
Access to Digital Information and Protective Awareness and Practices towards COVID-19 in Urban Marginalized Communities

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
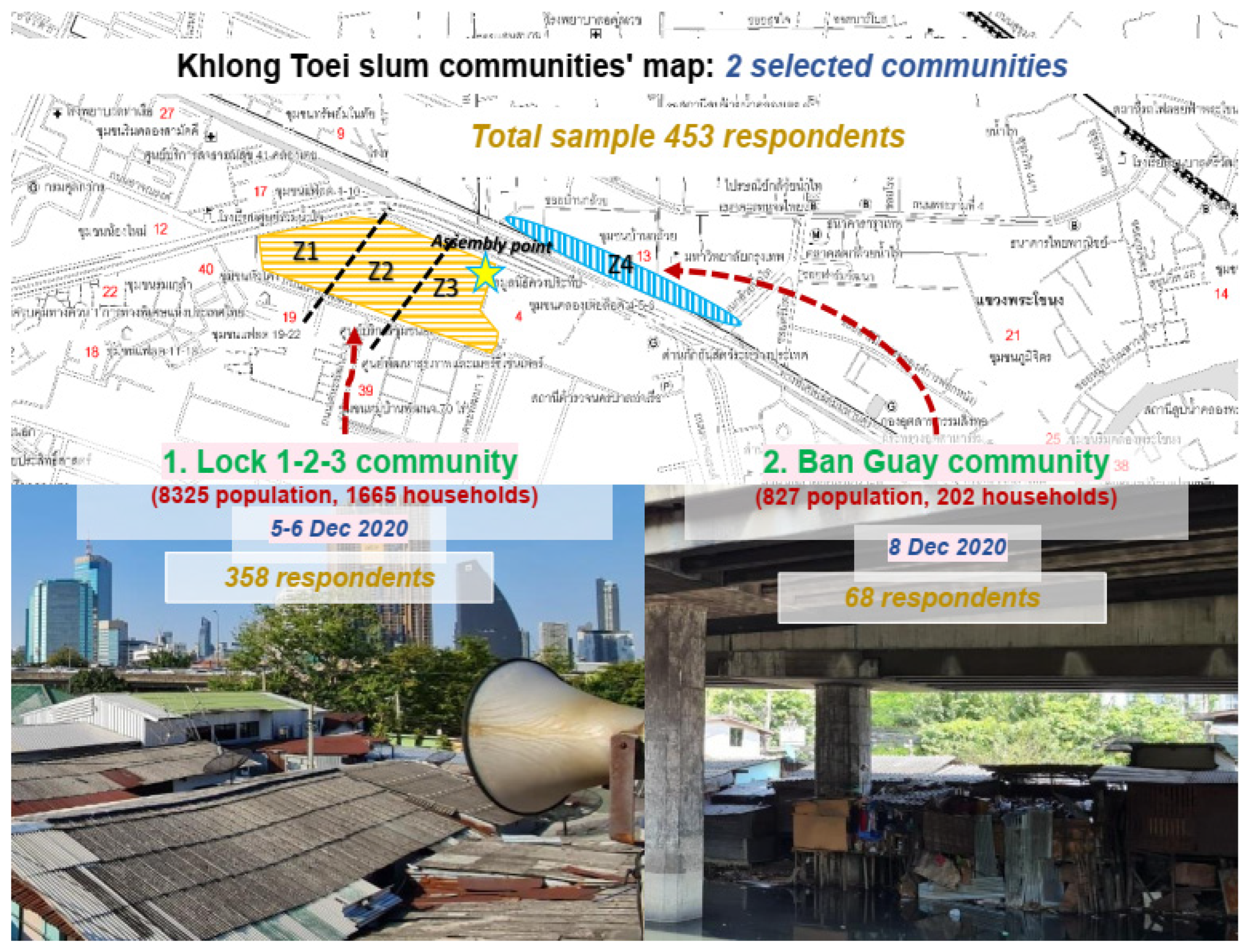
2.1. Site Selection
2.2. Research Design

- (1)
- Demographic information included age, gender, nationality, occupancy, education, family member, marital status, and state of residential occupancy.
- (2)
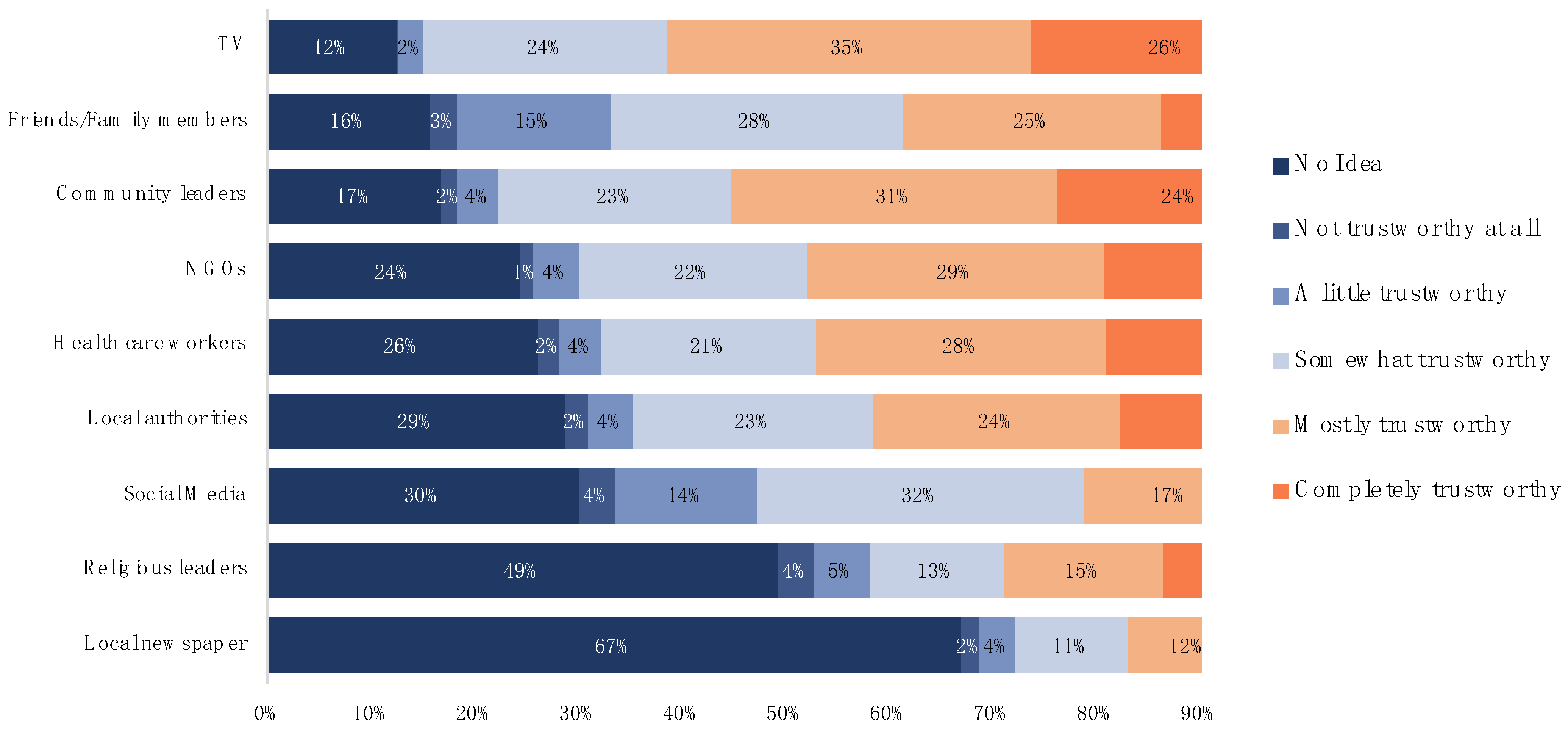
- Digital competence and skills and information sources included digital device occupancy and usage, digital competence during the pandemic, online service and information evaluation, reliability evaluation of information sources.
- (3)
- COVID-19 protection awareness and practices.
2.3. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Respondents
3.1.1. Marginalized Groups’ Profile
3.1.2. Marginalized Groups, Digital Communication, and Information Access
3.2. Factors Influencing Slum People’s Access to Digital COVID-19 Information during the Pandemic
4. Discussion
4.1. Role of Access to Online Information in Urban Marginalized People’s Awareness, Practices, and Protective Motivation Behaviors towards COVID-19
4.2. Digital Inequality among Urban Marginalized People
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johns Hopkins Coronavirus Resource Center. COVID-19 Global Information. Available online: https://coronavirus.jhu.edu/ (accessed on 14 December 2021).
- Mohammed, A.; Abed, H.; Hassoon, N. The Impact of Digital Communication on Social Networks: A Review. Int. J. Comput. Sci. Mob. Comput. 2016, 51, 183–190. [Google Scholar]
- Larsson, A. Utilizing Digitalization for Improved Knowledge Transfer in Project-Based Organizations: A Single Case Study of a Management Consulting Firm. Dissertation. 2018. Available online: http://diva-portal.org/ (accessed on 3 July 2021).
- Almuzaini, Y.; Mushi, A.; Aburas, A.; Yassin, Y.; Alamri, F.; Alahmari, A.; Yezli, S.; Khan, A.A.; Jokhdar, H.A. Risk Communication Effectiveness during COVID-19 Pandemic among General Population in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 779. [Google Scholar] [CrossRef] [PubMed]
- Farkas, C.; Gowadia, V.; Jain, A.; Roy, D. From XML to RDF: Syntax, Semantics, Security, and Integrity (Invited Paper). In IFIP Advances in Information and Communication Technology; Springer: Boston, MA, USA, 2004; Volume 193. [Google Scholar] [CrossRef]
- Sparf, J.; Ohman, S. On Risk and Disability Investigating the Influence of Disability and Social Capital on the Perception and Digital Communication of Risk. J. Risk Anal. Crisis Response 2014, 4, 20–33. [Google Scholar] [CrossRef] [Green Version]
- Ow Yong, L.M.; Xin, X.; Wee, J.M.L.; Poopalalingam, R.; Kwek, K.Y.C.; Thumboo, J. Perception Survey of Crisis and Emergency Risk Communication in an Acute Hospital in the Management of COVID-19 Pandemic in Singapore. BMC Public Health 2020, 20, 1919. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S. Digital 2020: APRIL GLOBAL STATSHOT. Available online: https://datareportal.com/reports/?tag=Global (accessed on 15 May 2022).
- Dimaggio, P.; Hargittai, E.; Celeste, C.; Shafer, S. Digital Inequality: From Unequal Access to Differentiated Use. In Social Inequality; Russell Sage Foundation: New York, NY, USA, 2004. [Google Scholar]
- Nguyen, T.P.L.; Seddaiu, G.; Roggero, P.P. Declarative or Procedural Knowledge? Knowledge for Enhancing Farmers’ Mitigation and Adaptation Behaviour to Climate Change. J. Rural. Stud. 2019, 67, 46–56. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Hargittai, E.; Marler, W. Digital Inequality in Communication during a Time of Physical Distancing: The Case of COVID-19. Comput. Hum. Behav. 2021, 120, 106717. [Google Scholar] [CrossRef]
- OECD Transparency. Communication and Trust: The Role of Public Communication in Responding to the Wave of Disinformation about the New Coronavirus. In Tackling Coronavirus (COVID-19); OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Ministry of Public Health: MOPH Department of Disease Control Proactive Testing for COVID-19 at Klong Toey Community. Available online: https://ddc.moph.go.th/ (accessed on 10 September 2021).
- Nguyen, T.P.L.; Pattanasri, S. The Influence of Nationality, Socio-demographic Factors on Urban Slum Dwellers’ Threat Appraisal, Awareness, and Protective Practices against COVID-19 in Thailand. Am. J. Trop. Med. Hygiene 2022, 1–6. [Google Scholar] [CrossRef]
- Baltar, F.; Brunet, I. Social Research 2.0: Virtual Snowball Sampling Method Using Facebook. Internet Res. 2012, 22, 57–74. [Google Scholar] [CrossRef]
- Moradzadeh, R.; Nazari, J.; Shamsi, M.; Amini, S. Knowledge, Attitudes, and Practices toward Coronavirus Disease 2019 in the Central Area of Iran: A Population-Based Study. Front. Public Health 2020, 8, 862. [Google Scholar] [CrossRef]
- Erfani, A.; Shahriarirad, R.; Ranjbar, K.; Mirahmadizadeh, A.; Moghadami, M. Knowledge, Attitude and Practice toward the Novel Coronavirus (COVID-19) Outbreak—A Population-Based Survey in Iran. Bull. World Health Organ. 2020, 30. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Carin, L.; Dzau, V.; Wong, T.Y. Digital Technology and COVID-19. Nat. Med. 2020, 26, 459–461. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.P.L.; Peña-García, A. Users’ Awareness, Attitudes, and Perceptions of Health Risks Associated with Excessive Lighting in Night Markets: Policy Implications for Sustainable Development. Sustainability 2019, 11, 6091. [Google Scholar] [CrossRef] [Green Version]
- Rippetoe, P.A.; Rogers, R.W. Effects of Components of Protection-Motivation Theory on Adaptive and Maladaptive Coping with a Health Threat. J. Personal. Soc. Psychol. 1987, 52, 596. [Google Scholar] [CrossRef]
- Renner, B.; Kwon, S.; Yang, B.H.; Paik, K.C.; Kim, S.H.; Roh, S.; Song, J.; Schwarzer, R. Social-Cognitive Predictors of Dietary Behaviors in South Korean Men and Women. Int. J. Behav. Med. 2008, 15, 4–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eppright, D.R.; Tanner, J.F.; Hunt, J.B. Knowledge and the Ordered Protection Motivation Model: Tools for Preventing AIDS. J. Bus. Res. 1994, 30, 13–24. [Google Scholar] [CrossRef]
- Fishbein, M.; Triandis, H.C.; Kanfer, F.H.; Becker, M.; Middlestadt, S.E. Factors Influencing Behavior and Behavior Change. In Handbook of Health Psychology; Taylor & Francis: Oxfordshire, UK, 2000. [Google Scholar]
- Tang, J.S.; Feng, J.Y. Residents’ Disaster Preparedness after the Meinong Taiwan Earthquake: A Test of Protection Motivation Theory. Int. J. Environ. Res. Public Health 2018, 15, 1434. [Google Scholar] [CrossRef] [Green Version]
- Gabbiadini, A.; Baldissarri, C.; Durante, F.; Valtorta, R.R.; de Rosa, M.; Gallucci, M. Together Apart: The Mitigating Role of Digital Communication Technologies on Negative Affect during the COVID-19 Outbreak in Italy. Front. Psychol. 2020, 11, 2763. [Google Scholar] [CrossRef]
- Seetharaman, P. Business Models Shifts: Impact of COVID-19. Int. J. Inf. Manag. 2020, 54, 102173. [Google Scholar] [CrossRef]
- Amankwah-Amoah, J.; Khan, Z.; Wood, G.; Knight, G. COVID-19 and Digitalization: The Great Acceleration. J. Bus. Res. 2021, 136, 602–611. [Google Scholar] [CrossRef]
- Chen, M.; Xu, S.; Husain, L.; Galea, G. Digital Health Interventions for COVID-19 in China: A Retrospective Analysis. Intell. Med. 2021, 1, 29–36. [Google Scholar] [CrossRef]
- Purnama, S.; Ulfah, M.; Machali, I.; Wibowo, A.; Narmaditya, B.S. Does Digital Literacy Influence Students’ Online Risk? Evidence from COVID-19. Heliyon 2021, 7, e07406. [Google Scholar] [CrossRef] [PubMed]
- Zeballos Rivas, D.R.; Lopez Jaldin, M.L.; Nina Canaviri, B.; Portugal Escalante, L.F.; Alanes Fernández, A.M.C.; Aguilar Ticona, J.P. Social Media Exposure, Risk Perception, Preventive Behaviors and Attitudes during the COVID-19 Epidemic in La Paz, Bolivia: A Cross Sectional Study. PLoS ONE 2021, 16, e0245859. [Google Scholar] [CrossRef] [PubMed]
- Austrian, K.; Pinchoff, J.; Tidwell, J.B.; White, C.; Abuya, T.; Kangwana, B.; Ochako, R.; Wanyungu, J.; Muluve, E.; Mbushi, F.; et al. COVID-19 Related Knowledge, Attitudes, Practices and Needs of Households in Informal Settlements in Nairobi, Kenya. Article, Preprint with THE LANCET. 2020. Available online: https://ssrn.com/abstract=3576785 (accessed on 7 July 2021).
- Pongutta, S.; Kantamaturapoj, K.; Phakdeesettakun, K.; Phonsuk, P. The Social Impact of the COVID-19 Outbreak on Urban Slums and the Response of Civil Society Organisations: A Case Study in Bangkok, Thailand. Heliyon 2021, 7, e07161. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Ervin, K.S.; Gardner, P.D.; Schmitt, N. Gender and the Internet: Women Communicating and Men Searching. Sex Roles 2001, 44, 363–379. [Google Scholar] [CrossRef]
- Beaunoyer, E.; Dupéré, S.; Guitton, M.J. COVID-19 and Digital Inequalities: Reciprocal Impacts and Mitigation Strategies. Comput. Hum. Behav. 2020, 111, 106424. [Google Scholar] [CrossRef]
- Seah, K.M. COVID-19: Exposing Digital Poverty in a Pandemic. Int. J. Surg. 2020, 79, 127. [Google Scholar] [CrossRef]
- Gonzales, A. The Contemporary US Digital Divide: From Initial Access to Technology Maintenance. Inf. Commun. Soc. 2016, 19, 234–248. [Google Scholar] [CrossRef]
- Robinson, L.; Schulz, J.; Khilnani, A.; Ono, H.; Cotten, S.R.; McClain, N.; Levine, L.; Chen, W.; Huang, G.; Casilli, A.A.; et al. Digital Inequalities in Time of Pandemic: COVID-19 Exposure Risk Profiles and New Forms of Vulnerability. First Monday 2020, 25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (Percent) | Access to Digital Communication (Frequency/Percent) | Non-Access Digital Communication (Frequency/Percent) | p-Value a |
|---|---|---|---|---|
| Total number of respondents | 453 | 220 | 233 | |
| Age (Years) | ||||
| 15–17 | 42 (9.3%) | - | 42 (18.0%) | <0.001 * |
| 18–35 | 168 (37.1%) | 89 (40.5%) | 79 (33.9%) | |
| 36–59 | 136 (30%) | 126 (57.3%) | 10 (4.3%) | |
| 60–90 | 107 (23.6%) | 5 (2.2%) | 102 (43.8%) | |
| Gender | ||||
| Male | 220 (48.6%) | 105 (47.7%) | 115 (49.4%) | 0.706 |
| Female | 232 (51.2%) | 114 (51.8%) | 118 (50.6%) | |
| Transgender | 1 (0.2%) | 1 (0.5%) | - | |
| Nationality | ||||
| Thai | 401 (88.5%) | 220 (100%) | 181 (77.7%) | <0.001 * |
| Myanmar | 28 (6.2%) | - | 28 (12%) | |
| Laos | 8 (1.8%) | - | 8 (3.4%) | |
| Cambodia | 12 (2.6%) | - | 12 (5.2%) | |
| Non-nationality | 4 (0.9%) | - | 4 (1.7%) | |
| Legal marital status | ||||
| Single | 205 (45.2%) | 86 (39.1%) | 119 (51.1%) | 0.001 * |
| Married | 195 (43.1%) | 112 (50.9%) | 83 (35.6%) | |
| Separated | 13 (2.9%) | 5 (2.3%) | 8 (3.4%) | |
| Cohabitation | 15 (3.3%) | 11 (5%) | 4 (1.7%) | |
| Widow(er) | 25 (5.5%) | 6 (2.7%) | 19 (8.2%) | |
| Family members (persons/household) | ||||
| Average household members = 5 people/household | 0.064 | |||
| State of residential occupancy | ||||
| Owner occupied | 54 (11.9%) | 30 (13.6%) | 24 (10.3%) | 0.154 |
| Squatter | 216 (47.7%) | 110 (50%) | 106 (45.5%) | |
| Tenant | 106 (23.4%) | 42 (19.1%) | 64 (27.5%) | |
| Living with a host family | 21 (4.6%) | 13 (5.9%) | 8 (3.4%) | |
| Others | 56 (12.4%) | 25 (11.4%) | 31 (13.3%) | |
| Highest Educational level | ||||
| None | 79 (17.4%) | 19 (8.6%) | 60 (25.8%) | <0.001 * |
| Primary | 92 (20.3%) | 30 (21.5%) | 62 (26.6%) | |
| Secondary | 112 (24.7%) | 54 (22.7%) | 58 (24.4%) | |
| Tertiary | 145 (32%) | 89 (40.5%) | 56 (22%) | |
| Others | 25 (5.6%) | 20 (6.7%) | 5 (1.2%) | |
| Occupation | ||||
| Trader | 65 (14.3%) | 35 (15.9%) | 30 (12.9%) | <0.001 * |
| Daily wage-earner | 153 (33.8%) | 81(36.8%) | 72 (30.9%) | |
| Public Servant | 1 (0.2%) | 1 (0.4%) | - | |
| Unemployed | 101 (22.3%) | 40 (18.6%) | 61 (25.8%) | |
| Student | 81 (17.9%) | 17 (7.7%) | 64 (27.5%) | |
| Private employee | 23 (5.1%) | 23 (10.3%) | - | |
| Others | 29 (6.4%) | 23 (10.3%) | 6 (2.9%) | |
| Variable | Frequency n = 453 (%) | Non-Access to Digital Information (%) | Access to Digital Information (%) | Chi-Square | df | p-Value |
|---|---|---|---|---|---|---|
| Types of COVID-19 WASH information | ||||||
| How to protect yourself | 400 (72%) | 209 (89.7%) | 191 (86.8%) | 0.90 | 1 | 0.340 |
| What to do in case of infection | 213 (38%) | 104 (44.6%) | 109 (49.5%) | 1.095 | 1 | 0.295 |
| Government response measure | 133 (24%) | 60 (25.8%) | 73 (33.2%) | 3.013 | 1 | 0.083 |
| How to protect elderly/vulnerable | 135 (30%) | 67 (28.8%) | 68 (30.9%) | 0.254 | 1 | 0.616 |
| How to behave in the public | 202 (36%) | 103 (44.4%) | 99 (45.0%) | 0.017 | 1 | 0.897 |
| COVID situation reports in Thailand (Number of Infection Cases, Death, Recovered) | 302 (55%) | 142 (60.9%) | 160 (72.7%) | 7.070 | 1 | 0.008 * |
| COVID global case and situation reports | 151 (27%) | 67 (28.8%) | 84 (38.2%) | 4.525 | 1 | 0.033 * |
| Urgent announcement/notice/measure from the government (e.g., Lockdown area, State quarantine) | 97 (17.5%) | 37 (15.9%) | 60 (27.3%) | 8.592 | 1 | 0.003 * |
| Sources of COVID-19 WASH information | ||||||
| Posters | 23 (4%) | 11 (5.0%) | 12 (5.2%) | 0.005 | 1 | 0.942 |
| Local television | 359 (65%) | 179 (76.8%) | 180 (81.8%) | 1.716 | 1 | 0.190 |
| Government COVID-19 websites | 20 (4.4%) | 2 (1.2%) | 18 (6.0%) | 1.566 | 1 | 0.211 |
| Neighbors/friends | 79 (14%) | 38 (16.3%) | 41 (18.6%) | 0.426 | 1 | 0.514 |
| Newspapers | 13 (2.9%) | 6 (2.6%) | 7 (3.2%) | 0.783 a | ||
| Radio | 18 (3%) | 6 (2.6%) | 12 (5.5%) | 0.150 a | ||
| Others | 7 (1%) | 2 (0.9%) | 5 (2.3%) | 0.273 a | ||
| Variable | Access to Online Information | |
|---|---|---|
| Beta | p-Value | |
| Age | −0.610 | 0.000 * |
| Gender | −0.110 | 0.003 * |
| Nationality | −0.169 | 0.000 * |
| Legal marital status | −0.037 | 0.369 |
| Total family members | −0.037 | 0.321 |
| State of residential occupancy | −0.059 | 0.118 |
| Highest educational level | 0.012 | 0.783 |
| Occupation | 0.032 | 0.409 |
| Model p-value | <0.001 * | |
| R2 | 0.411 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pattanasri, S.; Nguyen, T.P.L.; Vu, T.B.; Winijkul, E.; Ahmad, M.M. Access to Digital Information and Protective Awareness and Practices towards COVID-19 in Urban Marginalized Communities. Healthcare 2022, 10, 1097. https://doi.org/10.3390/healthcare10061097
Pattanasri S, Nguyen TPL, Vu TB, Winijkul E, Ahmad MM. Access to Digital Information and Protective Awareness and Practices towards COVID-19 in Urban Marginalized Communities. Healthcare. 2022; 10(6):1097. https://doi.org/10.3390/healthcare10061097
Chicago/Turabian StylePattanasri, Siwarat, Thi Phuoc Lai Nguyen, Thanh Bien Vu, Ekbordin Winijkul, and Mokbul Morshed Ahmad. 2022. "Access to Digital Information and Protective Awareness and Practices towards COVID-19 in Urban Marginalized Communities" Healthcare 10, no. 6: 1097. https://doi.org/10.3390/healthcare10061097
APA StylePattanasri, S., Nguyen, T. P. L., Vu, T. B., Winijkul, E., & Ahmad, M. M. (2022). Access to Digital Information and Protective Awareness and Practices towards COVID-19 in Urban Marginalized Communities. Healthcare, 10(6), 1097. https://doi.org/10.3390/healthcare10061097