
Piperacillin–Tazobactam Plus Vancomycin-Associated Acute Kidney Injury in Adults: Can Teicoplanin or Other Antipseudomonal Beta-Lactams Be Remedies?



Abstract
:1. Introduction
2. Epidemiology of TZP Plus VAN-Associated AKI
3. Epidemiology of TZP Plus VAN-Associated AKI in ICU Patients
4. How Can We Reduce the Risk of AKI due to TZP–VAN Exposure?
4.1. Restricting the Use of TZP–VAN Combination Therapy for More Than 72 h
4.2. Administration of TZP as an Extended Infusion Regimen
4.3. Application of Area under Curve (AUC)-Guided VAN Dosing
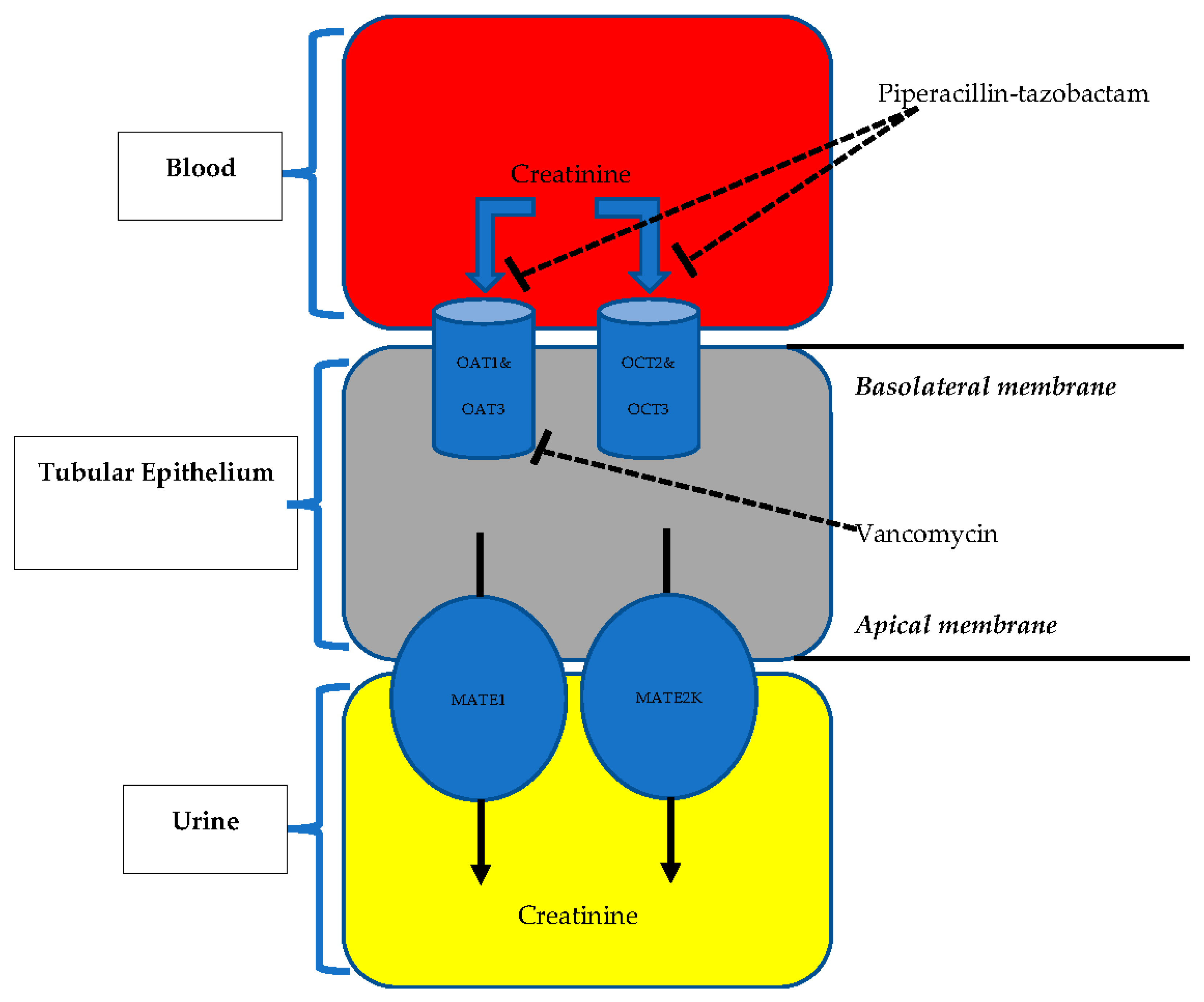
5. Pathophysiological Mechanisms of TZP Plus VAN-Associated AKI
6. Comparison of TZP–TEI and TZP–VAN Regimens in Terms of AKI Risk
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, H.E.; Muntner, P.; Chertow, G.M.; Warnock, D.G. Acute kidney injury and mortality in hospitalized patients. Am. J. Nephrol. 2012, 35, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslan, A.T.; Akova, M. The role of colistin in the era of new β-lactam β-lactamase inhibitor combinations. Antibiotics 2022, 11, 277. [Google Scholar] [CrossRef] [PubMed]
- Aslan, A.T.; Kırbas, E.; Sancak, B.; Tanriverdi, E.S.; Otlu, B.; Gursoy, N.C.; Yilmaz, Y.A.; Tozluyurt, A.; Liste, U.; Bicakcigil, A.; et al. A retrospective observational cohort study of the clinical epidemiology of bloodstream infections due to carbapenem-resistant Klebsiella pneumoniae in an OXA-48 endemic setting. Int. J. Antimicrob. Agents 2022, 59, 106554. [Google Scholar] [CrossRef] [PubMed]
- Nolin, T.D. Vancomycin and the risk of AKI: Now clearer than Mississippi mud. Clin. J. Am. Soc. Nephrol. 2016, 11, 2101–2103. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, C.A.; Patel, C.R.; Kale-Pradhan, P.B. Is the combination of piperacillin-tazobactam and vancomycin associated with development of acute kidney injury? A metanalysis. Pharmacotherapy 2016, 36, 1217–1228. [Google Scholar] [CrossRef]
- Elyasi, S.; Khalili, H.; Dashti-Khavidaki, S.; Mohammadpour, A. Vancomycin-induced nephrotoxicity: Mechanism, incidence, risk factors and special populations. A literature review. Eur. J. Clin. Pharmacol. 2012, 68, 1243–1255. [Google Scholar] [CrossRef]
- Bamgbola, O. Review of vancomycin-induced renal toxicity: An update. Ther. Adv. Endocrinol. Metab. 2016, 7, 136–147. [Google Scholar] [CrossRef]
- Luque, Y.; Louis, K.; Jouanneau, C.; Placier, S.; Esteve, E.; Bazin, D.; Rondeau, E.; Letavernier, E.; Wolfromm, A.; Gosset, C.; et al. Vancomycin-associated cast nephropathy. J. Am. Soc. Nephrol. 2017, 28, 1723–1728. [Google Scholar] [CrossRef] [Green Version]
- Rutter, W.C.; Cox, J.N.; Martin, C.A.; Burgess, D.R.; Burgess, D.S. Nephrotoxicity during vancomycin therapy in combination with piperacillin-tazobactam or cefepime. Antimicrob. Agents Chemother. 2017, 24, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Rutter, W.C.; Burgess, D.S. Incidence of acute kidney injury among patients treated with piperacillin-tazobactam or meropenem in combination with vancomycin. Antimicrob. Agents Chemother. 2018, 62, e00264-18. [Google Scholar] [CrossRef] [Green Version]
- Rutter, W.C.; Burgess, D.R.; Talbert, J.C.; Burgess, D.S. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: A retrospective cohort analysis. J. Hosp. Med. 2017, 12, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellos, I.; Karageorgiou, V.; Pergialiotis, V.; Perrea, D.N. Acute kidney injury following the concurrent administration of antipseudomonal β-lactams and vancomycin: A network meta-analysis. Clin. Microbiol. Infect. 2020, 26, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.A.; Smith, M.N.; Li, C.; Hayes, S.M.; Lusardi, K.; Bookstaver, P.B. Systematic review and meta-analysis of acute kidney injury associated with concomitant vancomycin and piperacillin/tazobactam. Clin. Infect. Dis. 2017, 64, 666–674. [Google Scholar] [CrossRef]
- Butler, M.S.; Hansford, K.A.; Blaskovich, M.A.T.; Halai, R.; Cooper, M.A. Glycopeptide antibiotics: Back to the future. J. Antibiot. 2014, 67, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Svetitsky, S.; Leibovici, L.; Paul, M. Comparative efficacy and safety of vancomycin versus teicoplanin: Systematic review and meta-analysis. Antimicrob. Agents Chemother. 2009, 53, 4069–4079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, A.B.; Goncalves, A.R.; Almeida, C.S.; Bugano, D.D.; Silva, E. Teicoplanin versus vancomycin for proven or suspected infection. Cochrane Database Syst. Rev. 2010, CD007022. [Google Scholar] [CrossRef] [PubMed]
- Hellwig, T.; Hammerquist, R.; Loecker, B.; Shields, J. Retrospective evaluation of the incidence of vancomycin and/or piperacillin-tazobactam induced acute renal failure. Crit. Care Med. 2011, 39, 79. [Google Scholar] [CrossRef]
- Moenster, R.P.; Linneman, T.W.; Finnegan, P.M.; Hand, S.; Thomas, Z.; McDonald, J.R. Acute renal failure associated with vancomycin and β-lactams for the treatment of osteomyelitis in diabetics: Piperacilline-tazobactam as compared with cefepime. Clin. Microbiol. Infect. 2014, 20, O384–O389. [Google Scholar] [CrossRef] [Green Version]
- Gomes, D.M.; Smotherman, C.; Birch, A.; Dupree, L.; Della Vecchia, B.J.; Kraemer, D.F.; Jankowski, C.A. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy 2014, 34, 662–669. [Google Scholar] [CrossRef]
- Hammond, D.A.; Smith, M.N.; Painter, J.T.; Meena, N.K.; Lusardi, K. Comparative incidence of acute kidney injury in critically ill patients receiving vancomycin with concomitant piperacillin-tazobactam or cefepime: A retrospective cohort study. Pharmacotherapy 2016, 36, 463–471. [Google Scholar] [CrossRef]
- Al Yami, M.S. Comparison of the incidence of acute kidney injury during treatment with vancomycin in combination with piperacilline-tazobactam or with meropenem. J. Infect. Public Health 2017, 10, 770–773. [Google Scholar] [CrossRef] [PubMed]
- Jeon, N.; Staley, B.; Klinker, K.P.; Hincapie Castillo, J.; Winterstein, A.G. Acute kidney injury risk associated with piperacillin/tazobactam compared with cefepime during vancomycin therapy in hospitalised patients: A cohort study stratified by baseline kidney function. Int. J. Antimicrob. Agents 2017, 50, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Navalkele, B.; Pogue, J.M.; Karino, S.; Nishan, B.; Salim, M.; Solanki, S.; Pervaiz, A.; Tashtoush, N.; Shaikh, H.; Koppula, S.; et al. Risk of acute kidney injury in patients on concomitant vancomycin and piperacilline-tazobactam compared to those on vancomycin and cefepime. Clin. Infect. Dis. 2017, 64, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Peyko, V.; Smalley, S.; Cohen, H. Prospective comparison of acute kidney injury during treatment with the combination of piperacillin-tazobactam and vancomycin versus the combination of cefepime or meropenem and vancomycin. J. Pharm. Pract. 2017, 30, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.M.; Douce, R.W.; Grubbs, E.R.; Wills, C.B.; Khan, A.; Schmidt, E.M.; Wang, M.S. Comparison of Acute Kidney Injury during Treatment with Vancomycin and either Piperacillin-Tazobactam or Meropenem. Spartan Med. Res. J. 2017, 2, 6440. [Google Scholar] [CrossRef] [PubMed]
- Clemmons, A.B.; Bech, C.F.; Pantin, J.; Ahmad, I. Acute kidney injury in hematopoietic cell transplantation patients receiving vancomycin and piperacillin/ tazobactam versus vancomycin and cefepime. Biol. Blood Marrow Transplant. 2018, 24, 820–826. [Google Scholar] [CrossRef] [Green Version]
- Mullins, B.P.; Kramer, C.J.; Bartel, B.J.; Catlin, J.S.; Gilder, R.E. Comparison of the nephrotoxicity of vancomycin in combination with cefepime, meropenem, or piperacillin/tazobactam: A prospective, multicenter study. Ann. Pharmacother. 2018, 52, 639–644. [Google Scholar] [CrossRef]
- Robertson, A.D.; Li, C.; Hammond, D.A.; Dickey, T.A. Incidence of acute kidney injury among patients receiving the combination of vancomycin with piperacillin-tazobactam or meropenem. Pharmacotherapy 2018, 38, 1184–1193. [Google Scholar] [CrossRef]
- Balcı, C.; Uzun, O.; Arıcı, M.; Hayran, S.A.; Yüce, D.; Ünal, S. Nephrotoxicity of piperacillin/tazobactam combined with vancomycin: Should it be a concern? Int. J. Antimicrob. Agents 2018, 52, 180–184. [Google Scholar] [CrossRef]
- Buckley, M.S.; Hartsock, N.C.; Berry, A.J.; Bikin, D.S.; Richards, E.C.; Yerondopoulos, M.J.; Kobic, E.; Wicks, L.M.; Hammond, D.A. Comparison of acute kidney injury risk associated with vancomycin and concomitant piperacillin/tazobactam or cefepime in the intensive care unit. J. Crit. Care 2018, 48, 32–38. [Google Scholar] [CrossRef]
- Ide, N.; Sato, S.; Sawaguchi, K. Risk of acute kidney injury in patients treated with vancomycin and piperacillin/tazobactam compared to vancomycin and meropenem or doripenem: A retrospective cohort study. Yakugaku Zasshi 2019, 139, 1609–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreier, D.J.; Kashani, K.B.; Sakhuja, A.; Mara, K.C.; Tootooni, M.S.; Personett, H.A.; Nelson, S.; Rule, A.D.; Steckelberg, J.M.; Tande, A.J.; et al. Incidence of acute kidney injury among critically ill patients with brief empiric use of antipseudomonal β-lactams with vancomycin. Clin. Infect. Dis. 2019, 68, 1456–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blevins, A.M.; Lashinsky, J.N.; McCammon, C.; Kollef, M.; Micek, S.; Juang, P. Incidence of acute kidney injury in critically ill patients receiving vancomycin with concomitant piperacillin-tazobactam, cefepime, or meropenem. Antimicrob. Agents Chemother. 2019, 63, e02658-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.; Park, J.; Yu, Y.M.; Park, M.S.; Han, E.; Chang, M.J. Comparison of acute kidney injury and clinical prognosis of vancomycin monotherapy and combination therapy with beta-lactams in the intensive care unit. PLoS ONE 2019, 14, e0217908. [Google Scholar] [CrossRef] [Green Version]
- Molina, K.C.; Barletta, J.F.; Hall, S.T.; Yazdani, C.; Huang, V. The risk of acute kidney injury in critically ill patients receiving concomitant vancomycin with piperacilline tazobactam or cefepime. J. Intensive Care Med. 2019, 35, 1434–1438. [Google Scholar] [CrossRef]
- Haruki, Y.; Hagiya, H.; Haruki, M.; Inoue, Y.; Sugiyama, T. Concomitant vancomycin and piperacillin/tazobactam treatment is associated with an increased risk of acute kidney injury in Japanese patients. J. Infect. Chemother. 2020, 26, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, K.; Hay, K.; Lavana, J.; McNamara, J.F. Acute kidney injury with combination vancomycin and piperacillin-tazobactam therapy in the ICU: A retrospective cohort study. Int. J. Antimicrob. Agents 2020, 56, 106010. [Google Scholar] [CrossRef]
- Yabes, J.M.; Stewart, L.; Shaikh, F.; Robben, P.M.; Petfield, J.L.; Ganesan, A.; Campbell, W.R.; Tribble, D.R.; Blyth, D.M. Risk of acute kidney injury in combat-injured patients associated with concomitant vancomycin and extended-spectrum β-lactam antibiotic use. J. Intensive Care Med. 2021, 36, 818–827. [Google Scholar] [CrossRef]
- Aslan, A.T.; Pashayev, T.; Dag, O.; Akova, M. Comparison of teicoplanin versus vancomycin in combination with piperacillin-tazobactam or meropenem for the risk of acute kidney injury. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1953–1961. [Google Scholar] [CrossRef]
- Tookhi, R.F.; Kabli, N.A.; Huntul, M.A.; Thabit, A.K. Impact of combining vancomycin with piperacillin/tazobactam or with meropenem on vancomycin-induced nephrotoxicity. Intern. Emerg. Med. 2021, 16, 975–979. [Google Scholar] [CrossRef]
- Elliott, B.P.; Tang, M.M.; Madden, J.A.; Markert, R.J.; Burdette, S.D.; Pleiman, C.M.; Speelmon, E.C. A retrospective cohort study assessing acute kidney injury and renal recovery among septic patients empirically treated with vancomycin piperacillin–tazobactam versus vancomycin cefepime. Intern. Emerg. Med. 2022, 17, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.Y.; Xu, R.X.; Zhou, X.; Liu, Y.; Hu, C.Y.; Xie, X.F. Acute kidney injury associated with concomitant vancomycin and piperacillin/tazobactam administration: A systematic review and meta-analysis. Int. Urol. Nephrol. 2018, 50, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Luther, M.K.; Timbrook, T.T.; Caffrey, A.R.; Dosa, D.; Lodise, T.P.; LaPlante, K.L. Vancomycin plus piperacillin-tazobactam and acute kidney in jury in adults: A systematic review and meta-analysis. Crit. Care Med. 2018, 46, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Ciarambino, T.; Giannico, O.V.; Campanile, A.; Tirelli, P.; Para, O.; Signoriello, G.; Giordano, M. Acute kidney injury and vancomycin/piperacillin/tazobactam in adult patients: A systematic review. Intern. Emerg. Med. 2020, 15, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, A.M.; Alzahrani, M.Y.; Abujamal, M.A.; Abdalla, M.H.; Alowais, S.A.; Alfayez, O.M.; Alyami, M.S.; Almutairi, A.R.; Almohammed, O.A. Comparative risk of acute kidney injury following concurrent administration of vancomycin with piperacillin/tazobactam or meropenem: A systematic review and meta-analysis of observational studies. Antibiotics 2022, 11, 526. [Google Scholar] [CrossRef] [PubMed]
- Karino, S.; Kaye, K.S.; Navalkele, B.; Nishan, B.; Salim, M.; Solanki, S.; Pervaiz, A.; Tashtoush, N.; Shaikh, H.; Koppula, S.; et al. Epidemiology of acute kidney injury among patients receiving concomitant vancomycin and piperacillin-tazobactam: Opportunities for antimicrobial stewardship. Antimicrob. Agents Chemother. 2016, 60, 3743–3750. [Google Scholar] [CrossRef] [Green Version]
- Neely, M.N.; Kato, L.; Youn, G.; Kraler, L.; Bayard, D.; van Guilder, M.; Schumitzky, A.; Yamada, W.; Jones, B.; Minejima, E. Prospective trial on the use of trough concentration versus area under the curve to determine therapeutic vancomycin dosing. Antimicrob. Agents Chemother. 2018, 62, e02042-17. [Google Scholar] [CrossRef] [Green Version]
- Linder, A.; Fjell, C.; Levin, A.; Walley, K.R.; Russell, J.A.; Boyd, J.H. Small acute increases in serum creatinine are associated with decreased long-term survival in the critically ill. Am. J. Respir. Crit. Care Med. 2014, 189, 1075–1081. [Google Scholar] [CrossRef]
- Self, W.H.; Wunderink, R.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Balk, R.A.; Fakhran, S.S.; Chappell, J.D.; Casimir, G.; Courtney, D.M.; et al. Staphylococcus aureus community-acquired pneumonia: Prevalence, clinical characteristics, and outcomes. Clin. Infect. Dis. 2016, 63, 300–309. [Google Scholar] [CrossRef] [Green Version]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Lorenz, M.A.; Moenster, R.P.; Linneman, T.W. Effect of piperacillin/tazobactam restriction on usage and rates of acute renal failure. J. Med. Microbiol. 2016, 65, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traversa, A.; Hammond, D.A.; Peksa, G.D.; DeMott, J.M. Short versus extended duration vancomycin and piperacillin/tazobactam and the incidence of acute kidney injury in noncritically ill patients. J. Pharm. Pract. 2021, 34, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Watkins, R.R.; Deresinski, S. Increasing evidence of the nephrotoxicity of piperacillin/tazobactam and vancomycin combination therapy-what is the clinician to do? Clin. Infect. Dis. 2017, 65, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, N.J.; Liu, J.; O’Donnell, J.N.; Dulhunty, J.M.; Abdul-Aziz, M.H.; Berko, P.Y.; Nadler, B.; Lipman, J.; Roberts, J.A. Prolonged infusion piperacillin-tazobactam decreases mortality and improves outcomes in severely ill patients: Results of a systematic review and meta-analysis. Crit. Care Med. 2018, 46, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Ram, R.; Halavy, Y.; Amit, O.; Paran, Y.; Katchman, E.; Yachini, B.; Kor, S.; Avivi, I.; Ben-Ami, R. Extended vs bolus infusion of broad-spectrum β-lactams for febrile neutropenia: An unblinded, randomized trial. Clin. Infect. Dis. 2018, 67, 1153–1160. [Google Scholar] [CrossRef]
- Cotner, S.E.; Rutter, W.C.; Burgess, D.R.; Wallace, K.L.; Martin, C.A.; Burgess, D.S. Influence of β-lactam infusion strategy on acute kidney injury. Antimicrob. Agents Chemother. 2017, 61, e00871-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousavi, M.; Zapolskaya, T.; Scipione, M.R.; Louie, E.; Papadopoulos, J.; Dubrovskaya, Y. Comparison of rates of nephrotoxicity associated with vancomycin in combination with piperacillin-tazobactam administered as an extended versus standard infusion. Pharmacotherapy 2017, 37, 379–385. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kawasaki, K.; Sato, Y.; Tokimatsu, I.; Itoh, H.; Hiramatsu, K.; Takeyama, M.; Kadota, J. Is peak concentration needed in therapeutic drug monitoring of vancomycin? A pharmacokinetic-pharmacodynamic analysis in patients with methicillin-resistant Staphylococcus aureus pneumonia. Chemotherapy 2012, 58, 308–312. [Google Scholar] [CrossRef]
- Lodise, T.P.; Patel, N.; Lomaestro, B.M.; Rodvold, K.A.; Drusano, G.L. Relationship between initial vancomycin concentration-time profile and nephrotoxicity among hospitalized patients. Clin. Infect. Dis. 2009, 49, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Van Hal, S.J.; Paterson, D.L.; Lodise, T.P. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob. Agents Chemother. 2013, 57, 734–744. [Google Scholar] [CrossRef] [Green Version]
- Aljefri, D.M.; Avedissian, S.N.; Rhodes, N.J.; Postelnick, M.J.; Nguyen, K.; Scheetz, M.H. Vancomycin area under the curve and acute kidney injury: A meta-analysis. Clin. Infect. Dis. 2019, 69, 1881–1887. [Google Scholar] [CrossRef]
- Avedissian, S.N.; Pais, G.M.; O’Donnell, J.N.; Lodise, T.P.; Liu, J.; Prozialeck, W.C.; Joshi, M.D.; Lamar, P.C.; Becher, L.; Gulati, A.; et al. Twenty-four hour pharmacokinetic relationships for intravenous vancomycin and novel urinary biomarkers of acute kidney injury in a rat model. J. Antimicrob. Chemother. 2019, 74, 2326–2334. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, N.J.; Prozialeck, W.C.; Lodise, T.P.; Venkatesan, N.; O’Donnell, J.N.; Pais, G.; Cluff, C.; Lamar, P.C.; Neely, M.N.; Gulati, A.; et al. Evaluation of vancomycin exposures associated with elevations in novel urinary biomarkers of acute kidney injury in vancomycin-treated rats. Antimicrob. Agents Chemother. 2016, 60, 5742–5751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, N.A.; Zasowski, E.J.; Murray, K.P.; Mynatt, R.P.; Zhao, J.J.; Yost, R.; Pogue, J.M.; Rybak, M.J. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycin-associated nephrotoxicity. Antimicrob. Agents Chemother. 2017, 61, e01293-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muklewicz, J.D.; Steuber, T.D.; Edwards, J.D. Evaluation of area underneath the concentration-time curve-guided vancomycin dosing with or without piperacillin-tazobactam on the incidence of acute kidney ınjury. Int. J. Antimicrob. Agents 2021, 57, 106234. [Google Scholar] [CrossRef]
- Waikar, S.S.; Betensky, R.A.; Emerson, S.C.; Bonventre, J.V. Imperfect gold standards for kidney injury biomarker evaluation. J. Am. Soc. Nephrol. 2012, 23, 13–21. [Google Scholar] [CrossRef]
- Duarte, C.G.; Preuss, H.G. Assessment of renal function–glomerular and tubular. Clin. Lab. Med. 1993, 13, 33–52. [Google Scholar] [CrossRef]
- Kastrup, J.; Petersen, P.; Bartram, R.; Hansen, J.M. The effect of trimethoprim on serum creatinine. Br. J. Urol. 1985, 57, 265–268. [Google Scholar] [CrossRef]
- Naderer, O.; Nafziger, A.N.; Bertino, J.S., Jr. Effects of moderate-dose versus high-dose trimethoprim on serum creatinine and creatinine clearance and adverse reactions. Antimicrob. Agents Chemother. 1997, 41, 2466–2470. [Google Scholar] [CrossRef] [Green Version]
- Komuro, M.; Maeda, T.; Kakuo, H.; Matsushita, H.; Shimada, J. Inhibition of the renal excretion of tazobactam by piperacillin. J. Antimicrob. Chemother. 1994, 34, 555–564. [Google Scholar] [CrossRef]
- Wen, S.; Wang, C.; Duan, Y.; Huo, X.; Meng, Q.; Liu, Z.; Yang, S.; Zhu, Y.; Sun, H.; Ma, X.; et al. OAT1 and OAT3 also mediate the drug-drug interaction between piperacillin and tazobactam. Int. J. Pharm. 2018, 537, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Vallon, V.; Eraly, S.A.; Rao, S.R.; Gerasimova, M.; Rose, M.; Nagle, M.; Anzai, N.; Smith, T.; Sharma, K.; Nigam, S.K.; et al. A role for the organic anion transporter OAT3 in renal creatinine secretion in mice. Am. J. Physiol. Renal Physiol. 2012, 302, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.; Wang, C.; Huo, X.; Meng, Q.; Liu, Z.; Yang, S.; Zhu, Y.; Sun, H.; Ma, X.; Liu, K. JBP485 attenuates vancomycin-induced nephrotoxicity by regulating the expressions of organic anion transporter (Oat) 1, Oat3, organic cation transporter 2 (Oct2), multidrug resistance-associated protein 2 (Mrp2) and P-glycoprotein (P-gp) in rats. Toxicol. Lett. 2018, 295, 195–204. [Google Scholar] [CrossRef]
- Avedissian, S.N.; Pais, G.M.; Liu, J.; Rhodes, N.J.; Scheetz, M.H. Piperacillin-tazobactam added to vancomycin increases risk for acute kidney injury: Fact or fiction? Clin. Infect. Dis. 2020, 71, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Pais, G.M.; Avedissian, S.N.; O’Donnell, J.N.; Rhodes, N.J.; Lodise, T.P.; Prozialeck, W.C.; Lamar, P.C.; Cluff, C.; Gulati, A.; Fitzgerald, J.C.; et al. Comparative performance of urinary biomarkers for vancomycin-induced kidney injury according to timeline of injury. Antimicrob. Agents Chemother. 2019, 63, e00079-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidya, V.S.; Ozer, J.S.; Dieterle, F.; Collings, F.B.; Ramirez, V.; Troth, S.; Muniappa, N.; Thudium, D.; Gerhold, D.; Holder, D.J.; et al. Kidney injury molecule-1 outperforms traditional biomarkers of kidney injury in preclinical biomarker qualification studies. Nat. Biotechnol. 2010, 28, 478–485. [Google Scholar] [CrossRef] [Green Version]
- Kane-Gill, S.L.; Ostermann, M.; Shi, J.; Joyce, E.L.; Kellum, J.A. Evaluating renal stress using pharmacokinetic urinary biomarker data in critically ill patients receiving vancomycin and/or piperacillin-tazobactam: A secondary analysis of the multicenter Sapphire study. Drug Saf. 2019, 42, 1149–1155. [Google Scholar] [CrossRef]
- Liu, T.J.; Lam, J.P. Piperacillin-tazobactam-induced acute interstitial nephritis with possible meropenem cross-sensitivity in a patient with osteomyelitis. Am. J. Health Syst. Pharm. 2012, 69, 1109. [Google Scholar] [CrossRef]
- Pill, M.W.; O’Neill, C.V.; Chapman, M.M.; Singh, A.K. Suspected acute interstitial nephritis induced by piperacillin-tazobactam. Pharmacotherapy 1997, 17, 166–169. [Google Scholar]
- Waring, W.S.; Moonie, A. Earlier recognition of nephrotoxicity using novel biomarkers of acute kidney injury. Clin. Toxicol. 2011, 49, 720–728. [Google Scholar] [CrossRef]
- Pratt, J.A.; Stricherz, M.K.; Verghese, P.S.; Burke, M.J. Suspected piperacillin-tazobactam in- duced nephrotoxicity in the pediatric oncology population. Pediatr. Blood Cancer. 2014, 61, 366–368. [Google Scholar] [CrossRef] [PubMed]
- Sawada, A.; Kawanishi, K.; Morikawa, S.; Nakano, T.; Kodama, M.; Mitobe, M.; Taneda, S.; Koike, J.; Ohara, M.; Nagashima, Y.; et al. Biopsy-proven vancomycin-induced acute kidney injury: A case report and literature review. BMC Nephrol. 2018, 19, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokol, H.; Vigneau, C.; Maury, E.; Guidet, B.; Offenstadt, G. Biopsy-proven anuric acute tubular necrosis associated with vancomycin and one dose of aminoside. Nephrol. Dial. Transplant. 2004, 19, 1921–1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, L.D.; Drew, R.H. Comparison of the incidence of vancomycin-induced nephrotoxicity in hospitalized patients with and without concomitant piperacillin-tazobactam. Pharmacotherapy 2014, 34, 670–676. [Google Scholar] [CrossRef]
- Pais, G.M.; Liu, J.; Avedissian, S.N.; Hiner, D.; Xanthos, T.; Chalkias, A.; d’Aloja, E.; Locci, E.; Gilchrist, A.; Prozialeck, W.C.; et al. Lack of synergistic nephrotoxicity between vancomycin and piperacillin/tazobactam in a rat model and a confirmatory cellular model. J. Antimicrob. Chemother. 2020, 75, 1228–1236. [Google Scholar] [CrossRef]
- Shao, C.H.; Tai, C.H.; Lin, F.J.; Wu, C.C.; Wang, J.T.; Wang, C.C. Comparison of risk of acute kidney injury between patients receiving the combination of teicoplanin and piperacillin/tazobactam versus vancomycin and piperacillin/tazobactam. J. Formos. Med. Assoc. 2022, 121, 117–125. [Google Scholar] [CrossRef]
- Workum, J.D.; Kramers, C.; Kolwijck, E.; Schouten, J.A.; de Wildt, S.N.; Brüggemann, R.J. Nephrotoxicity of concomitant piperacillin/tazobactam and teicoplanin compared with monotherapy. J. Antimicrob. Chemother. 2021, 76, 212–219. [Google Scholar] [CrossRef]
- Tai, C.H.; Shao, C.H.; Wang, C.C.; Lin, F.J.; Wang, J.T.; Wu, C.C. Nephrotoxicity of teicoplanin-based combination therapy: Focus on piperacillin/tazobactam and other antipseudomonal β-lactams. J. Antimicrob. Chemother. 2021, 76, 499–506. [Google Scholar] [CrossRef]


{kind=link}
| Authors and Type | Year | Country | Population | Definition of AKI * | ICU Residence and/or Critically Ill, % | Sample Size, n | Exposure to Other Nephrotoxins, % | Mean or Initial VAN Trough Level (mg/dl) | Treatment Duration, Days | Comparison Groups | Rate of AKI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Moenster RP, et al. R, SC, [18] | 2014 | USA | Adult patients with or without renal dysfunction | RIFLE | Not provided | 139 | Yes, percentage unknown | 15.8 vs. 14.5 | 14.7 vs. 11.3 | TZP–VAN vs. FEP–VAN | 29.3% vs. 13.3%; OR, 3.45 (0.96–12.4); p: 0.05 |
| Gomes DM, et al. R, SC, [19] | 2014 | USA | Adult patients without renal dysfunction | AKIN | 34.8 vs. 53.6 | 224 | Yes, percentage unknown | 14.1 vs. 13.06 | 7.1 vs. 6.7 | TZP–VAN vs. FEP–VAN | 34.8% vs. 12.5%; OR, 3.74 (1.89–7.39); p: <0.001 |
| Hammond DA, et al. R, SC, [20] | 2016 | USA | Adult patients without renal dysfunction | AKIN | 100 | 122 | Yes, percentage unknown | 17.9 vs. 15.1 | Not provided | TZP–VAN vs. FEP–VAN | 32.7% vs. 28.8%; p: 0.76 |
| Al Yami MS, et al. R, MC, [21] | 2017 | Saudi Arabia and USA | Adult patients without renal dysfunction | KDIGO | 17.6 vs. 17.3 | 183 | 62.9 vs. 46.6 | 15.7 vs. 16.9 | 4.3 vs. 5.4 | TZP–VAN vs. MER–VAN | 7.4% vs. 5.3%; p: 0.4 |
| Rutter WC, et al. R, SC, [9] | 2017 | USA | Adult patients with or without renal dysfunction | RIFLE | Not provided | 4193 | 60.7 vs. 59.4 | Percentage of >20 mg/L 30.4% vs. 27.4% | 3.0 vs. 4.0 | TZP–VAN vs. FEP–VAN | 21.4% vs. 12.5%; OR, 2.18 (1.64–2.94); p: < 0.001 |
| Jeon N, et al. R, SC, [22] | 2017 | USA | Adult patients with or without renal dysfunction | KDIGO | 14.09 vs. 18.75 | 5335 | Yes, percentage unknown | Percentage of >20 mg/L 2.5% vs. 1.9% | 5.0 vs. 5.0 | TZP–VAN vs. FEP–VAN | 19.6% vs. 16.2%; aHR, 1.25 (1.11–1.42); p: < 0.05 |
| Navalkele B, et al. R, SC, [23] | 2017 | USA | Adult patients without renal dysfunction | RIFLE and AKIN | 21 vs. 23 | 558 | Yes, percentage unknown | 17.3 vs. 17.7 | Not provided | TZP–VAN vs. FEP–VAN | 29% vs. 11%; HR, 4.27 (2.73–6.68); p: <0.001 |
| Peyko V, et al. P, SC, [24] | 2017 | USA | Adult patients with or without renal dysfunction | KDIGO | Not provided | 85 | 33.9 vs. 38.5 | 16.6 vs. 18.3 | Not provided | TZP–VAN vs. MER–VAN or FEP–VAN | 37.3% vs. 7.7%; p: 0.005 |
| Cannon JM, et al. R, SC, [25] | 2017 | USA | Adult patients without renal dysfunction | RIFLE | 15.8 vs. 31.1 | 366 | Yes, percentage unknown | Percentage of >20 mg/L 21.9% vs. 28.4% | Not provided | TZP–VAN vs. MER–VAN | 25.3% vs. 9.5%; p: 0.008 |
| Clemmons AB, et al. R, SC, [26] | 2018 | Georgia | Adult patients with or without renal dysfunction | KDIGO | Not provided | 170 | Not provided | Percentage of >20 mg/L 42.9% vs. 31.6% | 4.0 vs. 4.0 | TZP–VAN vs. FEP–VAN | 68% vs. 27%; OR, 5.1 (2.5–10.5); p: < 0.001 |
| Mullins BP, et al. P, MC, [27] | 2018 | USA | Adult patients without renal dysfunction | RIFLE | 34 vs. 41 | 242 | Yes, percentage unknown | 16.3 vs. 15.2 | 5.4 vs. 6.4 | TZP–VAN vs. MER–VAN or FEP–VAN | 29.8% vs. 8.8%; OR, 6.6 (2.8–15.8), p: <0.001 |
| Robertson AD, et al. R, SC, [28] | 2018 | USA | Adult patients without renal dysfunction | RIFLE | 0 | 169 | 81.2 vs. 83.3 | Percentage of >20 mg/L 21.2% vs. 19.0% | 4.6 vs. 4.7 | TZP–VAN vs. MER–VAN | 16.5% vs. 3.6%; OR, 6.8 (1.5–0.9); p: 0.009 |
| Balcı C, et al. R, SC, [29] | 2018 | Turkey | Adult patients with or without renal dysfunction | AKIN | Not provided | 132 | 52.8 vs. 65.2 | Not provided | Not provided | TZP–VAN vs. MER–VAN | 41.3% vs. 10.1%; OR, 0.33 (0.21–0.77); p: <0.001 |
| Buckley MS, et al. R, SC, [30] | 2018 | USA | Adult patients with or without renal dysfunction | RIFLE | 100 | 333 | Yes, percentage unknown | 13.5 vs. 13.1 | 5.1 vs. 5.8 | TZP–VAN vs. FEP–VAN | 19.5% vs. 17.3%; OR, 0.86 (0.49–1.53); p: 0.6 |
| Rutter WC, et al. R, SC, [10] | 2018 | USA | Adult patients with or without renal dysfunction | RIFLE | Not provided | 10,236 | Yes, percentage unknown | Not provided | 5.0 vs. 5.0 | TZP–VAN vs. MER–VAN | 27.4% vs. 15.4 %; OR, 2.53 (1.82–3.52); p: < 0.001 |
| Ide N, et al. R, SC, [31] | 2019 | Japan | Adult patients with or without renal dysfunction | KDIGO | 0 | 82 | Yes, percentage unknown | Percentage of >15 mg/L 52.0% vs. 50.0% | Not provided | TZP–VAN vs. MER–VAN | 33.3% vs. 9.1%; p: 0.015 |
| Schreier DJ, et al. R, SC, [32] | 2019 | USA | Adult patients with or without renal dysfunction | AKIN | 100 | 3299 | Yes, percentage unknown | Not provided | All patients received 24-72 h combination therapy | TZP–VAN vs. MER–VAN vs. FEP–VAN | 1.04 (0.71–1.42); p: 0.84 1.11 (0.85–1.45); p: 0.44 |
| Blevins AM, et al. R, SC, [33] | 2019 | USA | Adult patients with or without renal dysfunction | KDIGO | 100 | 2492 | 76.0 vs. 82.7 vs. 78.0 | 12.0 vs. 12.0 vs. 11.6 | 4.0 vs. 3.0 vs. 3.0 | TZP–VAN vs. MER–VAN vs. FEP–VAN | 39.3% vs. 23.5% vs. 24.2%; OR, 2.16 (1.62–2.88); p: < 0.001 |
| Kang S, et al. R, SC, [34] | 2019 | South Korea | Adult patients with or without renal dysfunction | KDIGO | 100 | 340 | Yes, percentage unknown | Not provided | 6.5 vs. 8.0 vs. 8.0 | TZP–VAN vs. MER–VAN vs. VAN | 52.7% vs. 27.7% vs. 25.7%; p: <0.001 |
| Molina KC, et al. R, SC, [35] | 2019 | USA | Adult patients without renal dysfunction | AKIN | 100 | 394 | Yes, percentage unknown | 11.2 vs. 11.0 | 3.3 vs. 3.7 | TZP–VAN vs. FEP–VAN | 28.7% vs. 21.3%; OR, 1.50 (0.88–2.57); p: 0.13 |
| Haruki Y, et al. R, SC, [36] | 2020 | Japan | Adult patients without renal dysfunction | RIFLE | 25.0 vs. 28.3 | 272 | 68.5 vs. 67.8 | 13.3 vs. 13.4 | 6.0 vs. 7.0 | TZP–VAN vs. VAN-Other β-lactams | 25.0% vs. 12.2%; OR, 2.40 (1.20–4.78); p: 0.01 |
| O’ Callaghan K et al. R, SC, [37] | 2020 | Australia | Adult patients with or without renal dysfunction | AKIN | 100 | 260 | Yes, percentage unknown | Not provided | 4.0 vs. 5.0 | TZP–VAN vs. MER–VAN or FEP–VAN | RRR, 2.2 (1.0–4.9); p: 0.05 |
| Yabes JM, et al. R, SC, [38] | 2021 | USA | Adult patients without renal dysfunction | RIFLE and AKIN | 88.5 vs. 93.7 | 268 | Yes, percentage unknown | 9.4 vs. 10.9 | Not provided | TZP–VAN vs. VAN-Other β-lactams | 13.1% vs. 9.7%; OR, 1.72 (1.02–2.76); p: 0.04 |
| Aslan AT, et al. R, SC, [39] | 2021 | Turkey | Adult patients with or without renal dysfunction | RIFLE | 32.0 vs. 34.6 | 154 | Yes, percentage unknown | Not provided | 5.0 vs. 9.0 | TZP–VAN vs. MER–VAN | 40.0% vs. 24.0%; aOR, 2.28 (1.01–5.18); p: 0.048 |
| Tookhi RF, et al. R, SC, [40] | 2021 | Saudi Arabia | Adult patients without renal dysfunction | KDIGO | 18.2 vs. 30.9 | 158 | 49.4 vs. 51.9 | Not provided | Not provided | TZP–VAN vs. MER–VAN | 10.4% vs. 21.0%; p: 0.07 |
| Elliott BP, et al. R, SC, [41] | 2022 | USA | Adult patients with sepsis | KDIGO | 100 | 418 | Yes, percentage unknown | Not provided | Not provided | TZP–VAN vs. FEP–VAN | 15.2% vs. 11.0%; p: 0.44 |
| Authors | Year | Total Number of Studies, n | Total Number of Patients | Deadline for Inclusion of Studies | Comparison Groups | The Risk of AKI | Additional or Secondary Results |
|---|---|---|---|---|---|---|---|
| Giuliano et al., [5] | 2016 | 15 (only studies including adult patients) | 3258 | 1 June 2016 | TZP–VAN vs. VAN alone TZP–VAN vs. VAN+ β-lactam TZP–VAN vs. VAN alone or VAN+ another antibiotic | TZP–VAN vs. VAN ± β-lactam: OR, 3.65; 95% CI, 2.15–6.17; I2 = 83.5%, p < 0.001 | Abstracts were removed: OR, 3.498; 95% CI 1.747–7.003, I2 = 82.3%, p < 0.001) Low-quality studies were removed: OR, 4.596; 95% CI 2.929–7.212; I2 = 0%, p < 0.001). |
| Hammond DM, et al., [13] | 2017 | 14 (11 included only adults and 3 included only children) | 3549 | October 2016 | TZP–VAN vs. VAN alone TZP–VAN vs. FEP–VAN TZP–VAN vs. VAN+ β-lactam | In adults: aOR, 3.15; 95% CI, 1.72–5.76 In children: OR, 4.55; 95% CI, 2.71–10.21 | <50% of patients received care in an ICU: aOR, 3.04; 95% CI, 1.49–6.22 ≥50% of patients received care in an ICU: aOR, 2.83; 95% CI, 0.74–10.85 |
| Chen et al., [42] | 2018 | 8 (7 included only adults and 1 included only children) | 10,727 | April 2017 | TZP–VAN vs. VAN+ β-lactam TZP–VAN vs. FEP–VAN TZP–VAN vs. VAN | TZP–VAN vs. VAN+ β-lactam: OR, 1.57; 95% CI, 1.13–2.01; I2 = 76.4%, p < 0.001 | TZP–VAN vs. FEP–VAN: OR, 1.50; 95% CI, 1.07–1.93; I2 = 80.5%, p < 0.001 TZP–VAN vs. VAN: OR, 1.49; 95% CI, 1.06–1.92; I2 = 84.1%, p < 0.001 |
| Luther et al., [43] | 2018 | 32 (Only studies including adult patients) | 24,799 | April 2017 | TZP–VAN vs. VAN alone TZP–VAN vs. FEP–VAN or carbapenem-VAN TZP–VAN vs. TZP | TZP–VAN vs. FEP or carbapenem-VAN: OR, 2.68; 95% CI, 1.83–3.91 TZP–VAN vs. VAN: OR, 3.40; 95% CI, 2.57–4.50 | Time to AKI for TZP–VAN vs. FEP–VAN or carbapenem: mean difference, −1.30; 95% CI, −3.00 to 0.41 d). |
| Ciarambino T, et al., [44] | 2020 | 6 (Only studies including adult patients) | 9672 | 2 June 2019 | TZP–VAN vs. VAN alone | OR, 2.77 (95% CI 1.94, 3.96); p < 0.0001 | Not provided |
| Bellos I, et al., [12] | 2020 | 47 (37 included only adults and 10 included only children) | 56,984 | 20 August 2019 | TZP–VAN vs. VAN alone TZP–VAN vs. FEP–VAN TZP–VAN vs. MER–VAN | TZP–VAN vs. VAN: OR, 2.05; 95% CI, 1.17–3.46 TZP–VAN vs. MER–VAN: OR, 1.84; 95% CI, 1.02–3.10 TZP–VAN vs. FEP–VAN: OR, 1.80; 95% CI, 1.13–2.77 | TZP–VAN insignificantly increased risk of severe AKI and requirement of RRT. Time to AKI, duration of AKI, recovery from AKI, length of hospitalization and mortality were similar between the comparison groups. |
| Alshehri AM, et al., [45] | 2022 | 12 (Only studies including adult patients) | 14,511 | November 2021 | TZP–VAN vs. MER–VAN | TZP–VAN vs. MER–VAN: OR, 2.31; 95%CI, 1.69–3.15 | The secondary outcomes, including hospital length of stay, RRT, or mortality were similar between the two groups |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslan, A.T.; Akova, M. Piperacillin–Tazobactam Plus Vancomycin-Associated Acute Kidney Injury in Adults: Can Teicoplanin or Other Antipseudomonal Beta-Lactams Be Remedies? Healthcare 2022, 10, 1582. https://doi.org/10.3390/healthcare10081582
Aslan AT, Akova M. Piperacillin–Tazobactam Plus Vancomycin-Associated Acute Kidney Injury in Adults: Can Teicoplanin or Other Antipseudomonal Beta-Lactams Be Remedies? Healthcare. 2022; 10(8):1582. https://doi.org/10.3390/healthcare10081582
Chicago/Turabian StyleAslan, Abdullah Tarık, and Murat Akova. 2022. "Piperacillin–Tazobactam Plus Vancomycin-Associated Acute Kidney Injury in Adults: Can Teicoplanin or Other Antipseudomonal Beta-Lactams Be Remedies?" Healthcare 10, no. 8: 1582. https://doi.org/10.3390/healthcare10081582
APA StyleAslan, A. T., & Akova, M. (2022). Piperacillin–Tazobactam Plus Vancomycin-Associated Acute Kidney Injury in Adults: Can Teicoplanin or Other Antipseudomonal Beta-Lactams Be Remedies? Healthcare, 10(8), 1582. https://doi.org/10.3390/healthcare10081582