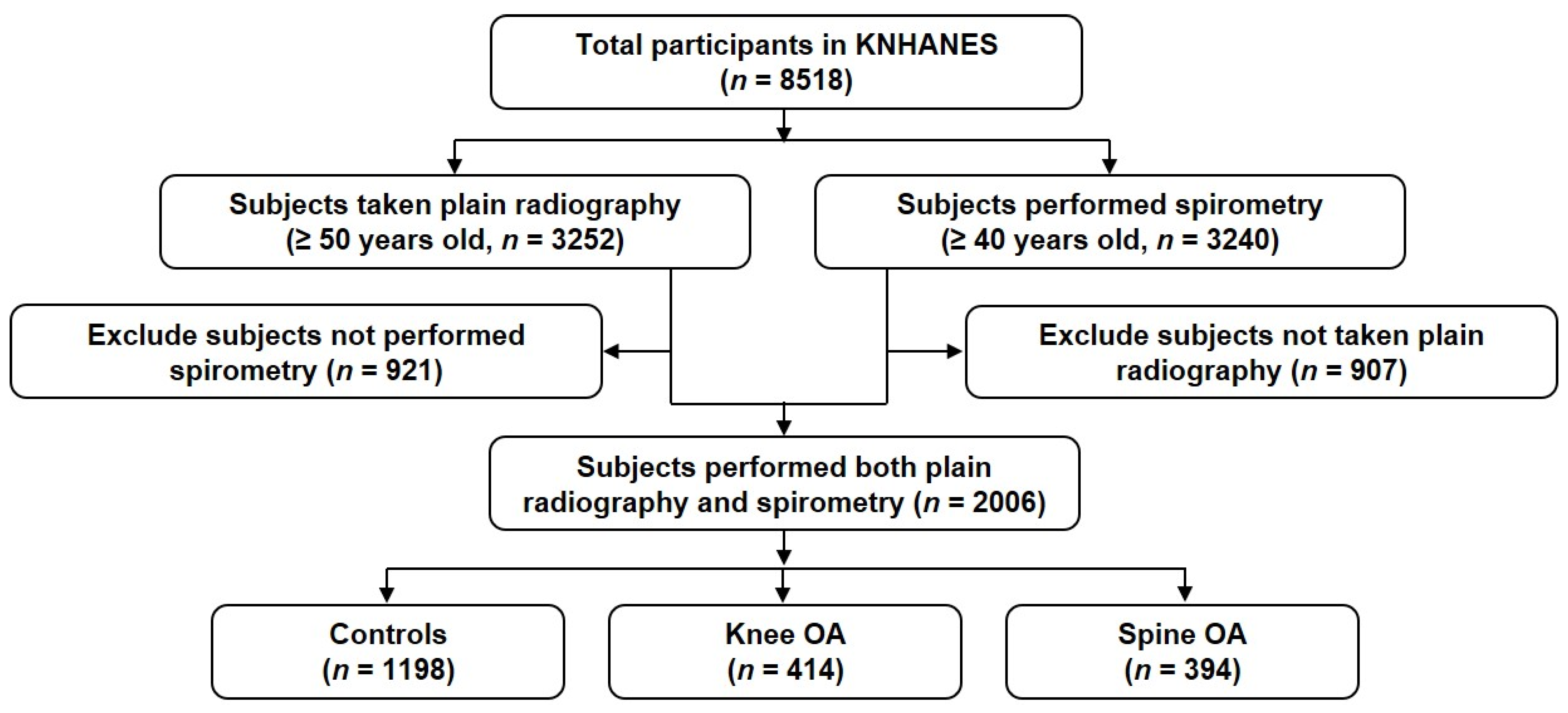
2.1. Study Population
2.2. Clinical Information
2.3. Radiographic Assessment
2.4. Lung Function Tests
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Comparison of Clinical Variables between OA and Controls
3.3. Comparison of Clinical Variables According to Presence of COPD
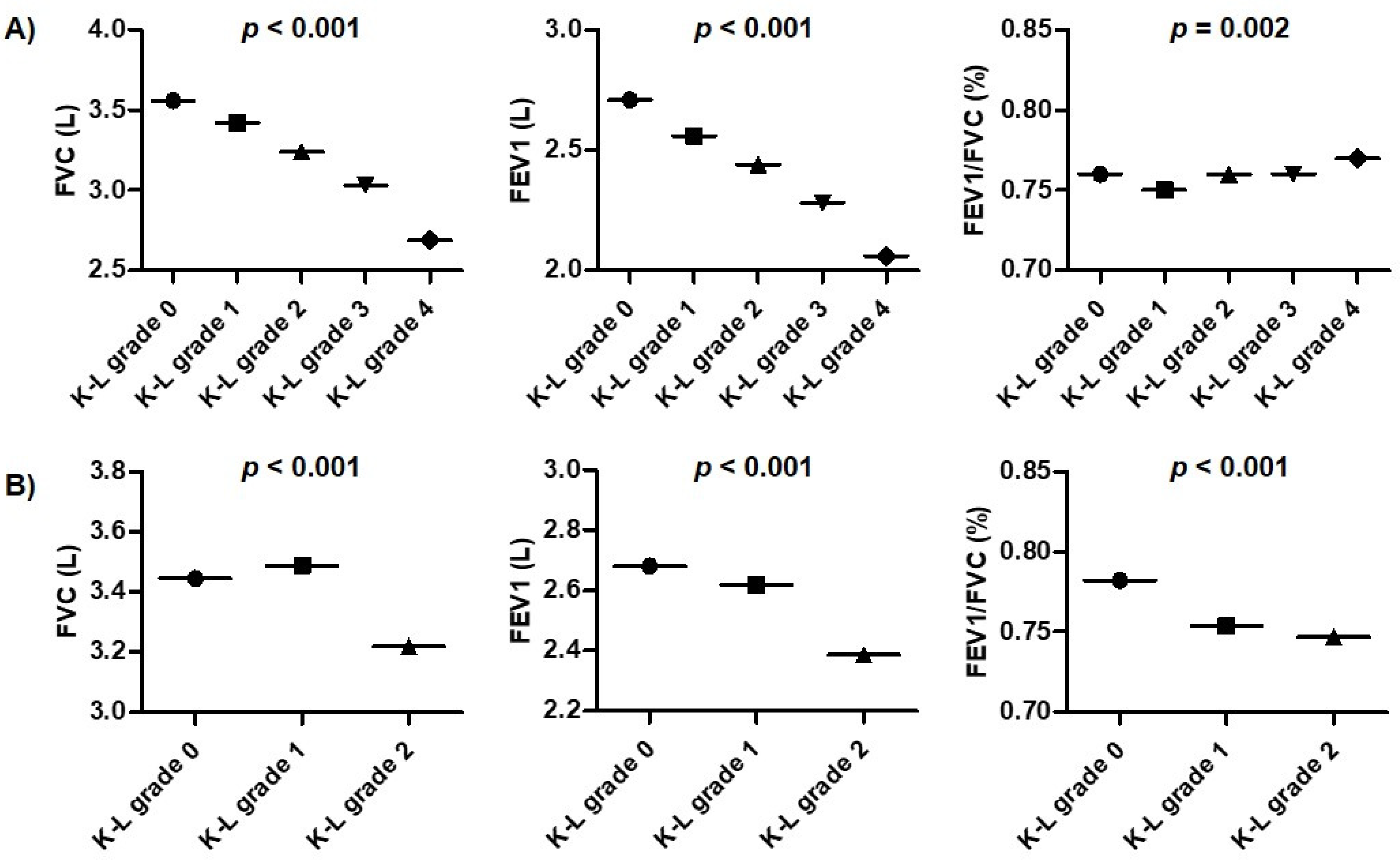
3.4. Comparison of Lung Function Tests between OA and Controls
3.5. Determination for Variables Related to COPD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Murphy, L.; Schwartz, T.A.; Helmick, C.G.; Renner, J.B.; Tudor, G.; Koch, G.; Dragomir, A.; Kalsbeek, W.D.; Luta, G.; Jordan, J.M. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Rheum. 2008, 59, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Osteo-arthrosis and disk degeneration in an urban population. Ann. Rheum. Dis. 1958, 17, 388–397. [Google Scholar] [CrossRef] [Green Version]
- van Saase, J.L.; van Romunde, L.K.; Cats, A.; Vandenbroucke, J.P.; Valkenburg, H.A. Epidemiology of osteoarthritis: Zoetermeer survey. Comparison of radiological osteoarthritis in a Dutch population with that in 10 other populations. Ann. Rheum. Dis. 1989, 48, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Battié, M.C.; Videman, T.; Parent, E. Lumbar disc degeneration: Epidemiology and genetic influences. Spine 2004, 29, 2679–2690. [Google Scholar] [CrossRef] [Green Version]
- Ko, S.; Vaccaro, A.R.; Lee, S.; Lee, J.; Chang, H. The prevalence of lumbar spine facet joint osteoarthritis and its association with low back pain in selected Korean populations. Clin. Orthop. Surg. 2014, 6, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.J.; Morey, V.; Kang, J.Y.; Kim, K.W.; Kim, T.K. Prevalence and Risk Factors of Spine, Shoulder, Hand, Hip, and Knee Osteoarthritis in Community-dwelling Koreans Older Than Age 65 Years. Clin. Orthop. Relat. Res. 2015, 473, 3307–3314. [Google Scholar] [CrossRef] [Green Version]
- Wesseling, J.; Welsing, P.M.; Bierma-Zeinstra, S.M.; Dekker, J.; Gorter, K.J.; Kloppenburg, M.; Roorda, L.D.; Bijlsma, J.W. Impact of self-reported comorbidity on physical and mental health status in early symptomatic osteoarthritis: The CHECK (Cohort Hip and Cohort Knee) study. Rheumatology 2013, 52, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Marshall, D.A.; Liu, X.; Barnabe, C.; Yee, K.; Faris, P.D.; Barber, C.; Mosher, D.; Noseworthy, T.; Werle, J.; Lix, L. Existing comorbidities in people with osteoarthritis: A retrospective analysis of a population-based cohort in Alberta, Canada. BMJ Open 2019, 9, e033334. [Google Scholar] [CrossRef] [Green Version]
- Swain, S.; Sarmanova, A.; Coupland, C.; Doherty, M.; Zhang, W. Comorbidities in Osteoarthritis: A Systematic Review and Meta-Analysis of Observational Studies. Arthritis Care Res. 2020, 72, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.B.; Yew, K.S. Diagnosis of chronic obstructive pulmonary disease. Am. Fam. Physician 2008, 78, 87–92. [Google Scholar] [PubMed]
- Barnes, P.J.; Celli, B.R. Systemic manifestations and comorbidities of COPD. Eur. Respir. J. 2009, 33, 1165–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wshah, A.; Guilcher, S.J.; Goldstein, R.; Brooks, D. Prevalence of osteoarthritis in individuals with COPD: A systematic review. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 1207–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.J.; Leem, A.Y.; Lee, S.H.; Song, J.H.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; Chung, K.S. Comorbidities in obstructive lung disease in Korea: Data from the fourth and fifth Korean National Health and Nutrition Examination Survey. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 1571–1582. [Google Scholar] [PubMed] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum Dis 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, N.; Muraki, S.; Oka, H.; Mabuchi, A.; En-Yo, Y.; Yoshida, M.; Saika, A.; Yoshida, H.; Suzuki, T.; Yamamoto, S.; et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: The research on osteoarthritis/osteoporosis against disability study. J. Bone Miner. Metab. 2009, 27, 620–628. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Rodriguez-Roisin, R. The 2011 revision of the global strategy for the diagnosis, management and prevention of COPD (GOLD)—Why and what. Clin. Respir. J. 2012, 6, 208–214. [Google Scholar] [CrossRef]
- Kim, S.K.; Choe, J.Y. Association between smoking and serum uric acid in Korean population: Data from the seventh Korea national health and nutrition examination survey. Medicine 2019, 98, e14507. [Google Scholar] [CrossRef]
- Kim, S.K.; Bae, J.; Choe, J.Y. The relationship between alcohol consumption and knee osteoarthritis in Korean population over 50 years-old: Results from Korea National Health and Nutrition Examination Survey. Medicine 2021, 100, e24746. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F. Cytokines in chronic obstructive pulmonary disease. Eur. Respir. J. Suppl. 2001, 34, 50s–59s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.J. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone. Res. 2017, 5, 16044. [Google Scholar] [CrossRef] [PubMed]
- Hacievliyagil, S.S.; Gunen, H.; Mutlu, L.C.; Karabulut, A.B.; Temel, I. Association between cytokines in induced sputum and severity of chronic obstructive pulmonary disease. Respir. Med. 2006, 100, 846–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, G.Q.; Chen, A.B.; Li, W.; Song, J.H.; Gao, C.Y. High MMP-1, MMP-2, and MMP-9 protein levels in osteoarthritis. Genet. Mol. Res. 2015, 14, 14811–14822. [Google Scholar] [CrossRef] [PubMed]
- Lipari, L.; Gerbino, A. Expression of gelatinases (MMP-2, MMP-9) in human articular cartilage. Int. J. Immunopathol. Pharmacol. 2013, 26, 817–823. [Google Scholar] [CrossRef] [Green Version]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Abbate, L.M.; Callahan, L.F.; et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar]
- Sarzi-Puttini, P.; Atzeni, F.; Fumagalli, M.; Capsoni, F.; Carrabba, M. Osteoarthritis of the spine. Semin. Arthritis Rheum. 2005, 34, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Reichert, M.M.; Davis, K.J. Lung function decline and outcomes in an adult population. Am. J. Respir. Crit. Care Med. 2006, 173, 985–990. [Google Scholar] [CrossRef] [Green Version]
- Santos, A.L.; Sinha, S.; Lindner, A.B. The Good, the Bad, and the Ugly of ROS: New Insights on Aging and Aging-Related Diseases from Eukaryotic and Prokaryotic Model Organisms. Oxid. Med. Cell Longev. 2018, 2018, 1941285. [Google Scholar] [CrossRef]
- McGuinness, A.J.; Sapey, E. Oxidative Stress in COPD: Sources, Markers, and Potential Mechanisms. J. Clin. Med. 2017, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Carey, M.A.; Card, J.W.; Voltz, J.W.; Germolec, D.R.; Korach, K.S.; Zeldin, D.C. The impact of sex and sex hormones on lung physiology and disease: Lessons from animal studies. Am. J. Physiol. Lung Cell. Mol. Physiol. 2007, 293, L272–L278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claassen, H.; Schünke, M.; Kurz, B. Estradiol protects cultured articular chondrocytes from oxygen-radical-induced damage. Cell. Tissue Res. 2005, 319, 439–445. [Google Scholar] [CrossRef]
- Lambert, A.A.; Putcha, N.; Drummond, M.B.; Boriek, A.M.; Hanania, N.A.; Kim, V.; Kinney, G.L.; McDonald, M.N.; Brigham, E.P.; Wise, R.; et al. Obesity Is Associated With Increased Morbidity in Moderate to Severe COPD. Chest 2017, 151, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Milne, S.; Jaw, J.E.; Yang, C.X.; Xu, F.; Li, X.; Obeidat, M.; Sin, D.D. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: A meta-analysis of clinical trials. Respir. Res. 2019, 20, 236. [Google Scholar] [CrossRef] [Green Version]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef]
- Vlietstra, L.; Stebbings, S.; Meredith-Jones, K.; Abbott, J.H.; Treharne, G.J.; Waters, D.L. Sarcopenia in osteoarthritis and rheumatoid arthritis: The association with self-reported fatigue, physical function and obesity. PLoS ONE 2019, 14, e0217462. [Google Scholar] [CrossRef] [Green Version]
- Jeon, H.; Lee, S.U.; Lim, J.Y.; Chung, S.G.; Lee, S.J.; Lee, S.Y. Low skeletal muscle mass and radiographic osteoarthritis in knee, hip, and lumbar spine: A cross-sectional study. Aging Clin. Exp. Res. 2019, 31, 1557–1562. [Google Scholar] [CrossRef]
- Koo, H.K.; Song, P.; Lee, J.H. Novel association between asthma and osteoarthritis: A nationwide health and nutrition examination survey. BMC Pulmonary Med. 2021, 21, 59. [Google Scholar] [CrossRef]
- Muraki, S.; Akune, T.; Oka, H.; Ishimoto, Y.; Nagata, K.; Yoshida, M.; Tokimura, F.; Nakamura, K.; Kawaguchi, H.; Yoshimura, N. Incidence and risk factors for radiographic lumbar spondylosis and lower back pain in Japanese men and women: The ROAD study. Osteoarthr. Cartil. 2012, 20, 712–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Age (years) | 59.2 (0.2) |
| Sex (female, n, %) | 1088 (50.3) |
| Body mass index (kg/m2) | 24.2 (0.1) |
| Smoking (n, %) * | |
| Non-smokers | 1145 (53.5) |
| Ex-smokers | 494 (24.8) |
| Current smokers | 348 (21.7) |
| Alcohol consumption (n, %) * | |
| Non-alcoholic | 360 (15.5) |
| Alcoholic | 1628 (84.5) |
| Comorbidities (n, %) * | |
| Hypertension | 707 (32.9) |
| Dyslipidemia | 427 (18.3) |
| Cerebral infarction | 39 (1.9) |
| Myocardial infarction/angina | 74 (3.5) |
| Pulmonary tuberculosis | 163 (8.0) |
| Bronchial asthma | 107 (5.6) |
| Diabetes mellitus | 261 (12.9) |
| COPD | 337 (16.4) |
| Parameters | Controls | Knee OA | p Value * | Spine OA | p Value * |
|---|---|---|---|---|---|
| Prevalence (n, %) | 1198 (62.1) | 414 (18.7) | 394 (19.2) | ||
| Age (years) | 57.3 (0.3) | 62.3 (0.5) | <0.001 | 62.5 (0.6) | <0.001 |
| Sex (female, n, %) | 604 (46.0) | 285 (66.3) | <0.001 | 199 (49.0) | 0.789 |
| Body mass index (kg/m2) | 23.9 (0.1) | 25.3 (0.2) | <0.001 | 24.2 (0.2) | 0.730 |
| Smoking (n, %) † | <0.001 | 0.871 | |||
| Non-smokers | 636 (49.1) | 296 (68.6) | 213 (52.8) | ||
| Ex-smokers | 317 (27.1) | 72 (15.9) | 105 (26.2) | ||
| Current smokers | 232 (23.8) | 43 (15.5) | 73 (20.9) | ||
| Alcohol consumption (n, %) † | <0.001 | 0.002 | |||
| Non-alcoholic | 178 (12.7) | 112 (24.2) | 70 (15.9) | ||
| Alcoholic | 1006 (87.3) | 300 (75.8) | 322 (84.1) | ||
| Comorbidities (n, %) † | |||||
| Hypertension | 346 (27.0) | 195 (44.1) | <0.001 | 166 (40.6) | <0.001 |
| Dyslipidemia | 254 (17.2) | 95 (22.0) | 0.497 | 78 (18.1) | 0.076 |
| Cerebral infarction | 29 (2.3) | 4 (0.8) | 0.069 | 6 (1.7) | 0.010 |
| Myocardial infarction/angina | 31 (2.6) | 20 (3.6) | 0.026 | 23 (6.1) | <0.001 |
| Pulmonary tuberculosis | 104 (8.4) | 39 (9.3) | 0.676 | 20 (5.4) | 0.218 |
| Bronchial asthma | 50 (4.5) | 32 (7.9) | 0.005 | 25 (6.7) | 0.012 |
| Diabetes mellitus | 133 (11.1) | 59 (14.2) | 0.097 | 69 (17.4) | <0.001 |
| COPD | 182 (15.0) | 63 (15.0) | 0.990 | 92 (22.1) | <0.001 |
| Parameters | Subjects without COPD | Subjects with COPD | p Value * |
|---|---|---|---|
| Prevalence (n, %) | 1669 (83.6) | 337 (16.4) | |
| Age (years) | 58.4 (0.2) | 63.5 (0.6) | <0.001 |
| Sex (female, n, %) | 1007 (55.7) | 81 (22.9) | <0.001 |
| Body mass index (kg/m2) | 24.4 (0.1) | 23.3 (0.2) | <0.001 |
| Smoking (n, %) † | <0.001 | ||
| Non-smokers | 1056 (59.4) | 89 (23.6) | |
| Ex-smokers | 345 (21.8) | 149 (40.1) | |
| Current smokers | 251 (18.8) | 97 (36.3) | |
| Alcohol intake (n, %) † | 0.302 | ||
| Non-alcoholic | 316 (16.2) | 44 (11.9) | |
| Alcoholic | 1336 (83.8) | 292 (88.1) | |
| Comorbidities (n, %) † | |||
| Hypertension | 580 (32.9) | 127 (32.8) | <0.001 |
| Dyslipidemia | 370 (19.1) | 57 (14.0) | 0.427 |
| Cerebral infarction | 31 (1.8) | 8 (2.4) | 0.068 |
| Myocardial infarction/angina | 59 (3.4) | 15 (3.8) | 0.249 |
| Pulmonary tuberculosis | 105 (6.2) | 58 (17.2) | <0.001 |
| Bronchial asthma | 68 (4.2) | 39 (12.3) | <0.001 |
| Diabetes mellitus | 215 (12.9) | 46 (12.7) | 0.053 |
| Knee OA | 351 (19.0) | 63 (17.2) | 0.876 |
| Spine OA | 302 (17.9) | 92 (25.9) | <0.001 |
| Parameters | Total | Controls | Knee OA | p Value * | Spine OA | p Value * |
|---|---|---|---|---|---|---|
| Spirometry | ||||||
| FVC (L) | 3.46 (0.02) | 3.56 (0.03) | 3.18 (0.05) | <0.001 | 3.41 (0.06) | 0.003 |
| FVC (%) | 92.0 (0.4) | 92.2 (0.48) | 91.1 (0.6) | 0.031 | 92.3 (0.7) | 0.665 |
| FEV1 (L) | 2.62 (0.02) | 2.71 (0.02) | 2.42 (0.04) | <0.001 | 2.52 (0.05) | <0.001 |
| FEV1 (%) | 90.8 (0.4) | 90.3 (0.5) | 91.9 (0.8) | 0.045 | 91.0 (1.0) | 0.619 |
| FEV1/FVC (%) | 0.76 (0.00) | 0.76 (0.00) | 0.76 (0.00) | 0.640 | 0.74 (0.01) | <0.001 |
| COPD stage | 0.523 | <0.001 | ||||
| Stage 0 | 1669 (83.6) | 1016 (85.0) | 351 (85.0) | 302 (77.9) | ||
| Stage 1 | 146 (7.2) | 78 (6.7) | 28 (5.9) | 40 (9.9) | ||
| Stage 2 | 176 (8.5) | 99 (7.9) | 33 (8.7) | 44 (10.3) | ||
| Stage 3 | 14 (0.7) | 5 (0.4) | 1 (0.2) | 8 (1.9) | ||
| Stage 4 | 1 (0.0) | 0 (0.0) | 1 (0.2) | 0 (0.0) |
| Parameters | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value * | OR | 95% CI | p Value * | |
| Age | 1.084 | 1.073–1.096 | <0.001 | 1.086 | 1.065–1.107 | <0.001 |
| Sex (ref: female) | 3.393 | 2.600–4.428 | <0.001 | 2.342 | 1.423–3.853 | 0.001 |
| Body mass index | 0.903 | 0.864–0.945 | <0.001 | 0.884 | 0.830–0.943 | <0.001 |
| Smoking (ref: non-smoker) † | ||||||
| Ex-smoker | 3.883 | 2.894–5.212 | <0.001 | 2.234 | 1.358–3.677 | <0.001 |
| Current smoker | 3.742 | 2.707–5.171 | <0.001 | 3.426 | 1.986–5.908 | 0.038 |
| Hypertension (ref: none) † | 1.656 | 1.299–2.110 | <0.001 | 0.910 | 0.645–1.284 | 0.588 |
| Pulmonary tuberculosis (ref: none) † | 3.714 | 2.577–5.353 | <0.001 | 3.277 | 1.976–5.434 | <0.001 |
| Bronchial asthma (ref: none) † | 3.389 | 2.192–5.242 | <0.001 | 3.022 | 1.934–4.722 | <0.001 |
| Spine OA (ref: controls) | 1.581 | 1.204–2.076 | 0.001 | 1.216 | 0.869–1.701 | 0.253 |
| Knee OA (ref: controls) | 1.062 | 0.765–1.475 | 0.716 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-K.; Kwak, S.G.; Choe, J.-Y. Decline of Lung Function in Knee and Spine Osteoarthritis in the Korean Population: Cross-Sectional Analysis of Data from the Korea National Health and Nutrition Examination Survey. Healthcare 2022, 10, 736. https://doi.org/10.3390/healthcare10040736
Kim S-K, Kwak SG, Choe J-Y. Decline of Lung Function in Knee and Spine Osteoarthritis in the Korean Population: Cross-Sectional Analysis of Data from the Korea National Health and Nutrition Examination Survey. Healthcare. 2022; 10(4):736. https://doi.org/10.3390/healthcare10040736
Chicago/Turabian StyleKim, Seong-Kyu, Sang Gyu Kwak, and Jung-Yoon Choe. 2022. "Decline of Lung Function in Knee and Spine Osteoarthritis in the Korean Population: Cross-Sectional Analysis of Data from the Korea National Health and Nutrition Examination Survey" Healthcare 10, no. 4: 736. https://doi.org/10.3390/healthcare10040736
APA StyleKim, S. -K., Kwak, S. G., & Choe, J. -Y. (2022). Decline of Lung Function in Knee and Spine Osteoarthritis in the Korean Population: Cross-Sectional Analysis of Data from the Korea National Health and Nutrition Examination Survey. Healthcare, 10(4), 736. https://doi.org/10.3390/healthcare10040736