1. Introduction
Augmented reality is a computer technology that brings digital information into reality and makes it seem as if it were in its original environment [
1]. This is a different concept from virtual reality (VR) because it exists and interacts in time and space like reality. Furthermore, advances in science and technology have made digital information, reality, and interaction between users smoothers. As a result, research is being conducted in various fields such as games and medical care, etc., and it is affecting society as a whole [
2].
In particular, active research is underway in the medical field. The most frequently studied subjects in diagnosis, surgery, rehabilitation, education, and training, including pain, stroke, Parkinson’s disease, Alzheimer’s disease, and degenerative neuropathy. This medical condition reduces balance and increases the risk of falling due to instability. However, continuous research is needed to determine whether AR-based rehabilitation is as effective as a physical therapist (PT)’s rehabilitation [
3].
Many studies are underway on whether AR-based rehabilitation can achieve the same effect as a PT. When comparing the improvement of balance ability by dividing 76 patients with Parkinson’s disease into two groups of exercise suggested by AR and proprioceptive exercise performed by a therapist, mobility, static, and dynamic balance (posture control) improved in both groups, and the average improvement in PT groups was greater. However, the actual difference between the two groups was minimal [
4]. In addition, AR-based exercise in groups with significantly reduced balance, such as the older people, stroke, and Parkinson’s disease, showed as much improvement in gait and balance as the therapist [
5,
6,
7].
Balance is the ability of the human body to maintain the position of COG within the BOS and process and execute input of visual, vestibular system, and somatic senses. And balance is essential to maintain stability from a static posture to a dynamic stance [
8]. The body’s equilibrium to maintain balance consists of inputs from three systems: 70% propitious system, 20% vestibular system, and 10% visual system, while the somatosensory system processes proprioceptive information input from spin-cerebellar paths [
9].
In many studies, proprioceptive exercise was carried out using tools such as BOSU and Swiss Ball to create the unstable ground, and a six-week proprioceptive program aimed at the older people greatly improved core stability and balance [
10]. In addition, proprioceptive exercise in patients with chronic ankle instability enhanced static and dynamic balance [
11]. Proprioceptive Neuromuscular Facility (PNF) stretching stimulates proprioceptors such as Golgi Tendon Organs (GTO) and Muscle Spindle located in muscles, tendons, and joints, and GTO activation inhibits muscle contraction. Neurophysiological mechanisms based on proprioceptive signals from these mechanical receptors can improve muscle length recovery and ROM, and as a result, it prevents biomechanical changes by relieving muscle tension. In the study comparing the effects of static, PNF, and mulligan stretching, the mulligan and hold-relax techniques of PNF stretching were effective [
12]. The proprioceptive exercise program that includes relaxation exercises such as stretching, slow walking, etc. during warm-up, and cool down exercises, greatly improve balance, muscle strength, and flexibility in old people and sitting women studies [
10,
13,
14].
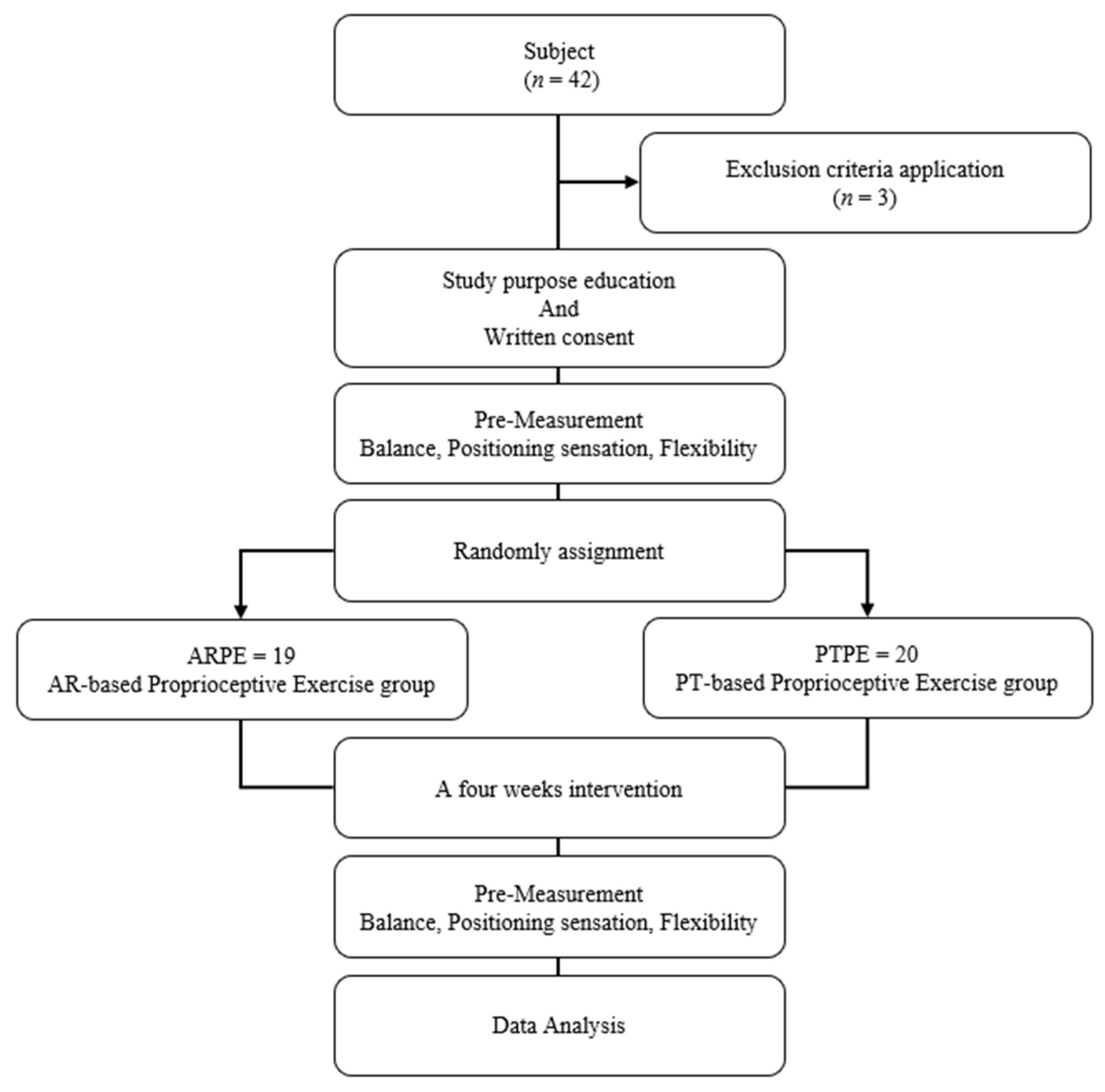
As a such, AR-based and Swiss Ball exercises greatly improved the patient’s balance and significantly reduced the risk of falling due to instability. However, there was no study to confirm the improvement of flexibility by applying both Swiss Ball and AR-based proprioceptive exercise. Therefore, this study aims to find out the effects of AR on its effectiveness and balance, positional sense, and flexibility.
4. Discussion
People who have problems with static balance are more dependent on proprioception than normal people. So, proprioceptive exercise is important in the rehabilitation process and needs to be designed appropriately [
22]. We have conducted balance training using unstable training tools such as balance boards, and these have been effective in stimulating proprioception [
10,
11]. Research based on augmented reality (AR), as well as existing educational tools, is being conducted. A four-week of AR exercise for older people showed improvements in lower limb function and balance, lowering the risk of falling, Im et al. reported [
23]. This suggests that AR alone can improve balance in general exercise therapy. This study confirmed that there was no significant difference between the two groups. In the case of regular people, it is difficult to determine the difference in effects without external stimulus, but due to changes in the environment, such as blocking visibility and providing unstable support, the dependence on unique perception is further increased [
24]. Hebner (2021) confirmed that the contribution of proprioception varies with the presence or absence of time when adjusting standing balance under various conditions [
25]. Previous studies prove that it can be affected by the presence or absence of vision and confirm that NC and PC of ST have improved in this study.
In addition, the exercise program of this study was also involved in improving dynamic balance and is related to YBT performance ability and muscle strength. Jaber et al. (2018) reported that the reduction of hip muscles affects the ability to maintain balance, negatively affecting functional movement [
26]. Nelson et al. (2021) demonstrated that neuromuscular regulation and intensity of the quadriceps group are important predictors of ANT arrival performance, and asymmetry of ANT arrival distance is associated with an increased risk of various limb injuries [
27]. In addition, according to Kang et al. (2015), the balanced movement obtained by trunk stabilization and extension is correlated with ANT’s maximum reach, and trunk flexion also has a positive effect on the maximum distance that can be reached backward [
28]. Wilson et al. (2018) announced that PM and PL reach are related to backward muscle strength, including hip extensor moment [
29]. In conclusion, the trunk, hips, and knees movement are all-important to YBT reach, and knee extensors in ANT and PM and hip extensors in PL and PM are the most notable factors. The exercise program in this study consisted of the exercise of these muscle groups, showed dynamic balance improvement in all directions, and was consistent with those reported in previous studies. In AR-based research, the results of YBT are not significantly different. The eight-week Otago exercise for middle-aged adults improved dynamic balance by improving hip muscles and pelvic stability. This indicates that the performance of AR-based strengthening and balance exercises is not different from the results of previous exercises performed by therapists [
30]. In this study, no significant difference was found between groups.
Muscle strength required to maintain balance is less when stationary than in functional movement. QipengSong et al. (2021) indicated that muscle strength was correlated with dynamic balance but not static balance [
31]. In addition, hip muscles correct large errors, while ankle muscles correct minor errors. Since the COP continues to change due to repulsive ground force, it is suggested that the ankle strategy, which is considered to help reduce the angle of swing of ankle torque, is a good strategy during static balance [
32]. However, this study does not include exercise targeting only the ankle, so it is expected that there was no significant difference in WDI.
Proprioception is a complex entity that includes a positioning sensation, a velocity sensation, and a sense of force to perform this movement in space [
33]. Positioning sensation is measured based on accuracy in reproducing the target angle [
34]. In this study, positioning sensation was improved than before, but it was not easy to identify statistically significant differences. For this reason, participants were recruited as young, healthy adults with no problems with proprioception. In addition, the stretching techniques applied to the two groups may not have been sufficient to apply time or tension enough to make a difference in positional sensations to all machine receptors around the knee. Aslan et al. (2018) immediately after applying HR-PNF, re-measurements were made over time and finally compared with the values before and after, confirming that the effect decreased over time. Additionally, HR-PNF application is also related to the relationship between the characteristics of YBT and the direction of arrival. It is explained as a decrease in reciprocal inhibition of gluteus maximus, and the difference between directions was maintained over time after stretching. In particular, it showed a significant improvement in PM and PL [
35]. Mani et al. (2021) applied static stretching and PNF stretching to the hamstring immediately and long-term to compare positional sensations, and immediately they were similar to each other. In the long run, PNF further improved the positioning sensation [
36]. This study was applied shorter than the previous study due to its four-week application. However, it is expected that it can be significantly improved when applied in the long run.
As mentioned earlier, stretching is effective in improving flexibility. In addition, stretching is essential to restore optimal muscle length. In particular, it has been reported that the tension of the hamstring causes biomechanical changes and negatively affects dynamic balance. Therefore, warming up, which includes stretching, results in beneficial results in exercise performance [
37]. Salami et al. (2021) announced that static stretching of the hamstring could have a positive effect on improving balance ability as well as increasing flexibility [
38]. Furthermore, Mani et al. (2021) compared static and PNF stretching in the short and long term and found that both groups greatly improved flexibility [
36]. Based on the results of previous studies, it can be confirmed that the application of warming up, including stretching in this study, greatly improved flexibility and had a positive effect on balance. Miklaus et al. (2021) announced that combining high-level exercise, including visual feedback, improves cognitive function and effectively controls motion. Exercise in virtual reality (VR), including visual feedback, has created a favorable environment for rehabilitation of the lower extremity of chronic patients after stroke and has better results in straight leg raise growth, which correlates flexibility with ROM [
39]. AR equipment can also have the same effect as VR because it recognizes the subject’s body, shows the subject’s location through the screen, and analyzes and provides the patient’s posture and movement at the same time as visual feedback. The effect of virtual and AR-based strengthening exercises on physical performance is explained by the social cognitive theory mechanism by meta-analysis. In other words, when subjects exercise in AR, they can observe and learn their action without rewards and punishment, and when their illuminated self-image and virtual models are similar to themselves, they are more likely to learn the results of their actions [
40]. Based on the experimental results of this study and the results of previous studies, AR has similar effects to PT.
This study has several limitations. This study has several limitations. It is challenging to generalize compared to various age groups because it targets healthy adults in their 20 s. In addition, there were restrictions on controlling the daily life of the subjects. However, as the results of this study and previous studies support, exercise (intervention) using AR can have a similar effect as a physical therapist. AR is easily accessible in areas such as islands and mountains that are medically alienated, and it is a new motivation for exercise. In addition, AR can overcome home limitations and improve exercise accuracy by providing immediate feedback without a therapist.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






