
Informal Caregivers’ Experiences with Performing Telemonitoring in Heart Failure Care at Home—A Qualitative Study

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Objective
3. Methods
3.1. Design
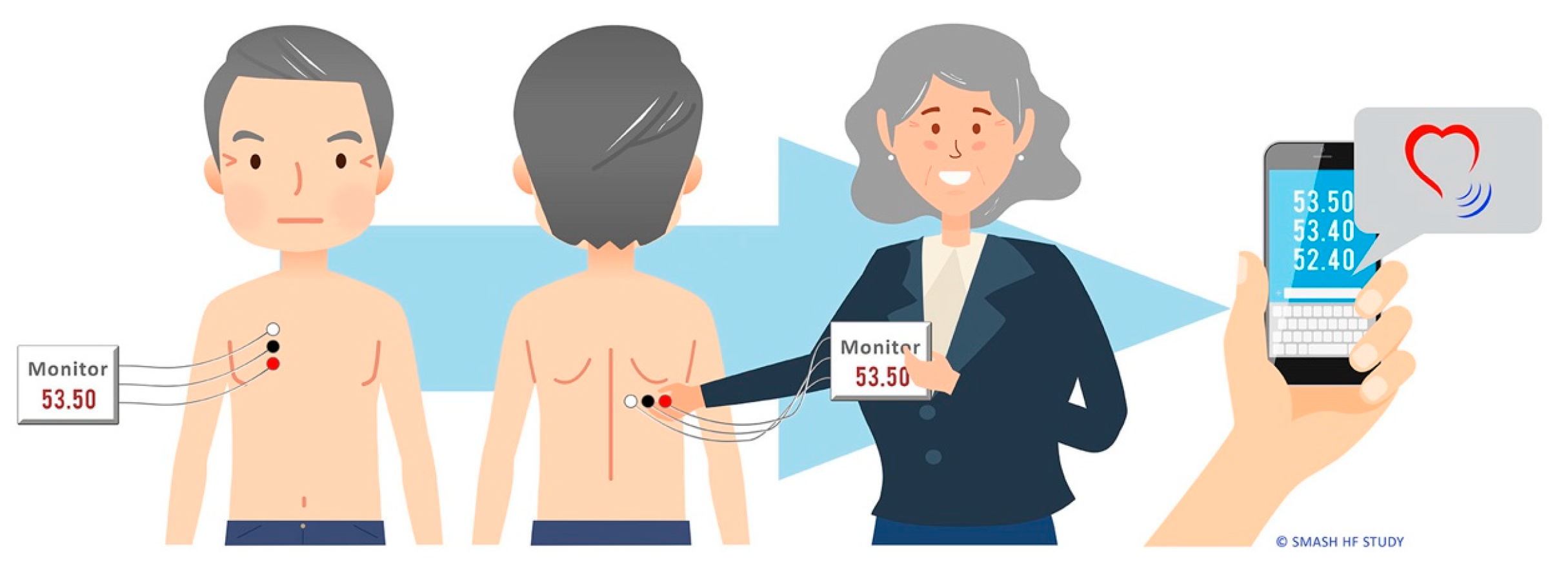
3.2. Setting and Telemonitoring Device
3.3. Participants
3.4. Education Session with Using Telemonitoring
3.5. Data Collection
3.6. Data Analysis
3.7. Ethical Consideration
4. Results
4.1. Access to Support
“I felt a bit uncertain about the patches and placing them in the right way. The nurse came to our home and confirmed that I did it correct. That was nice. Sometimes I also look at the illustrations, then I am more certain”.Participant no. 1 (wife).
4.2. Towards Routinizing
“In the beginning, the first two or three days it was a little bit difficult to locate the correct place for the electrode, but later this procedure went automatically. We were taking the measurements in the morning before I was leaving for work and almost at the same time. When we got used to it, the measurements took less than 10 min”.Participant no. 6 (wife).
“We did it together because it is so easy to forget. Suddenly my husband asked, where do I press now. Then I could sit next to him and say press start. Because you do get a bit occupied doing this and being two is a comfort. I get more information as well, about how things are with him, his condition”.Participant no. 5 (wife).
“One thing to mention is that he has been ill for å long period of time and been in and out of hospital, and he found it a bit troublesome. So, we had a little motivation talk. That is how it is sometimes he does not want to take his pills either and is part of his cannot bear it anymore”.Participant no. 4 (wife).
4.3. Mastering
“When I was talking to his doctor because his weight gained and shortness of breath increased, it was a support to have those measurements. I told him that the measurements from the device were worse. We discussed my husband’s symptoms and measurements. He knew we were in this study and performing measurements. My husband was re-admitted to hospital”.Participant no. 4 (wife).
5. Discussion
5.1. Ongoing Individualized Support
5.2. Establishing Routines Is Teamwork
5.3. Becoming an Expert
6. Conclusions
Limitations and Strengths
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, F.; Rodrigues, R. Informal Carers: Who Takes Care of Them? Report No.: 4/2010; European Centre For Social Welfare Policy and Research: Vienna, Austria, 2010. [Google Scholar]
- OECD. Health at a Glance 2019. Available online: https://www.oecd.org/health/health-systems/Health-at-a-Glance-2019-Chartset.pdf (accessed on 1 May 2022).
- Jaarsma, T.; Hill, L.; Bayes-Genis, A.; La Rocca, H.B.; Castiello, T.; Čelutkienė, J.; Marques-Sule, E.; Plymen, C.M.; Piper, S.E.; Riegel, B.; et al. Self-care of heart failure patients: Practical management recommendations from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Aamodt, I.T.; Strömberg, A.; Hellesø, R.; Jaarsma, T.; Lie, I. Tools to Support Self-Care Monitoring at Home: Perspectives of Patients with Heart Failure. Int. J. Environ. Res. Public Health 2020, 17, 8916. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Jaarsma, T.; Strömberg, A. A Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Riegel, B.; Jaarsma, T.; Lee, C.S.; Strömberg, A. Integrating Symptoms Into the Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2019, 42, 206–215. [Google Scholar] [CrossRef]
- Grant, J.S.; Graven, L.J. Problems experienced by informal caregivers of individuals with heart failure: An integrative review. Int. J. Nurs. Stud. 2018, 80, 41–66. [Google Scholar] [CrossRef]
- Hellesø, R.; Eines, J.; Fagermoen, M.S. The significance of informal caregivers in information management from the perspective of heart failure patients. J. Clin. Nurs. 2012, 21, 495–503. [Google Scholar] [CrossRef]
- Sedlar, N.; Lainscak, M.; Farkas, J. Living with Chronic Heart Failure: Exploring Patient, Informal Caregiver, and Healthcare Professional Perceptions. Int. J. Environ. Res. Public Health 2020, 17, 2666. [Google Scholar] [CrossRef]
- Kitko, L.; McIlvennan, C.K.; Bidwell, J.T.; Dionne-Odom, J.N.; Dunlay, S.M.; Lewis, L.M.; Meadows, G.; Sattler, E.L.; Schulz, R.; Strömberg, A.; et al. Family Caregiving for Individuals With Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2020, 141, e864–e878. [Google Scholar] [CrossRef]
- Durante, A.; Greco, A.; Annoni, A.M.; Steca, P.; Alvaro, R.; Vellone, E. Determinants of caregiver burden in heart failure: Does caregiver contribution to heart failure patient self-care increase caregiver burden? Eur. J. Cardiovasc. Nurs. 2019, 18, 691–699. [Google Scholar] [CrossRef]
- Buck, H.G.; Stromberg, A.; Chung, M.L.; Donovan, K.A.; Harkness, K.; Howard, A.M.; Kato, N.; Polo, R.; Evangelista, L.S. A systematic review of heart failure dyadic self-care interventions focusing on intervention components, contexts, and outcomes. Int. J. Nurs. Stud. 2018, 77, 232–242. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Isautier, J.M.; Copp, T.; Ayre, J.; Cvejic, E.; Meyerowitz-Katz, G.; Batcup, C.; Bonner, C.; Dodd, R.; Nickel, B.; Pickles, K.; et al. People’s Experiences and Satisfaction With Telehealth During the COVID-19 Pandemic in Australia: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e24531. [Google Scholar] [CrossRef] [PubMed]
- Walkden, J.-A.; McCullagh, P.J.; Kernohan, W.G. Patient and carer survey of remote vital sign telemonitoring for self-management of long-term conditions. BMJ Health Care Inform. 2019, 26, e100079. [Google Scholar] [CrossRef] [Green Version]
- Drews, T.E.; Laukkanen, J.; Nieminen, T. Non-invasive home telemonitoring in patients with decompensated heart failure: A systematic review and meta-analysis. ESC Heart Fail. 2021, 8, 3696–3708. [Google Scholar] [CrossRef] [PubMed]
- Shochat, M.K.; Shotan, A.; Blondheim, D.S.; Kazatsker, M.; Dahan, I.; Asif, A.; Rozenman, Y.; Kleiner, I.; Weinstein, J.; Frimerman, A.; et al. Non-Invasive Lung IMPEDANCE-Guided Preemptive Treatment in Chronic Heart Failure Patients: A Randomized Controlled Trial (IMPEDANCE-HF Trial). J. Card. Fail. 2016, 22, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, A. In the field: Notes on observation in qualitative research. J. Adv. Nurs. 2003, 41, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Aamodt, I.T.; Lycholip, E.; Celutkiene, J.; Von Lueder, T.; Atar, D.; Falk, R.S.; Hellesø, R.; Jaarsma, T.; Strömberg, A.; Lie, I. Self-Care Monitoring of Heart Failure Symptoms and Lung Impedance at Home Following Hospital Discharge: Longitudinal Study. J. Med. Internet Res. 2020, 22, e15445. [Google Scholar] [CrossRef]
- Aamodt, I.T.; Lycholip, E.; Celutkiene, J.; Strömberg, A.; Atar, D.; Falk, R.S.; Von Lueder, T.; Hellesø, R.; Jaarsma, T.; Lie, I. Health Care Professionals’ Perceptions of Home Telemonitoring in Heart Failure Care: Cross-Sectional Survey. J. Med. Internet Res. 2019, 21, e10362. [Google Scholar] [CrossRef] [Green Version]
- Gudmundsson, K.; Lyngå, P.; Rosenqvist, M.; Braunschweig, F. Monitoring of Daily Body Weight and Intrathoracic Impedance in Heart Failure Patients With a High Risk of Volume Overload Decompensation. Clin. Cardiol. 2016, 39, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Dejonckheere, M.; Vaughn, L.M. Semistructured interviewing in primary care research: A balance of relationship and rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindgren, B.-M.; Lundman, B.; Graneheim, U.H. Abstraction and interpretation during the qualitative content analysis process. Int. J. Nurs. Stud. 2020, 108, 103632. [Google Scholar] [CrossRef] [PubMed]
- Mattingly, C.; Grøn, L.; Meinert, L. Chronic Homework in Emerging Borderlands of Healthcare. Cult. Med. Psychiatry 2011, 35, 347–375. [Google Scholar] [CrossRef]
- Nick, J.M.; Roberts, L.R.; Petersen, A.B. Effectiveness of telemonitoring on self-care behaviors among community-dwelling adults with heart failure: A quantitative systematic review. JBI Evid. Synth. 2021, 19, 2659–2694. [Google Scholar] [CrossRef]
- Veenis, J.F.; Radhoe, S.P.; Hooijmans, P.; Brugts, J.J. Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go? Sensors 2021, 21, 887. [Google Scholar] [CrossRef]
- McBeath, K.C.C.; Angermann, C.E.; Cowie, M.R. Digital Technologies to Support Better Outcome and Experience of Care in Patients with Heart Failure. Curr. Heart Fail. Rep. 2022, 19, 75–108. [Google Scholar] [CrossRef]
- Nordfonn, O.K.; Morken, I.M.; Bru, L.E.; Husebø, A.M.L.; Bru, E.L. Patients’ experience with heart failure treatment and self-care—A qualitative study exploring the burden of treatment. J. Clin. Nurs. 2019, 28, 1782–1793. [Google Scholar] [CrossRef]
- Faragli, A.; Abawi, D.; Quinn, C.; Cvetkovic, M.; Schlabs, T.; Tahirovic, E.; Düngen, H.-D.; Pieske, B.; Kelle, S.; Edelmann, F.; et al. The role of non-invasive devices for the telemonitoring of heart failure patients. Heart Fail. Rev. 2021, 26, 1063–1080. [Google Scholar] [CrossRef]
- Bugajski, A.; Buck, H.; Zeffiro, V.; Morgan, H.; Szalacha, L.; Alvaro, R.; Vellone, E. The influence of dyadic congruence and satisfaction with dyadic type on patient self-care in heart failure. Eur. J. Cardiovasc. Nurs. 2021, 20, 268–275. [Google Scholar] [CrossRef]
- Kim, J.S.R.; Risbud, R.; Gray, C.; Banerjee, D.; Trivedi, R. The Dyadic Experience of Managing Heart Failure: A Qualitative Investigation. J. Cardiovasc. Nurs. 2020, 35, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Durante, A.; Ahtisham, Y.; Cuoco, A.; Boyne, J.; Brawner, B.; Juarez-Vela, R.; Vellone, E. Informal caregivers of people with heart failure and resilience: A convergent mixed methods study. J. Adv. Nurs. 2021, 78, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Dombestein, H.; Norheim, A.; Husebø, A.M.L. Understanding informal caregivers’ motivation from the perspective of self-determination theory: An integrative review. Scand. J. Caring Sci. 2020, 34, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Leiro, M.G.; Barge-Caballero, E. Advanced Heart Failure: Definition, Epidemiology, and Clinical Course. Heart Fail Clin. 2021, 17, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Canepa, M.; Straburzynska-Migaj, E.; Drozdz, J.; Fernandez-Vivancos, C.; Pinilla, J.M.G.; Nyolczas, N.; Temporelli, P.L.; Mebazaa, A.; Lainscak, M.; Laroche, C.; et al. Characteristics, treatments and 1-year prognosis of hospitalized and ambulatory heart failure patients with chronic obstructive pulmonary disease in the European Society of Cardiology Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2018, 20, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Ziaeian, B.; Hernandez, A.F.; DeVore, A.D.; Wu, J.; Xu, H.; Heidenreich, P.A.; Matsouaka, R.A.; Bhatt, D.L.; Yancy, C.W.; Fonarow, G.C. Long-term outcomes for heart failure patients with and without diabetes: From the Get With The Guidelines–Heart Failure Registry. Am. Heart J. 2019, 211, 1–10. [Google Scholar] [CrossRef] [Green Version]
- van Deursen, V.M.; Damman, K.; van der Meer, P.; Wijkstra, P.J.; Luijckx, G.J.; van Beek, A.; van Veldhuisen, D.J.; Voors, A.A. Co-morbidities in heart failure. Heart Fail Rev. 2014, 19, 163–172. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Ringard, A.; Sagan, A.; Saunes, I.S.; Lindahl, A.K. Norway: Health system review. Health Syst. Transit. 2013, 15, 1–162. [Google Scholar]
- Murauskiene, L.; Janoniene, R.; Veniute, M.; Van Ginneken, E.; Karanikolos, M. Lithuania: Health system review. Health Syst. Transit. 2013, 15, 1–150. [Google Scholar]



{kind=link}
{kind=link}
| Transcribed Texts | Meaning Unit | Sub-Category | Category |
|---|---|---|---|
| The first days there were alarms with bad coupling and difficulty with the pads. I sent an SMS to you. Participant no. 3 (wife). | There were alarms with bad coupling and difficulty with the pads the first days. I sent you an SMS. | Practical and technical support | Access to support |
| Those who are suffering from the disease should come to you and undergo training how to live and what to observe. Family doctors only continue prescription of the medication and do not explain anything. Participant no. 8 (son). | Those suffering from the disease should come to you for training how to live and what to observe. Family doctors only continue prescription and do not explain. | Medical support | |
| I had to go to him every day to help him to apply electrodes on his back. He decided to do it at 12.00 o’clock. It was the middle of my work. Participant no. 9 (son) | Every day in the middle of my work, I had to go to him and help him apply electrodes on his back. | Adjusting to a new routine | Towards routinizing |
| At first, I doubted whether the measurements were taken correctly with the electrodes appropriately and in the correct place. Participant no. 7 (daughter). I am managing this better and better all the time, and now it is almost automatic. Participant no. 3 (wife). | First, I doubted taking the measurements correctly and electrodes in the correct place. Now, it is almost automatic. I am managing better all the time. | A learning process | |
| We have made photos of the chest and the back showing where to place the patches and the sequence of the white, red, and black cable. Participant no. 6 (wife). | We made photos to show placement and sequence of the white, red, and black cable. | Assess measurements | Mastering |
| During this month we observed my mother’s condition when the measurements were low or very high, e.g., if socks made mark on her ancle or when it was very high, and her condition worsened with nausea and dizziness. Participant no. 9 (daughter). | When the measurements were low or high, we observed my mother’s condition, e.g., if socks made a mark on her ancle, nausea, or dizziness. | Assess symptoms |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aamodt, I.T.; Lie, I.; Lycholip, E.; Strömberg, A.; Jaarsma, T.; Celutkiene, J.; Hellesø, R. Informal Caregivers’ Experiences with Performing Telemonitoring in Heart Failure Care at Home—A Qualitative Study. Healthcare 2022, 10, 1237. https://doi.org/10.3390/healthcare10071237
Aamodt IT, Lie I, Lycholip E, Strömberg A, Jaarsma T, Celutkiene J, Hellesø R. Informal Caregivers’ Experiences with Performing Telemonitoring in Heart Failure Care at Home—A Qualitative Study. Healthcare. 2022; 10(7):1237. https://doi.org/10.3390/healthcare10071237
Chicago/Turabian StyleAamodt, Ina Thon, Irene Lie, Edita Lycholip, Anna Strömberg, Tiny Jaarsma, Jelena Celutkiene, and Ragnhild Hellesø. 2022. "Informal Caregivers’ Experiences with Performing Telemonitoring in Heart Failure Care at Home—A Qualitative Study" Healthcare 10, no. 7: 1237. https://doi.org/10.3390/healthcare10071237
APA StyleAamodt, I. T., Lie, I., Lycholip, E., Strömberg, A., Jaarsma, T., Celutkiene, J., & Hellesø, R. (2022). Informal Caregivers’ Experiences with Performing Telemonitoring in Heart Failure Care at Home—A Qualitative Study. Healthcare, 10(7), 1237. https://doi.org/10.3390/healthcare10071237