
Diabetes Management after a Therapeutic Education Program: A Qualitative Study

 ,
,  , and
, and 
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Participants
2.3. Procedure
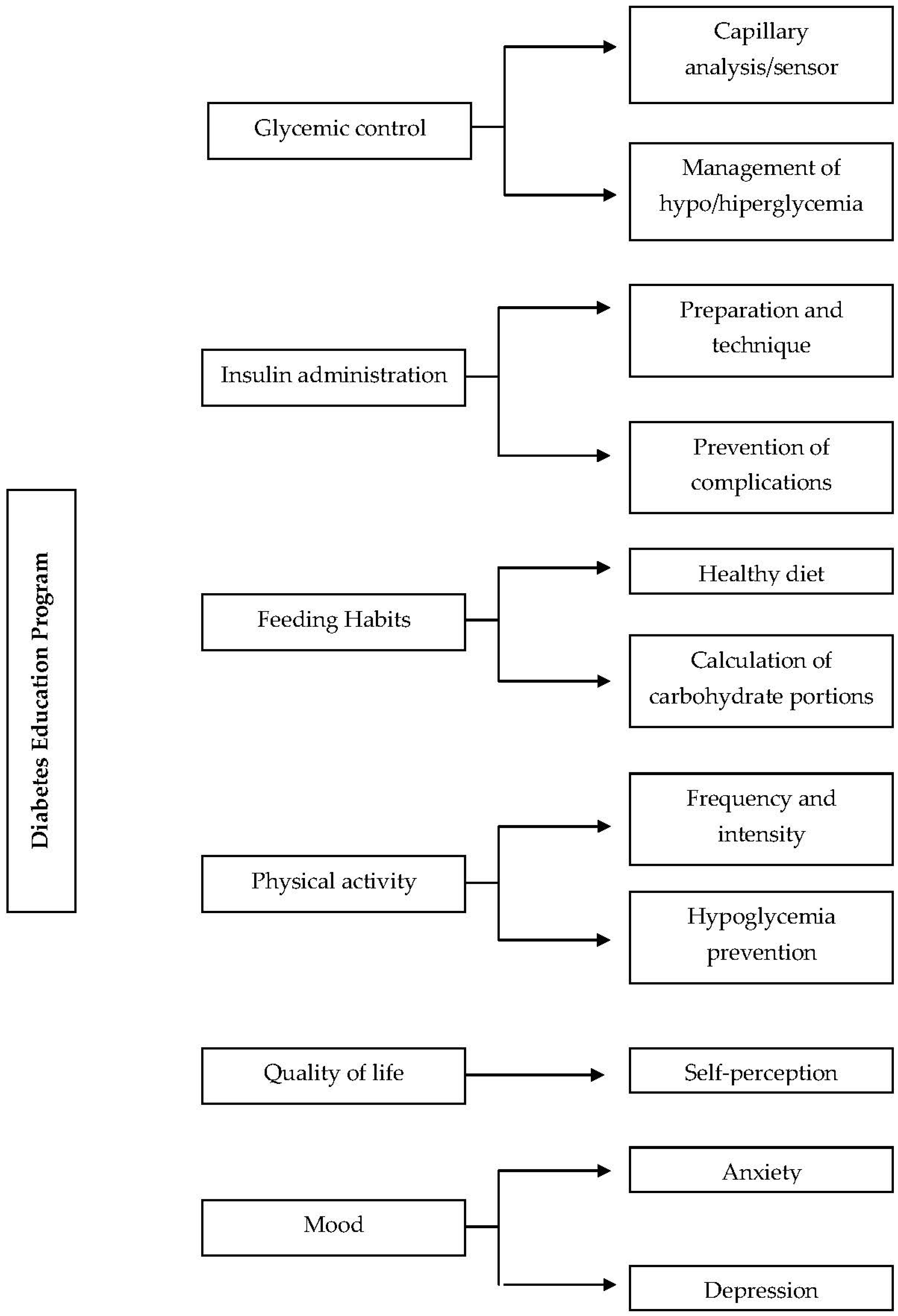
- First session. Insulin administration and blood glucose self-analysis.
- Second session. Management of hypoglycemia and hyperglycemia.
- Third session. Healthy diet adapted to the diabetic patient.
- Fourth session. Physical exercise.
2.4. Qualitative Data Collection
- “Do you think that the diabetes education program has been useful to improve your glycemic control?”
- “Have you implemented the recommendations offered in your daily life? Have you had any difficulty with it?”
- “Do you consider that your quality of life and your state of mind have improved after participating in the diabetes education program?”
- “Would you improve something of the course or add some aspect or activity?”
- “Is there anything else you would like to share with me or tell me?”
2.5. Qualitative Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Thematic Results
3.2.1. Theme 1: Usefulness of the Therapeutic Education Program in Glycemic Control
“When I had low blood sugar, I would have a cake and they recommended me to take a liquid food with sugar, juice or soft drink. These products are absorbed faster. I have to wait fifteen minutes and I make a new control to see if the hypoglycemia has resolved. I also did not know how to adjust my dose when I had high sugar and the nurse helped me calculate my sensitivity factor.”(42 years old, female, married)
“I sometimes skipped meals so I didn’t have to take insulin. I had decompensation, ups and downs. Since I attended the course, I am having a better control of my glucose. I have learned to adjust my insulin dose regimen, before it seemed difficult to me.”(23 years old, female, single)
“I didn’t know that the device had so many properties. I learned to program hypoglycemia and hyperglycemia alarms in the course. The nurse taught me how to interpret the trend arrows and how to write down the extra doses of insulin.”(38 years old, male, single)
“Since the hospital financed me the sensor, I have used it little. Sometimes, it fell off my arm… I didn’t know how to program it… In the course the nurse taught me protectors to prevent the fall and gave me tips to protect it and handle it better. This summer, I will even have it on the beach.”(24 years old, male, single)
3.2.2. Theme 2: Implementation of Program Recommendations and Difficulties Encountered
“I sometimes had nodules in my abdomen. The course nurse taught me that I could avoid it if I alternated the areas where I prick myself. Since the course, I have started to administer insulin in areas of the arms, legs and buttocks. I hope that little by little the nodules will be removed of my abdomen…”(54 years old, female, married)
“I used the needle of the insulin pen. I was stuck with the same needle for two or three days. The nurse told me that I had to change it after each puncture. I have ordered more needle at the pharmacy and I am trying to remember to change it.”(48 years old, male, single)
“I admit that I like cakes and sugary products… I don’t like the vegetables… In recent months, I have been trying to do things right and follow the advice that they gave me. It is difficult to change habits, but I am in the process.”(34 years old, male, single)
“I have never been clear carbohydrate serving counts. Since I went to the course I am learning and trying to adapt me. They also taught me to read the labels on packaged foods.”(42 years old, female, single)
“I really like swimming. Sometimes I was afraid to go down in the water, I had a bad time… but I don’t want to stop playing this sport because of diabetes. The nurse advised me to take an extra carbohydrate and adjust the insulin dose before doing the activity.”(51 years old, female, married)
3.2.3. Theme 3: Influence of Therapeutic Education on Quality of Life and Mood of the Patient
“A few months ago, I had many hypoglycemias and hyperglycemias. I got up at night with low blood sugar… I had hypoglycemia at work. Since the nurse gave me guidelines to improve my control, I am somewhat better… I am also more confident in what I have to do with my illness.”(43 years old, male, married)
“Since I have better control, I am more animated… I have dared to travel. I have clarified doubts so I am a little more relaxed. I think it is important to understand and treat in this disease because it gives you greater confidence and greatly reduces your anxiety.”(32 years old, female, single)
“I am eating better; I have learned new things from the sensor and I am trying to do things right. I feel more motivated more eager to go out and willing to take care of myself.”(41 years old, male, married)
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, W.; Wei, W.; Wang, J.; Lyu, Y.; Li, L. Effectiveness of a nurse-led online educational programme based on basic insulin therapy in patients with diabetes mellitus: A quasi-experimental trial. J. Clin. Nurs. 2021, 31, 2227–2239. [Google Scholar] [CrossRef]
- Hagger, V.; Hendrieckx, C.; Cameron, F.; Pouwer, F.; Skinner, T.C.; Speight, J. Diabetes distress is more strongly associated with HbA1c than depressive symptoms in adolescents with type 1 diabetes: Results from Diabetes MILES Youth-Australia. Pediatr. Diabetes 2018, 19, 840–847. [Google Scholar] [CrossRef]
- Luo, J.; Wang, H.; Li, X.; Zhou, Z.; Valimaki, M.; Whittemore, R.; Grey, M.; Guo, J. Factors associated with diabetes distress among adolescents with type 1 diabetes. J. Clin. Nurs. 2021, 30, 1893–1903. [Google Scholar] [CrossRef]
- Wang, A.; Zhang, H.; Zhang, J.; Zhang, Y.; Cao, H.; Liu, J.; Xu, H.; Chen, K. Adjuvant Effects of Health Education of Chinese Medicine for Chronic Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2020, 2020, 3738753. [Google Scholar] [CrossRef] [Green Version]
- Weissberg-Benchell, J.; Rausch, J.; Iturralde, E.; Jedraszko, A.; Hood, K. A randomized clinical trial aimed at preventing por psychosocial and glycemic outcomes in teens with type 1 diabetes (T1D). Contemp. Clin. Trials 2016, 49, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.H.; Ji, L.N.; Lu, J.M.; Liu, J.; Lou, Q.Q.; Liu, J.; Shen, L.; Zhang, M.X.; Gu, M.J. Efficacy of structured education in patients with type 2 diabetes mellitus receiving insulin treatment. J. Diabetes 2014, 6, 290–297. [Google Scholar] [CrossRef]
- Heller, S.R.; Gianfrancesco, C.; Taylor, C.; Elliott, J. What are the characteristics of the best type 1 diabetes patient education programmes (from diagnosis to long-term care), do they improve outcomes and what is required to make them more effective? Diabetes Med. 2020, 37, 545–554. [Google Scholar] [CrossRef]
- Heller, S.; Lawton, J.; Amiel, S.; Cooke, D.; Mansell, P.; Brennan, A. Improving Management of type 1 Diabetes in the UK: The Dose Adjustment for Normal Eating (DAFNE) Programme as a Research Test-Bed. A Mixed-Method Analysis of the Barriers to and Facilitators of Successful Diabetes Self-Management, a Health Economic Analysis, a Cluster Randomised Controlled Trial of Different Models of Delivery of an Educational Intervention and the Potential of Insulin Pumps and Additional Educator Input to Improve Outcome; National Institute for Health and Care Research (NIHR): Sothampton, UK, 2014. [Google Scholar]
- National Institute of Health and Care Excellence (NICE). Guidance on the Use of Patient-Education Models for Diabetes; National Institute of Health and Care Excellence (NICE): London, UK, 2003. [Google Scholar]
- He, X.; Li, J.; Wang, B.; Yao, Q.; Li, L.; Song, R.; Shi, X.; Zhang, J. Diabetes self-management education reduces risk of all-cause mortality in type 2 diabetes patients: A systematic review and meta-analysis. Endocrine 2017, 55, 712–731. [Google Scholar] [CrossRef]
- Humayun, M.A.; Jenkins, E.; Knott, J.; Ryder, J.; Shaban, C.; Weiss, M.; Charman, J.; Cavan, D.; Brooks, A. Intensive structured education for type 1 diabetes management using BERTIE: Long-term follow-up to assess impacto n glycaemic control and quality of life índices. Diabetes Res. Clin. Pract. 2018, 143, 275–281. [Google Scholar] [CrossRef]
- Davis, J.; Fischl, A.; Beck, J.; Browning, L.; Carter, A.; Condon, J.E. National Standards for Diabetes Self-Management Education and Support. Sci. Diabetes Self-Manag. Care 2022, 48, 44–59. [Google Scholar] [CrossRef]
- Chrvala, C.A.; Sherr, D.; Lipman, R.D. Diabetes self-management education for adults with type 2 diabetes mellitus: A systematic review of the effect on glycemic control. Patient Educ. Couns. 2016, 99, 926–943. [Google Scholar] [CrossRef] [Green Version]
- Zhao, F.F.; Suhonen, R.; Koskinen, S.; Leino-Kilpi, H. Theory based self-management educational interventions on patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. J. Adv. Nurs. 2017, 73, 812–833. [Google Scholar] [CrossRef]
- Bernard, M.; Lehmann, T.; Hecht, L.; Fabisch, G.; Harder, A.; Müller, N.; Luck-Sikorski, C. Efficacy of Dia Life, an Education Program for Relatives of Adults with Diabetes—A Cluster Randomized Controlled Trial. Patient Educ. Couns. 2022, 105, 2158–2165. [Google Scholar] [CrossRef]
- De Melo-Ghisi, G.L.; Aultman, C.; Konidis, R.; Foster, E.; Tahsinul, A.; Sandison, N.; Sarin, M.; Oh, P. Effectiveness of an education intervention associated with an exercise program in improving disease-related knowledge and health behaviours among diabetes patients. Patient Educ. Cons. 2020, 103, 1790–1797. [Google Scholar] [CrossRef]
- Alonso-Domínguez, R.; García-Ortiz, L.; Patino-Alonso, M.C.; Sánchez-Aguadero, N.; Gómez-Marcos, M.A.; Recio-Rodríguez, J.I. Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus: A Controlled and Randomized Study (EMID Study). Nutrients 2019, 11, 162. [Google Scholar] [CrossRef] [Green Version]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuas: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef]
- Geremia, G.; Fornari, A.; Tschiedel, B. Comparison of the effect of a compact vs a conventional, long-term education program on metabolic control in children and adolescents with type 1 diabetes: A pilot, randomized clinical trial. Pediat. Diabetes 2019, 20, 778–784. [Google Scholar] [CrossRef]
- Alvarado-Martel, D.; Ruiz-Fernández, M.A.; Cuadrado-Vigaray, M.; Carrillo, A.; Boronat, M.; Expósito-Montesdeoca, A.; Wägner, A.M. Identification of Psychological Factors Associated with Adherence to Self-Care Behaviors amongst Patients with Type 1 Diabetes. J. Diabetes Res. 2019, 2019, 6271591. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Blaikie, N. Confounding issues related to determining sample size in qualitative research. Int. J. Soc. Res. Methodol. 2018, 21, 635–641. [Google Scholar] [CrossRef]
- Romero-Castillo, R.; Pabón-Carrasco, M.; Jiménez-Picón, N.; Ponce-Blandón, J.A. Effects of Nursing Diabetes Self-Management Education on Glycemic Control and Self-Care in Type 1 Diabetes: Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 5079. [Google Scholar] [CrossRef]
- Fisher, L.; Hessler, D.; Polonsky, W.H.; Masharani, U.; Guzman, S.; Bowyer, V. T1-REDEEM: A Randomized Controlled Trial to Reduce Diabetes Distress Among Adults With Type 1 Diabetes. Diabetes Care 2018, 41, 1862–1869. [Google Scholar] [CrossRef] [Green Version]
- Azami, G.; Soh, K.L.; Sazlina, S.G.; Salmiah, M.S.; Aazami, S.; Mozafari, M.; Taghinejad, H. Effects of a Nurse-Led Diabetes Self-Management Education Program on Glycosylated Hemoglobin among Adults with Type 2 Diabetes. J. Diabetes Res. 2018, 2018, 4930157. [Google Scholar] [CrossRef]
- Young, H.M.; Miyamoto, S.; Dharmar, M.; Tang-Feldman, Y. Nurse Coaching and Mobile Health Compared With Usual Care to Improve Diabetes Self-Efficacy for Persons With Type 2 Diabetes: Randomized Controlled Trial. JMIR MHealth UHealth 2020, 8, e16665. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Castillo, R.; Pabón-Carrasco, M.; Jiménez-Picón, N.; Ponce-Blandón, J.A. Diabetes Management after a Therapeutic Education Program: A Qualitative Study. Healthcare 2022, 10, 1375. https://doi.org/10.3390/healthcare10081375
Romero-Castillo R, Pabón-Carrasco M, Jiménez-Picón N, Ponce-Blandón JA. Diabetes Management after a Therapeutic Education Program: A Qualitative Study. Healthcare. 2022; 10(8):1375. https://doi.org/10.3390/healthcare10081375
Chicago/Turabian StyleRomero-Castillo, Rocío, Manuel Pabón-Carrasco, Nerea Jiménez-Picón, and José Antonio Ponce-Blandón. 2022. "Diabetes Management after a Therapeutic Education Program: A Qualitative Study" Healthcare 10, no. 8: 1375. https://doi.org/10.3390/healthcare10081375
APA StyleRomero-Castillo, R., Pabón-Carrasco, M., Jiménez-Picón, N., & Ponce-Blandón, J. A. (2022). Diabetes Management after a Therapeutic Education Program: A Qualitative Study. Healthcare, 10(8), 1375. https://doi.org/10.3390/healthcare10081375