
Development and Validation of a Novel Pre-Pregnancy Score Predictive of Preterm Birth in Nulliparous Women Using Data from Italian Healthcare Utilization Databases

 ,
,  , ,
, ,  ,
,  , ,
, ,  on behalf of the CHRP-Sicily Region Working Group
on behalf of the CHRP-Sicily Region Working Group
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Data Sources
2.3. Score Development
2.4. Score Validation
2.5. Statistical Software
3. Results
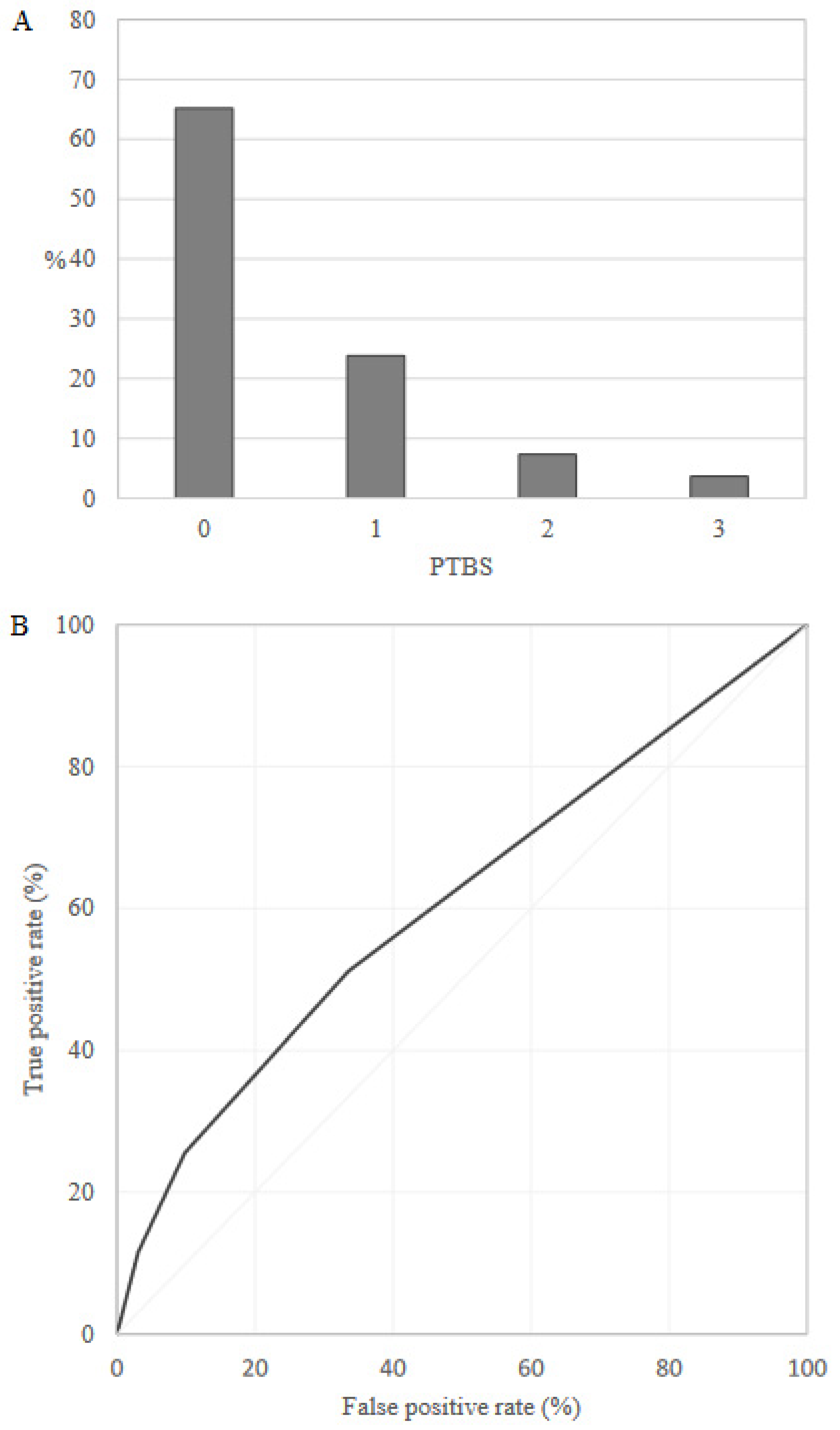
3.1. PTBS Development
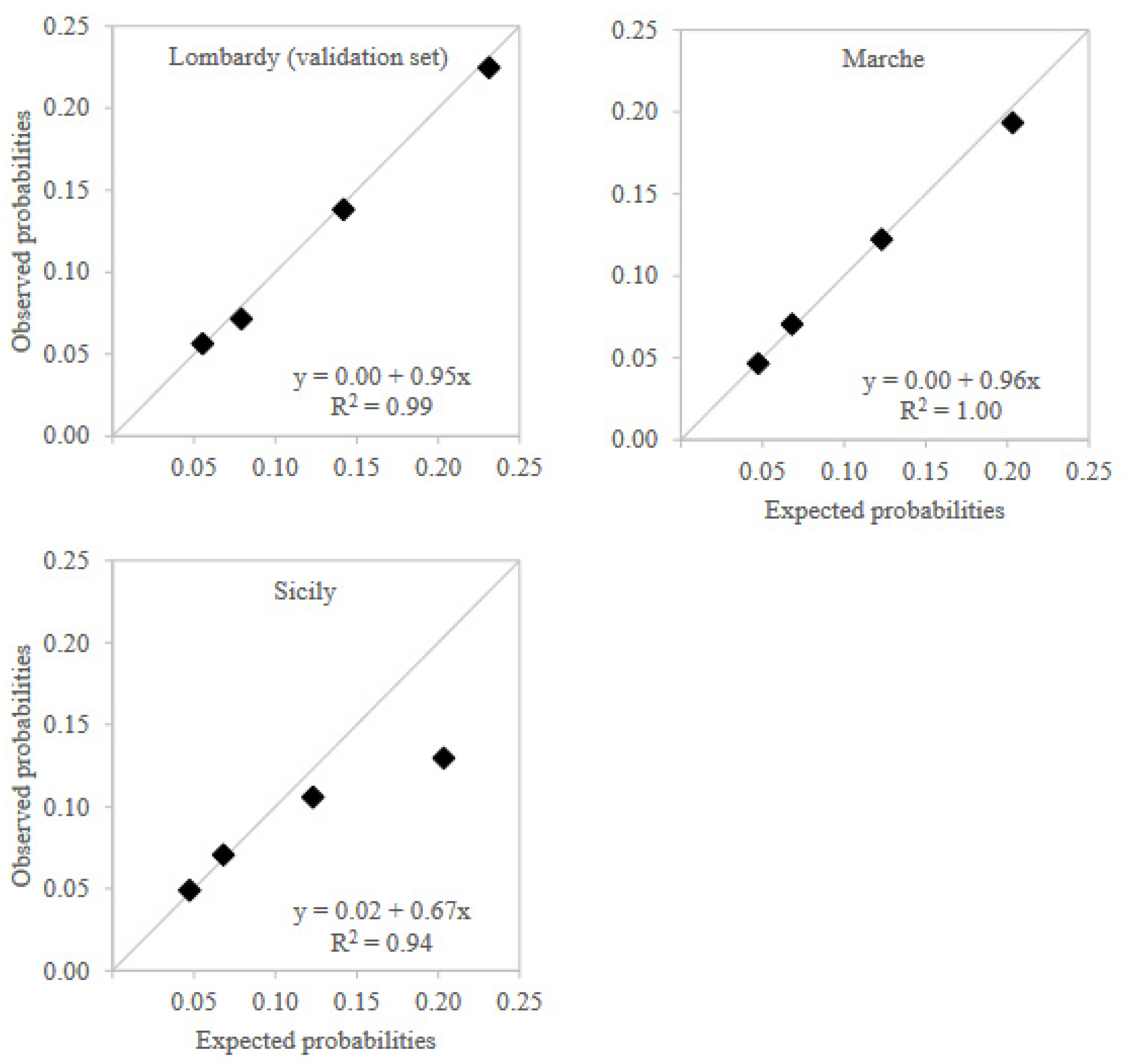
3.2. PTBS Validation



4. Comment
4.1. Principal Findings
4.2. Results in the Context of What Is Known
4.3. Clinical Implications—The Meaning of the Study
4.4. Strengths and Limitations
4.5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawn, J.E.; Gravett, M.G.; Nunes, T.M.; Rubens, C.E.; Stanton, C. GAPPS Review Group. Global report on preterm birth and stillbirth (1 of 7): Definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth 2010, 10 (Suppl. S1), S1. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000-15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Lawn, J.E.; Cousens, S.; Zupan, J.; Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: When? Where? Why? Lancet 2005, 365, 891–900. [Google Scholar] [CrossRef]
- Chehade, H.; Simeoni, U.; Guignard, J.P.; Boubred, F. Preterm Birth: Long Term Cardiovascular and Renal Consequences. Curr. Pediatric Rev. 2018, 14, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Moster, D.; Lie, R.T.; Markestad, T. Long-term medical and social consequences of preterm birth. N. Engl. J. Med. 2008, 359, 262–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Son, M.; Miller, E.S. Predicting preterm birth: Cervical length and fetal fibronectin. Semin. Perinatol. 2017, 41, 445–451. [Google Scholar] [CrossRef]
- Jackson, R.A.; Gibson, K.A.; Wu, Y.W.; Croughan, M.S. Perinatal outcomes in singletons following in vitro fertilization: A meta-analysis. Obstet. Gynecol. 2004, 103, 551–563. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, D.M.; Larson, J.; Jacobsson, B.; Di Renzo, G.C.; Norman, J.E.; Martin, J.N., Jr.; Simpson, J.L. Cross-Country Individual Participant Analysis of 4.1 Million Singleton Births in 5 Countries with Very High Human Development Index Confirms Known Associations but Provides No Biologic Explanation for 2/3 of All Preterm Births. PLoS ONE 2016, 11, e0162506. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Goepfert, A.R.; Ramsey, P.S. Biochemical markers for the prediction of preterm birth. Am. J. Obstet. Gynecol. 2005, 192, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Society. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Refaeilzadeh, P.; Tang, L.; Liu, H. Cross-validation. Encycl. Database Syst. 2009, 5, 532–538. [Google Scholar]
- Steyerberg, E.W.; Harrell, F.E., Jr. Prediction models need appropriate internal, internal-external, and external validation. J. Clin. Epidemiol. 2016, 69, 245–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, K.J.; Vergouwe, Y.; Kalkman, C.J.; Grobbee, D.E.; Moons, K.G. A simple method to adjust clinical prediction models to local circumstances. Can. J. Anaesth. J. Can. Danesthesie 2009, 56, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabi Belaghi, R.; Beyene, J.; McDonald, S.D. Prediction of preterm birth in nulliparous women using logistic regression and machine learning. PLoS ONE 2021, 16, e0252025. [Google Scholar] [CrossRef] [PubMed]
- Meertens, L.; van Montfort, P.; Scheepers, H.; Van Kuijk, S.M.; Aardenburg, R.; Langenveld, J.; Van Dooren, I.M.; Zwaan, I.M.; Spaanderman, M.E.; Smits, L.J. Prediction models for the risk of spontaneous preterm birth based on maternal characteristics: A systematic review and independent external validation. Acta Obstet. Gynecol. Scand. 2018, 97, 907–920. [Google Scholar] [CrossRef] [PubMed]
- Köck, K.; Köck, F.; Klein, K.; Bancher-Todesca, D.; Helmer, H. Diabetes mellitus and the risk of preterm birth with regard to the risk of spontaneous preterm birth. J. Matern. Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2010, 23, 1004–1008. [Google Scholar] [CrossRef] [PubMed]
- Wahabi, H.A.; Esmaeil, S.A.; Fayed, A.; Al-Shaikh, G.; Alzeidan, R.A. Pre-existing diabetes mellitus and adverse pregnancy outcomes. BMC Res. Notes 2012, 5, 496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ram, C.V. Antihypertensive drugs: An overview. Am. J. Cardiovasc. Drugs Drugs Devices Other Interv. 2002, 2, 77–89. [Google Scholar] [CrossRef]
- Bramham, K.; Parnell, B.; Nelson-Piercy, C.; Seed, P.T.; Poston, L.; Chappell, L.C. Chronic hypertension and pregnancy outcomes: Systematic review and meta-analysis. BMJ 2014, 348, g2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Venkatesan, R.L.; Gupta, A.; Sanghavi, M.K.; Welge, J.; Johansen, R.; Kean, E.; Kaur, T.; Gupta, A.; Grant, T.; et al. Pregnancy outcomes in women with kidney transplant: Metaanalysis and systematic review. BMC Nephrol. 2019, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Marson, E.J.; Kamarajah, S.K.; Dyson, J.K.; White, S.A. Pregnancy outcomes in women with liver transplants: Systematic review and meta-analysis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2020, 22, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.; Zaffar, N.; Dong, S.; Ross, H.; D’Souza, R. Pregnancy outcomes in women with cardiothoracic transplants: A Systematic review and meta-analysis. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2020, 39, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Lai, K.; Yang, Z.; Zeng, K. Systemic lupus erythematosus and risk of preterm birth: A systematic review and meta-analysis of observational studies. Lupus 2017, 26, 563–571. [Google Scholar] [CrossRef]
- Zhang, J.J.; Ma, X.X.; Hao, L.; Liu, L.J.; Lv, J.C.; Zhang, H. A Systematic Review and Meta-Analysis of Outcomes of Pregnancy in CKD and CKD Outcomes in Pregnancy. Clin. J. Am. Soc. Nephrol. CJASN 2015, 10, 1964–1978. [Google Scholar] [CrossRef]
- Jensen, E.T.; Daniels, J.L.; Stürmer, T.; Robinson, W.; Williams, C.J.; Vejrup, K.; Magnus, P.; Longnecker, M.P. Hormonal contraceptive use before and after conception in relation to preterm birth and small for gestational age: An observational cohort study. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 1349–1361. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (%) | Weight | ||
|---|---|---|---|---|
| Term Birth | Preterm Birth | Total | ||
| n = 117,480 | n = 9358 | n = 126,839 | ||
| Drugs | ||||
| Pancreatic hormones | 63 (0.05) | 33 (0.35) | 96 (0.08) | 10 |
| Agents acting on the renin-angiotensin system | 803 (0.68) | 173 (1.85) | 976 (0.77) | 5 |
| Sex hormones and modulators of the genital system | 22,664 (19.29) | 3216 (34.36) | 25,880 (20.40) | 4 |
| Endocrine therapy | 567 (0.48) | 156 (1.67) | 723 (0.57) | 3 |
| Drugs used in diabetes | 459 (0.39) | 112 (1.20) | 571 (0.45) | 3 |
| Immunosuppressants | 266 (0.23) | 53 (0.57) | 319 (0.25) | 2 |
| Corticosteroids for systemic use | 13,200 (11.24) | 1341 (14.33) | 14,541 (11.46) | 1 |
| Beta blocking agents | 1034 (0.88) | 163 (1.74) | 1197 (0.94) | 1 |
| Calcium channel blockers | 498 (0.42) | 98 (1.05) | 596 (0.47) | 1 |
| Hospital diagnosis | ||||
| Heart failure | 3 (0.00) | 5 (0.05) | 8 (0.01) | 8 |
| Chronic renal failure | 2 (0.00) | 4 (0.04) | 6 (0.00) | 4 |
| Diffuse diseases of connective tissue | 31 (0.03) | 13 (0.14) | 44 (0.03) | 3 |
| Inpatient procedures | ||||
| Other operations on rectum and perirectal tissue | 7 (0.01) | 7 (0.07) | 14 (0.01) | 12 |
| Diagnostic procedures on liver | 23 (0.02) | 12 (0.13) | 35 (0.03) | 4 |
| Lysis of peritoneal adhesions | 586 (0.50) | 132 (1.41) | 718 (0.57) | 4 |
| Exemptions | ||||
| Transplant recipients | 13 (0.01) | 12 (0.13) | 25 (0.02) | 8 |
| Diabetes mellitus | 303 (0.26) | 83 (0.89) | 386 (0.30) | 4 |
| Systemic lupus erythematosus | 97 (0.08) | 27 (0.29) | 124 (0.10) | 4 |
| Affections of the circulatory system | 343 (0.29) | 56 (0.60) | 399 (0.31) | 1 |
| Chronic (active) hepatitis | 270 (0.23) | 51 (0.54) | 321 (0.25) | 1 |
| Outpatient services | ||||
| Psychiatry | 4324 (3.68) | 549 (5.87) | 4873 (3.84) | 1 |
| General consultation | 474 (0.40) | 86 (0.92) | 560 (0.44) | 1 |
| Socio-demographic conditions | ||||
| Age at conception ≥36 years | 22,095 (18.81) | 2723 (29.09) | 24,818 (19.57) | 3 |
| Born abroad | 14,014 (11.93) | 1300 (13.89) | 15,314 (12.07) | 1 |
| Low education | 20,597 (17.53) | 1815 (19.39) | 22,412 (17.67) | 1 |
| Use of assisted medical conception techniques | 6005 (5.11) | 1587 (16.96) | 7592 (5.99) | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merlo, I.; Cantarutti, A.; Allotta, A.; Tavormina, E.E.; Iommi, M.; Pompili, M.; Rea, F.; Agodi, A.; Locatelli, A.; Zanini, R.; et al. Development and Validation of a Novel Pre-Pregnancy Score Predictive of Preterm Birth in Nulliparous Women Using Data from Italian Healthcare Utilization Databases. Healthcare 2022, 10, 1443. https://doi.org/10.3390/healthcare10081443
Merlo I, Cantarutti A, Allotta A, Tavormina EE, Iommi M, Pompili M, Rea F, Agodi A, Locatelli A, Zanini R, et al. Development and Validation of a Novel Pre-Pregnancy Score Predictive of Preterm Birth in Nulliparous Women Using Data from Italian Healthcare Utilization Databases. Healthcare. 2022; 10(8):1443. https://doi.org/10.3390/healthcare10081443
Chicago/Turabian StyleMerlo, Ivan, Anna Cantarutti, Alessandra Allotta, Elisa Eleonora Tavormina, Marica Iommi, Marco Pompili, Federico Rea, Antonella Agodi, Anna Locatelli, Rinaldo Zanini, and et al. 2022. "Development and Validation of a Novel Pre-Pregnancy Score Predictive of Preterm Birth in Nulliparous Women Using Data from Italian Healthcare Utilization Databases" Healthcare 10, no. 8: 1443. https://doi.org/10.3390/healthcare10081443
APA StyleMerlo, I., Cantarutti, A., Allotta, A., Tavormina, E. E., Iommi, M., Pompili, M., Rea, F., Agodi, A., Locatelli, A., Zanini, R., Carle, F., Addario, S. P., Scondotto, S., & Corrao, G., on behalf of the CHRP-Sicily Region Working Group. (2022). Development and Validation of a Novel Pre-Pregnancy Score Predictive of Preterm Birth in Nulliparous Women Using Data from Italian Healthcare Utilization Databases. Healthcare, 10(8), 1443. https://doi.org/10.3390/healthcare10081443