
MIH and Dental Caries in Children: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , ,
, ,  , and
, and 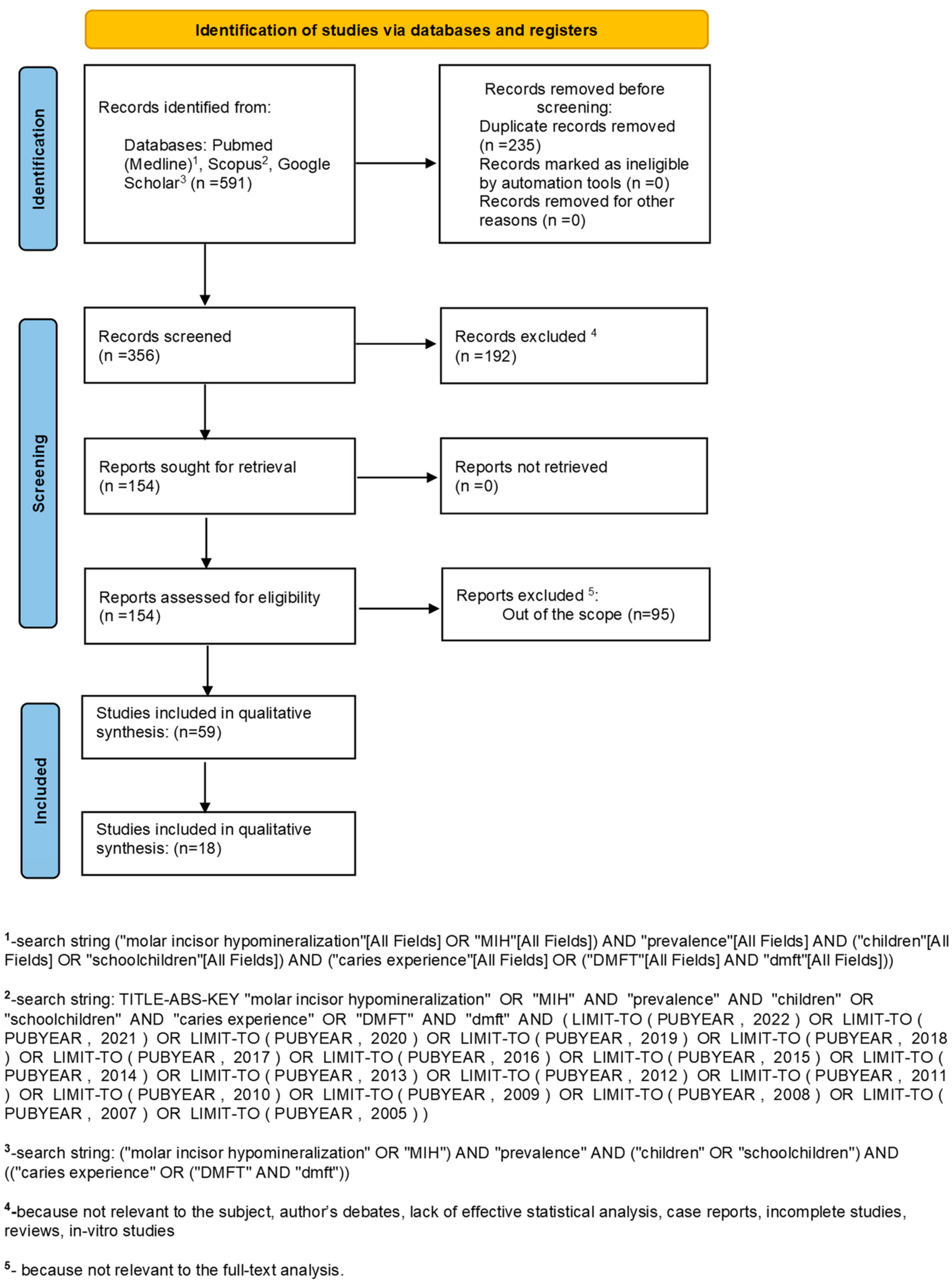{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Study Selection
2.3. Data Collection
2.4. Data Items
2.5. Quality Assessment
2.6. Risk of Bias in Individual Studies
2.7. Summary Measures and Heterogeneity
2.8. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
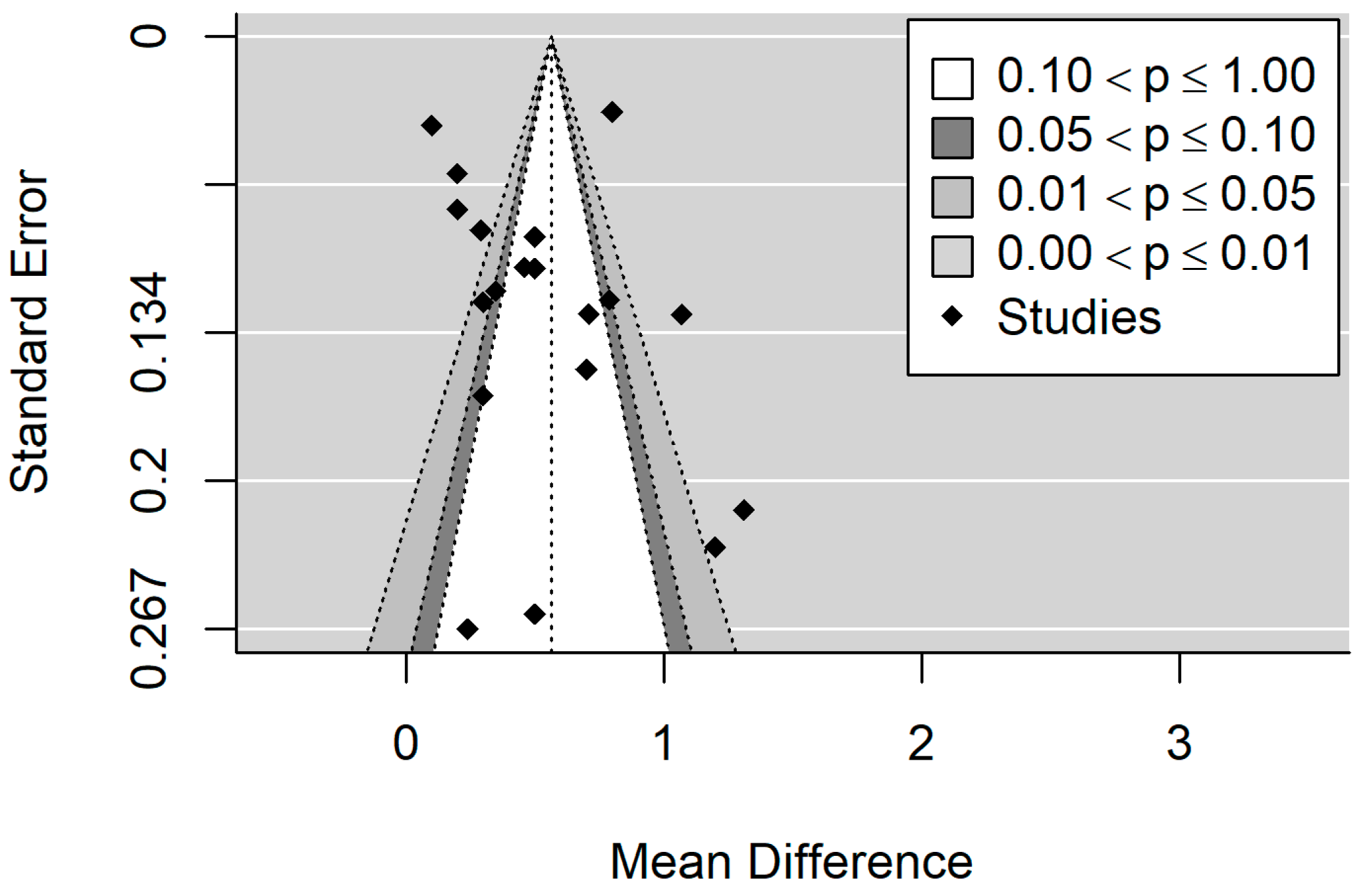
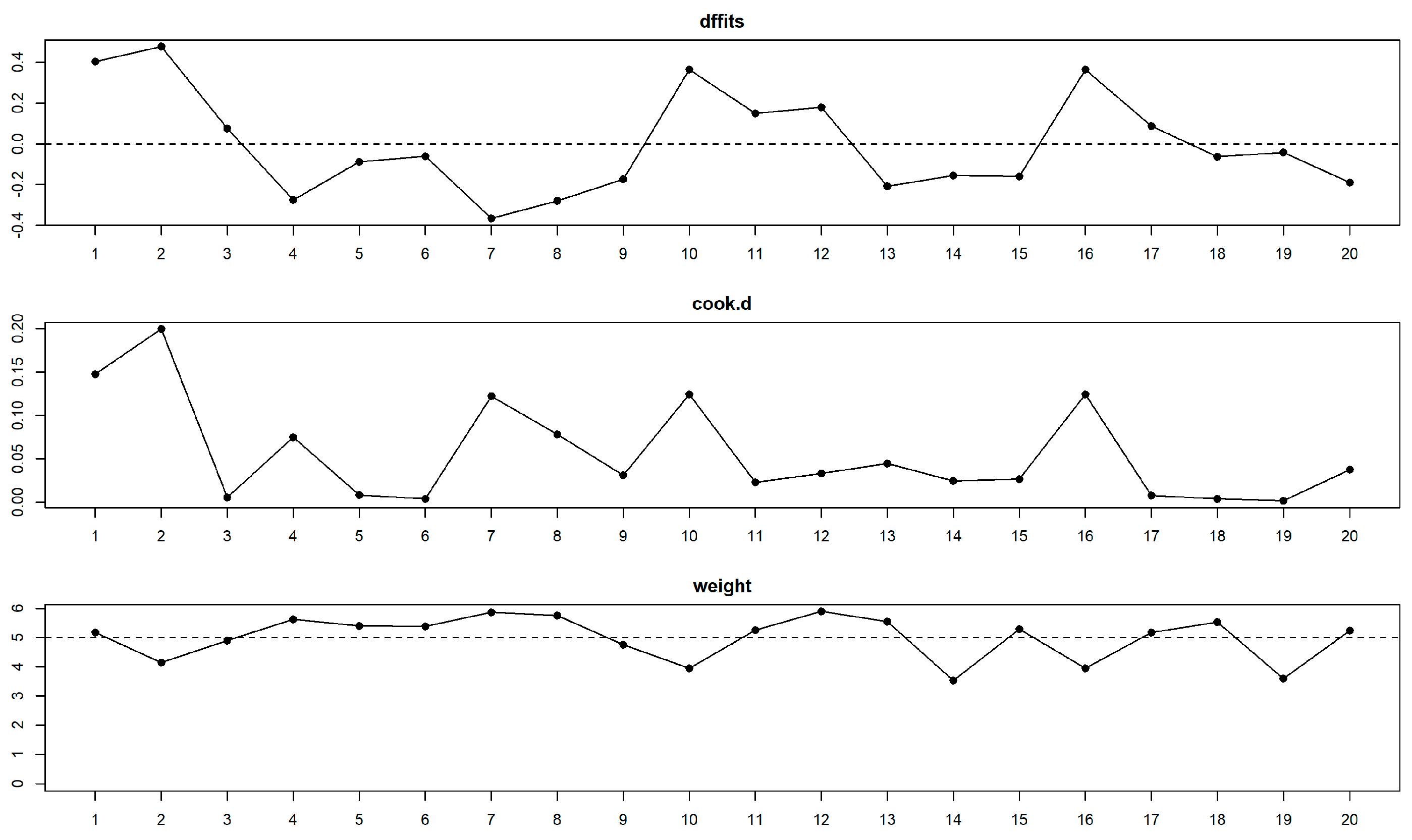
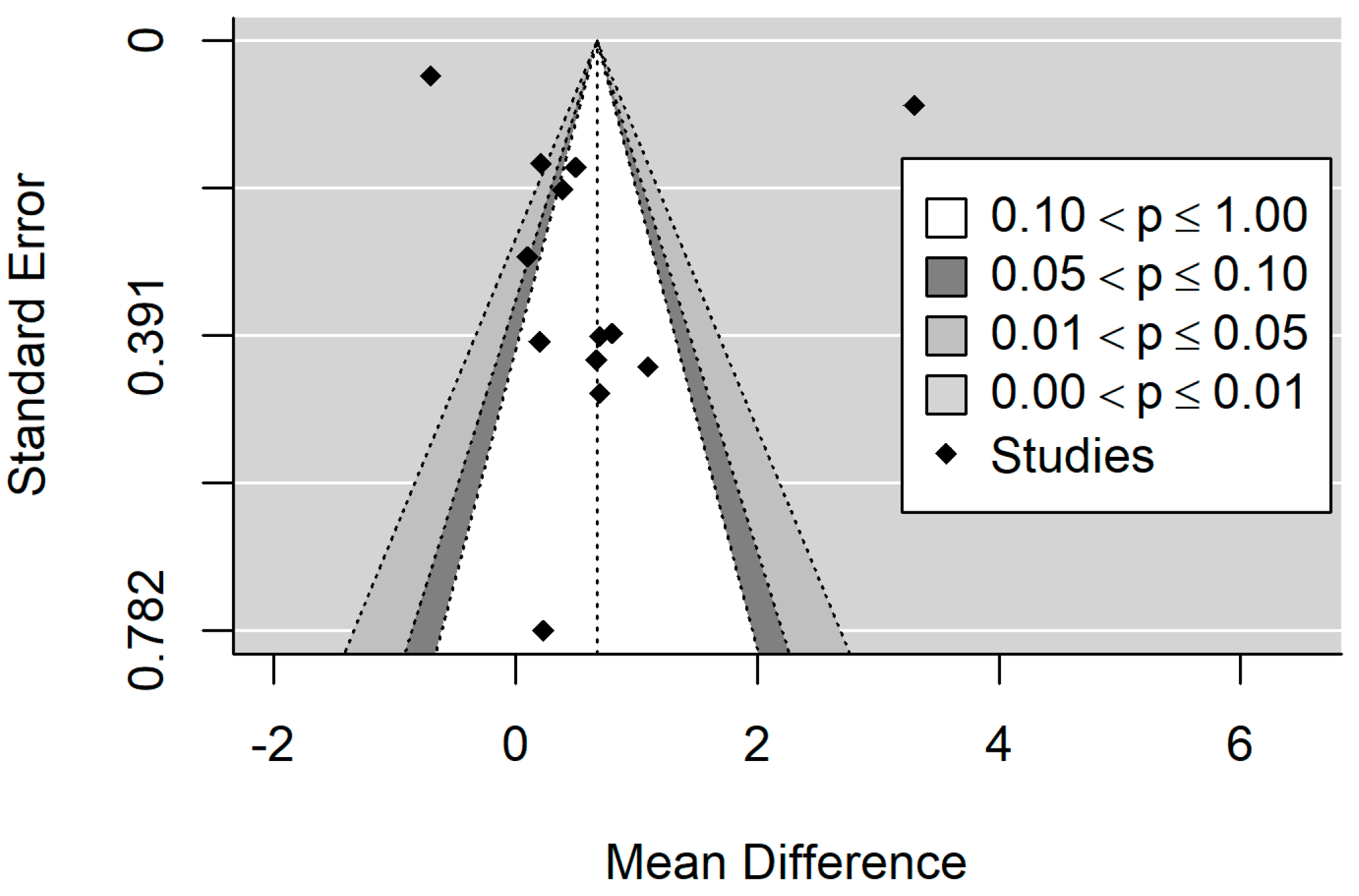
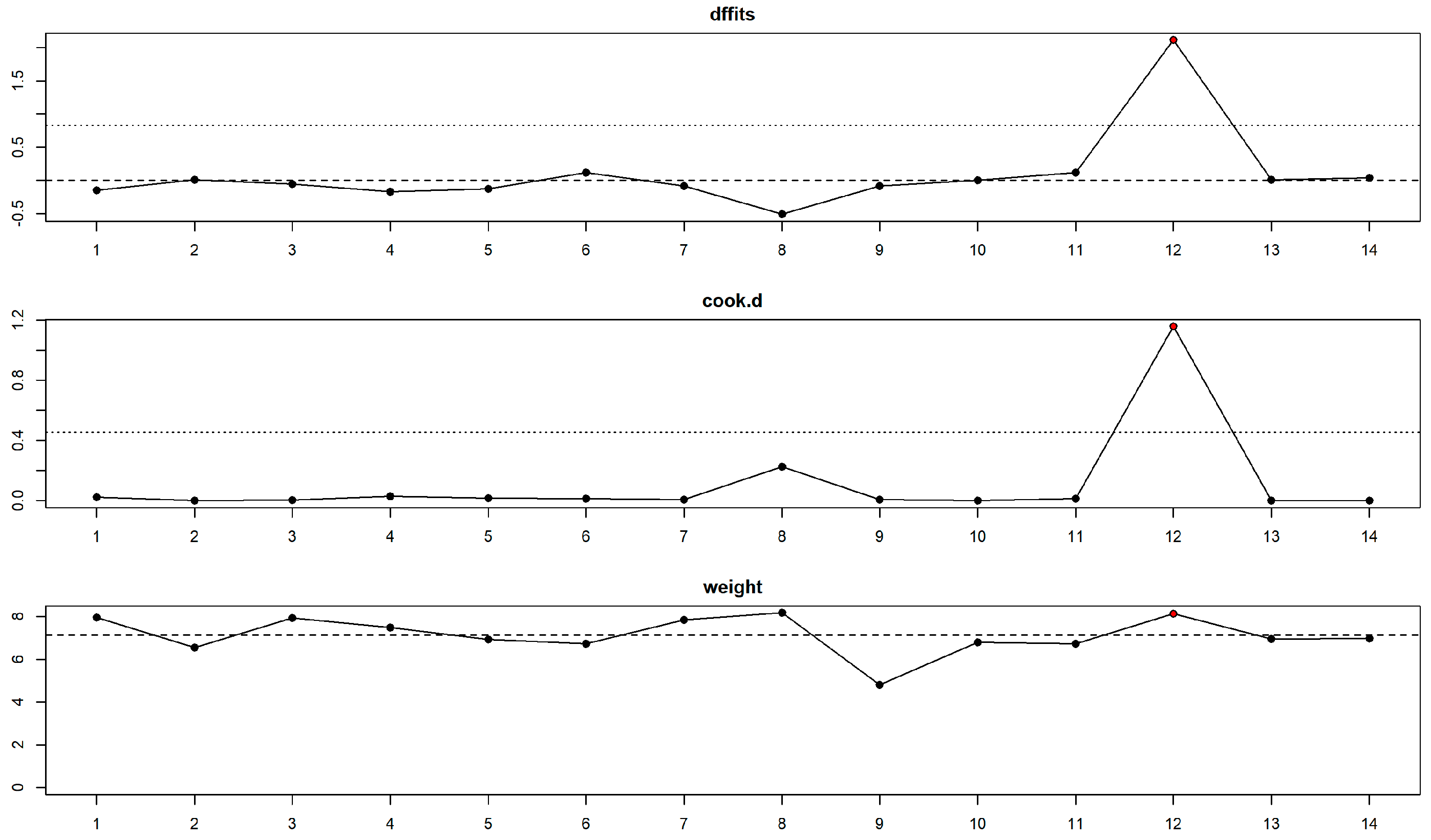
3.4. Risk of Bias Assessment
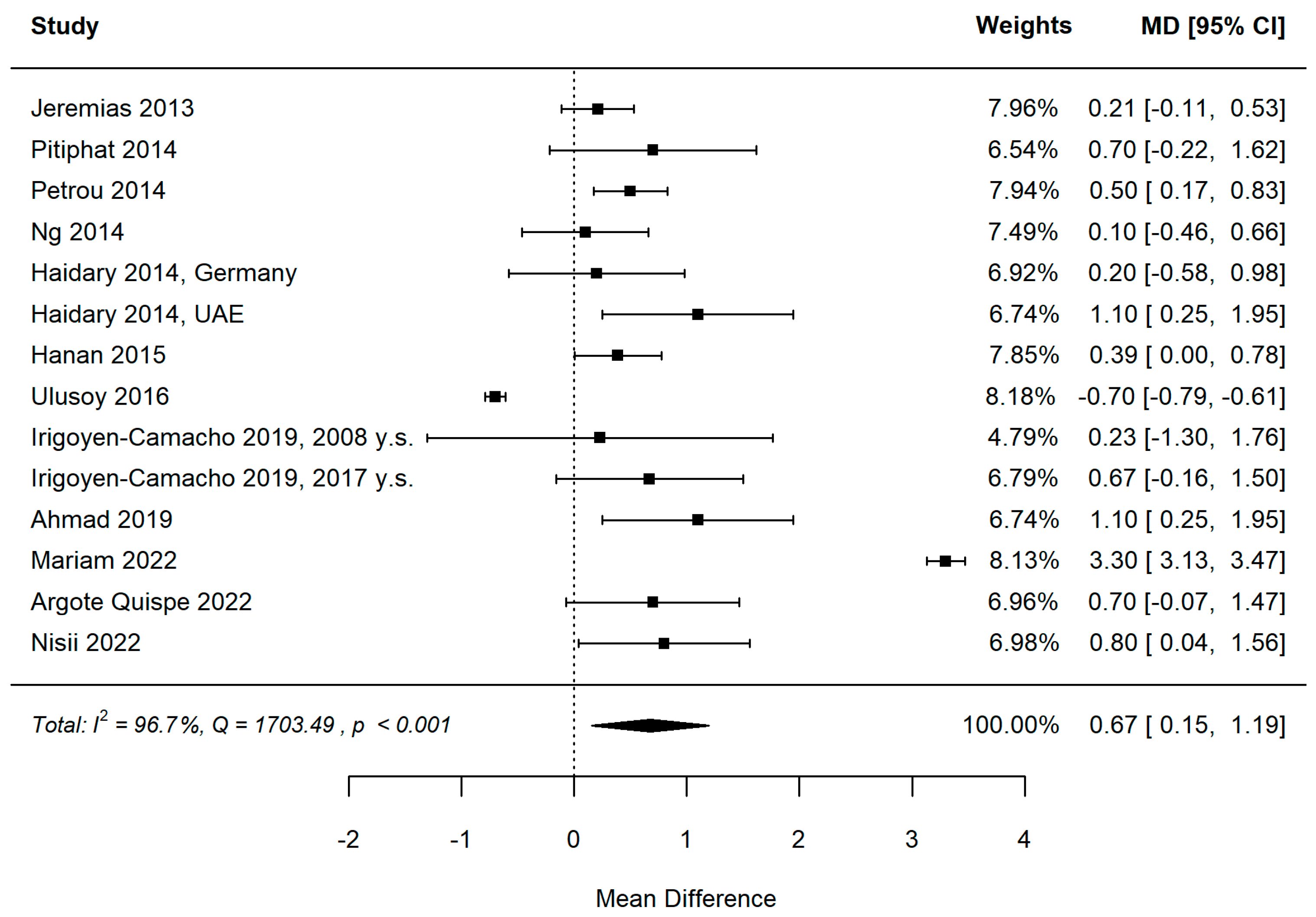
3.5. Meta-Analysis
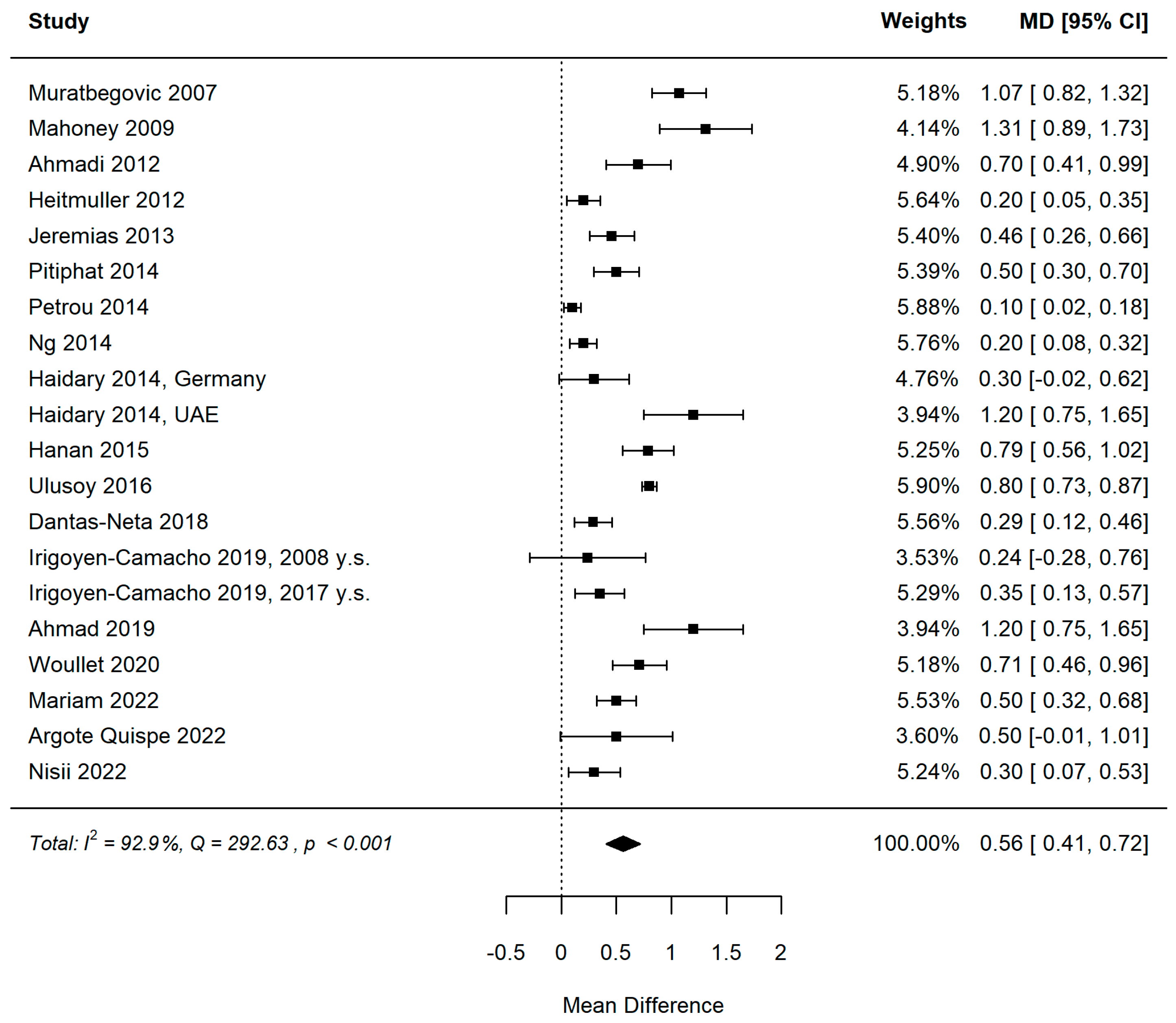
3.5.1. MIH and DMFT
3.5.2. MIH and dmft
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weerheijm, K.L. Molar incisor hypomineralisation (MIH). Eur. J. Paediatr. Dent. 2003, 4, 114–120. [Google Scholar]
- Elfrink, M.E.; Schuller, A.A.; Weerheijm, K.L.; Veerkamp, J.S. Hypomineralized second primary molars: Prevalence data in Dutch 5-year-olds. Caries Res. 2008, 42, 282–285. [Google Scholar] [CrossRef]
- Jälevik, B. Prevalence and Diagnosis of Molar-Incisor- Hypomineralisation (MIH): A systematic review. Eur. Arch. Paediatr. Dent. 2010, 11, 59–64. [Google Scholar] [CrossRef]
- Hubbard, M.J.; Mangum, J.E.; Perez, V.A.; Nervo, G.J.; Hall, R.K. Molar Hypomineralisation: A Call to Arms for Enamel Researchers. Front. Physiol. 2017, 8, 546. [Google Scholar] [CrossRef] [Green Version]
- Garot, E.; Rouas, P.; Somani, C.; Taylor, G.D.; Wong, F.; Lygidakis, N.A. An update of the aetiological factors involved in molar incisor hypomineralisation (MIH): A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2022, 23, 23–38. [Google Scholar] [CrossRef]
- Nardi, G.M.; Grassi, R.; Ndokaj, A.; Antonioni, M.; Jedlinski, M.; Rumi, G.; Grocholewicz, K.; Dus-Ilnicka, I.; Grassi, F.R.; Ottolenghi, L.; et al. Maternal and Neonatal Oral Mi-crobiome Developmental Patterns and Correlated Factors: A Systematic Review-Does the Apple Fall Close to the Tree? Int. J. Environ. Res. Public Health 2021, 18, 5569. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.; Mikulewicz, M.; Duś-Ilnicka, I. Current Concepts and Challenges in the Treatment of Cleft Lip and Palate Patients-A Comprehensive Review. J. Pers. Med. 2022, 12, 2089. [Google Scholar] [CrossRef]
- Guerra, F.; Mazur, M.; Corridore, D.; Pasqualotto, D.; Nardi, G.M.; Ottolenghi, L. Evaluation of the esthetic properties of developmental defects of enamel: A spectrophotometric clinical study. Sci. World J. 2015, 2015, 878235. [Google Scholar] [CrossRef]
- Cabral, R.N.; Nyvad, B.; Soviero, V.L.V.M.; Freitas, E.; Leal, S.C. Reliability and validity of a new classification of MIH based on severity. Clin. Oral Investig. 2020, 24, 727–734. [Google Scholar] [CrossRef]
- Schwendicke, F.; Elhennawy, K.; Reda, S.; Bekes, K.; Manton, D.J.; Krois, J. Global burden of molar incisor hypomineralization. J. Dent. 2018, 68, 10–18. [Google Scholar] [CrossRef]
- Shubha, A.B.; Hegde, S. Molar-Incisor Hypomineralization: Review of its Prevalence, Etiology, Clinical Appearance and Management. Int. J. Oral Maxillofac. Surg. 2013, 4, 26–33. [Google Scholar]
- Nisii, F.; Mazur, M.; De Nuccio, C.; Martucci, C.; Spuntarelli, M.; Labozzetta, S.; Fratini, A.; Sozzi, S.; Maruotti, A.; Vozza, I.; et al. Prevalence of molar incisor hypomineralization among school children in Rome, Italy. Sci. Rep. 2022, 12, 7343. [Google Scholar] [CrossRef]
- Condò, R.; Perugia, C.; Maturo, P.; Docimo, R. MIH: Epidemiologic clinic study in paediatric patient. Oral Implantol. 2012, 5, 58–69. [Google Scholar]
- Mazur, M.; Westland, S.; Ndokaj, A.; Nardi, G.M.; Guerra, F.; Ottolenghi, L. In-vivo colour stability of enamel after ICON® treatment at 6 years of follow-up: A prospective single center study. J. Dent. 2022, 122, 103943. [Google Scholar] [CrossRef]
- Mazur, M.; Westland, S.; Guerra, F.; Corridore, D.; Vichi, M.; Maruotti, A.; Nardi, G.M.; Ottolenghi, L. Objective and subjective aesthetic performance of icon® treatment for enamel hypomineralization lesions in young adolescents: A retrospective single center study. J. Dent. 2018, 68, 104–108. [Google Scholar] [CrossRef] [Green Version]
- Nardi, G.M.; Mazur, M.; Corridore, D.; Capocci, M.; Rinaldo, F.M.; Maruotti, A.; Ottolenghi, L.; Guerra, F. Clinical comparison between an opaque and a clear pit and fissures sealants: A 12-month split-mouth, randomized controlled study. Clin. Ther. 2018, 169, e5–e9. [Google Scholar] [CrossRef]
- Lygidakis, N.A.; Garot, E.; Somani, C.; Taylor, G.D.; Rouas, P.; Wong, F.S.L. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): An updated European Academy of Paediatric Dentistry policy document. Eur. Arch. Paediatr. Dent. 2022, 23, 3–21. [Google Scholar] [CrossRef]
- Tirlet, G.; Chabouis, H.F.; Attal, J.P. Infiltration, a new therapy for masking enamel white spots: A 19-month follow-up case series. Eur. J. Esthet. Dent. 2013, 8, 180–190. [Google Scholar]
- Elhennawy, K.; Jost-Brinkmann, P.G.; Manton, D.J.; Paris, S.; Schwendicke, F. Managing molars with severe molar-incisor hypomineralization: A cost-effectiveness analysis within German healthcare. J. Dent. 2017, 63, 65–71. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://www.cochrane-handbook.org/2011 (accessed on 13 October 2022).
- Weerheijm, K.; Mejàre, I. Molar incisor hypomineralization: A questionnaire inventory of its occurrence in member countries of the European Academy of Paediatric Dentistry (EAPD). Int. J. Paediatr. Dent. 2003, 13, 411–416. [Google Scholar] [CrossRef]
- Ghanim, A.; Elfrink, M.; Weerheijm, K.; Mariño, R.; Manton, D. A practical method for use in epidemiological studies on enamel hypomineralisation. Eur. Arch. Paediatr. Dent. 2015, 16, 235–246. [Google Scholar] [CrossRef] [Green Version]
- La Torre, G.; Calzoni, L.; Colamesta, V.; Guzzo, A.S.; Mafongelli, E.; Mannocci, A.; Meggiolaro, A.; Mipatrini, D.; Pagano, L.; Saulle, R. Management Sanitario, Un Approccio Metodologico; Società Editrice Universo: Rome, Italy, 2014; p. 200. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.; Schneider, M.; Minder, C.H. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Del Re, A.C. A Practical Tutorial on Conducting Meta-Analysis in R. Quant. Meth. Psych. 2015, 11, 37–50. [Google Scholar] [CrossRef] [Green Version]
- Muratbegovic, A.; Markovic, N.; Ganibegovic Selimovic, M. Molar incisor hypomineralisation in Bosnia and Herzegovina: Aetiology and clinical consequences in medium caries activity population. Eur. Arch. Paediatr. Dent. 2007, 8, 189–194. [Google Scholar] [CrossRef]
- Mahoney, E.K.; Morrison, D.G. The prevalence of Molar-Incisor Hypomineralisation (MIH) in Wainuiomata children. N. Z. Dent. J. 2009, 105, 121–127. [Google Scholar]
- Ahmadi, R.; Ramazani, N.; Nourinasab, R. Molar incisor hypomineralization: A study of prevalence and etiology in a group of Iranian children. Iran J. Pediatr. 2012, 22, 245–251. [Google Scholar]
- Heitmüller, D.; Thiering, E.; Hoffmann, U.; Heinrich, J.; Manton, D.; Kühnisch, J.; Neumann, C.; Bauer, C.P.; Heinrich-Weltzien, R.; Hickel, R. GINIplus Study Group. Is there a positive relationship between molar incisor hypomineralisations and the presence of dental caries? Int. J. Paediatr. Dent. 2013, 23, 116–124. [Google Scholar] [CrossRef]
- Jeremias, F.; Souza, J.F.D.; Costa Silva, C.M.D.; Cordeiro, R.D.C.L.; Zuanon, Â.C.C.; Santos-Pinto, L. Dental caries experience and molar-incisor hypomineralization. Acta Odontol. Scand. 2013, 71, 870–876. [Google Scholar] [CrossRef]
- Pitiphat, W.; Savisit, R.; Chansamak, N.; Subarnbhesaj, A. Molar incisor hypomineralization and dental caries in six- to seven-year-old Thai children. Pediatr. Dent. 2014, 36, 478–482. [Google Scholar]
- Petrou, M.A.; Giraki, M.; Bissar, A.R.; Basner, R.; Wempe, C.; Altarabulsi, M.B.; Schäfer, M.; Schiffner, U.; Beikler, T.; Schulte, A.G.; et al. Prevalence of Molar-Incisor-Hypomineralisation among school children in four German cities. Int. J. Paediatr. Dent. 2014, 24, 434–440. [Google Scholar] [CrossRef]
- Ng, J.J.; Eu, O.C.; Nair, R.; Hong, C.H. Prevalence of molar incisor hypomineralization (MIH) in Singaporean children. Int. J. Paediatr. Dent. 2015, 25, 73–78. [Google Scholar] [CrossRef]
- Haidary, S. Comparison of the Prevalence of Molar Incisor Hypomineralization in Dubai/United Arab Emirate and Greifswald/Germany. Ph.D. Thesis, Universitätsbibliothek Greifswald, Greifswald, Germany, 2015. [Google Scholar]
- Hanan, S.A.; de Oliveira Alves Filho, A.; Medina, P.O.; Cordeiro, R.D.C.L.; Santos-Pinto, L.; Zuanon, Â.C.C. Molar-incisor hypomineralization in schoolchildren of Manaus, Brazil. Pesqui. Bras. Odontopediatr. Clin. Integr. 2015, 15, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Ulusoy, A.T.; Sen Tunc, E.; Bayrak, Ş.; Onder, H. A Comparative Study of Oral Health Parameters in Molar Incisor Hypomineralization and High-Caries-Risk Children Aged 8-11 Years. Med. Princ. Pract. 2016, 25, 85–89. [Google Scholar] [CrossRef]
- Dantas-Neta, N.B.; Soares Figueiredo, M.; Lima, C.C.B.; Bendo, C.B.; Matos de Andrade, É.M.; Lima, M.D.M.; Pordeus, I.A.; Paiva, S.M. Factors associated with molar-incisor hypomineralisation in schoolchildren aged 8–10 years: A case-control study. Int. J. Paediatr. Dent. 2018, 28, 570–577. [Google Scholar] [CrossRef]
- Irigoyen-Camacho, M.E.; Villanueva-Gutierrez, T.; Castano-Seiquer, A.; Molina-Frechero, N.; Zepeda-Zepeda, M.; Sánchez-Pérez, L. Evaluating the changes in molar incisor hypomineralization prevalence: A comparison of two cross-sectional studies in two elementary schools in Mexico City between 2008 and 2017. Clin. Exp. Dent. Res. 2020, 6, 82–89. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.H.; Petrou, M.A.; Alhumrani, A.; Hashim, R.; Splieth, C. Prevalence of Molar-Incisor Hypomineralisation in an Emerging Community, and a Possible Correlation with Caries, Fluorosis and Socioeconomic Status. Oral Health Prev. Dent. 2019, 17, 323–327. [Google Scholar] [CrossRef]
- Wuollet, E. Molar-Incisor Hypomineralization: Observations from Groups of Finnish Children and a Treatment Practice Survey among Finnish Dentists. Ph.D. Thesis, University of Helsinki, Helsinki, Finland, 2020. [Google Scholar]
- Mariam, S.; Goyal, A.; Dhareula, A.; Gauba, K.; Bhatia, S.K.; Kapur, A. A case-controlled investigation of risk factors associated with molar incisor hypomineralization (MIH) in 8-12 year-old children living in Chandigarh, India. Eur. Arch. Paediatr. Dent. 2022, 23, 97–107. [Google Scholar] [CrossRef]
- Argote Quispe, D.M.; De Priego, G.P.M.; Leon Manco, R.A.; Portaro, C.P. Molar incisor hypomineralization: Prevalence and severity in schoolchildren of Puno, Peru. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 246–250. [Google Scholar] [CrossRef]
- Dietrich, G.; Sperling, S.; Hetzer, G. Molar incisor hypomineralisation in a group of children and adolescents living in Dresden (Germany). Eur. J. Paediatr. Dent. 2003, 4, 133–137. [Google Scholar]
- Fteita, D.; Ali, A.; Alaluusua, S. Molar-incisor hypomineralization (MIH) in a group of school-aged children in Benghazi, Libya. Eur. Arch. Paediatr. Dent. 2006, 7, 92–95. [Google Scholar] [CrossRef]
- Jasulaityte, L.; Veerkamp, J.S.; Weerheijm, K.L. Molar incisor hypomineralization: Review and prevalence data from the study of primary school children in Kaunas/Lithuania. Eur. Arch. Paediatr. Dent. 2007, 8, 87–94. [Google Scholar] [CrossRef]
- Cho, S.Y.; Ki, Y.; Chu, V. Molar incisor hypomineralization in Hong Kong Chinese children. Int. J. Paediatr.Dent. 2008, 18, 348–352. [Google Scholar] [CrossRef]
- Kemoli, A.M. Prevalence of molar incisor hypomineralisation in six to eight year-olds in two rural divisions in Kenya. East Afr. Med. J. 2008, 85, 514–519. [Google Scholar] [CrossRef]
- Kukleva, M.P.; Petrova, S.G.; Kondeva, V.K.; Nihtyanova, T.I. Molar incisor hypomineralisation in 7-to-14-year old children in Plovdiv, Bulgaria—An epidemiologic study. Folia Med. 2008, 50, 71–75. [Google Scholar]
- Lygidakis, N.A.; Dimou, G.; Briseniou, E. Molar-incisor-hypomineralisation (MIH). Retrospective clinical study in Greek children. I. Prevalence and defect characteristics. Eur. Arch. Paediatr. Dent. 2008, 9, 200–206. [Google Scholar] [CrossRef]
- Shin, J.H.; An, U.J.; Kim, S.; Jeong, T.S. The prevalence of molar incisor hypomineralization and status of first molars in primary school children. J. Korean Acad. Pediatr. Dent. 2010, 37, 179–185. [Google Scholar]
- da Costa-Silva, C.M.; Jeremias, F.; de Souza, J.F.; Cordeiro, R.C.; Santos-Pinto, L.; Zuanon, A.C. Molar incisor hypomineralization: Prevalence, severity and clinical consequences in Brazilian children. Int. J. Paediatr. Dent. 2010, 20, 426–434. [Google Scholar] [CrossRef]
- Ghanim, A.; Morgan, M.; Mariño, R.; Bailey, D.; Manton, D. Molar-incisor hypomineralisation: Prevalence and defect characteristics in Iraqi children. Int. J. Paediatr. Dent. 2011, 21, 413–421. [Google Scholar] [CrossRef]
- Păsăreanu, M.; Mocanu, R.M.; Bălan, A. The syndrome MIH systemic impact in children and adolescents: Relevance area. Rom. J. Oral Rehabil. 2012, 4, 82–89. [Google Scholar]
- Parikh, D.R.; Ganesh, M.; Bhaskar, V. Prevalence and characteristics of Molar Incisor Hypomineralisation (MIH) in the child population residing in Gandhinagar, Gujarat, India. Eur. Arch. Paediatr. Dent. 2012, 13, 21–26. [Google Scholar] [CrossRef]
- Sönmez, H.; Yıldırım, G.; Bezgin, T. Putative factors associated with molar incisor hypomineralisation: An epidemiological study. Eur. Arch. Paediatr. Dent. 2013, 14, 375–380. [Google Scholar] [CrossRef]
- Shrestha, R.; Upadhaya, S.; Bajracharya, M. Prevalence of molar incisor hypomineralisation among school children in Kavre. Kathmandu Univ. Med. J. 2014, 12, 38–42. [Google Scholar] [CrossRef] [Green Version]
- López Jordi Mdel, C.; Cortese, S.G.; Álvarez, L.; Salveraglio, I.; Ortolani, A.M.; Biondi, A.M. Comparison of the prevalence of molar incisor hypomineralization among children with different health care coverage in the cities of Buenos Aires (Argentina) and Montevideo (Uruguay). Salud. Colect. 2014, 10, 243–251. [Google Scholar] [CrossRef]
- Garcia-Margarit, M.; Catalá-Pizarro, M.; Montiel-Company, J.M.; Almerich-Silla, J.M. Epidemiologic study of molar-incisor hypomineralization in 8-year-old Spanish children. Int. J. Paediatr. Dent. 2014, 24, 14–22. [Google Scholar] [CrossRef]
- Mittal, N.P.; Goyal, A.; Gauba, K.; Kapur, A. Molar incisor hypomineralisation: Prevalence and clinical presentation in school children of the northern region of India. Eur. Arch. Paediatr Dent. 2014, 15, 11–18. [Google Scholar] [CrossRef]
- Oyedele, T.A.; Folayan, M.O.; Adekoya-Sofowora, C.A.; Oziegbe, E.O.; Esan, T.A. Prevalence, pattern and severity of molar incisor hypomineralisation in 8- to 10-year-old school children in Ile-Ife, Nigeria. Eur. Arch. Paediatr. Dent. 2015, 16, 277–282. [Google Scholar] [CrossRef]
- Krishnan, R.; Ramesh, M.; Chalakkal, P. Prevalence and characteristics of MIH in school children residing in an endemic fluorosis area of India: An epidemiological study. Eur. Arch. Paediatr. Dent. 2015, 16, 455–460. [Google Scholar] [CrossRef]
- Ofi, W.A.; Salih, B.A. Prevalence and severity of molar-incisor hypomineralisation with relation to its etiological factors among school children 7-9 years of Al-Najaf governorate. J. Baghdad Coll. Dent. 2015, 27, 169–173. [Google Scholar] [CrossRef]
- Kirthiga, M.; Poornima, P.; Praveen, R.; Gayathri, P.; Manju, M.; Priya, M. Prevalence and severity of molar incisor hypomineralization in children aged 11-16 years of a city in Karnataka, Davangere. J. Indian Soc. Pedod. Prev. Dent. 2015, 33, 213–217. [Google Scholar] [CrossRef]
- Yannam, S.D.; Amarlal, D.; Rekha, C.V. Prevalence of molar incisor hypomineralization in school children aged 8-12 years in Chennai. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 134–138. [Google Scholar] [CrossRef]
- Garot, E.; Manton, D.; Rouas, P. Peripartum events and molar-incisor hypomineralisation (MIH) amongst young patients in southwest France. Eur. Arch. Paediatr. Dent. 2016, 17, 245–250. [Google Scholar] [CrossRef]
- Siddaiah, S.H.B.; Thimmegowda, U.; Parameshwara, P.M.; Ramachandra, J.A. Molar Incisor Hypomineralization: A study of prevalence and etiology in a group of south Bangalore children. Int. J. Curr. Res. 2016, 8, 43784–43788. [Google Scholar]
- Ullah, I.; Parveen, N.; Shabbir, R. Pattern and Presentation of Molar Incisor Hypomineralizaion in Pakistani Children. Int. J. Contemp. Med. Res. 2016, 3, 724–726. [Google Scholar]
- Teixeira, R.J.P.B.; Andrade, N.S.; Queiroz, L.C.C.; Mendes, F.M.; Moura, M.S.; Moura, L.F.A.D.; Lima, M.D.M. Exploring the association between genetic and environmental factors and molar incisor hypomineralization: Evidence from a twin study. Int. J. Paediatr. Dent. 2018, 28, 198–206. [Google Scholar] [CrossRef]
- Gambetta-Tessini, K.; Mariño, R.; Ghanim, A.; Calache, H.; Manton, D.J. Carious lesion severity and demarcated hypomineralized lesions of tooth enamel in schoolchildren from Melbourne, Australia. Austral. Dent. J. 2018, 63, 365–373. [Google Scholar] [CrossRef]
- Rai, A.; Singh, A.; Menon, I.; Singh, J.; Rai, V.; Aswal, G.S. Molar Incisor Hypomineralization: Prevalence and Risk Factors Among 7–9 Years Old School Children in Muradnagar, Ghaziabad. Open Dent. J. 2018, 28, 714–722. [Google Scholar] [CrossRef]
- Al-Hammad, N.S.; Al-Dhubaiban, M.; Alhowaish, L.; Bello, L.L. Prevalence and clinical characteristics of molar-incisor-hypomineralization in school children in Riyadh, Saudi Arabia. Int. J. Med. Sci. Clin. Invent. 2018, 5, 3570–3576. [Google Scholar] [CrossRef]
- Santos, P.S.; Martins-Júnior, P.A.; Paiva, S.M.; Klein, D.; Torres, F.M.; Giacomin, A.; Cardoso, M. Prevalence of self-reported dental pain and associated factors among eight-to ten-year-old Brazilian schoolchildren. PLoS ONE 2019, 14, e0214990. [Google Scholar] [CrossRef]
- Davenport, M.; Welles, A.D.; Angelopoulou, M.V.; Gonzalez, C.; Okunseri, C.; Barbeau, L.; Bansal, N.K.; Vergotine, R.J.; Hodgson, B.D. Prevalence of molar-incisor hypomineralization in Milwaukee, Wisconsin, USA: A pilot study. Clin. Cosmet. Investig. Dent. 2019, 30, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Datana, S. Molar Incisor Hypomineralisation (MIH): Estimating prevalence and characteristics among children of Pune, Maharashtra. IJDRR 2019, 10, 28933. [Google Scholar]
- Gutiérrez, T.V.; Ortega, C.C.B.; Pérez, N.P.; Pérez, A.G. Impact of Molar Incisor Hypomineralization on Oral Health-Related Quality of Life in Mexican Schoolchildren. J. Clin. Pediatr. Dent. 2019, 43, 324–330. [Google Scholar] [CrossRef]
- Menoncin, B.L.V.; Portella, P.D.; Ramos, B.L.M.; da Silva Assunção, L.R.; de Souza, J.F.; Menezes, J.V.N.B. Dental anxiety in schoolchildren with molar incisor hypomineralization—A population-based cross-sectional study. Int. J. Paediatr. Dent. 2019, 29, 615–623. [Google Scholar] [CrossRef]
- Zafar, R.; Urooj, A.; Masood, S. Frequency of Molar Incisor Hypomineralization and Associated Risk Factors—A Study from Southern Punjab. Pak. Biomed. 2020, 36, 291. [Google Scholar] [CrossRef]
- Jurlina, D.; Uzarevic, Z.; Ivanisevic, Z.; Matijevic, N.; Matijevic, M. Prevalence of Molar–Incisor Hypomineralization and Caries in Eight-Year-Old Children in Croatia. Int. J. Environ. Res. Public Health 2020, 17, 6358. [Google Scholar] [CrossRef]
- Fragelli, C.; Barbosa, T.S.; Bussaneli, D.G.; Restrepo, M.; Cordeiro, R.C.L.; Santos-Pinto, L. Aesthetic perception in children with molar incisor hypomineralization. Eur. Arch. Paediatr. Dent. 2021, 22, 227–234. [Google Scholar] [CrossRef]
- Khazaei, Y.; Harris, C.P.; Heinrich, J.; Standl, M.; Kühnisch, J. Association Study on Nutrition in the First Year of Life and Molar-Incisor Hypomineralization (MIH)-Results from the GINIplus and LISA Birth Cohort Studies. Int. J. Environ. Res. Public Health 2021, 18, 11411. [Google Scholar] [CrossRef]
- Brzovic Rajic, V.; Modric, V.E.; Ivanisevic Malcic, A.; Gorseta, K.; Karlovic, Z.; Verzak, Z. Molar Incisor Hypomineralization in Children with Intellectual Disabilities. Dent. J. 2021, 9, 21. [Google Scholar] [CrossRef]
- Vanhée, T.; Poncelet, J.; Cheikh-Ali, S.; Bottenberg, P. Prevalence, Caries, Dental Anxiety and Quality of Life in Children with MIH in Brussels, Belgium. J. Clin. Med. 2022, 11, 3065. [Google Scholar] [CrossRef]
- Altner, S.; Ebel, M.; Ritschl, V.; Stamm, T.; Hirsch, C.; Bekes, K. Treatment of Severe Caries and Molar Incisor Hypomineralization and Its Influence on Oral Health-Related Quality of Life in Children: A Comparative Study. Int. J. Environ. Res. Public Health 2022, 19, 2983. [Google Scholar] [CrossRef]
- Lago, D.J.; Restrepo, M.; Bussaneli, G.D.; Cavalheiro, P.J.; de Souza, P.J.; Pinto, S.L.; de Cássia, L.C.R.; Jeremias, F. Molar-Incisor Hypomineralization: Prevalence Comparative Study in 6 Years of Interval. Sci. World J. 2022, 2022, 4743252. [Google Scholar] [CrossRef]
- Salem, M.B.; Chouchene, F.; Masmoudi, F.; Baaziz, A.; Maatouk, F.; Ghedira, H. Are Molar-Incisor Hypomineralization and Hypomineralized Second Primary Molars Predictive of Dental Caries? A Systematic Review. Eur. J. Dent. 2022, 17, 7–15. [Google Scholar] [CrossRef]
- Ghanim, A.; Silva, M.J.; Elfrink, M.E.C.; Lygidakis, N.A.; Mariño, R.J.; Weerheijm, K.L.; Manton, D.J. Molar incisor hypomineralisation (MIH) training manual for clinical field surveys and practice. Eur. Arch. Paediatr. Dent. 2017, 18, 225–242. [Google Scholar] [CrossRef]
- Hobdell, M.; Petersen, P.E.; Clarkson, J.; Johnson, N. Global goals for oral health 2020. Int. Dent. J. 2003, 53, 285–288. [Google Scholar] [CrossRef]
- Chen, K.J.; Gao, S.S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Prevalence of early childhood caries among 5-year-old children: A systematic review. J. Investig. Clin. Dent. 2019, 10, e12376. [Google Scholar] [CrossRef] [Green Version]
- Oral Health Country/Area Profile Project. Available online: https://capp.mau.se/dental-caries/ (accessed on 7 January 2023).
- Bencze, Z.; Kovalecz, G.; Márton, S.; Gáll, T.; Mahrouseh, N.; Varga, O. Childhood caries management in the European Union: A cross-sectional study. Heliyon. 2021, 7, e06198. [Google Scholar] [CrossRef]
- Calderara, P.C.; Gerthoux, P.M.; Mocarelli, P.; Lukinmaa, P.L.; Tramacere, P.L.; Alaluusua, S. The prevalence of Molar Incisor Hypomineralisation (MIH) in a group of Italian school children. Eur. J. Paediatr. Dent. 2005, 6, 79–83. [Google Scholar]
- Almuallem, Z.; Busuttil-Naudi, A. Molar incisor hypomineralisation (MIH)—An over-view. Br. Dent. J. 2018, 225, 601–609. [Google Scholar] [CrossRef] [Green Version]
- Elhennawy, K.; Schwendicke, F. Managing molar-incisor hypomineralization: A systematic review. J. Dent. 2016, 55, 16–24. [Google Scholar] [CrossRef]
- Joshi, T.; Rahman, A.; Rienhoff, S.; Rienhoff, J.; Stamm, T.; Bekes, K. Impact of molar incisor hypomineralization on oral health-related quality of life in 8–10-year-old children. Clin. Oral Investig. 2022, 26, 1753–1759. [Google Scholar] [CrossRef]
- Turkmen, E.; Ozukoc, C. Impact of molar incisor hypomineralization on oral hygiene and gingival health in 8-15-years-old children. Aust. Dent. J. 2022, 67, S50–S56. [Google Scholar] [CrossRef]
- Raposo, F.; de Carvalho Rodrigues, A.C.; Lia, É.N.; Leal, S.C. Prevalence of Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralization (MIH). Caries Res. 2019, 53, 424–430. [Google Scholar] [CrossRef]
- Americano, G.C.; Jacobsen, P.E.; Soviero, V.M.; Haubek, D. A systematic review on the association between molar incisor hypomineralization and dental caries. Int. J. Paediatr. Dent. 2017, 27, 11–21. [Google Scholar] [CrossRef]
- Grossi, J.A.; Cabral, R.N.; Leal, S.C. Caries Experience in Children with and without Molar-Incisor Hypomineralisation: A Case-Control Study. Caries Res. 2017, 51, 419–424. [Google Scholar] [CrossRef]
- Neves, A.B.; Americano, G.C.A.; Soares, D.V.; Soviero, V.M. Breakdown of demarcated opacities related to molar-incisor hypomineralization: A longitudinal study. Clin. Oral Investig. 2019, 23, 611–615. [Google Scholar] [CrossRef]
- Mazur, M.; Ndokaj, A.; Bietolini, S.; Nisii, V.; Duś-Ilnicka, I.; Ottolenghi, L. Green dentistry: Organic toothpaste formulations. A literature review. Dent. Med. Probl. 2022, 59, 461–474. [Google Scholar] [CrossRef]
- Frencken, J.E.; Peters, M.C.; Manton, D.J.; Leal, S.C.; Gordan, V.V.; Eden, E. Minimal inter-vention dentistry for managing dental caries—A review: Report of a FDI task group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [Green Version]
- Linner, T.; Khazaei, Y.; Bücher, K.; Pfisterer, J.; Hickel, R.; Kühnisch, J. Comparison of four different treatment strategies in teeth with molar-incisor hypomineralization-related enamel breakdown-A retrospective cohort study. Int. J. Paediatr. Dent. 2020, 30, 597–606. [Google Scholar] [CrossRef]
- Tahmasebi, E.; Mohammadi, M.; Alam, M.; Abbasi, K.; Gharibian Bajestani, S.; Khanmo-hammad, R.; Haseli, M.; Yazdanian, M.; Barzegar, P.E.F.; Tebyaniyan, H. The current regenerative medicine approaches of craniofacial diseases: A narrative review. Front. Cell Dev. Biol. 2023, 11, 1112378. [Google Scholar] [CrossRef]
- Larmas, M.; Sándor, G.K. Enzymes, dentinogenesis and dental caries: A literature review. J. Oral Maxillofac. Res. 2014, 5, e3. [Google Scholar] [CrossRef] [Green Version]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazur, M.; Corridore, D.; Ndokaj, A.; Ardan, R.; Vozza, I.; Babajko, S.; Jedeon, K. MIH and Dental Caries in Children: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 1795. https://doi.org/10.3390/healthcare11121795
Mazur M, Corridore D, Ndokaj A, Ardan R, Vozza I, Babajko S, Jedeon K. MIH and Dental Caries in Children: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(12):1795. https://doi.org/10.3390/healthcare11121795
Chicago/Turabian StyleMazur, Marta, Denise Corridore, Artnora Ndokaj, Roman Ardan, Iole Vozza, Sylvie Babajko, and Katia Jedeon. 2023. "MIH and Dental Caries in Children: A Systematic Review and Meta-Analysis" Healthcare 11, no. 12: 1795. https://doi.org/10.3390/healthcare11121795
APA StyleMazur, M., Corridore, D., Ndokaj, A., Ardan, R., Vozza, I., Babajko, S., & Jedeon, K. (2023). MIH and Dental Caries in Children: A Systematic Review and Meta-Analysis. Healthcare, 11(12), 1795. https://doi.org/10.3390/healthcare11121795