

Excess Mortality among Physicians and Dentists during COVID-19 in Italy: A Cross-Sectional Study Related to a High-Risk Territory

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
- M1 = mortality in 2020 or 2021
- M0 = mean mortality in 2015–2019
- k: multiplicative constant used (100).
- Observed: observed mortality
- Attended: expected mortality
- n: number of deaths among doctors
- Ri: mortality rate in the reference population of the age group -i
- Pi: number of the population under observation in the population in the age group -i
- k: multiplicative constant used (100).
2.3. Statistical Analysis
3. Results
- -
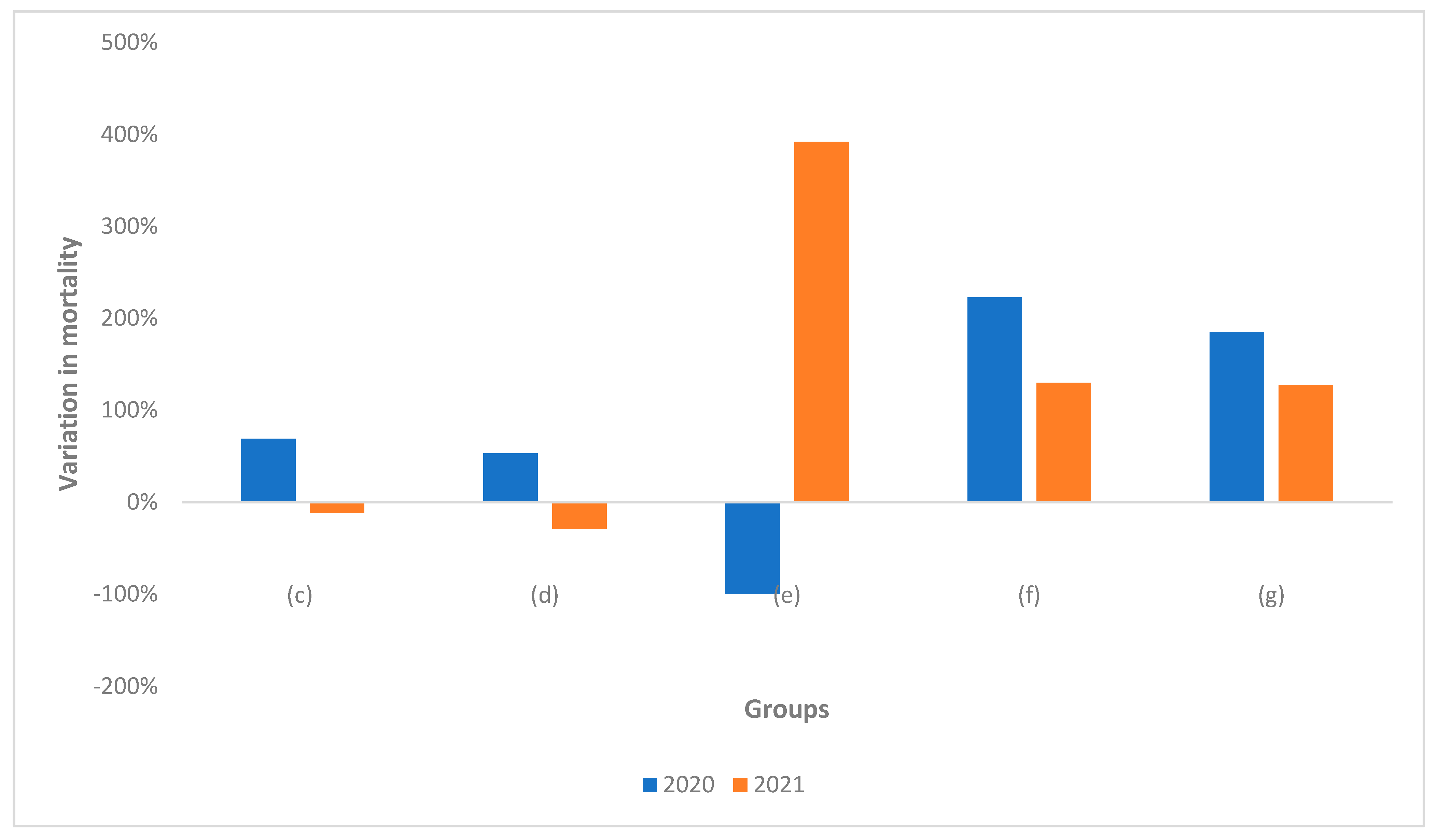
- Mortality increased significantly by 53%, 225% and 68% among physicians (d), physician-dentists (f) and total (c), respectively.
- -
- Considering the total number of dentists (g), mortality increased significantly by 175%.
- -
- Mortality increased significantly by 131% among dentists (f).
- -
- Considering the total number of dentists (g), mortality increased significantly by 127%.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Z.; Bing, X.; Zhi, X.Z. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Lu, H.; Stratton, C.W.; Tang, Y.-W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef]
- Dong, L.; Hu, S.; Gao, J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov. Ther. 2020, 14, 58–60. [Google Scholar] [CrossRef]
- Konstantinoudis, G.; Konstantinoudis, G.; Cameletti, M.; Gómez-Rubio, V.; Gómez, I.L.; Pirani, M.; Baio, G.; Larrauri, A.; Riou, J.; Egger, M.; et al. Regional excess mortality during the 2020 COVID-19 pandemic in five European countries. Nat. Commun. 2020, 13, 482. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P.A. What Other Countries Can Learn from Italy During the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 927–928. [Google Scholar] [CrossRef]
- Scortichini, M.; Schneider Dos Santos, R.; De’ Donato, F.; De Sario, M.; Michelozzi, P.; Davoli, M.; Masselot, P.; Sera, F. & Gasparrini, A.. Excess mortality during the COVID-19 outbreak in Italy: A two-stage interrupted time-series analysis. Int. J. Epidemiol. 2021, 49, 1909–1917. [Google Scholar]
- Odone, A.; Delmonte, D.; Gaetti, G.; Signorelli, C. Doubled mortality rate during the COVID-19 pandemic in Italy: Quantifying what is not captured by surveillance. Public Health 2021, 190, 108–115. [Google Scholar] [CrossRef]
- Buja, A.; Paganini, M.; Fusinato, R.; Cozzolino, C.; Cocchio, S.; Scioni, M.; Rebba, V.; Baldo, V.; & Boccuzzo, G. Health and healthcare variables associated with Italy’s excess mortality during the first wave of the COVID-19 pandemic: An ecological study. Health Policy 2022, 126, 294–301. [Google Scholar] [CrossRef]
- Gatto, M.; Bertuzzo, E.; Mari, L.; Miccoli, S.; Carraro, L.; Casagrandi, R.; Rinaldo, A. Spread and dynamics of the COVID-19 epidemic in Italy: Effects of emergency containment measures. Proc. Natl. Acad. Sci. USA 2020, 117, 10484–10491. [Google Scholar]
- Antonini, C.; Calandrini, S.; Bianconi, F. Robustness analysis for quantitative assessment of vaccination effects and SARS-CoV-2 lineages in Italy. BMC Infect. Dis. 2022, 22, 415. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19). 2022 May 12. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M. A.; Aliabadi, S.; Seaman, S. R.; Harris, R. J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Emergence-of-SARS-CoV-2-B.1.617-Variants-in-India-and-Situation-in-the-EUEEA. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Emergence-of-SARS-CoV-2-B.1.617-variants-in-India-and-situation-in-the-EUEEA_0.pdf (accessed on 15 April 2022).
- COVID-19 Variants. Available online: https://www.gisaid.org/hcov19-variants/ (accessed on 15 April 2022).
- Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 15 April 2022).
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D. G.; Everatt, J.; Bhiman, J. N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Sheikh, A.; Kerr, S.; Woolhouse, M.; McMenamin, J.; Robertson, C. Severity of omicron variant of concern and effectiveness of vaccine boosters against symptomatic disease in Scotland (EAVE II): A national cohort study with nested test-negative design. Lancet Infect. Dis. 2022, 22, 959–966. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hong, V. X.; Patel, M. M.; Kahn, R.; Lipsitch, M.; Tartof, S.Y. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in southern California. Nat. Med. 2022, 1–11. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. COVID infection severity in children under 5 years old before and after Omicron emergence in the US. medRxiv. [CrossRef]
- Veneti, L.; Bøås, H.; Bråthen Kristoffersen, A.; Stålcrantz, J.; Bragstad, K.; Hungnes, O.; Storm, M. L.; Aasand, N.; Rø, G.; Starrfelt, J.; et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron BA.1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Eurosurveillance 2022, 27, 2200077. [Google Scholar] [CrossRef]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant COVID-19 outbreak in a large hospital in tshwane, south africa. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef]
- Davies, M.-A.; Kassanjee, R.; Rosseau, P.; Morden, E.; Johnson, L.; Solomon, W.; Hsiao, N.-Y.; Hussey, H.; Meintjes, G.; Paleker, M.; et al. Outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave compared with previous waves in the Western Cape Province, South Africa. medRxiv 2022. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Russo, A.G.; Tunesi, S.; Consolazio, D.; Decarli, A.; Bergamaschi, W. Evaluation of the anti-COVID-19 vaccination campaign in the Metropolitan Area of Milan (Lombardy Region, Northern Italy). Epidemiol. Prev. 2021, 45, 568–579. [Google Scholar]
- Amit, S.; Gonen, T.; Regev-Yochay, G. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. Reply. N. Engl. J. Med. 2021, 385, 1630–1631. [Google Scholar] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Odone, A.; Delmonte, D.; Scognamiglio, T.; Signorelli, C. COVID-19 deaths in Lombardy, Italy: Data in context. Lancet Public Health 2020, 5, e310. [Google Scholar] [CrossRef]
- Beaney, T.; Clarke, J.M.; Jain, V.; Golestaneh, A.K.; Lyons, G.; Salman, D.; Majeed, A. Excess mortality: The gold standard in measuring the impact of COVID-19 worldwide? J. R. Soc. Med. 2020, 113, 329–334. [Google Scholar] [CrossRef]
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Weinberger, D.M.; Hill, L. Excess Deaths From COVID-19 and Other Causes, March-April 2020. JAMA 2020, 324, 510–513. [Google Scholar] [CrossRef]
- Vestergaard, L.S.; Nielsen, J.; Krause, T.G.; Espenhain, L.; Tersago, K.; Bustos Sierra, N.; Denissov, G.; Innos, K.; Virtanen, M.J.; Fouillet, A.; et al. Excess all-cause and influenza-attributable mortality in Europe, December 2016 to February 2017. Eurosurveillance 2017, 22, 30506. [Google Scholar] [CrossRef]
- Understanding Excess Mortality—What is the Fairest Way to Compare COVID-19 Deaths Internationally? Available online: https://www.health.org.uk/news-and-comment/charts-and-infographics/understanding-excess-mortality-the-fairest-way-to-make-international-comparisons (accessed on 15 April 2022).
- Islam, M.I.; Freeman, J.; Chadwick, V.; Martiniuk, A. Healthcare Avoidance before and during the COVID-19 Pandemic among Australian Youth: A Longitudinal Study. Healthcare 2022, 10, 1261. [Google Scholar] [CrossRef]
- Hick, J.L.; Barbera, J.A.; Kelen, G.D. Refining surge capacity: Conventional, contingency, and crisis capacity. Disaster Med. Public Health Prep. 2009, 3, S59–S67. [Google Scholar] [CrossRef] [PubMed]
- Ing, E.B.; Xu, Q.A.; Salimi, A.; Torun, N. Physician deaths from corona virus (COVID-19) disease. Occup. Med. 2020, 70, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef] [PubMed]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Hassan Khamis, A.; Ho, S.B. COVID-19 and healthcare workers: A systematic review and meta-analysis. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 104, 335–346. [Google Scholar]
- Iyengar, K.P.; Ish, P.; Upadhyaya, G.K.; Malhotra, N.; Vaishya, R.; Jain, V.K. COVID-19 and mortality in doctors. Diabetes Metab. Syndr. 2020, 14, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; Kc, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A systematic review of droplet and aerosol generation in dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef]
- Motallebi, S.; Cheung, R.C.Y.; Mohit, B.; Shahabi, S.; Alishahi Tabriz, A.; Moattari, S. Modeling COVID-19 Mortality Across 44 Countries: Face Covering May Reduce Deaths. Am. J. Prev. Med. 2022, 62, 483–491. [Google Scholar] [CrossRef]
- Felice, C.; Di Tanna, G.L.; Zanus, G.; Grossi, U. Impact of COVID-19 Outbreak on Healthcare Workers in Italy: Results from a National E-Survey. J. Community Health 2020, 45, 675–683. [Google Scholar] [CrossRef]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) in Dentistry. Management of Biological Risk in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [Google Scholar] [CrossRef]
- Provincia di Pavia. Available online: https://it.wikipedia.org/wiki/Provincia_di_Pavia (accessed on 15 April 2022).
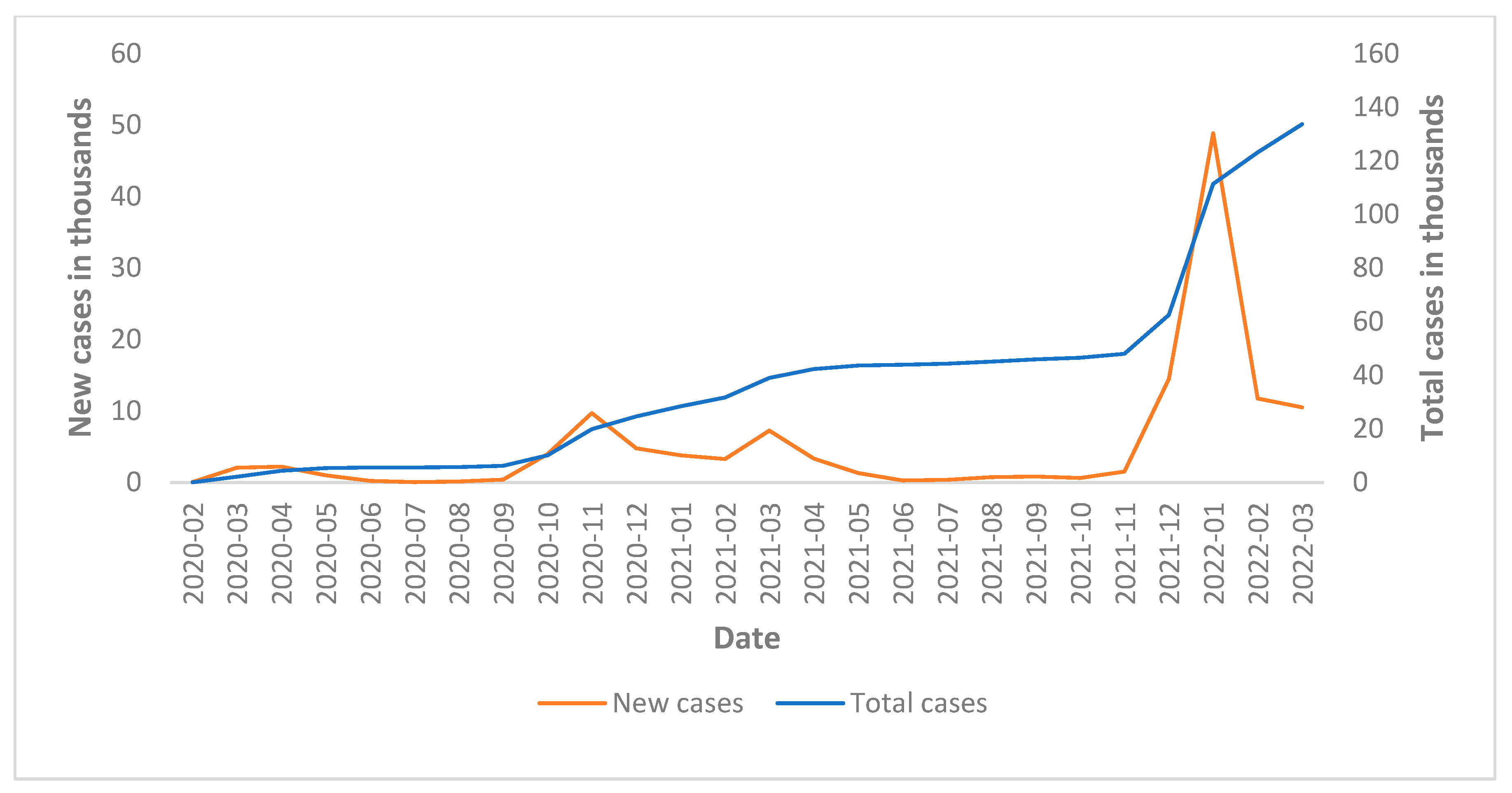
- Italian Civil Protection—Contagion Rates. Available online: https://github.com/pcm-dpc/COVID-19/tree/master/dati-province (accessed on 15 April 2022).
- Italian Istitute of Statistic—Mortality Rates. Available online: http://dati.istat.it/ (accessed on 15 April 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573. [Google Scholar] [CrossRef] [PubMed]
- Araja, D.; Berkis, U.; Murovska, M. COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View. Healthcare 2022, 10, 1018. [Google Scholar] [CrossRef] [PubMed]
- Perotti, P.; Bertuccio, P.; Cacitti, S.; Deandrea, S.; Boschetti, L.; Dalle Carbonare, S.; Marguati, S.; Migliazza, S.; Porzio, E.; Riboli, S.; et al. Impact of the COVID-19 Pandemic on Total and Cause-Specific Mortality in Pavia, Northern Italy. Int. J. Environ. Res. Public Health 2022, 19, 6498. [Google Scholar] [CrossRef] [PubMed]
- Cedrone, F.; Di Martino, G.; Di Giovanni, P.; Greco, E.; Trebbi, E.; Romano, F.; Staniscia, T. Reduction in Hospital Admissions for Cardiovascular Diseases (CVDs) during the Coronavirus Disease 2019 (COVID-19) Pandemic: A Retrospective Study from a Southern Italian Region in the Year 2020. Healthcare 2022, 10, 871. [Google Scholar] [CrossRef]
- Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Radu, D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania. Healthcare 2022, 10, 639. [Google Scholar] [CrossRef]
- Ren, Y.; Feng, C.; Rasubala, L.; Malmstrom, H.; Eliav, E. Risk for dental healthcare professionals during the COVID-19 global pandemic: An evidence-based assessment. J. Dent. 2020, 101, 103434. [Google Scholar] [CrossRef]
- Modenese, A.; Loney, T.; Gobba, F. COVID-19-Related Mortality amongst Physicians in Italy: Trend Pre- and Post-SARS-CoV-2 Vaccination Campaign. Healthcare 2022, 10, 1187. [Google Scholar] [CrossRef]
- Monami, M.; Gori, D.; Guaraldi, F.; Montalti, M.; Nreu, B.; Burioni, R.; Mannucci, E. COVID-19 Vaccine Hesitancy and Early Adverse Events Reported in a Cohort of 7881 Italian Physicians. Ann. Ig. 2022, 34, 344–357. [Google Scholar]
- Suppapitnarm, N.; Saengpattrachai, M. Physician Engagement before and during the COVID-19 Pandemic in Thailand. Healthcare 2022, 10, 1394. [Google Scholar] [CrossRef]
- Rupa, R.; Vladimirov, T.; Pojskic, M.; Nimsky, C.; Voellger, B. Dynamics in the Neurotrauma Catchment Area of a German University Hospital during the COVID-19 Pandemic. Healthcare 2022, 10, 1376. [Google Scholar] [CrossRef]
- Becerra, M.B.; Roland, T.C.; Avina, R.M.; Becerra, B.J. Unmet Healthcare Needs among College Students during the COVID-19 Pandemic: Implications for System-Wide and Structural Changes for Service Delivery. Healthcare 2022, 10, 1360. [Google Scholar] [CrossRef] [PubMed]
- Sono-Setati, M.E.; Mphekgwana, P.M.; Mabila, L.N.; Mbombi, M.O.; Muthelo, L.; Matlala, S.F.; Tshitangano, T.G.; Ramalivhana, N.J. Health System- and Patient-Related Factors Associated with COVID-19 Mortality among Hospitalized Patients in Limpopo Province of South Africa’s Public Hospitals. Healthcare 2022, 10, 1338. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, Y.; Guo, X. Research on the Equity and Influencing Factors of Medical and Health Resources Allocation in the Context of COVID-19: A Case of Taiyuan, China. Healthcare 2022, 10, 1319. [Google Scholar] [CrossRef] [PubMed]
- Çolak, E.; Çiftci, A.B. Acute Biliary Pancreatitis Management during the Coronavirus Disease 2019 Pandemic. Healthcare 2022, 10, 1284. [Google Scholar] [CrossRef] [PubMed]
- Enciu, B.G.; Tănase, A.A.; Drăgănescu, A.C.; Aramă, V.; Pițigoi, D.; Crăciun, M.D. The COVID-19 Pandemic in Romania: A Comparative Description with Its Border Countries. Healthcare 2022, 10, 1223. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, A.K.; Almalki, Z.S.; Albassam, A.A.; Alsultan, M.M.; Alshehri, A.M.; Ahmed, N.J.; Alqahtani, A.M. Factors Associated with Length of Hospital Stay among COVID-19 Patients in Saudi Arabia: A Retrospective Study during the First Pandemic Wave. Healthcare 2022, 10, 1201. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Description | Annotations | |
|---|---|---|---|
| a | Italian population | Entire Italian population, without exclusion of sex or age groups | |
| b | Population of the province of Pavia | Entire population residing in the Province of Pavia, without exclusion of sex or age groups | |
| c | All those enrolled in the register of physicians and dentists | All those enrolled in the Province of Pavia register of physicians and dentists with any qualification | c = d + e + f = d + g |
| d | Physicians | Those enrolled in the Province of Pavia register only with the qualification of physician | |
| e | Dentists | Those enrolled in the Province of Pavia register only with the qualification of dentist | |
| f | Physicians-Dentists | Those enrolled in the Province of Pavia register with the qualification of both physician and dentist | f ≠ d + e |
| g | Total Dentists | Those enrolled in the Province of Pavia register with the qualification of both physician and dentist plus those enrolled in the register with only the qualification of dentist | g = e + f |
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2015–2019 ** | |
|---|---|---|---|---|---|---|---|---|
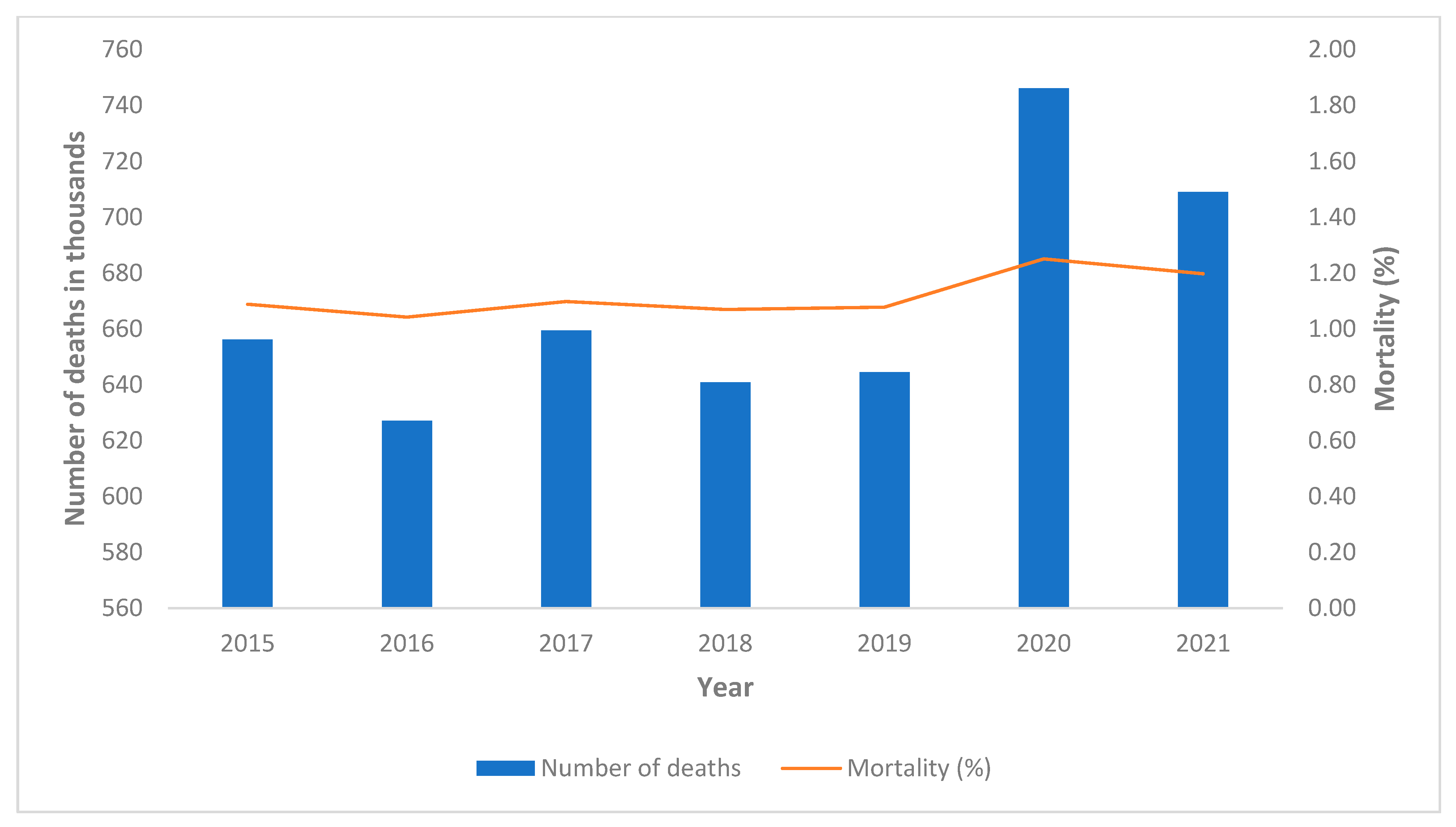
| Italy (a) | ||||||||
| Dead | 656,196 | 627,071 | 659,473 | 640,843 | 644,515 | 746,146 | 709,035 | 645,620 ± 12,960 |
| Population on January 1st | 60,295,497 | 60,163,712 | 60,066,734 | 59,937,769 | 59,816,673 | 59,641,488 | 59,236,213 | 60,056,077 ± 187,304 |
| Mortality | 1.09% | 1.04% | 1.10% | 1.07% | 1.08% | 1.25% | 1.20% | 1.08 ± 0.02% |
| Mortality variation * | 1.23% | −3.05% | 2.13% | −0.54% | 0.23% | 16.37% | 11.34% | |
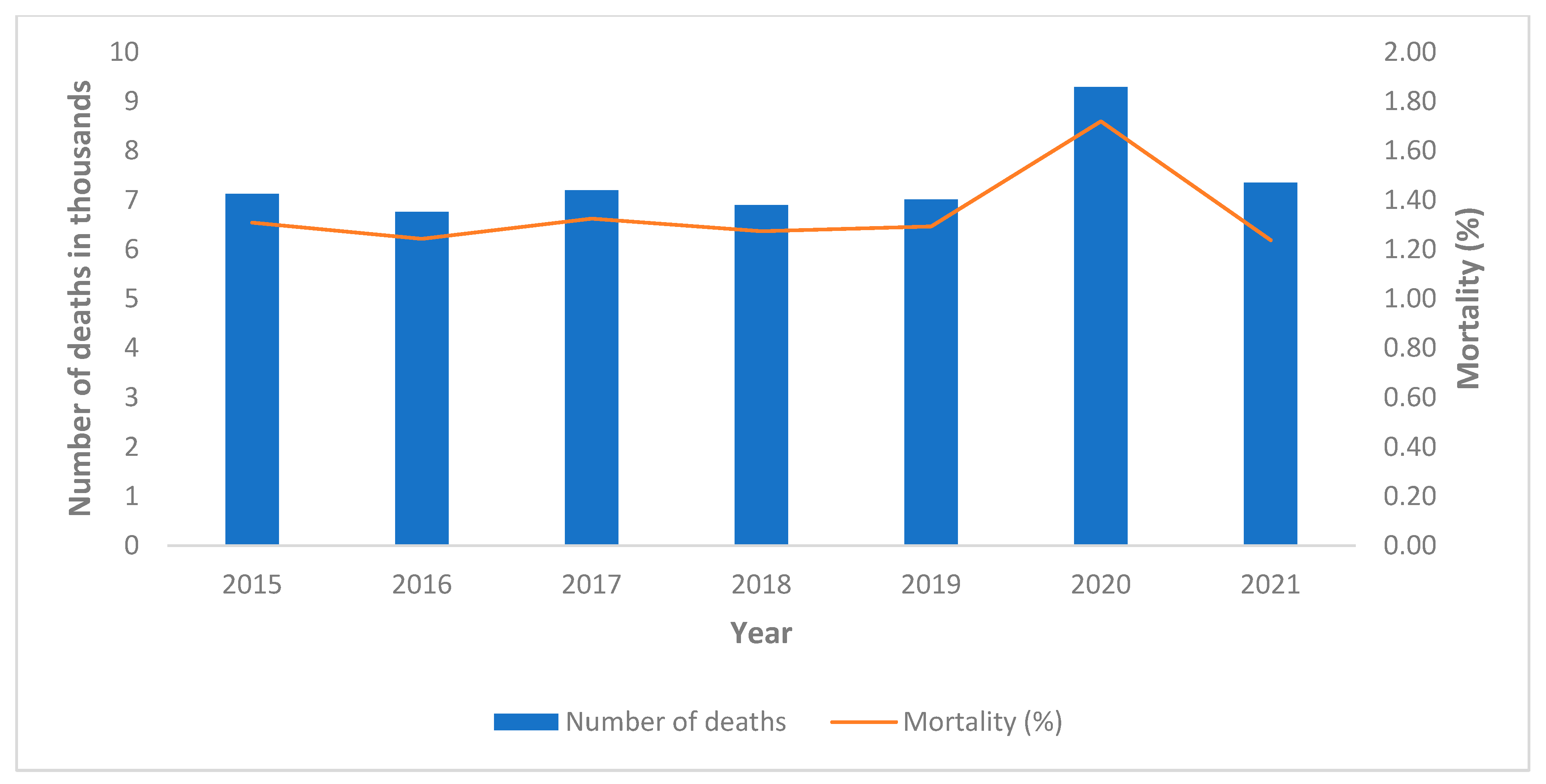
| Province of Pavia (b) | ||||||||
| Dead | 7129 | 6762 | 7196 | 6901 | 7008 | 9293 | 7352 | 6999 ± 174 |
| Population | 544,841 | 543,875 | 543,138 | 541,617 | 541,717 | 540,376 | 535,801 | 543,038 ± 1390 |
| Mortality | 1.31% | 1.24% | 1.32% | 1.27% | 1.29% | 1.72% | 1.37% | 1.29 ± 0.03% |
| Mortality variation * | 1.52% | −3.54% | 2.79% | −1.14% | 0.37% | 33.43% | 6.46% | |
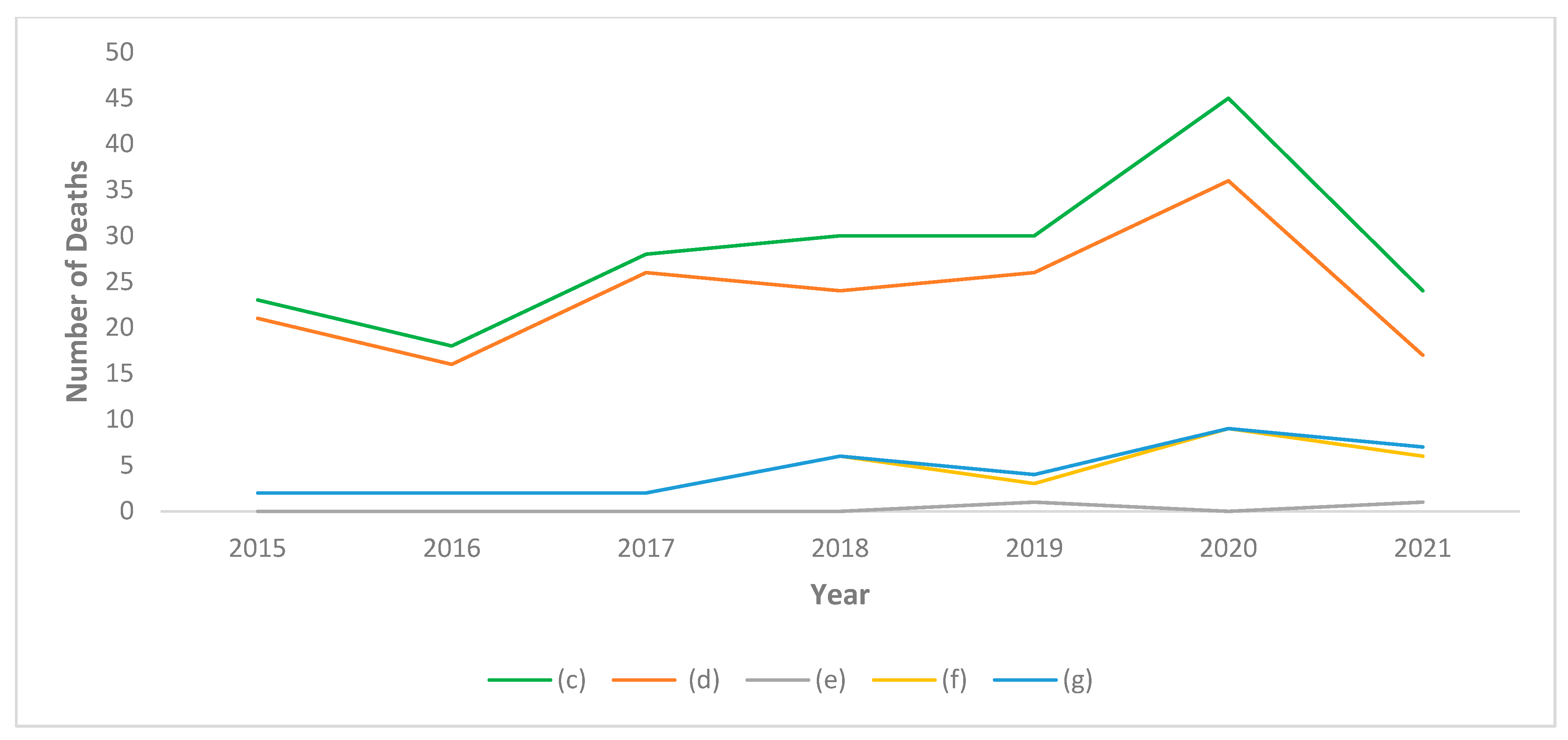
| All Doctors (c) | ||||||||
| Dead | 23 | 18 | 28 | 30 | 30 | 45 | 24 | 26 ± 5 |
| Population | 5100 | 5222 | 5282 | 5342 | 5394 | 5454 | 5529 | 5268 ± 114 |
| Mortality | 0.45% | 0.34% | 0.53% | 0.56% | 0.56% | 0.83% | 0.43% | 0.49 ± 0.09% |
| Mortality variation * | −7.72% | −29.47% | 8.47% | 14.91% | 13.80% | 68.83% | −11.18% | |
| Physicians (d) | ||||||||
| Dead | 21 | 16 | 26 | 24 | 26 | 36 | 17 | 23 ± 4 |
| Population | 4389 | 4513 | 4567 | 4622 | 4660 | 4744 | 4836 | 4550 ± 106 |
| Mortality | 0.48% | 0.35% | 0.57% | 0.52% | 0.56% | 0.76% | 0.35% | 0.50 ± 0.09% |
| Mortality variation * | −3.51% | −28.51% | 14.80% | 4.71% | 12.51% | 53.03% | −29.11% | |
| Dentists (e) | ||||||||
| Dead | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 ± 0.45 |
| Population | 254 | 261 | 276 | 289 | 308 | 304 | 313 | 278 ± 22 |
| Mortality | 0.00% | 0.00% | 0.00% | 0.00% | 0.32% | 0.00% | 0.32% | 0.06 ± 0.15% |
| Mortality variation * | −100.00% | −100.00% | −100.00% | −100.00% | 400.00% | −100.00% | 392.01% | |
| Physicians-Dentists (f) | ||||||||
| Dead | 2 | 2 | 2 | 6 | 3 | 9 | 6 | 3 ± 2 |
| Population | 457 | 448 | 439 | 431 | 426 | 406 | 380 | 440 ± 13 |
| Mortality | 0.44% | 0.45% | 0.46% | 1.39% | 0.70% | 2.22% | 1.58% | 0.69 ± 0.41% |
| Mortality variation * | −36.32% | −35.04% | −33.70% | 102.58% | 2.48% | 222.58% | 129.77% | |
| All Dentists (g) | ||||||||
| Dead | 2 | 2 | 2 | 6 | 4 | 9 | 7 | 3 ± 2 |
| Population | 711 | 709 | 715 | 720 | 734 | 710 | 693 | 718 ± 10 |
| Mortality | 0.28% | 0.28% | 0.28% | 0.83% | 0.54% | 1.27% | 1.01% | 0.44 ± 0.25% |
| Mortality variation * | −36.69% | −36.51% | −37.04% | 87.57% | 22.66% | 185.32% | 127.36% |
| 2020 | All Doctors (c) | Physicians (d) | Dentists (e) | Doctors-Dentists (f) | All Dentists (g) |
|---|---|---|---|---|---|
| Observed mortality rate | 0.83% | 0.76% | 0.00% | 2.22% | 1.23% |
| Expected mortality rate | 0.49% | 0.50% | 0.07% | 0.68% | 0.45% |
| Number of deaths expected | 27 | 24 | 0 | 3 | 3 |
| Excess of mortality | 0.34% | 0.26% | −0.07% | 1.54% | 0.78% |
| Excess of deaths | 18 | 12 | 0 | 6 | 6 |
| MR% (95% CI) | 168 (131–206) | 153 (112–193) | 0 (0–419) | 325 (207–443) | 275 (167–383) |
| Probability according to the Poisson distribution | *** | ** | N.S. | ** | ** |
| 2021 | |||||
| Observed mortality rate | 0.43% | 0.35% | 0.32% | 1.58% | 1.01% |
| Expected mortality rate | 0.49% | 0.50% | 0.07% | 0.68% | 0.45% |
| Number of deaths expected | 27 | 24 | 0 | 3 | 3 |
| Excess of mortality | −0.06% | −0.15% | 0.25% | 0.90% | 0.56% |
| Excess of deaths | −3 | −7 | 1 | 3 | 4 |
| MR (95% CI) | 89 (51–126) | 71 (31–111) | 443 (31–856) | 232 (110–353) | 227 (115–338) |
| Probability according to the Poisson distribution | N.S. | N.S. | N.S. | N.S. | * |
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|---|---|
| All Doctors (c) | 17 (0–33) | 13 (0–29) | 18 (2–34) | 19 (3–34) | 18 (3–33) | 20 (7–33) | 12 (0–26) |
| Physicians (d) | 18 (0–36) | 14 (0–32) | 20 (2–37) | 18 (1–35) | 19 (2–35) | 19 (5–33) | 10 (0–25) |
| Dentists (e) | 0 (0–122) | 0 (0–114) | 0 (0–109) | 0 (0–104) | 25 (0–123) | 0 (0–86) | 19 (0–105) |
| Physicians-Dentists (f) | 12 (0–59) | 11 (0–56) | 11 (0–56) | 30 (0–74) | 14 (0–56) | 27 (0–63) | 24 (0–63) |
| All Dentists (g) | 10 (0–55) | 9 (0–52) | 9 (0–51) | 25 (0–66) | 16 (0–54) | 23 (0–56) | 23 (0–59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupi, S.M.; Todaro, C.; Camassa, D.; Rizzo, S.; Storelli, S.; Rodriguez y Baena, R. Excess Mortality among Physicians and Dentists during COVID-19 in Italy: A Cross-Sectional Study Related to a High-Risk Territory. Healthcare 2022, 10, 1684. https://doi.org/10.3390/healthcare10091684
Lupi SM, Todaro C, Camassa D, Rizzo S, Storelli S, Rodriguez y Baena R. Excess Mortality among Physicians and Dentists during COVID-19 in Italy: A Cross-Sectional Study Related to a High-Risk Territory. Healthcare. 2022; 10(9):1684. https://doi.org/10.3390/healthcare10091684
Chicago/Turabian StyleLupi, Saturnino Marco, Claudia Todaro, Domenico Camassa, Silvana Rizzo, Stefano Storelli, and Ruggero Rodriguez y Baena. 2022. "Excess Mortality among Physicians and Dentists during COVID-19 in Italy: A Cross-Sectional Study Related to a High-Risk Territory" Healthcare 10, no. 9: 1684. https://doi.org/10.3390/healthcare10091684
APA StyleLupi, S. M., Todaro, C., Camassa, D., Rizzo, S., Storelli, S., & Rodriguez y Baena, R. (2022). Excess Mortality among Physicians and Dentists during COVID-19 in Italy: A Cross-Sectional Study Related to a High-Risk Territory. Healthcare, 10(9), 1684. https://doi.org/10.3390/healthcare10091684