
Impact of the COVID-19 Pandemic on Utilization of Inpatient Mental Health Services in Shanghai, China


 and
and
Abstract
:1. Background
2. Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
3.1. Participants
3.2. Descriptive Data
Characteristics of Inpatients
3.3. Outcome Data
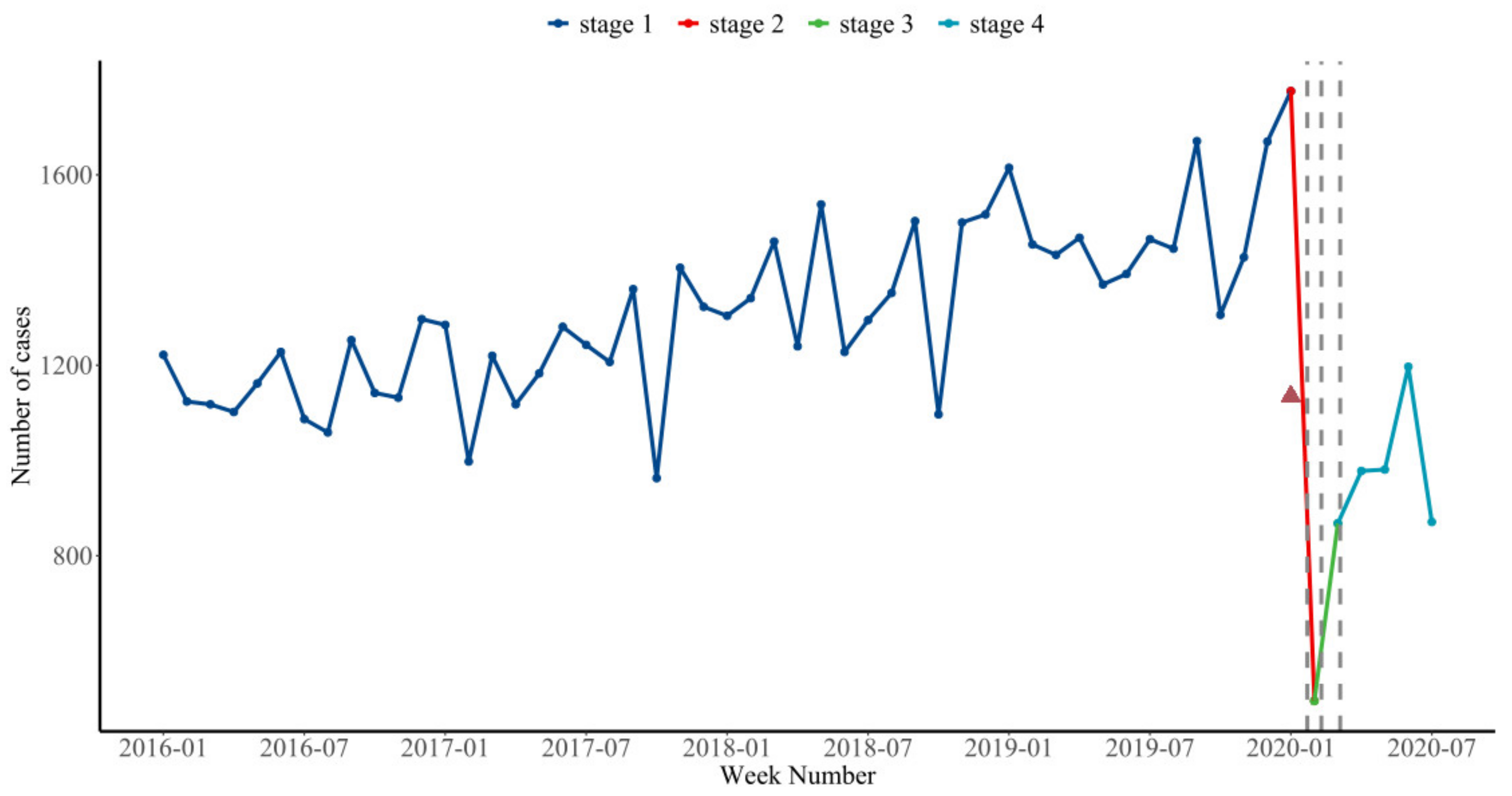
Overall Utilization of Psychiatric Inpatient Care during Different Stages of the Pandemic
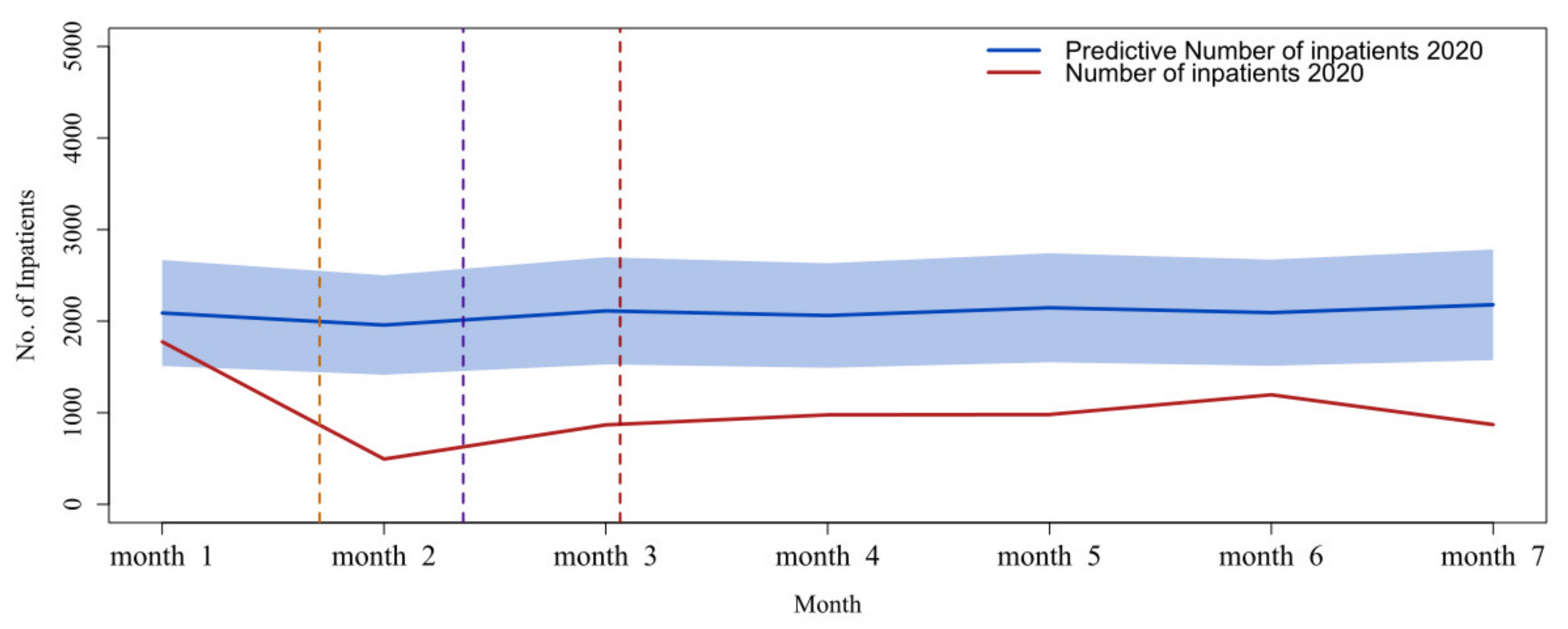
3.4. Main Results
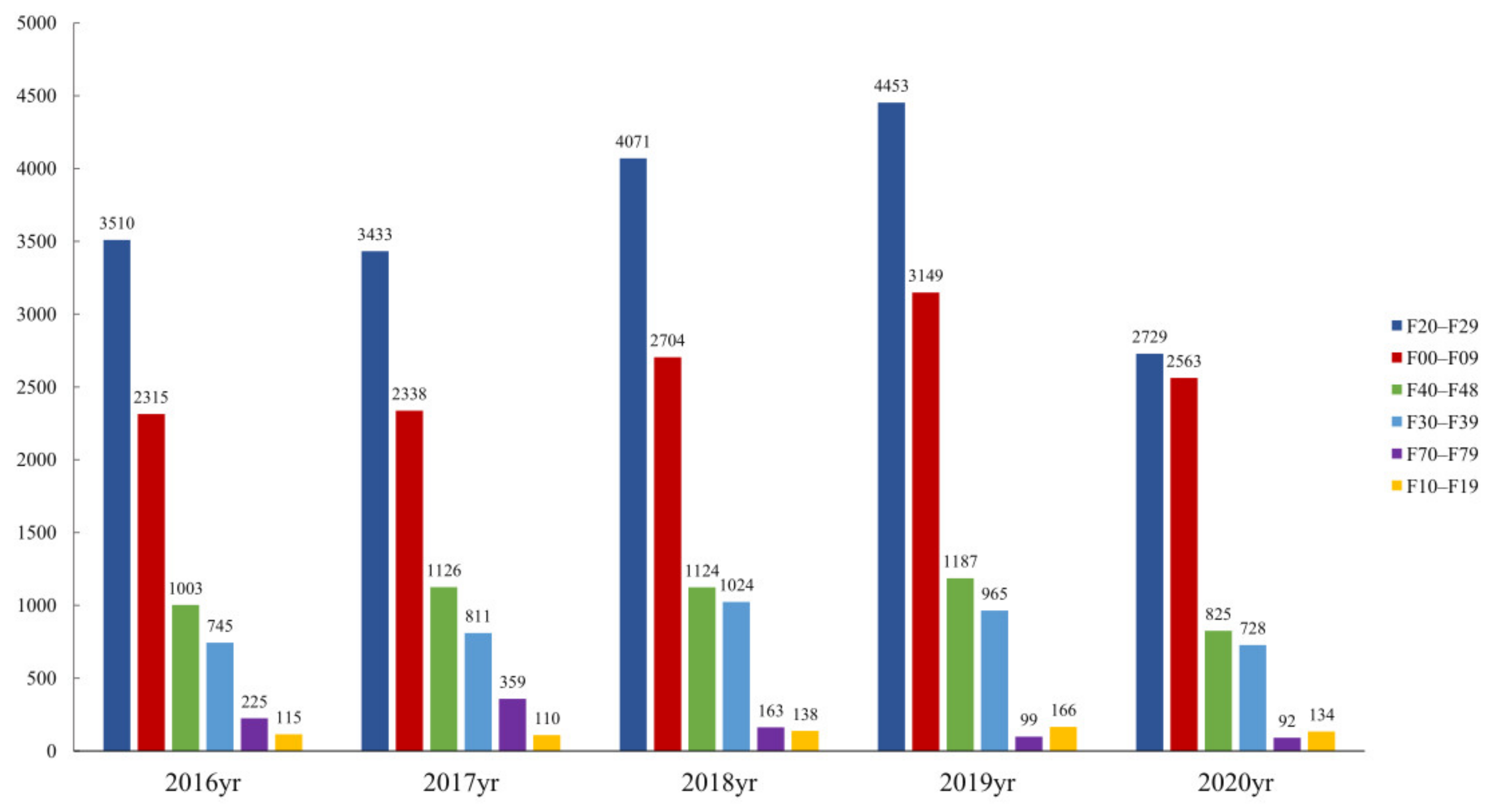
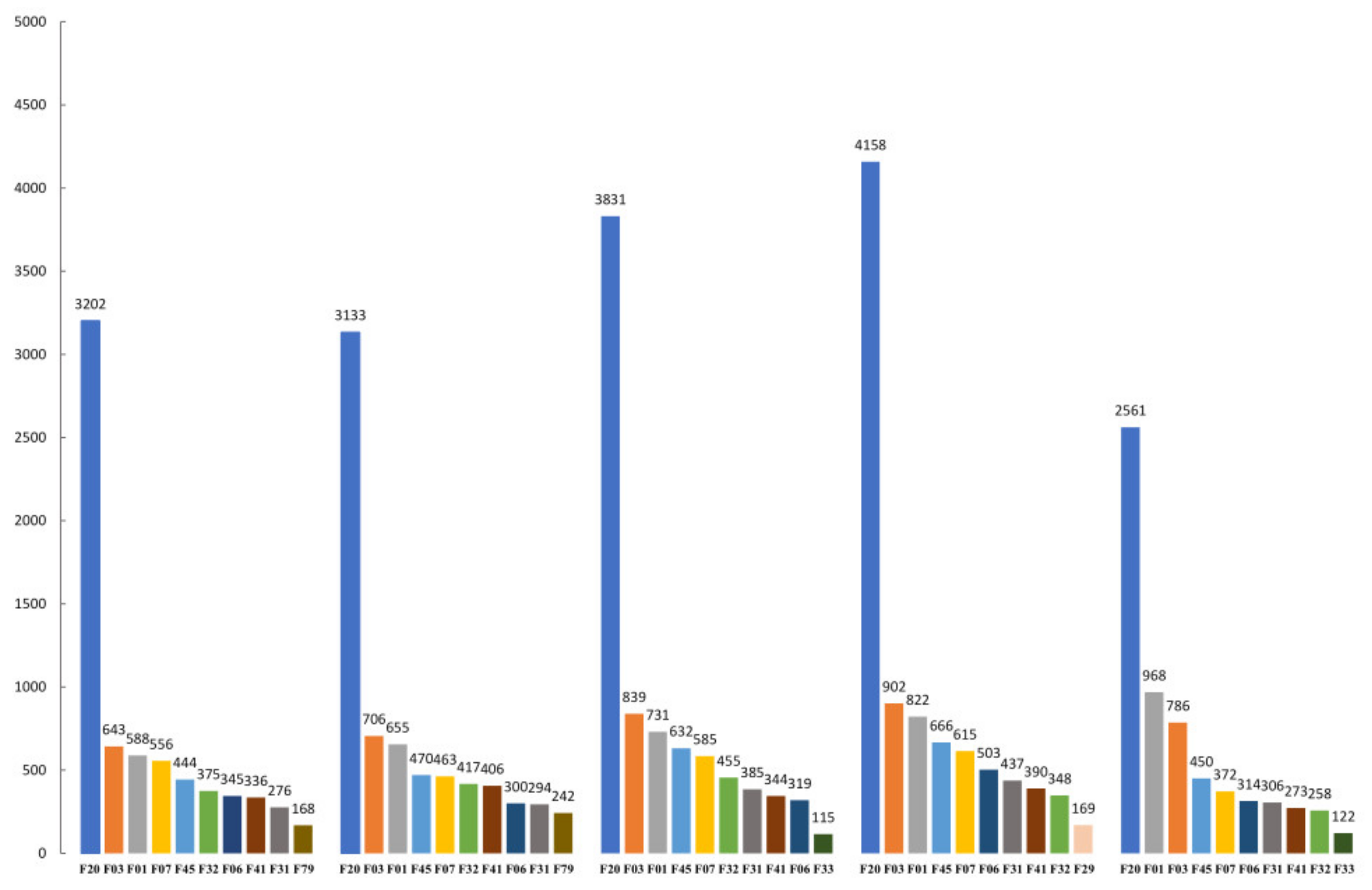
Overall Utilization of Psychiatric Inpatient Care during Different Years
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | One-way analysis of variance |
| COVID-19 | Coronavirus disease 2019 |
| ICD-10 | International Classification of Diseases-10th revision |
| SHIB | Shanghai Medical Insurance Bureau |
| VAD | Vascular dementia |
| WHO | World Health Organization |
References
- Li, W.; Yang, Y.; Liu, Z.-H.; Zhao, Y.-J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.-T. Progression of Mental Health Services during the COVID-19 Outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Health Commission of China, Press Conference: The Central Steering Group Guides and Organizes the Progress of Hubei Epidemic Prevention and Control and Medical Treatment. Available online: http://www.nhc.gov.cn/xcs/s3574/202002/2fb820181d8a41969bca041793c11bcb.shtml (accessed on 8 February 2020).
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; Di Bernardo, A.; Capelli, F.; Pacitti, F. Mental health outcomes of the CoViD-19 pandemic. Riv. Psichiatr. 2020, 55, 137–144. [Google Scholar] [PubMed]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Tanoue, Y.; Nomura, S.; Yoneoka, D.; Kawashima, T.; Eguchi, A.; Shi, S.; Miyata, H. Mental health of family, friends, and co-workers of COVID-19 patients in Japan. Psychiatry Res. 2020, 291, 113067. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- The National Health Commission of Shanghai. Notice on the City’s Health System to Do a Good Job in the Prevention and Control of Pneumonia Caused by COVID-19 Infection. Available online: http://wsjkw.sh.gov.cn/wsyj2/20200217/a84421decf7f4369bf63c39bb97f059a.html (accessed on 10 February 2020).
- Xiang, Y.T.; Zhao, Y.J.; Liu, Z.H.; Li, X.H.; Zhao, N.; Cheung, T.; Ng, C.H. The COVID-19 outbreak and psychiatric hospitals in China: Managing challenges through mental health service reform. Int. J. Biol. Sci. 2020, 16, 1741–1744. [Google Scholar] [CrossRef] [Green Version]
- Pignon, B.; Gourevitch, R.; Tebeka, S.; Dubertret, C.; Cardot, H.; Dauriac-Le Masson, V.; Pham-Scottez, A. Dramatic reduction of psychiatric emergency consultations during lockdown linked to COVID-19 in Paris and suburbs. Psychiatry Clin. Neurosci. 2020, 74, 557–559. [Google Scholar] [CrossRef]
- Chen, S.; Jones, P.B.; Underwood, B.R.; Moore, A.; Bullmore, E.T.; Banerjee, S.; Cardinal, R.N. The early impact of COVID-19 on mental health and community physical health services and their patients’ mortality in Cambridgeshire and Peterborough, UK. J. Psychiatr. Res. 2020, 131, 244–254. [Google Scholar] [CrossRef]
- Abbas, M.J.; Kronenberg, G.; McBride, M.; Chari, D.; Alam, F.; Mukaetova-Ladinska, E.; Al-Uzri, M.; Brugha, T. The Early Impact of the COVID-19 Pandemic on Acute Care Mental Health Services. Psychiatr. Serv. 2021, 72, 242–246. [Google Scholar] [CrossRef]
- Zielasek, J.; Vrinssen, J.; Gouzoulis-Mayfrank, E. Utilization of Inpatient Mental Health Care in the Rhineland during the COVID-19 Pandemic. Front. Public Health 2021, 9, 593307. [Google Scholar] [CrossRef]
- Johnson, S.; Dalton-Locke, C.; Vera San Juan, N.; Foye, U.; Oram, S.; Papamichail, A.; Landau, S.; Rowan Olive, R.; Jeynes, T.; Shah, P.; et al. COVID-19 Mental Health Policy Research Unit Group. Impact on mental health care and on mental health service users of the COVID-19 pandemic: A mixed methods survey of UK mental health care staff. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 25–37. [Google Scholar] [CrossRef]
- Han, R.H.; Schmidt, M.N.; Waits, W.M.; Bell, A.K.C.; Miller, T.L. Planning for Mental Health Needs During COVID-19. Curr. Psychiatry Rep. 2020, 22, 66. [Google Scholar] [CrossRef]
- Zhou, S.-J.; Zhang, L.-G.; Wang, L.-L.; Guo, Z.-C.; Wang, J.-Q.; Chen, J.-C.; Liu, M.; Chen, X.; Chen, J.-X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Seifert, J.; Meissner, C.; Birkenstock, A.; Bleich, S.; Toto, S.; Ihlefeld, C.; Zindler, T. Peripandemic psychiatric emergencies: Impact of the COVID-19 pandemic on patients according to diagnostic subgroup. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 259–270. [Google Scholar] [CrossRef]
- Gómez-Ramiro, M.; Fico, G.; Anmella, G.; Vázquez, M.; Sagué-Vilavella, M.; Hidalgo-Mazzei, D.; Pacchiarotti, I.; Garriga, M.; Murru, A.; Parellada, E.; et al. Changing trends in psychiatric emergency service admissions during the COVID-19 outbreak: Report from a worldwide epicentre. J. Affect. Disord. 2020, 282, 26–32. [Google Scholar] [CrossRef]
- Ness, E.; Salvador, E.M.; Gardsjord, E.S. Patient visits to a psychiatric casualty clinic during the initial phase of the COVID-19 pandemic. Tidsskr. Nor. Laegeforen. 2020, 13, 140. [Google Scholar]
- Aoki, T.; Fujinuma, Y.; Matsushima, M. Usual source of primary care and preventive care measures in the COVID-19 pandemic: A nationwide cross-sectional study in Japan. BMJ Open 2022, 12, e057418. [Google Scholar] [CrossRef]
- Dragovic, M.; Pascu, V.; Hall, T.; Ingram, J.; Waters, F. Emergency department mental health presentations before and during the COVID-19 outbreak in Western Australia. Australas. Psychiatry 2020, 28, 627–631. [Google Scholar] [CrossRef]
- Holland, K.M.; Jones, C.; Vivolo-Kantor, A.M.; Idaikkadar, N.; Zwald, M.; Hoots, B.; Yard, E.; D’Inverno, A.; Swedo, E.; Chen, M.S.; et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes before and during the COVID-19 Pandemic. JAMA Psychiatry 2021, 78, 372. [Google Scholar] [CrossRef]
- Ryu, S.; Nam, H.J.; Baek, S.-H.; Jhon, M.; Kim, J.-M.; Kim, S.-W. Decline in Hospital Visits by Patients with Schizophrenia Early in the COVID-19 Outbreak in Korea. Clin. Psychopharmacol. Neurosci. 2022, 20, 185–189. [Google Scholar] [CrossRef]
- Kolar, D. Psychiatric emergency services and non-acute psychiatric services utilization during COVID-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 271, 391–392. [Google Scholar] [CrossRef]
- World Health Organization. Policy Brief: COVID-19 and the Need for Action on Mental Health; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zhang, Y.-N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.-H.; Tang, S.-L.; Fu, C.-W. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Glob. Health 2020, 5, e003421. [Google Scholar] [CrossRef]
- Cui, Y.; Li, Y.; Zheng, Y.; Chinese Society of Child & Adolescent Psychiatry. Mental health services for children in China during the COVID-19 pandemic: Results of an expert-based national survey among child and adolescent psychiatric hospitals. Eur. Child Adolesc. Psychiatry 2020, 29, 743–748. [Google Scholar] [CrossRef]
- Gonçalves-Pinho, M.; Mota, P.; Ribeiro, J.; Macedo, S.; Freitas, A. The Impact of COVID-19 Pandemic on Psychiatric Emergency Department Visits–A Descriptive Study. Psychiatr. Q. 2021, 92, 621–631. [Google Scholar] [CrossRef]
- Ryoo, N.; Pyun, J.-M.; Baek, M.J.; Suh, J.; Kang, M.J.; Wang, M.J.; Youn, Y.C.; Yang, D.W.; Kim, S.Y.; Park, Y.H.; et al. Coping with Dementia in the Middle of the COVID-19 Pandemic. J. Korean Med. Sci. 2020, 35, e383. [Google Scholar] [CrossRef]
- Hoyer, C.; Ebert, A.; Szabo, K.; Platten, M.; Meyer-Lindenberg, A.; Kranaster, L. Decreased utilization of mental health emergency service during the COVID-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 377–379. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, L.; Ji, H.; Xi, M.; Fang, Y.; Li, Y. The Risk and Prevention of Novel Coronavirus Pneumonia Infections among Inpatients in Psychiatric Hospitals. Neurosci. Bull. 2020, 36, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Aragona, M.; Barbato, A.; Cavani, A.; Costanzo, G.; Mirisola, C. Negative impacts of COVID-19 lockdown on mental health service access and follow-up adherence for immigrants and individuals in socio-economic difficulties. Public Health 2020, 186, 52–56. [Google Scholar] [CrossRef]
- Castro-de-Araujo, L.F.S.; Machado, D.B. Impact of COVID-19 on mental health in a Low and Middle-Income Country. Cien. Saude Colet. 2020, 25 (Suppl. S1), 2457–2460. [Google Scholar] [CrossRef]
- Rizzi, L.; Rosset, I.; Roriz-Cruz, M. Global Epidemiology of Dementia: Alzheimer’s and Vascular Types. BioMed Res. Int. 2014, 2014, 908915. [Google Scholar] [CrossRef]
- Annachiara, C.; Raffaele, D.; Camillo, M.; Laura, B.; Chiara, C.; Valentina, L.; Elisa, R.; Alessandro, V.; Paolo, P.; Valeria, I.; et al. Behavioral and Psychological Effects of Coronavirus Disease-19 Quarantine in Patients with Dementia. Front. Psychiatry 2020, 9, 578015. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|
| N % | N % | N % | N % | N % | |
| No. Patients | (20.0%) | (20.9%) | (23.5%) | (25.4%) | 7166 (10.3%) |
| Gender | |||||
| Male | 6804 (48.9%) | 7177 (49.2%) | 7966 (48.6%) | 8683 (49.0%) | 3431 (47.9%) |
| Female | 7122 (51.1%) | 7409 (50.8%) | 8409 (51.4%) | 9032 (51.0%) | 3735 (52.1%) |
| Age, years | |||||
| ≤44 | 4353 (31.3%) | 4454 (30.5%) | 5029 (30.7%) | 5527 (31.2%) | 2130 (29.7%) |
| 45–64 | 3350 (24.1%) | 3551 (24.3%) | 4113 (25.1%) | 4313 (24.3%) | 1759 (24.5%) |
| 65–74 | 3557 (25.5%) | 3797 (26.0%) | 4121 (25.2%) | 4274 (24.1%) | 1871 (26.1%) |
| ≥75 | 2666 (19.1%) | 2784 (19.1%) | 3112 (19.0%) | 3601 (20.3%) | 1406 (19.6%) |
| Length of stay (days) M (P25, P75) | 32 (13~81) | 31 (12~76) | 31 (13~71) | 27 (11~60) | 25 (11~59) |
| Diagnosis | |||||
| Organic, including symptomatic, mental disorders (F00–F09) | 3914 (28.1%) | 4192 (28.7%) | 4938 (30.2%) | 5661 (32.0%) | 2563 (35.8%) |
| Mental and behavioral disorders due to psychoactive substance use (F10–F19) | 203 (1.5%) | 230 (1.6%) | 231 (1.4%) | 278 (1.6%) | 134 (1.9%) |
| Schizophrenia, schizotypal and delusional disorders (F20–F29) | 6033 (43.3%) | 5984 (41.0%) | 6979 (42.6%) | 7439 (42.0%) | 2729 (38.1%) |
| Mood disorders (F30–F39) | 1326 (9.5%) | 1426 (9.8%) | 1681 (10.3%) | 1720 (9.7%) | 728 (10.2%) |
| Neurotic, stress-related and somatoform disorders (F40–F48) | 1775 (12.7%) | 2002 (13.7%) | 2036 (12.4%) | 2078 (11.7%) | 825 (11.5%) |
| Behavior syndromes associated with physiological disturbances and physical factors (F50–F59) | 139 (1.0%) | 124 (0.9%) | 132 (0.8%) | 238 (1.3%) | 61 (0.9%) |
| Disorders of adult personality and behavior (F60–F69) | 26 (0.2%) | 25 (0.2%) | 31 (0.2%) | 41 (0.2%) | 10 (0.1%) |
| Mental retardation (F70–F79) | 431 (3.1%) | 503 (3.4%) | 230 (1.4%) | 173 (1.0%) | 92 (1.3%) |
| Disorders of physiological development (F80–F89) | 3 (0.0%) | 3 (0.0%) | 12 (0.1%) | 12 (0.1%) | 1 (0.0%) |
| Behavioral and emotional disorders that usually start in childhood and adolescence (F90–F99) | 76 (0.5%) | 97 (0.7%) | 105 (0.6%) | 75 (0.4%) | 23 (0.3%) |
| Date | January 2020 | February 2020 | March 2020 | April 2020 | May 2020 | June 2020 | July 2020 |
|---|---|---|---|---|---|---|---|
| Inpatients | |||||||
| Observed | 1776 | 495 | 868 | 978 | 981 | 1197 | 871 |
| Predicted | 2090 | 1959 | 2113 | 2062 | 2147 | 2094 | 2180 |
| 95% CI for Predicted | 1511 to 2669 | 1416 to 2502 | 1528 to 2699 | 1491 to 2634 | 1552 to 2742 | 1513 to 2674 | 1575 to 2784 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Chen, X.; Pan, J.; Li, M.; Wang, M.; Wang, W.; Wang, Y. Impact of the COVID-19 Pandemic on Utilization of Inpatient Mental Health Services in Shanghai, China. Healthcare 2022, 10, 1402. https://doi.org/10.3390/healthcare10081402
Li H, Chen X, Pan J, Li M, Wang M, Wang W, Wang Y. Impact of the COVID-19 Pandemic on Utilization of Inpatient Mental Health Services in Shanghai, China. Healthcare. 2022; 10(8):1402. https://doi.org/10.3390/healthcare10081402
Chicago/Turabian StyleLi, Hao, Xiaoli Chen, Jinhua Pan, Mengying Li, Meng Wang, Weibing Wang, and Ying Wang. 2022. "Impact of the COVID-19 Pandemic on Utilization of Inpatient Mental Health Services in Shanghai, China" Healthcare 10, no. 8: 1402. https://doi.org/10.3390/healthcare10081402
APA StyleLi, H., Chen, X., Pan, J., Li, M., Wang, M., Wang, W., & Wang, Y. (2022). Impact of the COVID-19 Pandemic on Utilization of Inpatient Mental Health Services in Shanghai, China. Healthcare, 10(8), 1402. https://doi.org/10.3390/healthcare10081402