
The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes

 ,
,  ,
,  , , and
, , and  on behalf of the REPOSI Investigators
on behalf of the REPOSI Investigators
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Study Population
2.2. Socio-Demographic and Clinical Characteristics
2.3. Statistical Analysis
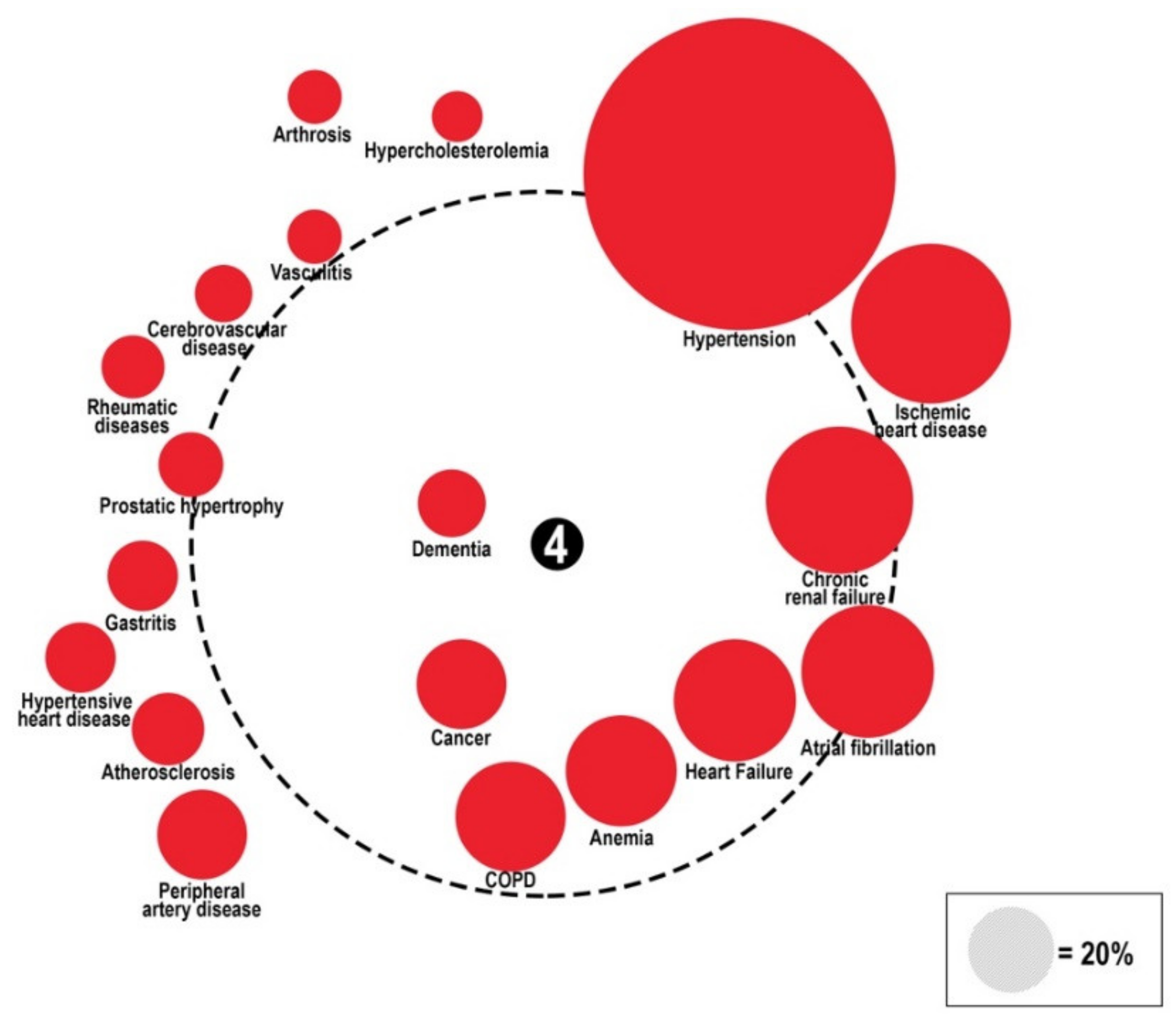
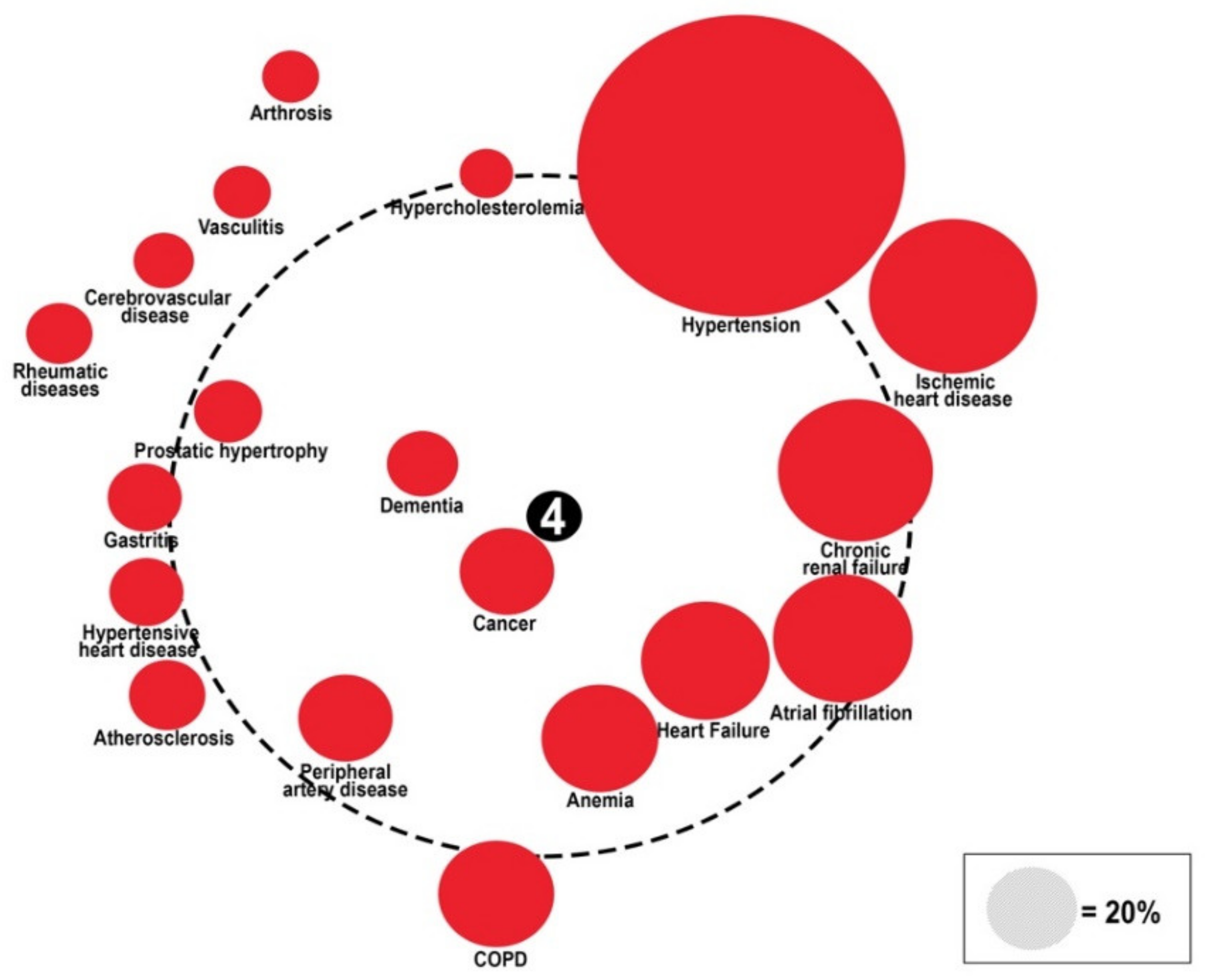
The “Diabetes Comorbidome”
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
- -
- Domenico Prisco, Elena Silvestri, Giacomo Emmi, Alessandra Bettiol, Irene Mattioli (Azienda Ospedaliero Universitaria Careggi Firenze, SOD Medicina Interna Interdisciplinare);
- -
- Gianni Biolo, Michela Zanetti, Giacomo Bartelloni, Michele Zaccari, Massimiliano Chiuch (Azienda Sanitaria Universitaria Integrata di Trieste, Clinica Medica Generale e Terapia Medica);
- -
- Massimo Vanoli, Giulia Grignani, Edoardo Alessandro Pulixi (Azienda Ospedaliera della Provincia di Lecco, Ospedale di Merate, Lecco, Medicina Interna);
- -
- Matteo Pirro, Graziana Lupattelli, Vanessa Bianconi, Riccardo Alcidi, Alessia Giotta, Massimo R. Mannarino (Azienda Ospedaliera Santa Maria della Misericordia, Perugia, Medicina Interna, Angiologia Malattie da Arteriosclerosi);
- -
- Domenico Girelli, Fabiana Busti, Giacomo Marchi (Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Medicina Generale e Malattie Aterotrombotiche e Degenerative);
- -
- Mario Barbagallo, Ligia Dominguez, Vincenza Beneduce, Federica Cacioppo (Azienda Ospedaliera Universitaria Policlinico Giaccone Policlinico di Palermo, Palermo, Unità Operativa di Geriatria e Lungodegenza);
- -
- Salvatore Corrao, Giuseppe Natoli, Salvatore Mularo, Massimo Raspanti, Christiano Argano (A.R.N.A.S. Civico, Di Cristina, Benfratelli, Palermo, UOC Medicina Interna ad Indirizzo Geriatrico-Riabilitativo);
- -
- Marco Zoli, Maria Laura Matacena, Giuseppe Orio, Eleonora Magnolfi, Giovanni Serafini, Angelo Simili, Mattia Brunori, Ilaria Lazzari, Angelo Simili (Azienda Ospedaliera Universitaria Policlinico S. Orsola-Malpighi, Bologna, Unità Operativa di Medicina Interna Zoli);
- -
- Maria Domenica Cappellini, Giovanna Fabio, Margherita Migone De Amicis, Giacomo De Luca, Natalia Scaramellini, Valeria Di Stefano, Simona Leoni, Sonia Seghezzi, Alessandra Danuto Di Mauro, Diletta Maira, Marta Mancarella (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Unità Operativa Medicina Interna IA);
- -
- Tiziano Lucchi, Paolo Dionigi Rossi, Marta Clerici, Simona Leoni, Alessandra Danuta Di Mauro, Giulia Bonini, Federica Conti, Silvia Prolo, Maddalena Fabrizi, Miriana Martelengo, Giulia Vigani (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Geriatria);
- -
- Antonio Di Sabatino, Emanuela Miceli, Marco Vincenzo Lenti, Martina Pisati, Costanza Caccia Dominioni, Lavinia Pitotti, Donatella Padula (IRCCS Policlinico San Matteo di Pavia, Pavia, Clinica Medica I, Reparto 11);
- -
- Roberto Pontremoli, Valentina Beccati, Giulia Nobili, Giovanna Leoncini, Jacopo Alberto, Federico Cattaneo (IRCCS Azienda Ospedaliera Universitaria San Martino-IST di Genova, Genova, Clinica di Medicina Interna 2);
- -
- Luigi Anastasio, Lucia Sofia, Maria Carbone (Ospedale Civile Jazzolino di Vibo Valentia, Vibo Valentia, Medicina Generale);
- -
- Francesco Cipollone, Maria Teresa Guagnano, Ilaria Rossi, Emanuele Valeriani, Damiani D’Ardes, Lucia Esposito, Simona Sestili, Ermanno Angelucci (Ospedale Clinicizzato SS. Annunziata, Chieti, Clinica Medica);
- -
- Gerardo Mancuso, Daniela Calipari, Mosè Bartone (Ospedale Giovanni Paolo II Lamezia Terme, Catanzaro, Unità Operativa Complessa Medicina Interna);
- -
- Giuseppe Delitala, Maria Berria, Alessandro Delitala (Azienda Ospedaliera—Universitaria di Sassari, Clinica Medica);
- -
- Maurizio Muscaritoli, Alessio Molfino, Enrico Petrillo, Antonella Giorgi, Christian Gracin, Giovanni Imbimbo (Policlinico Umberto I, Sapienza Università di Roma, Medicina Interna e Nutrizione Clinica Policlinico Umberto I);
- -
- Giuseppe Zuccalà, Gabriella D’Aurizio (Policlinico Universitario A. Gemelli, Roma, Roma, Unità Operativa Complessa Medicina d’Urgenza e Pronto Soccorso);
- -
- Giuseppe Romanelli, Alessandra Marengoni, Andrea Volpini, Daniela Lucente, Francesca Manzoni, Annalisa Pirozzi, Alberto Zucchelli (Unità Operativa Complessa di Medicina I a indirizzo geriatrico, Spedali Civili, Montichiari, Brescia);
- -
- Antonio Picardi, Umberto Vespasiani Gentilucci, Paolo Gallo, Chiara Dell’Unto (Università Campus Bio-Medico, Roma, Medicina Clinica-Epatologia);
- -
- Giuseppe Bellelli, Maurizio Corsi, Cesare Antonucci, Chiara Sidoli, Giulia Principato, Alessandra Bonfanti, Hajnalka Szabo, Paolo Mazzola, Andrea Piazzoli, Maurizio Corsi (Università degli studi di Milano-Bicocca Ospedale S. Gerardo, Monza, Unità Operativa di Geriatria);
- -
- Franco Arturi, Elena Succurro, Bruno Tassone, Federica Giofrè (Università degli Studi Magna Grecia, Policlinico Mater Domini, Catanzaro, Unità Operativa Complessa di Medicina Interna);
- -
- Maria Grazia Serra, Maria Antonietta Bleve (Azienda Ospedaliera "Cardinale Panico" Tricase, Lecce, Unità Operativa Complessa Medicina);
- -
- Antonio Brucato, Teresa De Falco, Enrica Negro, Martino Brenna, Lucia Trotta, Giovanni Lorenzo Squintani (ASST Fatebenefratelli—Sacco, Milano, Medicina Interna);
- -
- Maria Luisa Randi, Fabrizio Fabris, Irene Bertozzi, Giulia Bogoni, Maria Victoria Rabuini, Tancredi Prandini, Francesco Ratti, Chiara Zurlo, Lorenzo Cerruti, Elisabetta Cosi (Azienda Ospedaliera Università di Padova, Padova, Clinica Medica I);
- -
- Roberto Manfredini, Fabio Fabbian, Benedetta Boari, Alfredo De Giorgi, Ruana Tiseo (Azienda Ospedaliera—Universitaria Sant’Anna, Ferrara, Unità Operativa Clinica Medica);
- -
- Giuseppe Paolisso, Maria Rosaria Rizzo, Claudia Catalano, Irene Di Meo (Azienda Ospedaliera Universitaria della Seconda Università degli Studi di Napoli, Napoli, VI Divisione di Medicina Interna e Malattie Nutrizionali dell’Invecchiamento);
- -
- Claudio Borghi, Enrico Strocchi, Eugenia Ianniello, Mario Soldati, Silvia Schiavone, Alessio Bragagni, Francesca Giulia Leoni, Valeria De Sando, Sara Scarduelli, Michela Cammarosano, Ilenia Pareo (Azienda Ospedaliera Universitaria Policlinico S. Orsola-Malpighi, Bologna, Unità Operativa di Medicina Interna Borghi);
- -
- Carlo Sabbà, Francesco Saverio Vella, Patrizia Suppressa, Giovanni Michele De Vincenzo, Alessio Comitangelo, Emanuele Amoruso, Carlo Custodero, Giuseppe Re, Andrea Schilardi, Francesca Loparco (Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Medicina Interna Universitaria C. Frugoni);
- -
- Luigi Fenoglio, Andrea Falcetta, Alessia Valentina Giraudo, Salvatore D’Aniano (Azienda Sanitaria Ospedaliera Santa Croce e Carle di Cuneo, Cuneo, S. C. Medicina Interna);
- -
- Anna L. Fracanzani, Silvia Tiraboschi, Annalisa Cespiati, Giovanna Oberti, Giordano Sigon, Felice Cinque (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, UOC Medicina Generale ad Indirizzo Metabolico);
- -
- Flora Peyvandi, Raffaella Rossio, Giulia Colombo, Pasquale Agosti, Erica Pagliaro (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna 2, Ematologia non tumorale e Coagulopatie);
- -
- Canetta Ciro, Valter Monzani, Valeria Savojardo, Giuliana Ceriani, Christian Folli (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna Alta Intensità di Cure);
- -
- Francesco Salerno, Giada Pallini (IRCCS Policlinico San Donato e Università di Milano, San Donato Milanese, Medicina Interna);
- -
- Fabrizio Montecucco, Luciano Ottonello, Lara Caserza, Giulia Vischi, Salam Kassem, Luca Liberale (IRCCS Ospedale Policlinico San Martino e Università di Genova, Genova, Clinica Medica 1, Medicina Interna e Specialità Mediche);
- -
- Nicola Lucio Liberato, Tiziana Tognin (ASST di Pavia, UOSD Medicina Interna, Ospedale di Casorate Primo, Pavia);
- -
- Francesco Purrello, Antonino Di Pino, Salvatore Piro (Ospedale Garibaldi Nesima, Catania, Unità Operativa Complessa di Medicina Interna);
- -
- Renzo Rozzini, Lina Falanga, Maria Stella Pisciotta, Francesco Baffa Bellucci, Stefano Buffelli, Camillo Ferrandina, Francesca Mazzeo, Elena Spazzini, Giulia Cono, Giulia Cesaroni (Ospedale Poliambulanza, Brescia, Medicina Interna e Geriatria);
- -
- Giuseppe Montrucchio, Paolo Peasso, Edoardo Favale, Cesare Poletto, Carl Margaria, Maura Sanino (Dipartimento di Scienze Mediche, Università di Torino, Città della Scienza e della Salute, Torino, Medicina Interna 2 Unità Indirizzo d’Urgenza);
- -
- Francesco Violi, Ludovica Perri (Policlinico Umberto I, Roma, Prima Clinica Medica);
- -
- Luigina Guasti, Francesca Rotunno, Luana Castiglioni, Andrea Maresca, Alessandro Squizzato, Leonardo Campiotti, Alessandra Grossi, Roberto Davide Diprizio, Francesco Dentali (Università degli Studi dell’Insubria, Ospedale di Circolo e Fondazione Macchi, Varese, Medicina e Geriatria);
- -
- Marco Bertolotti, Chiara Mussi, Giulia Lancellotti, Maria Vittoria Libbra, Matteo Galassi, Yasmine Grassi, Alessio Greco, Elena Bigi, Elisa Pellegrini, Laura Orlandi, Giulia Dondi, Lucia Carulli (Università di Modena e Reggio Emilia, Azienda Ospedaliero-Universitaria di Modena; Ospedale Civile di Baggiovara, Unità Operativa di Geriatria);
- -
- Angela Sciacqua, Maria Perticone, Rosa Battaglia, Raffaele Maio, Aleandra Scozzafava, Valentino Condoleo, Tania Falbo, Lidia Colangelo; Marco Filice, Elvira Clausi (Università Magna Grecia Policlinico Mater Domini, Catanzaro, Unità Operativa Malattie Cardiovascolari Geriatriche);
- -
- Vincenzo Stanghellini, Eugenio Ruggeri, Sara del Vecchio, Ilaria Benzoni (Dipartimento di Scienze Mediche e Chirurgiche, Unità Operativa di Medicina Interna, Università degli Studi di Bologna/Azienda Ospedaliero—Universitaria S.Orsola-Malpighi, Bologna);
- -
- Andrea Salvi, Roberto Leonardi, Giampaolo Damiani (Spedali Civili di Brescia, U.O. 3a Medicina Generale);
- -
- Gianluca Moroncini, William Capeci, Massimo Mattioli, Giuseppe Pio Martino, Lorenzo Biondi, Pietro Pettinari, Monica Ormas, Emanuele Filippini, Devis Benfaremo, Roberto Romiti (Clinica Medica, Azienda Ospedaliera Universitaria—Ospedali Riuniti di Ancona);
- -
- Riccardo Ghio, Anna Dal Col (Azienda Ospedaliera Università San Martino, Genova, Medicina III);
- -
- Salvatore Minisola, Luciano Colangelo, Mirella Cilli, Giancarlo Labbadia (Policlinico Umberto I, Roma, SMSC03—Medicina Interna F e Malattie Metaboliche dell’osso);
- -
- Antonella Afeltra, Benedetta Marigliano, Maria Elena Pipita (Policlinico Campus Biomedico Roma, Roma, Medicina Clinica);
- -
- Pietro Castellino, Luca Zanoli, Alfio Gennaro, Agostino Gaudio, Samuele Pignataro (Azienda Ospedaliera Universitaria Policlinico—V. Emanuele, Catania, Dipartimento di Medicina);
- -
- Francesca Mete, Miriam Gino (Ospedale degli Infermi di Rivoli, Torino, Medicina Interna);
- -
- Guido Moreo, Silvia Prolo, Gloria Pina (Clinica San Carlo Casa di Cura Polispecialistica, Paderno Dugnano, Milano, Unità Operativa di Medicina Generale Emilio Bernardelli);
- -
- Alberto Ballestrero, Fabio Ferrando, Roberta Gonella, Domenico Cerminara, Paolo Setti, Chiara Traversa, Camilla Scarsi (Clinica Di Medicina Interna ad Indirizzo Oncologico, Azienda Ospedaliera Università San Martino di Genova);
- -
- Bruno Graziella, Stefano Baldassarre, Salvatore Fragapani, Gabriella Gruden (Medicina Interna III, Ospedale S. Giovanni Battista Molinette, Torino);
- -
- Franco Berti, Giuseppe Famularo, Patrizia Tarsitani (Azienda Ospedaliera San Camillo Forlanini, Roma, Medicina Interna II);
- -
- Roberto Castello, Michela Pasino (Ospedale Civile Maggiore Borgo Trento, Verona, Medicina Generale e Sezione di Decisione Clinica);
- -
- Marcello Giuseppe Maggio Gian Paolo Ceda, Simonetta Morganti, Andrea Artoni, Margherita Grossi (Azienda Ospedaliero Universitaria di Parma, U.O.C Clinica Geriatrica);
- -
- Stefano Del Giacco, Davide Firinu, Giulia Costanzo, Giacomo Argiolas, Giovanni Paoletti, Francesca Losa (Policlinico Universitario Duilio Casula, Azienda Ospedaliero-Universitaria di Cagliari, Cagliari, Medicina Interna, Allergologia ed Immunologia Clinica);
- -
- Giuseppe Montalto, Anna Licata, Filippo Alessandro Montalto (Azienda Ospedaliera Universitaria Policlinico Paolo Giaccone, Palermo, UOC di Medicina Interna);
- -
- Francesco Corica, Giorgio Basile, Antonino Catalano, Federica Bellone, Concetto Principato (Azienda Ospedaliera Universitaria Policlinico G. Martino, Messina, Unità Operativa di Geriatria);
- -
- Lorenzo Malatino, Benedetta Stancanelli, Valentina Terranova, Salvatore Di Marca, Rosario Di Quattro, Lara La Malfa, Rossella Caruso (Azienda Ospedaliera per l’Emergenza Cannizzaro, Catania, Clinica Medica Università di Catania);
- -
- Patrizia Mecocci, Carmelinda Ruggiero, Virginia Boccardi (Università degli Studi di Perugia-Azienda Ospedaliera S.M. della Misericordia, Perugia, Struttura Complessa di Geriatria);
- -
- Tiziana Meschi, Andrea Ticinesi, Antonio Nouvenne (Azienda Ospedaliera Universitaria di Parma, U.O Medicina Interna e Lungodegenza Critica);
- -
- Pietro Minuz, Luigi Fondrieschi, Giandomenico Nigro Imperiale, Sarah Morellini (Azienda Ospedaliera Universitaria Verona, Policlinico GB Rossi, Verona, Medicina Generale per lo Studio ed il Trattamento dell’Ipertensione Arteriosa);
- -
- Mario Pirisi, Gian Paolo Fra, Daniele Sola, Mattia Bellan (Azienda Ospedaliera Universitaria Maggiore della Carità, Medicina Interna 1);
- -
- Roberto Quadri, Erica Larovere, Marco Novelli (Ospedale di Ciriè, ASL TO4, Torino, S.C. Medicina Interna);
- -
- Emilio Simeone, Rosa Scurti, Fabio Tolloso (Ospedale Spirito Santo di Pescara, Geriatria);
- -
- Roberto Tarquini, Alice Valoriani, Silvia Dolenti, Giulia Vannini (Ospedale San Giuseppe, Empoli, USL Toscana Centro, Firenze, Medicina Interna I);
- -
- Riccardo Volpi, Pietro Bocchi, Alessandro Vignali (Azienda Ospedaliera Universitaria di Parma, Clinica e Terapia Medica);
- -
- Sergio Harari, Chiara Lonati, Federico Napoli, Italia Aiello (Divisione di Medicina Interna, Multimedica IRCSS, Milano);
- -
- Francesco Purrello, Antonino Di Pino (Ospedale Garibaldi—Nesima—Catania, U.O.C Medicina Interna);
- -
- Teresa Salvatore, Lucio Monaco, Carmen Ricozzi (Policlinico Università della Campania L. Vanvitelli, UOC Medicina Interna);
- -
- Alberto Pilotto, Ilaria Indiano, Federica Gandolfo (Ente Ospedaliero Ospedali Galliera Genova, SC Geriatria Dipartimento Cure Geriatriche, Ortogeriatria e Riabilitazione);
- -
- Franco Laghi Pasini, Pier Leopoldo Capecchi (Azienda Ospedaliera Universitaria Senese, Siena, Unità Operativa Complessa Medicina 2);
- -
- Ranuccio Nuti, Roberto Valenti, Martina Ruvio, Silvia Cappelli, Alberto Palazzuoli (Azienda Ospedaliera Università Senese, Siena, Medicina Interna I);
- -
- Mauro Bernardi, Silvia Li Bassi, Luca Santi, Giacomo Zaccherini (Azienda Ospedaliera Policlinico Sant’Orsola-Malpighi, Bologna, Semeiotica Medica Bernardi);
- -
- Vittorio Durante, Daniela Tirotta, Giovanna Eusebi (Ospedale di Cattolica, Rimini, Medicina Interna);
- -
- Marco Cattaneo, Maria Valentina Amoruso, Paola Fracasso, Cristina Fasolino (Azienda ospedaliera San Paolo, Milano, Medicina III);
- -
- Moreno Tresoldi, Enrica Bozzolo, Sarah Damanti (IRCCS Ospedale San Raffaele—Milano, Medicina Generale e delle Cure Avanzate);
- -
- Massimo Porta, Miriam Gino (AOU Città della Salute e della Scienza di Torino—Torino, Medicina Interna 1U).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Inpatient with Diabetes (%) | O.R. In-Hospital Mortality | O.R. 3-Months Mortality | O.R. 12-Months Mortality |
|---|---|---|---|---|
| Hypertension | 57.1 | 0.53 (0.33–0.84) | 0.60 (0.44–0.99) | 0.67 (0.49–1.11) |
| Ischemic heart disease | 31.3 | 0.55 (0.31–0.97) | 0.71 (0.54–1.43) | 0.64 (0.26–1.49) |
| Chronic renal failure | 28.9 | 1.19 (0.73–1.95) | 1.17 (0.72–1.87) | 1.13 (0.41–2.23) |
| Atrial fibrillation | 26.0 | 0.92 (0.54–1.57) | 1.07 (0.74–1.96) | 1.28 (1.05–5.07) |
| COPD | 22.7 | 1.31 (0.77–2.23) | 1.12 (0.58–1.71) | 0.79 (0.04–1.01) |
| Heart Failure | 22.6 | 1.27 (0.77–2.13) | 1.36 (0.81–2.20) | 1.50 (0.85–4.38) |
| Anemia | 22.0 | 1.11 (0.64–1.92) | 1.33 (0.83–2.32) | 1.29 (0.54–3.21) |
| Peripheral artery disease | 17.6 | 0.61 (0.30–1.26) | 0.53 (0.22–0.98) | 1.13 (0.54–2.87) |
| Cancer | 17.5 | 1.74 (1.01–3.04) | 2.02 (1.28–3.52) | 3.62 (1.49–9.78) |
| Atherosclerosis | 14.2 | 0.74 (0.33–1.66) | 0.60 (0.19–1.27) | 0.78 (0.31–3.13) |
| Hypertensive heart disease | 13.9 | 0.81 (0.40–1.65) | 0.36 (0.03–0.50) | 0.88 (0.37–1.13) |
| Gastritis | 13.8 | 0.17 (0.42–0.72) | 0.78 (0.34–2.07) | 0.87 (0.19–2.43) |
| Prostatic hypertrophy | 12.7 | 1.02 (0.52–2.03) | 0.96 (0.52–1.89) | 1.14 (0.70–4.78) |
| Rheumatic diseases | 12.4 | 0.59 (0.23–1.51) | 0.40 (0.09–0.98) | 0.32 (0.13–1.56) |
| Cerebrovascular disease | 11.3 | 0.59 (0.07–4.64) | 0.89 (0.38–2.94) | 0.57 (0.21–2.09) |
| Vasculitis | 10.7 | 0.62 (0.15–2.69) | 0.96 (0.48–2.60) | 0.54 (0.23–2.34) |
| Arthrosis | 10.6 | 0.33 (0.10–1.06) | 0.26 (0.08–0.79) | 0.23 (0.14–0.78) |
| Hypercholesterolemia | 10.0 | 0.47 (0.17–1.32) | 0.62 (0.34–1.70) | 0.94 (0.33–4.77) |
| Dementia | 9.1 | 3.32 (1.95–5.66) | 2.39 (1.01–2.83) | 2.10 (1.03–3.53) |
References
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.Z. Diabetes and its drivers: The largest epidemic in human history? Clin. Diabetes Endocrinol. 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Global Health Estimates. Disease Burden by Cause, Age, Sex, by Country and by Region, 2000–2016; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. Prevalence of Both Diagnosed and Undiagnosed Diabetes. Available online: https://www.cdc.gov/diabetes/data/statistics-report/diagnosed-undiagnosed-diabetes.html (accessed on 25 August 2021).
- Huang, E.S. Management of diabetes mellitus in older people with comorbidities. BMJ 2016, 353, i2200. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, Expenditures, and Complications of Multiple Chronic Conditions in the Elderly. Arch. Intern. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Zghebi, S.S.; Steinke, D.T.; Rutter, M.K.; Ashcroft, D.M. Eleven-year multimorbidity burden among 637 255 people with and without type 2 diabetes: A population-based study using primary care and linked hospitalisation data. BMJ Open 2020, 10, e033866. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Natoli, G.; Mularo, S.; Nobili, A.; Monaco, M.L.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Corrao, S. Impact of Diabetes Mellitus and Its Comorbidities on Elderly Patients Hospitalized in Internal Medicine Wards: Data from the RePoSi Registry. Healthcare 2022, 10, 86. [Google Scholar] [CrossRef]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R.; et al. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019, 17, 145, Erratum in BMC Med. 2020, 18, 22. [Google Scholar] [CrossRef]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef]
- Divo, M.; Cote, C.; de Torres, J.P.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.; Zulueta, J.; Cabrera, C.; Zagaceta, J.; Hunninghake, G.; et al. Comorbidities and Risk of Mortality in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2012, 186, 155–161. [Google Scholar] [CrossRef]
- Trudzinski, F.C.; Jörres, R.A.; Alter, P.; Walter, J.; Watz, H.; Koch, A.; John, M.; Lommatzsch, M.; Vogelmeier, C.F.; Kauczor, H.-U.; et al. Sex-specific associations of comorbidome and pulmorbidome with mortality in chronic obstructive pulmonary disease: Results from COSYCONET. Sci. Rep. 2022, 12, 8790. [Google Scholar] [CrossRef]
- Meireles, M.A.; Golçalves, J.; Neves, J. Acute Heart Failure Comorbidome: The Impact of Everything Else. Acta Med. Port. 2020, 33, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Uddin, S.; Srinivasan, U. Comorbidity network for chronic disease: A novel approach to understand type 2 diabetes progression. Int. J. Med Inform. 2018, 115, 1–9. [Google Scholar] [CrossRef]
- Argano, C.; Scichilone, N.; Natoli, G.; Nobili, A.; Corazza, G.R.; Mannucci, P.M.; Perticone, F.; Corrao, S.; Pietrangelo, A.; Licata, G.; et al. Pattern of comorbidities and 1-year mortality in elderly patients with COPD hospitalized in internal medicine wards: Data from the RePoSI Registry. Intern. Emerg. Med. 2020, 16, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Arcoraci, V.; Barbieri, M.A.; Rottura, M.; Nobili, A.; Natoli, G.; Argano, C.; Squadrito, G.; Squadrito, F.; Corrao, S.; REPOSI Investigators. Kidney Disease Management in the Hospital Setting: A Focus on Inappropriate Drug Prescriptions in Older Patients. Front. Pharmacol. 2021, 12, 749711. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Argano, C.; Natoli, G.; Nobili, A.; Corazza, G.R.; Mannucci, P.M.; Perticone, F.; REPOSI Investigators. Sex-Differences in the Pattern of Comorbidities, Functional Independence, and Mortality in Elderly Inpatients: Evidence from the RePoSI Register. J. Clin. Med. 2019, 8, 81. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef]
- Mannucci, P.M.; Nobili, A.; Pasina, L.; REPOSI Collaborators. Polypharmacy in older people: Lessons from 10 years of experience with the REPOSI register. Intern. Emerg. Med. 2018, 13, 1191–1200. [Google Scholar] [CrossRef]
- Corrao, S.; Pinelli, K.; Vacca, M.; Raspanti, M.; Argano, C. Type 2 Diabetes Mellitus and COVID-19: A Narrative Review. Front. Endocrinol. 2021, 12, 609470. [Google Scholar] [CrossRef]
- Corrao, S.; REPOSI Investigators; Natoli, G.; Nobili, A.; Mannucci, P.M.; Pietrangelo, A.; Perticone, F.; Argano, C. Comorbidity does not mean clinical complexity: Evidence from the RePoSI register. Intern. Emerg. Med. 2019, 15, 621–628. [Google Scholar] [CrossRef]
- Corrao, S.; Argano, C.; Natoli, G.; Nobili, A.; Corazza, G.; Mannucci, P.; Perticone, F. Disability, and not diabetes, is a strong predictor of mortality in oldest old patients hospitalized with pneumonia. Eur. J. Intern. Med. 2018, 54, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Pasina, L.; Cococcia, S.; Cortesi, L.; Miceli, E.; Caccia Dominioni, C.; Pisati, M.; Mengoli, C.; Perticone, F.; Nobili, A.; et al. Mortality rate and risk factors for gastrointestinal bleeding in elderly patients. Eur. J. Intern. Med. 2019, 61, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef]
- Beloosesky, Y.; Weiss, A.; Mansur, N. Validity of the Medication-based Disease Burden Index compared with the Charlson Comorbidity Index and the Cumulative Illness Rating Scale for geriatrics: A cohort study. Drugs Aging 2011, 28, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Nobili, A.; Natoli, G.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Argano, C.; REPOSI Investigators. Hyperglycemia at admission, comorbidities, and in-hospital mortality in elderly patients hospitalized in internal medicine wards: Data from the RePoSI Registry. Acta Diabetol. 2021, 58, 1225–1236. [Google Scholar] [CrossRef]
- Gofir, A.; Mulyono, B.; Sutarni, S. Hyperglycemia as a prognosis predictor of length of stay and functional outcomes in patients with acute ischemic stroke. Int. J. Neurosci. 2017, 127, 923–929. [Google Scholar] [CrossRef]
- Ryg, J.; Engberg, H.; Mariadas, P.; Pedersen, S.G.H.; Jorgensen, M.G.; Vinding, K.L.; Andersen-Ranberg, K. Barthel Index at hospital admission is associated with mortality in geriatric patients: A Danish nationwide population-based cohort study. Clin. Epidemiol. 2018, 10, 1789–1800. [Google Scholar] [CrossRef]
- Tsalamandris, S.; Antonopoulos, A.S.; Oikonomou, E.; Papamikroulis, G.-A.; Vogiatzi, G.; Papaioannou, S.; Deftereos, S.; Tousoulis, D. The Role of Inflammation in Diabetes: Current Concepts and Future Perspectives. Eur. Cardiol. Rev. 2019, 14, 50–59. [Google Scholar] [CrossRef]
- O’Brien, H.; O’Leary, N.; Scarlett, S.; O’Hare, C.; Kenny, R.A. Hospitalisation and surgery: Are there hidden cognitive consequences? Evidence from The Irish Longitudinal study on Ageing (TILDA). Age Ageing 2018, 47, 408–415. [Google Scholar] [CrossRef]
- Argano, C.; Catalano, N.; Natoli, G.; Monaco, M.L.; Corrao, S. GDS score as screening tool to assess the risk of impact of chronic conditions and depression on quality of life in hospitalized elderly patients in internal medicine wards. Medicine 2021, 100, e26346. [Google Scholar] [CrossRef]
- Ganz, T. Anemia of Inflammation. N. Engl. J. Med. 2019, 381, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Dick, S.A.; Epelman, S. Chronic Heart Failure and Inflammation: What Do We Really Know? Circ. Res. 2016, 119, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T. Epidemiological Evidence of the Relationship Between Diabetes and Dementia. Diabetes Mellit. 2019, 1128, 13–25. [Google Scholar]
- Feuerer, M.; Shen, Y.; Littman, D.R.; Benoist, C.; Mathis, D. How Punctual Ablation of Regulatory T Cells Unleashes an Autoimmune Lesion within the Pancreatic Islets. Immunity 2009, 31, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef]
- Di Chiara, T.; Argano, C.; Scaglione, A.; Corrao, S.; Pinto, A.; Scaglione, R. Circulating adiponectin: A cardiometabolic marker associated with global cardiovascular risk. Acta Cardiol. 2015, 70, 33–40. [Google Scholar] [CrossRef]
- Di Chiara, T.; Licata, A.; Argano, C.; Duro, G.; Corrao, S.; Scaglione, R. Plasma adiponectin: A contributing factor for cardiac changes in visceral obesity-associated hypertension. Blood Press. 2014, 23, 147–153. [Google Scholar] [CrossRef]
- Di Chiara, T.; Argano, C.; Scaglione, A.; Duro, G.; Corrao, S.; Scaglione, R.; Licata, G. Hypoadiponectinemia, cardiometabolic comorbidities and left ventricular hypertrophy. Intern. Emerg. Med. 2014, 10, 33–40. [Google Scholar] [CrossRef]
- Di Chiara, T.; Argano, C.; Corrao, S.; Scaglione, R.; Licata, G. Hypoadiponectinemia: A Link between Visceral Obesity and Metabolic Syndrome. J. Nutr. Metab. 2012, 2012, 175245. [Google Scholar] [CrossRef]
- Satish, S.; Freeman, D.H., Jr.; Ray, L.; Goodwin, J.S. The Relationship Between Blood Pressure and Mortality in the Oldest Old. J. Am. Geriatr. Soc. 2001, 49, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Odden, M.C.; Peralta, C.A.; Haan, M.N.; Covinsky, K.E. Rethinking the association of high blood pressure with mortality in elderly adults: The impact of frailty. Arch. Intern. Med. 2012, 172, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Langan, R.C. Men’s Health: Benign Prostatic Hyperplasia. FP Essent. 2021, 503, 18–22. [Google Scholar]
- Parsons, J.K. Benign Prostatic Hyperplasia and Male Lower Urinary Tract Symptoms: Epidemiology and Risk Factors. Curr. Bl. Dysfunct. Rep. 2010, 5, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.K.; Carter, H.B.; Partin, A.W.; Windham, B.G.; Metter, E.J.; Ferrucci, L.; Landis, P.; Platz, E.A. Metabolic factors associated with benign prostatic hyperplasia. J. Clin. Endocrinol. Metab. 2006, 91, 2562–2568. [Google Scholar] [CrossRef]
- Tseng, C.H. Benign prostatic hyperplasia is a significant risk factor for bladder cancer in diabetic patients: A population-based cohort study using the National Health Insurance in Taiwan. BMC Cancer 2013, 13, 7. [Google Scholar] [CrossRef]
- Vrsalovic, M.; Vucur, K.; Vrsalovic Presecki, A.; Fabijanic, D.; Milosevic, M. Impact of diabetes on mortality in peripheral artery disease: A meta-analysis. Clin. Cardiol. 2017, 40, 287–291. [Google Scholar] [CrossRef]
- Low Wang, C.C.; Blomster, J.I.; Heizer, G.; Berger, J.S.; Baumgartner, I.; Fowkes, F.G.R.; Held, P.; Katona, B.G.; Norgren, L.; Jones, W.S.; et al. Cardiovascular and Limb Outcomes in Patients with Diabetes and Peripheral Artery Disease: The EUCLID Trial. J. Am. Coll. Cardiol. 2018, 72, 3274–3284. [Google Scholar] [CrossRef]
- Hanyu, H. Diabetes-Related Dementia. Diabetes Mellit. 2019, 1128, 147–160. [Google Scholar] [CrossRef]
- Xue, M.; Xu, W.; Ou, Y.-N.; Cao, X.-P.; Tan, M.-S.; Tan, L.; Yu, J.-T. Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing Res. Rev. 2019, 55, 100944. [Google Scholar] [CrossRef]
- Bruce, D.G.; Davis, T.M.E.; Davis, W.A. Dementia complicating type 2 diabetes and the influence of premature mortality: The Fremantle Diabetes Study. Acta Diabetol. 2019, 56, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.; Li, J.; Wei, W.; Wang, L.; Zhang, Y.; Li, J.; Wang, C.; Sun, S. Association between diabetes mellitus and breast cancer risk: A meta-analysis of the literature. Asian Pac. J. Cancer Prev. 2011, 12, 1061–1065. [Google Scholar]
- Ben, Q.; Xu, M.; Ning, X.; Liu, J.; Hong, S.; Huang, W.; Zhang, H.; Li, Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur. J. Cancer 2011, 47, 1928–1937. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, X.; Gong, G.; Ben, Q.; Qiu, W.; Chen, Y.; Li, G.; Wang, L. Increased risk of hepatocellular carcinoma in patients with diabetes mellitus: A systematic review and meta-analysis of cohort studies. Int. J. Cancer 2011, 130, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Joh, H.-K.; Willett, W.C.; Cho, E. Type 2 Diabetes and the Risk of Renal Cell Cancer in Women. Diabetes Care 2011, 34, 1552–1556. [Google Scholar] [CrossRef]
- Chen, H.-F.; Liu, M.-D.; Chen, P.; Chen, L.-H.; Chang, Y.-H.; Wen, P.-C.; Li, C.-Y. Risks of Breast and Endometrial Cancer in Women with Diabetes: A Population-Based Cohort Study. PLoS ONE 2013, 8, e67420. [Google Scholar] [CrossRef]
- Jiang, Y.; Ben, Q.; Shen, H.; Lu, W.; Zhang, Y.; Zhu, J. Diabetes mellitus and incidence and mortality of colorectal cancer: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 2011, 26, 863–876. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, X.; Shen, Z.; Lu, Y.; Zhong, S.; Xu, C. Risk of bladder cancer in patients with diabetes mellitus: An updated meta-analysis of 36 observational studies. BMC Cancer 2013, 13, 310. [Google Scholar] [CrossRef]
- Mitri, J.; Castillo, J.; Pittas, A.G. Diabetes and risk of Non-Hodgkin’s lymphoma: A meta-analysis of observational studies. Diabetes Care 2008, 31, 2391–2397. [Google Scholar] [CrossRef]
- Collins, K.K. The Diabetes-Cancer Link. Diabetes Spectr. 2014, 27, 276–280. [Google Scholar] [CrossRef]
- Vigneri, P.; Frasca, F.; Sciacca, L.; Pandini, G.; Vigneri, R. Diabetes and cancer. Endocr. Relat. Cancer 2009, 16, 1103–1123. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Forte, V.; Abdallah, M.; Alickaj, A.; Mahmud, S.; Asad, S.; McFarlane, S.I. Diabetes mellitus and the risk of cancer. Minerva Endocrinol. 2011, 36, 187–209. [Google Scholar] [PubMed]
- Scappaticcio, L.; Maiorino, M.I.; Bellastella, G.; Giugliano, D.; Esposito, K. Insights into the relationships between diabetes, prediabetes, and cancer. Endocrine 2016, 56, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Ryu, T.Y.; Park, J.; Scherer, P.E. Hyperglycemia as a Risk Factor for Cancer Progression. Diabetes Metab. J. 2014, 38, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Wojciechowska, J.; Krajewski, W.; Bolanowski, M.; Kręcicki, T.; Zatoński, T. Diabetes and Cancer: A Review of Current Knowledge. Exp. Clin. Endocrinol. Diabetes 2016, 124, 263–275. [Google Scholar] [CrossRef]
- Li, W.; Zhang, X.; Sang, H.; Zhou, Y.; Shang, C.; Wang, Y.; Zhu, H. Effects of hyperglycemia on the progression of tumor diseases. J. Exp. Clin. Cancer Res. 2019, 38, 327. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrao, S.; Natoli, G.; Nobili, A.; Mannucci, P.M.; Perticone, F.; Arcoraci, V.; Argano, C., on behalf of the REPOSI Investigators. The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes. Healthcare 2022, 10, 1459. https://doi.org/10.3390/healthcare10081459
Corrao S, Natoli G, Nobili A, Mannucci PM, Perticone F, Arcoraci V, Argano C on behalf of the REPOSI Investigators. The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes. Healthcare. 2022; 10(8):1459. https://doi.org/10.3390/healthcare10081459
Chicago/Turabian StyleCorrao, Salvatore, Giuseppe Natoli, Alessandro Nobili, Pier Mannuccio Mannucci, Francesco Perticone, Vincenzo Arcoraci, and Christiano Argano on behalf of the REPOSI Investigators. 2022. "The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes" Healthcare 10, no. 8: 1459. https://doi.org/10.3390/healthcare10081459
APA StyleCorrao, S., Natoli, G., Nobili, A., Mannucci, P. M., Perticone, F., Arcoraci, V., & Argano, C., on behalf of the REPOSI Investigators. (2022). The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes. Healthcare, 10(8), 1459. https://doi.org/10.3390/healthcare10081459