

KIT 1 (Keep in Touch) Project—Televisits for Cancer Patients during Italian Lockdown for COVID-19 Pandemic: The Real-World Experience of Establishing a Telemedicine System
 , ,
, ,  , , ,
, , ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- -
- -
- -
- -
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zanardo, M.; Cornacchione, P.; Marconi, E.; Dinapoli, L.; Fellin, F.; Gerasia, R.; Monti, C.B.; Sardanelli, F.; Tagliaferri, L.; Jereczek-Fossa, B.A.; et al. Occupational burnout among radiation therapy technologists in Italy before and during COVID-19 pandemic. J. Med. Imaging Radiat. Sci. 2021, 53, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Fragomeni, S.M.; Tagliaferri, L.; Rios, L.S.G.; Lancellotta, V.; Gentileschi, S.; Corrado, G.; Gui, B.; Colloca, G.; Rufini, V.; et al. Clinical impact of SARS-CoV-2 infection among patients with vulvar cancer: The Gemelli Vul.Can multidisciplinary team. Int. J. Gynecol. Cancer 2021, 32, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Halpern, S.D.; Truog, R.D.; Miller, F.G. Cognitive Bias and Public Health Policy During the COVID-19 Pandemic. JAMA 2020, 324, 337–338. [Google Scholar] [CrossRef]
- Marconi, E.; Chiesa, S.; Dinapoli, L.; Lepre, E.; Tagliaferri, L.; Balducci, M.; Frascino, V.; Casà, C.; Chieffo, D.P.R.; Gambacorta, M.A.; et al. A radiotherapy staff experience of gratitude during COVID-19 pandemic. Tech. Innov. Patient Support Radiat. Oncol. 2021, 18, 32–34. [Google Scholar] [CrossRef]
- Garganese, G.; Tagliaferri, L.; Fragomeni, S.M.; Lancellotta, V.; Colloca, G.; Corrado, G.; Gentileschi, S.; Macchia, G.; Tamburrini, E.; Gambacorta, M.A.; et al. Personalizing vulvar cancer workflow in COVID-19 era: A proposal from Vul.Can MDT. J. Cancer Res. Clin. Oncol. 2020, 146, 2535–2545. [Google Scholar] [CrossRef]
- Vavassori, A.; Tagliaferri, L.; Vicenzi, L.; D’Aviero, A.; Ciabattoni, A.; Gribaudo, S.; Lapadula, L.; Mattiucci, G.C.; Vinante, L.; De Sanctis, V.; et al. Practical indications for management of patients candidate to Interventional and Intraoperative Radiotherapy (Brachytherapy, IORT) during COVID-19 pandemic—A document endorsed by AIRO (Italian Association of Radiotherapy and Clinical Oncology) Interventional Radiotherapy Working Group. Radiother. Oncol. 2020, 149, 73–77. [Google Scholar] [CrossRef]
- Gentileschi, S.; Caretto, A.A.; Tagliaferri, L.; Salgarello, M.; Peris, K. Skin cancer plastic surgery during the COVID-19 pandemic. Eur. J. Surg. Oncol. 2020, 46, 1194–1195. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Di Stefani, A.; Schinzari, G.; Fionda, B.; Rossi, E.; Del Regno, L.; Gentileschi, S.; Federico, F.; Valentini, V.; Tortora, G.; et al. Skin cancer triage and management during COVID-19 pandemic. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1136–1139. [Google Scholar] [CrossRef]
- Cornacchione, P.; Tagliaferri, L.; D’Aviero, A.; Ciabattoni, A.; Galdieri, C.; De Sanctis, V.; Fellin, F.; Gribaudo, S.; Lambertini, D.; Gambacorta, M.A.; et al. The role of radiation therapy technologist in interventional radiotherapy (brachytherapy) in Italy: Italian Association of Radiotherapy and Clinical Oncology (AIRO) and Italian Association of Radiation Therapy and Medical Physics Technologists (AITRO) joint project. J. Contemp. Brachytherapy 2021, 13, 599–604. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Vavassori, A.; Lancellotta, V.; De Sanctis, V.; Barbera, F.; Fusco, V.; Vidali, C.; Fionda, B.; Colloca, G.; Gambacorta, M.; et al. Can brachytherapy be properly considered in the clinical practice? Trilogy project: The vision of the AIRO (Italian Association of Radiotherapy and Clinical Oncology) Interventional Radiotherapy study group. J. Contemp. Brachytherapy 2020, 12, 84–90. [Google Scholar] [CrossRef]
- Thureau, S.; Faivre, J.C.; Assaker, R.; Biver, E.; Confavreux, C.B.; Debiais, F.; Duterque-Coquillaud, M.; Giammarile, F.; Heymann, D.; Lecouvet, F.E.; et al. Adapting palliative radiation therapy for bone metastases during the COVID-19 pandemic: GEMO position paper. J. Bone Oncol. 2020, 22, 100291. [Google Scholar] [CrossRef]
- Braunstein, L.Z.; Gillespie, E.F.; Hong, L.; Xu, A.; Bakhoum, S.F.; Cuaron, J.; Mueller, B.; McCormick, B.; Cahlon, O.; Powell, S.; et al. Breast Radiation Therapy Under COVID-19 Pandemic Resource Constraints—Approaches to Defer or Shorten Treatment From a Comprehensive Cancer Center in the United States. Adv. Radiat. Oncol. 2020, 5, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Belka, C.; Bezjak, A.; Bradley, J.; Daly, M.E.; DeRuysscher, D.; Dziadziuszko, R.; Faivre-Finn, C.; Flentje, M.; Gore, E.; et al. Practice recommendations for lung cancer radiotherapy during the COVID-19 pandemic: An ESTRO-ASTRO consensus statement. Radiother. Oncol. 2020, 146, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Thomson, D.J.; Palma, D.; Guckenberger, M.; Balermpas, P.; Beitler, J.J.; Blanchard, P.; Brizel, D.; Budach, W.; Caudell, J.; Corry, J.; et al. Practice Recommendations for Risk-Adapted Head and Neck Cancer Radiation Therapy During the COVID-19 Pandemic: An ASTRO-ESTRO Consensus Statement. Int. J. Radiat. Oncol. 2020, 107, 618–627. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Yu, J.B.; McBride, S.M.; Dess, R.T.; Jackson, W.C.; Mahal, B.A.; Chen, R.; Choudhury, A.; Henry, A.; Syndikus, I.; et al. Prostate Cancer Radiation Therapy Recommendations in Response to COVID-19. Adv. Radiat. Oncol. 2020, 5, 659–665. [Google Scholar] [CrossRef]
- Meattini, I.; Franco, P.; Belgioia, L.; Boldrini, L.; Botticella, A.; De Santis, M.C.; Marvaso, G.; Montesi, G.; Parisi, S.; Triggiani, L.; et al. Radiation therapy during the coronavirus disease 2019 (COVID-19) pandemic in Italy: A view of the nation’s young oncologists. ESMO Open 2020, 5, e000779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitelaw, S.; Mamas, M.A.; Topol, E.; Van Spall, H.G. Applications of digital technology in COVID-19 pandemic planning and response. Lancet Digit. Health 2020, 2, e435–e440. [Google Scholar] [CrossRef]
- Wang, C.J.; Ng, C.; Brook, R.H. Response to COVID-19 in Taiwan. JAMA 2020, 323, 1341. [Google Scholar] [CrossRef]
- Naudé, W. Artificial intelligence vs COVID-19: Limitations, constraints and pitfalls. AI Soc. 2020, 35, 761–765. [Google Scholar] [CrossRef]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: Evaluation of the diagnostic accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef] [Green Version]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Parker, M.; Bonsall, D.G.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.C.; Singh, I.; Koehler, E.; Polgreen, P.M. A Smartphone-Driven Thermometer Application for Real-time Population- and Individual-Level Influenza Surveillance. Clin. Infect. Dis. 2018, 67, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Or, C.K.; Liu, K.; So, M.K.P.; Cheung, B.; Yam, L.Y.C.; Tiwari, A.; Lau, Y.F.E.; Lau, T.; Hui, P.S.G.; Cheng, H.C.; et al. Improving Self-Care in Patients With Coexisting Type 2 Diabetes and Hypertension by Technological Surrogate Nursing: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e16769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hans, P.K.; Gray, C.S.; Gill, A.; Tiessen, J. The provider perspective: Investigating the effect of the Electronic Patient-Reported Outcome (ePRO) mobile application and portal on primary care provider workflow. Prim. Health Care Res. Dev. 2017, 19, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorsey, E.R.; Topol, E.J. State of Telehealth. N. Engl. J. Med. 2016, 375, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Reed, M.E.; Huang, J.; Parikh, R.; Millman, A.; Ballard, D.W.; Barr, I.; Wargon, C. Patient–Provider Video Telemedicine Integrated With Clinical Care: Patient Experiences. Ann. Intern. Med. 2019, 171, 222–224. [Google Scholar] [CrossRef]
- Kahn, J.M. Virtual Visits—Confronting the Challenges of Telemedicine. N. Engl. J. Med. 2015, 372, 1684–1685. [Google Scholar] [CrossRef] [Green Version]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. Can Mobile Health Technologies Transform Health Care? JAMA 2013, 310, 2395–2396. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef]
- World Health Organization. Report by the Director-General. World Health Assembly Seventy-First World Health Assembly—Promote Health, Keep the World Safe, Serve the Vulnerable. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/324775/WHO-PRP-18.1-eng.pdf (accessed on 5 May 2021).
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring with Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 557–565. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef] [Green Version]
- Basch, E.; Schrag, D.; Henson, S.; Jansen, J.; Ginos, B.; Stover, A.M.; Carr, P.; Spears, P.A.; Jonsson, M.; Deal, A.M.; et al. Effect of Electronic Symptom Monitoring on Patient-Reported Outcomes Among Patients With Metastatic Cancer. JAMA 2022, 327, 2413. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Wani, S.U.D.; Masoodi, M.H.; Khan, N.A.; Shivakumar, H.; Osmani, R.M.A.; Khan, K.A. Global Effect of COVID-19 Pandemic on Cancer Patients and its Treatment: A Systematic Review. Clin. Complement. Med. Pharmacol. 2022, 2, 100041. [Google Scholar] [CrossRef] [PubMed]
- Orazem, M.; Oblak, I.; Spanic, T.; Ratosa, I. Telemedicine in Radiation Oncology Post–COVID-19 Pandemic: There Is No Turning Back. Int. J. Radiat. Oncol. 2020, 108, 411–415. [Google Scholar] [CrossRef]
- Ma, T.M.; Parikh, N.R.; Philipson, R.G.; van Dams, R.; Chang, E.M.; Hegde, J.V.; Kishan, A.U.; Kaprealian, T.B.; Steinberg, M.L.; Raldow, A.C. Experience of Telemedicine Visits in Radiation Oncology During the COVID-19 Pandemic: A US National Survey and Lessons Learned for Incorporating Telemedicine Post-COVID-19. Adv. Radiat. Oncol. 2022, 8, 100924. [Google Scholar] [CrossRef]
- Damiani, A.; Masciocchi, C.; Lenkowicz, J.; Capocchiano, N.D.; Boldrini, L.; Tagliaferri, L.; Cesario, A.; Sergi, P.; Marchetti, A.; Luraschi, A.; et al. Building an Artificial Intelligence Laboratory Based on Real World Data: The Experience of Gemelli Generator. Front. Comput. Sci. 2021, 3, 768266. [Google Scholar] [CrossRef]
- Lizée, T.; Basch, E.; Trémolières, P.; Voog, E.; Domont, J.; Peyraga, G.; Urban, T.; Bennouna, J.; Septans, A.-L.; Balavoine, M.; et al. Cost-Effectiveness of Web-Based Patient-Reported Outcome Surveillance in Patients With Lung Cancer. J. Thorac. Oncol. 2019, 14, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Lethrosne, C.; Pourel, N.; Molinier, O.; Pointreau, Y.; Domont, J.; Bourgeois, H.; Senellart, H.; Trémolières, P.; Lizée, T.; et al. Randomized Trial Comparing a Web-Mediated Follow-up With Routine Surveillance in Lung Cancer Patients. Gynecol. Oncol. 2017, 109, djx029. [Google Scholar] [CrossRef] [Green Version]
- Olsen, D.R.; Bruland, S.; Davis, B.J. Telemedicine in radiotherapy treatment planning: Requirements and applications. Radiother. Oncol. 2000, 54, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Hauth, F.; Bizu, V.; App, R.; Lautenbacher, H.; Tenev, A.; Bitzer, M.; Malek, N.P.; Zips, D.; Gani, C. Electronic Patient-Reported Outcome Measures in Radiation Oncology: Initial Experience After Workflow Implementation. JMIR mHealth uHealth 2019, 7, e12345. [Google Scholar] [CrossRef] [Green Version]
- Lewis, G.D.; Hatch, S.S.; Wiederhold, L.R.; Swanson, T.A. Long-Term Institutional Experience With Telemedicine Services for Radiation Oncology: A Potential Model for Long-Term Utilization. Adv. Radiat. Oncol. 2020, 5, 780–782. [Google Scholar] [CrossRef]
- Price, A.; Henke, L.E.; Maraghechi, B.; Kim, T.; Spraker, M.B.; Hugo, G.D.; Robinson, C.G.; Knutson, N.C. Implementation of a Novel Remote Physician Stereotactic Body Radiation Therapy Coverage Process during the Coronavirus Pandemic. Adv. Radiat. Oncol. 2020, 5, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Deantonio, L.; Bosetti, D.; Cima, S.; Martucci, F.; Borgonovo, G.; Di Bella, G.; Pesce, G.A.; Valli, M.; Richetti, A. #Stayathome: Smart working for radiation oncologists during the corona pandemic. Strahlenther. Onkol. 2020, 196, 1094–1095. [Google Scholar] [CrossRef] [PubMed]
- Caravatta, L.; Rosa, C.; Di Sciascio, M.B.; Scaringi, A.T.; Di Pilla, A.; Ursini, L.A.; Taraborrelli, M.; Vinciguerra, A.; Augurio, A.; Di Tommaso, M.; et al. COVID-19 and radiation oncology: The experience of a two-phase plan within a single institution in central Italy. Radiat. Oncol. 2020, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- Fallahzadeh, R.; Rokni, S.A.; Ghasemzadeh, H.; Soto-Perez-De-Celis, E.; Shahrokni, A. Digital Health for Geriatric Oncology. JCO Clin. Cancer Informatics 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Cesario, A.; D’Oria, M.; Bove, F.; Privitera, G.; Boškoski, I.; Pedicino, D.; Boldrini, L.; Erra, C.; Loreti, C.; Liuzzo, G.; et al. Personalized Clinical Phenotyping through Systems Medicine and Artificial Intelligence. J. Pers. Med. 2021, 11, 265. [Google Scholar] [CrossRef]
- Cesario, A.; D’Oria, M.; Calvani, R.; Picca, A.; Pietragalla, A.; Lorusso, D.; Daniele, G.; Lohmeyer, F.M.; Boldrini, L.; Valentini, V.; et al. The Role of Artificial Intelligence in Managing Multimorbidity and Cancer. J. Pers. Med. 2021, 11, 314. [Google Scholar] [CrossRef]
- Cesario, A.; Lohmeyer, F.M.; D’Oria, M.; Manto, A.; Scambia, G. The personalized medicine discourse: Archaeology and genealogy. Med. Health Care Philos. 2021, 24, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Chiloiro, G.; Romano, A.; D’Aviero, A.; Dinapoli, L.; Zane, E.; Tenore, A.; Boldrini, L.; Balducci, M.; Gambacorta, M.A.; Mattiucci, G.C.; et al. Patients’ Satisfaction by SmileInTM Totems in Radiotherapy: A Two-Year Mono-Institutional Experience. Healthcare 2021, 9, 1268. [Google Scholar] [CrossRef]
- Dinapoli, N.; Casà, C.; Barbaro, B.; Chiloiro, G.V.; Damiani, A.; Di Matteo, M.; Farchione, A.; Gambacorta, M.A.; Gatta, R.; Lanzotti, V.; et al. Radiomics for rectal cancer. Transl. Cancer Res. 2016, 5, 424–431. [Google Scholar] [CrossRef]
- Dinapoli, N.; Barbaro, B.; Gatta, R.; Chiloiro, G.; Casà, C.; Masciocchi, C.; Damiani, A.; Boldrini, L.; Gambacorta, M.A.; Dezio, M.; et al. Magnetic Resonance, Vendor-independent, Intensity Histogram Analysis Predicting Pathologic Complete Response After Radiochemotherapy of Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, D.; Boldrini, L.; Yadav, P.; Casà, C.; Lee, S.L.; Romano, A.; Piras, A.; Chiloiro, G.; Placidi, L.; Catucci, F.; et al. Delta Radiomics Analysis for Local Control Prediction in Pancreatic Cancer Patients Treated Using Magnetic Resonance Guided Radiotherapy. Diagnostics 2021, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, D.; Dinapoli, N.; Boldrini, L.; Chiloiro, G.; Gatta, R.; Masciocchi, C.; Lenkowicz, J.; Casà, C.; Damiani, A.; Azario, L.; et al. Fractal-based radiomic approach to predict complete pathological response after chemo-radiotherapy in rectal cancer. Radiol. Med. 2018, 123, 286–295. [Google Scholar] [CrossRef]
- Chiloiro, G.; Rodriguez-Carnero, P.; Lenkowicz, J.; Casà, C.; Masciocchi, C.; Boldrini, L.; Cusumano, D.; DiNapoli, N.; Meldolesi, E.; Carano, D.; et al. Delta Radiomics Can Predict Distant Metastasis in Locally Advanced Rectal Cancer: The Challenge to Personalize the Cure. Front. Oncol. 2020, 10, 595012. [Google Scholar] [CrossRef]
- Gatta, R.; Vallati, M.; Dinapoli, N.; Masciocchi, C.; Lenkowicz, J.; Cusumano, D.; Casá, C.; Farchione, A.; Damiani, A.; van Soest, J.; et al. Towards a modular decision support system for radiomics: A case study on rectal cancer. Artif. Intell. Med. 2018, 96, 145–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boldrini, L.; Cusumano, D.; Chiloiro, G.; Casà, C.; Masciocchi, C.; Lenkowicz, J.; Cellini, F.; Dinapoli, N.; Azario, L.; Teodoli, S.; et al. Delta radiomics for rectal cancer response prediction with hybrid 0.35 T magnetic resonance-guided radiotherapy (MRgRT): A hypothesis-generating study for an innovative personalized medicine approach. Radiol. Med. 2019, 124, 145–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casà, C.; Piras, A.; D’Aviero, A.; Preziosi, F.; Mariani, S.; Cusumano, D.; Romano, A.; Boskoski, I.; Lenkowicz, J.; Dinapoli, N.; et al. The impact of radiomics in diagnosis and staging of pancreatic cancer. Ther. Adv. Gastrointest. Endosc. 2022, 15, 263177452210815. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Pagliara, M.M.; Masciocchi, C.; Scupola, A.; Azario, L.; Grimaldi, G.; Autorino, R.; Gambacorta, M.A.; Laricchiuta, A.; Boldrini, L.; et al. Nomogram for predicting radiation maculopathy in patients treated with Ruthenium-106 plaque brachytherapy for uveal melanoma. J. Contemp. Brachytherapy 2017, 9, 540–547. [Google Scholar] [CrossRef] [Green Version]
- Balducci, M.; Fiorentino, A.; de Bonis, P.; Chiesa, S.; Manfrida, S.; D’Agostino, G.R.; Mantini, G.; Frascino, V.; Mattiucci, G.C.; De Bari, B.; et al. Impact of age and co-morbidities in patients with newly diagnosed glioblastoma: A pooled data analysis of three prospective mono-institutional phase II studies. Med. Oncol. 2012, 29, 3478–3483. [Google Scholar] [CrossRef]
- Van Gijn, W.; van Stiphout, R.G.P.M.; van de Velde, C.J.H.; Valentini, V.; Lammering, G.; Gambacorta, M.A.; Påhlman, L.; Bujko, K.; Lambin, P. Nomograms to predict survival and the risk for developing local or distant recurrence in patients with rectal cancer treated with optional short-term radiotherapy. Ann. Oncol. 2015, 26, 928–935. [Google Scholar] [CrossRef]
- Boldrini, L.; Lenkowicz, J.; Orlandini, L.C.; Yin, G.; Cusumano, D.; Chiloiro, G.; Dinapoli, N.; Peng, Q.; Casà, C.; Gambacorta, M.A.; et al. Applicability of a pathological complete response magnetic resonance-based radiomics model for locally advanced rectal cancer in intercontinental cohort. Radiat. Oncol. 2022, 17, 78. [Google Scholar] [CrossRef]
- Iezzi, R.; Casà, C.; Posa, A.; Cornacchione, P.; Carchesio, F.; Boldrini, L.; Tanzilli, A.; Cerrito, L.; Fionda, B.; Longo, V.; et al. Project for interventional Oncology LArge-database in liveR Hepatocellular carcinoma—Preliminary CT-based radiomic analysis (POLAR Liver 1.1). Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2891–2899. [Google Scholar] [CrossRef] [PubMed]
- Sicilia, R.; Cordelli, E.; Ramella, S.; Fiore, M.; Greco, C.; Molfese, E.; Miele, M.; Vinciguerra, E.; Cornacchione, P.; Ippolito, E.; et al. Exploratory Radiomics for Predicting Adaptive Radiotherapy in Non-Small Cell Lung Cancer. In Proceedings of the 2018 IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 250–255. [Google Scholar] [CrossRef]
- Soror, T.; Lancellotta, V.; Kovács, G.; Lanzotti, V.; Tagliaferri, L.; Casà, C.; Aristei, C.; Barberini, F.; Mahmoud, M.; Badakhshi, H. kOBCS©: A novel software calculator program of the Objective Breast Cosmesis Scale (OBCS). Breast Cancer 2019, 27, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, L.; Giarrizzo, I.; Fionda, B.; Rigante, M.; Pagliara, M.M.; Casà, C.; Parrilla, C.; Lancellotta, V.; Placidi, E.; Salvati, A.; et al. ORIFICE (Interventional Radiotherapy for Face Aesthetic Preservation) Study: Results of Interdisciplinary Assessment of Interstitial Interventional Radiotherapy (Brachytherapy) for Periorificial Face Cancer. J. Pers. Med. 2022, 12, 1038. [Google Scholar] [CrossRef]
- Lancellotta, V.; Macchia, G.; Dinapoli, N.; Autorino, R.; Campitelli, M.; Nardangeli, A.; Salvati, A.; Fionda, B.; Casà, C.; Cornacchione, P.; et al. EROS 2.0 study: Evaluation of two interventional radiotherapy (brachytherapy) schedules for endometrial cancer: A comparison of late vaginal toxicity rates. Radiol. Med. 2022, 127, 341–348. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Kovács, G.; Autorino, R.; Budrukkar, A.; Guinot, J.L.; Hildebrand, G.; Johansson, B.; Monge, R.M.; Meyer, J.E.; Niehoff, P.; et al. ENT COBRA (Consortium for Brachytherapy Data Analysis): Interdisciplinary standardized data collection system for head and neck patients treated with interventional radiotherapy (brachytherapy). J. Contemp. Brachytherapy 2016, 8, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Tagliaferri, L.; Budrukkar, A.; Lenkowicz, J.; Cambeiro, M.; Bussu, F.; Guinot, J.L.; Hildebrandt, G.; Johansson, B.; Meyer, J.E.; Niehoff, P.; et al. ENT COBRA ONTOLOGY: The covariates classification system proposed by the Head & Neck and Skin GEC-ESTRO Working Group for interdisciplinary standardized data collection in head and neck patient cohorts treated with interventional radiotherapy (brachytherapy). J. Contemp. Brachytherapy 2018, 10, 260–266. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Ciardo, F.G.; Fionda, B.; Casà, C.; Di Stefani, A.; Lancellotta, V.; Placidi, E.; Macchia, G.; Capocchiano, N.D.; Morganti, A.G.; et al. Non-melanoma Skin Cancer Treated by Contact High-dose-rate Radiotherapy (Brachytherapy): A Mono-institutional Series and Literature Review. Vivo 2021, 35, 2313–2319. [Google Scholar] [CrossRef]
- Lancellotta, V.; D’Aviero, A.; Fionda, B.; Di Stefani, A.; Casà, C.; Del Regno, L.; Gentileschi, S.; Colloca, G.F.; Rossi, E.; Schinzari, G.; et al. Contact skin radiotherapy (brachytherapy) for the treatment of non-melanoma skin cancers during COVID-19 pandemic. Dermatol. Ther. 2021, 35, e15276. [Google Scholar] [CrossRef]
- Lancellotta, V.; Guinot, J.L.; Fionda, B.; Rembielak, A.; Di Stefani, A.; Gentileschi, S.; Federico, F.; Rossi, E.; Guix, B.; Chyrek, A.J.; et al. SKIN-COBRA (Consortium for Brachytherapy data Analysis) ontology: The first step towards interdisciplinary standardized data collection for personalized oncology in skin cancer. J. Contemp. Brachytherapy 2020, 12, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Gatta, R.; Vallati, M.; Lenkowicz, J.; Casa, C.; Cellini, F.; Damiani, A.; Valentini, V. A Framework for Event Log Generation and Knowledge Representation for Process Mining in Healthcare. In Proceedings of the 2018 IEEE 30th International Conference on Tools with Artificial Intelligence (ICTAI), Volos, Greece, 5–7 November 2018; pp. 647–654. [Google Scholar] [CrossRef] [Green Version]
- Lenkowicz, J.; Gatta, R.; Masciocchi, C.; Casà, C.; Cellini, F.; Damiani, A.; Dinapoli, N.; Valentini, V. Assessing the conformity to clinical guidelines in oncology: An example for the multidisciplinary management of locally advanced colorectal cancer treatment. Manag. Decis. 2018, 56, 2172–2186. [Google Scholar] [CrossRef]
- Marazzi, F.; Tagliaferri, L.; Masiello, V.; Moschella, F.; Colloca, G.F.; Corvari, B.; Sanchez, A.M.; Capocchiano, N.D.; Pastorino, R.; Iacomini, C.; et al. GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives. J. Pers. Med. 2021, 11, 65. [Google Scholar] [CrossRef] [PubMed]
- Fionda, B.; Boldrini, L.; D’Aviero, A.; Lancellotta, V.; Gambacorta, M.; Kovács, G.; Patarnello, S.; Valentini, V.; Tagliaferri, L. Artificial intelligence (AI) and interventional radiotherapy (brachytherapy): State of art and future perspectives. J. Contemp. Brachytherapy 2020, 12, 497–500. [Google Scholar] [CrossRef]
- Mattiucci, G.C.; Boldrini, L.; Chiloiro, G.; D’Agostino, G.R.; Chiesa, S.; De Rose, F.; Azario, L.; Pasini, D.; Gambacorta, M.A.; Balducci, M.; et al. Automatic delineation for replanning in nasopharynx radiotherapy: What is the agreement among experts to be considered as benchmark? Acta Oncol. 2013, 52, 1417–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fionda, B.; Piras, A.; D’Aviero, A.; Venuti, V.; Casà, C.; Preziosi, F.; Catucci, F.; Boldrini, L.; Daidone, A.; Tagliaferri, L.; et al. The “PC-WIRED” study: Patient Centred Evolution of Websites of Italian Radiotherapy Departments. Patient Educ. Couns. 2021, 104, 2152–2153. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, L.; Dinapoli, L.; Casà, C.; Colloca, G.F.; Marazzi, F.; Cornacchione, P.; Mazzarella, C.; Masiello, V.; Chiesa, S.; Bartoli, F.B.; et al. Art and digital technologies to support resilience during the oncological journey: The Art4ART project. Tech. Innov. Patient Support Radiat. Oncol. 2022, 24, 101–106. [Google Scholar] [CrossRef]
- Casà, C.; Dinapoli, L.; Marconi, E.; Chiesa, S.; Cornacchione, P.; Bartoli, F.B.; Bracci, S.; Salvati, A.; Scalise, S.; Colloca, G.F.; et al. Integration of art and technology in personalized radiation oncology care: Experiences, evidence, and perspectives. Front. Public Health 2023, 11, 1056307. [Google Scholar] [CrossRef]
- Keesara, S.; Jonas, A.; Schulman, K. COVID-19 and Health Care’s Digital Revolution. N. Engl. J. Med. 2020, 382, e82. [Google Scholar] [CrossRef]
- Cilla, S.; Deodato, F.; Romano, C.; Ianiro, A.; Macchia, G.; Re, A.; Buwenge, M.; Boldrini, L.; Indovina, L.; Valentini, V.; et al. Personalized automation of treatment planning in head-neck cancer: A step forward for quality in radiation therapy? Phys. Medica 2021, 82, 7–16. [Google Scholar] [CrossRef]
- Johnson, S.B.; King, A.J.; Warner, E.L.; Aneja, S.; Kann, B.H.; Bylund, C.L. Using ChatGPT to evaluate cancer myths and misconceptions: Artificial intelligence and cancer information. JNCI Cancer Spectr. 2023, 7, pkad015. [Google Scholar] [CrossRef]
- Patel, S.B.; Lam, K. ChatGPT: The future of discharge summaries? Lancet Digit. Health 2023, 5, e107–e108. [Google Scholar] [CrossRef]
- Uprety, D.; Zhu, D.; West, H. ChatGPT—A promising generative AI tool and its implications for cancer care. Cancer 2023. early view. [Google Scholar] [CrossRef] [PubMed]
- Casà, C.; Marotta, C.; Di Pumpo, M.; Cozzolino, A.; D’Aviero, A.; Frisicale, E.M.; Silenzi, A.; Gabbrielli, F.; Bertinato, L.; Brusaferro, S. COVID-19 and digital competencies among young physicians: Are we (really) ready for the new era? A national survey of the Italian Young Medical Doctors Association. Ann. Ist. Super. Sanita. 2021, 57, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Valentini, V.; Marconi, E.; Dinapoli, L.; Casà, C. Come cambia la percezione della professione medica di fronte alla richiesta di morte. Med. Morale 2022, 71, 413–423. [Google Scholar] [CrossRef]
- Lancellotta, V.; De Sanctis, V.; Cornacchione, P.; Barbera, F.; Fusco, V.; Vidali, C.; Scalise, S.; Panza, G.; Tenore, A.; Colloca, G.; et al. HAPPY—Humanity Assurance Protocol in interventional radiotheraPY (brachytherapy)—An AIRO Interventional Radiotherapy Study Group project. J. Contemp. Brachytherapy 2019, 11, 510–515. [Google Scholar] [CrossRef]
- Abbasi, A.N.; Tariq, M.; Karim, M.U.; Casa, C. Emotional Intelligence Training can be Incorporated as an Essential Component of Postgraduate Medical Education: Paving the Way Towards the Development of Multidisciplinary Team Culture. J. Coll. Phys. Surg. Pak. 2023, 33, 362–363. [Google Scholar] [CrossRef]
- Pareek, P.; Vishnoi, J.R.; Kombathula, S.H.; Vyas, R.K.; Misra, S. Teleoncology: The Youngest Pillar of Oncology. JCO Glob. Oncol. 2020, 6, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Finazzi, T.; Papachristofilou, A.; Zimmermann, F. “Connection Failed”: A Word of Caution on Telemedicine in Radiation Oncology. Int. J. Radiat. Oncol. 2020, 108, 435–437. [Google Scholar] [CrossRef]
- Gabbrielli, F.; Bertinato, L.; De Filippis, G.; Bonomini, M.; Cipolla, M. Indicazioni ad Interim per Servizi Assistenziali di Telemedicina Durante l’Emergenza Sanitaria COVID-19. Published Online 13 April 2020. Rapporto ISS COVID-19 n. 12/2020. Available online: https://www.iss.it/rapporti-covid-19/-/asset_publisher/btw1J82wtYzH/content/rapporto-iss-covid-19-n.-12-2020-indicazioni-ad-interim-per-servizi-assistenziali-di-telemedicina-durante-l-emergenza-sanitaria-covid-19.-versione-del-13-aprile-2020?_com (accessed on 20 April 2020).




{kind=link}
{kind=link}
{kind=link}
| Project Phases | |
|---|---|
| 1 | Creation of the multi-professional group |
| 2 | Planning visits with the new scheme: Value 1 = visit not deferrable and held in person Value 2 = visit postponed Value 3 = visit performed via email management and call Value 4 = visit performed via complete teleconsultation using teleconsultation system |
| 3 | Identification of the equipment necessary for the teleconsultation |
| 4 | Request for collaboration with the Patients’ Association for the buying of equipment |
| 5 | Start of televisit/teleconsultation |
| 6 | Telephone interviews for patient satisfaction surveys |
| Questionnaire for Telephone Interview |
|---|
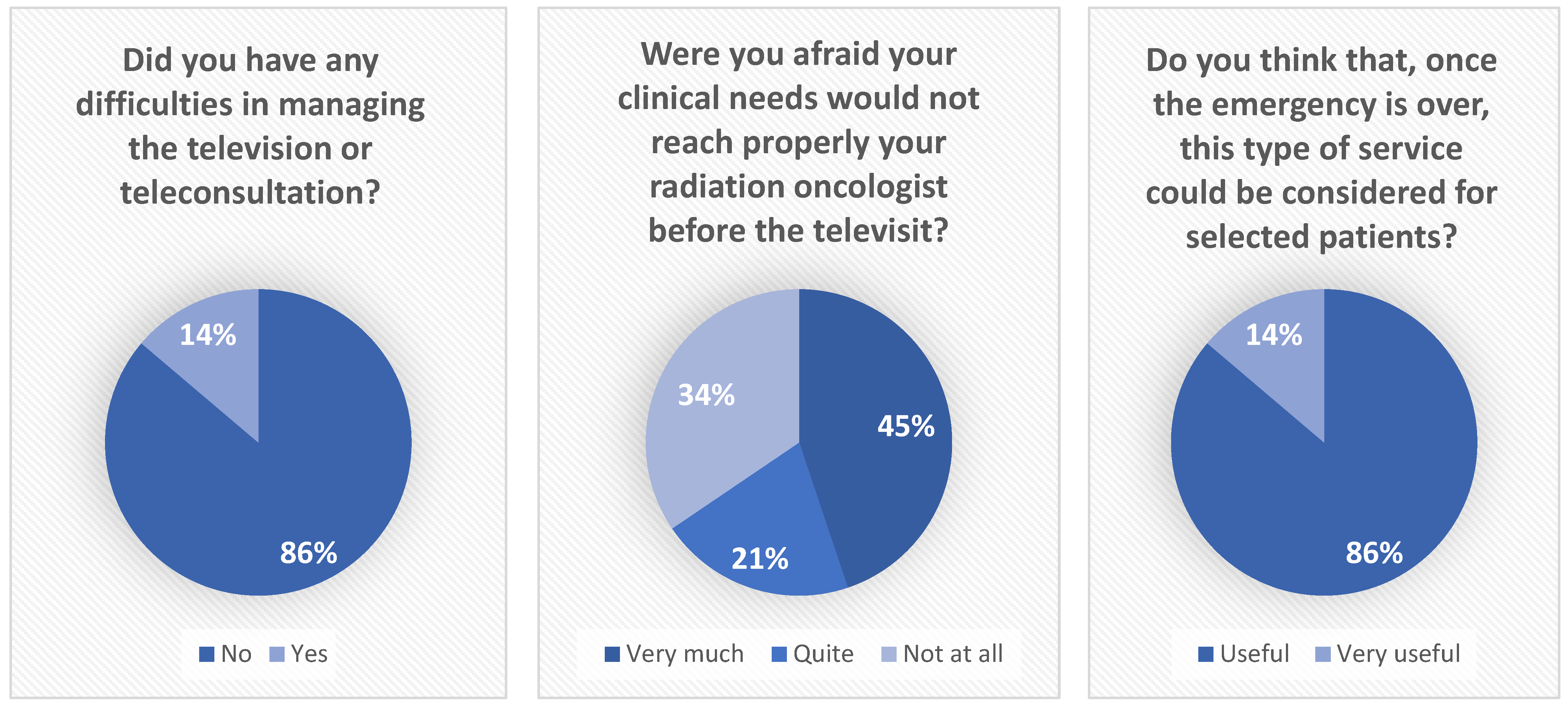
| Did you have any difficulties in managing the televisit or teleconsultation? [answers: yes/no] How much satisfied were you with the video-teleconsultation system? [answers in 5-likert scale] |
| When you realized that the pandemic could hamper your contact visit with your radiation oncologists, were you afraid your clinical needs would not reach properly your radiation oncologist before the televisit? [answers in 5-likert scale] |
| Do you think that, once the emergency is over, this type of service could be considered as an alternative of traditional on-site visits for selected patients? [answers in 5-likert scale] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casà, C.; Corvari, B.; Cellini, F.; Cornacchione, P.; D’Aviero, A.; Reina, S.; Di Franco, S.; Salvati, A.; Colloca, G.F.; Cesario, A.; et al. KIT 1 (Keep in Touch) Project—Televisits for Cancer Patients during Italian Lockdown for COVID-19 Pandemic: The Real-World Experience of Establishing a Telemedicine System. Healthcare 2023, 11, 1950. https://doi.org/10.3390/healthcare11131950
Casà C, Corvari B, Cellini F, Cornacchione P, D’Aviero A, Reina S, Di Franco S, Salvati A, Colloca GF, Cesario A, et al. KIT 1 (Keep in Touch) Project—Televisits for Cancer Patients during Italian Lockdown for COVID-19 Pandemic: The Real-World Experience of Establishing a Telemedicine System. Healthcare. 2023; 11(13):1950. https://doi.org/10.3390/healthcare11131950
Chicago/Turabian StyleCasà, Calogero, Barbara Corvari, Francesco Cellini, Patrizia Cornacchione, Andrea D’Aviero, Sara Reina, Silvia Di Franco, Alessandra Salvati, Giuseppe Ferdinando Colloca, Alfredo Cesario, and et al. 2023. "KIT 1 (Keep in Touch) Project—Televisits for Cancer Patients during Italian Lockdown for COVID-19 Pandemic: The Real-World Experience of Establishing a Telemedicine System" Healthcare 11, no. 13: 1950. https://doi.org/10.3390/healthcare11131950
APA StyleCasà, C., Corvari, B., Cellini, F., Cornacchione, P., D’Aviero, A., Reina, S., Di Franco, S., Salvati, A., Colloca, G. F., Cesario, A., Patarnello, S., Balducci, M., Morganti, A. G., Valentini, V., Gambacorta, M. A., & Tagliaferri, L. (2023). KIT 1 (Keep in Touch) Project—Televisits for Cancer Patients during Italian Lockdown for COVID-19 Pandemic: The Real-World Experience of Establishing a Telemedicine System. Healthcare, 11(13), 1950. https://doi.org/10.3390/healthcare11131950