
Short-Term Effects of Dietary Protein Supplementation on Physical Recovery in Older Patients at Risk of Malnutrition during Inpatient Rehabilitation: A Pilot, Randomized, Controlled Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
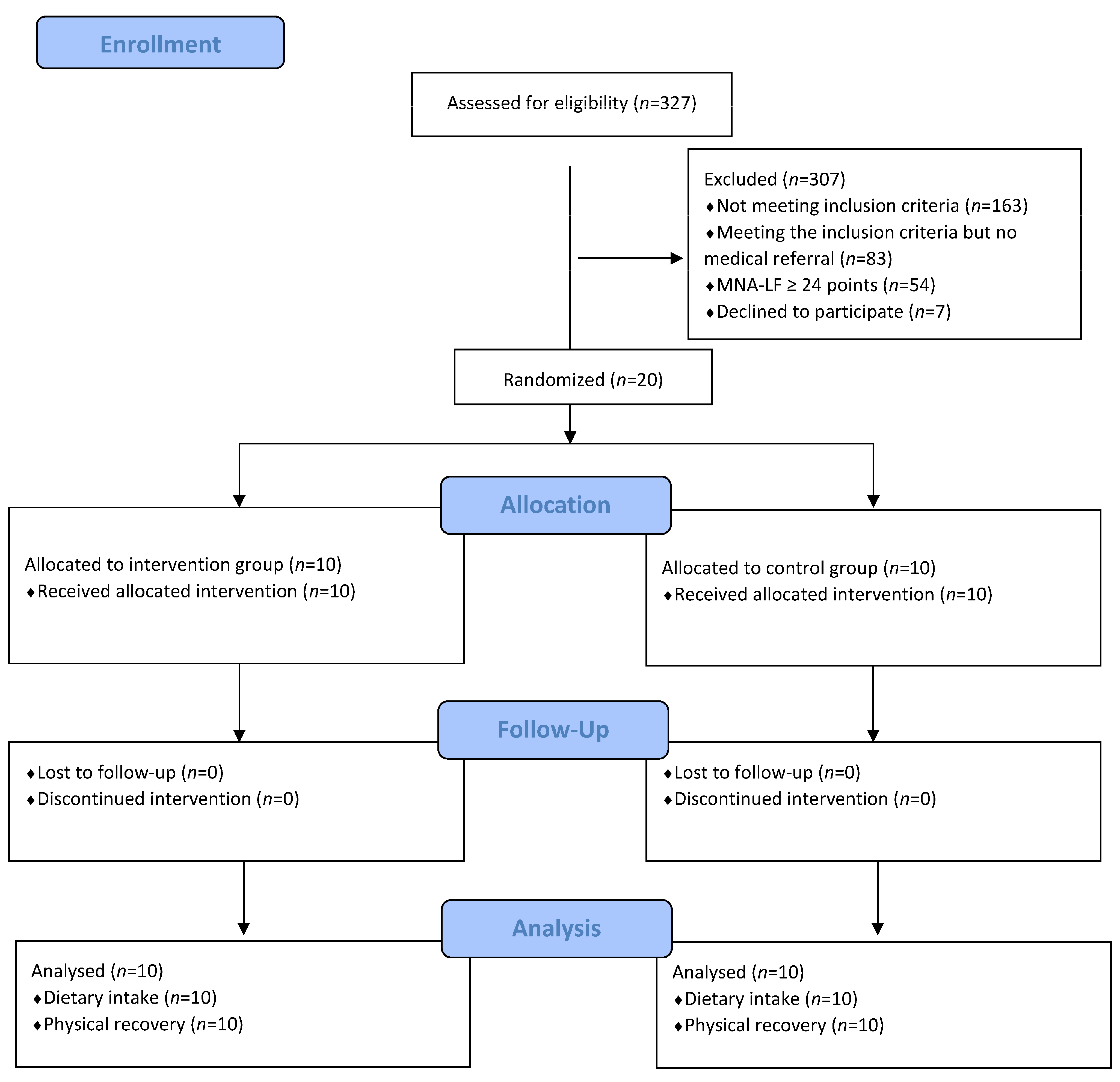
2.1. Study Design and Participants
2.2. Diagnosis of Malnutrition
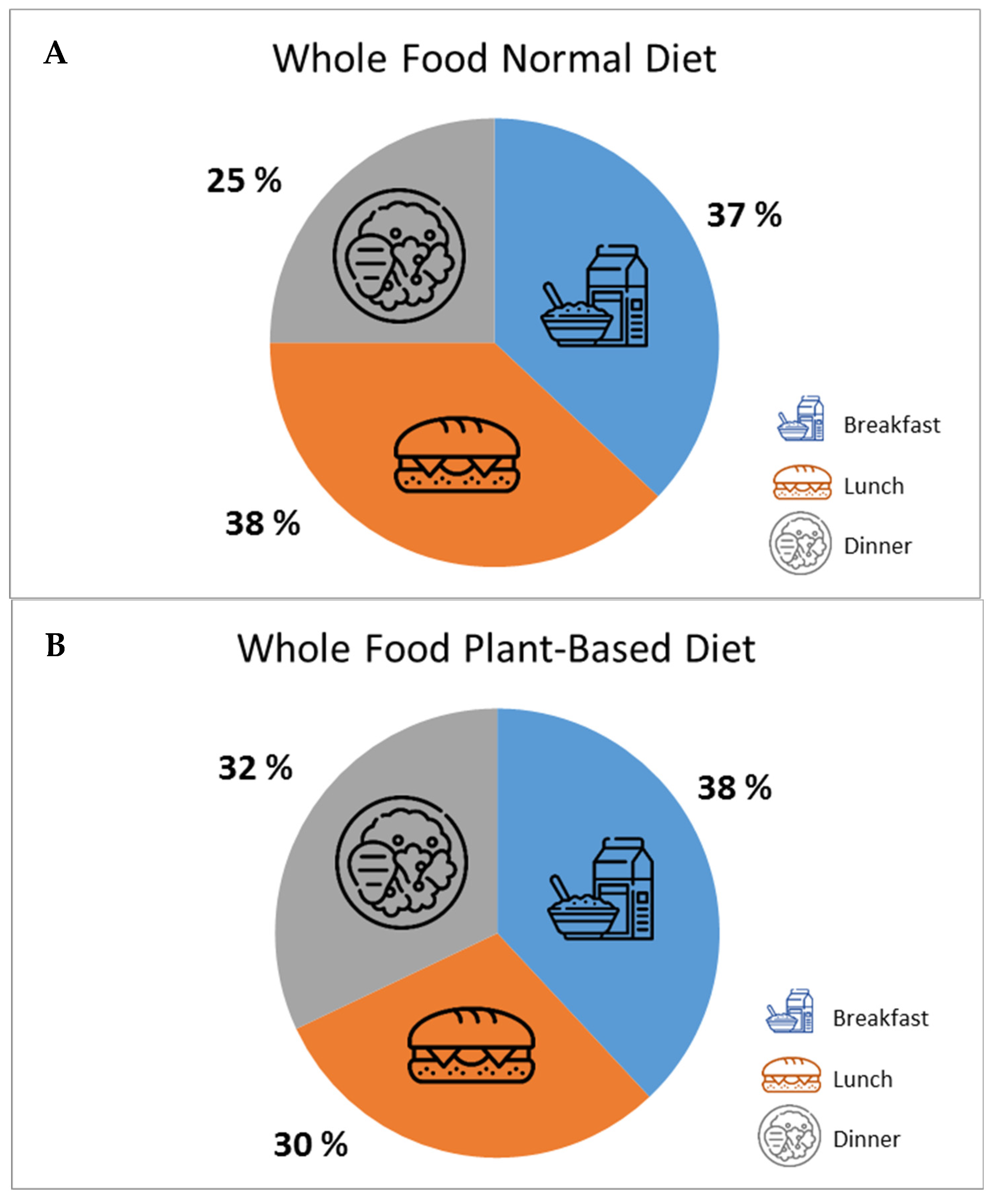
2.3. Nutritional Intervention
2.4. Rehabilitation Program
2.5. Outcomes and Data Collection
2.6. Sample Size
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.-Y.; Lengelé, L.; Bruyère, O. Malnutrition as a Strong Predictor of the Onset of Sarcopenia. Nutrients 2019, 11, 2883. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Santoro, L.; Santoliquido, A.; Sisto, A.; Picca, A.; Marzetti, E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos. Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, L.; van Wijngaarden, J.; Pacifico, J.; Reijnierse, E.; Meskers, C.; Maier, A. Association between malnutrition and stages of sarcopenia in geriatric rehabilitation inpatients: RESORT. Clin. Nutr. 2021, 40, 4090–4096. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Purcell, S.A.; Alish, C.; Pereira, S.L.; Deutz, N.E.; Heyland, D.K.; Goodpaster, B.H.; Tappenden, K.A.; Heymsfield, S.B. Implica-tions of low muscle mass across the continuum of care: A narrative review. Ann. Med. 2018, 50, 675–693. [Google Scholar] [CrossRef]
- Ramadi, A.; Ezeugwu, V.E.; Weber, S.; Funabashi, M.; Lima, C.A.; Perracini, M.R.; Beaupre, L.A. Progressive Resistance Training Pro-gram Characteristics in Rehabilitation Programs Following Hip Fracture: A Meta-Analysis and Meta-Regression. Geriatr. Orthop. Surg. Rehabil. 2022, 13, 21514593221090799. [Google Scholar] [CrossRef]
- Rondanelli, M.; Cereda, E.; Klersy, C.; Faliva, M.A.; Peroni, G.; Nichetti, M.; Gasparri, C.; Iannello, G.; Spadaccini, D.; Infantino, V.; et al. Improving rehabilitation in sarcopenia: A randomized-controlled trial utilizing a muscle-targeted food for special medical purposes. J. Cachex-Sarcopenia Muscle 2020, 11, 1535–1547. [Google Scholar] [CrossRef]
- Van Wijngaarden, J.P.; Wojzischke, J.; van den Berg, C.; Cetinyurek-Yavuz, A.; Diekmann, R.; Luiking, Y.C.; Bauer, J.M. Effects of Nu-tritional Interventions on Nutritional and Functional Outcomes in Geriatric Rehabilitation Patients: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1207–1215.e9. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Groenendijk, I.; Kramer, C.S.; Boeft, L.M.D.; Hobbelen, H.S.M.; van der Putten, G.-J.; de Groot, L.C.P.G.M. Hip Fracture Patients in Geriatric Rehabilitation Show Poor Nutritional Status, Dietary Intake and Muscle Health. Nutrients 2020, 12, 2528. [Google Scholar] [CrossRef]
- Weijzen, M.E.G.; Kouw, I.W.K.; Geerlings, P.; Verdijk, L.B.; Loon, L.J.C. During Hospitalization, Older Patients at Risk for Malnutrition Consume <0.65 Grams of Protein per Kilogram Body Weight per Day. Nutr. Clin. Pract. 2020, 35, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Hermanky, M.; Korninger, C.; Fuchs, D.; Strasser, B. Effects of a protein optimized diet combined with moderate resistance training on the postoperative course in older patients with hip fracture. Aktuel. Ernahrungsmed. 2017, 42, 180–187. [Google Scholar]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment Short-Form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Grote, V.; Unger, A.; Böttcher, E.; Muntean, M.; Puff, H.; Marktl, W.; Mur, E.; Kullich, W.; Holasek, S.; Hofmann, P.; et al. General and Disease-Specific Health Indicator Changes Associated with Inpatient Rehabilitation. J. Am. Med. Dir. Assoc. 2020, 21, 2017.e10–2017.e27. [Google Scholar] [CrossRef]
- Roza, A.M.; Shizgal, H.M. The Harris Benedict equation reevaluated: Resting energy requirements and the body cell mass. Am. J. Clin. Nutr. 1984, 40, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2018, 38, 10–47. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sar-copenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Di Vincenzo, O.; Marra, M.; Di Gregorio, A.; Pasanisi, F.; Scalfi, L. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: A systematic review. Clin. Nutr. 2020, 40, 3052–3061. [Google Scholar] [CrossRef]
- Norman, K.; Herpich, C.; Müller-Werdan, U. Role of phase angle in older adults with focus on the geriatric syndromes sarco-penia and frailty. Rev. Endocr. Metab. Disord. 2023, 24, 429–437. [Google Scholar] [CrossRef]
- Bruce, B.; Fries, J.F. The Stanford Health Assessment Questionnaire: Dimensions and Practical Applications. Health Qual. Life Outcomes 2003, 1, 20. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.; Sobotka, L.; et al. ESPEN practical guideline: Clinical nutrition and hydration in geriatrics. Clin. Nutr. 2022, 41, 958–989. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Chen, H.C.; Huang, S.W.; Liou, T.H. The role of muscle mass gain following protein supplementation plus exercise therapy in older adults with sarcopenia and frailty risks: A systematic review and meta-regression analysis of randomized trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [PubMed]
- Gomes, F.; Baumgartner, A.; Bounoure, L.; Bally, M.; Deutz, N.E.; Greenwald, J.L.; Stanga, Z.; Mueller, B.; Schuetz, P. Association of Nutritional Support With Clinical Outcomes Among Medical Inpatients Who Are Malnourished or at Nutritional Risk: An Updated Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e1915138. [Google Scholar] [CrossRef]
- Bhasin, S.; Apovian, C.M.; Travison, T.G.; Pencina, K.; Moore, L.L.; Huang, G.; Campbell, W.W.; Li, Z.; Howland, A.S.; Chen, R.; et al. Effect of Protein Intake on Lean Body Mass in Functionally Limited Older Men: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 530–541. [Google Scholar] [CrossRef]
- Tieland, M.; Dirks, M.L.; van der Zwaluw, N.; Verdijk, L.B.; van de Rest, O.; de Groot, L.C.; van Loon, L. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: A randomized, dou-ble-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef]
- Churchward-Venne, T.A.; Tieland, M.; Verdijk, L.B.; Leenders, M.; Dirks, M.L.; de Groot, L.C.; van Loon, L.J. There Are No Nonre-sponders to Resistance-Type Exercise Training in Older Men and Women. J. Am. Med. Dir. Assoc. 2015, 16, 400–411. [Google Scholar] [CrossRef]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip Strength across the Life Course: Normative Data from Twelve British Studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Tsintavis, P.; Potsaki, P.; Papandreou, D. Differences in the Prevalence of Sarcopenia in Communi-ty-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 83–90. [Google Scholar] [CrossRef]
- Bianchi, L.; Ferrucci, L.; Cherubini, A.; Maggio, M.; Bandinelli, S.; Savino, E.; Brombo, G.; Zuliani, G.; Guralnik, J.M.; Landi, F.; et al. The Predictive Value of the EWGSOP Definition of Sarcopenia: Results From the InCHIANTI Study. J. Gerontol. Ser. A 2015, 71, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Tan, V.M.H.; Pang, B.W.J.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Chen, K.K.; Ng, T.P.; Wee, S.L. Malnutrition and Sarcopenia in Communi-ty-Dwelling Adults in Singapore: Yishun Health Study. J. Nutr. Health Aging 2021, 25, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Lengelé, L.; Bruyère, O.; Beaudart, C.; Reginster, J.-Y.; Locquet, M. Impact of Malnutrition Status on Muscle Parameter Changes over a 5-Year Follow-Up of Community-Dwelling Older Adults from the SarcoPhAge Cohort. Nutrients 2021, 13, 407. [Google Scholar] [CrossRef]
- Pourhassan, M.; Rommersbach, N.; Lueg, G.; Klimek, C.; Schnatmann, M.; Liermann, D.; Janssen, G.; Wirth, R. The Impact of Malnu-trition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients 2020, 12, 1387. [Google Scholar] [CrossRef]
- Rossi, A.P.; Zanandrea, V.; Zoico, E.; Zanardo, M.; Caliari, C.; Confente, S.; Gabriele, S.; Mazzali, G.; Fantin, F.; Zamboni, M. Inflamma-tion and nutritional status as predictors of physical performance and strength loss during hospitalization. Eur. J. Clin. Nutr. 2016, 70, 1439–1442. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Jung, Y.W.; Hong, N.; Kim, C.O.; Kim, H.C.; Youm, Y.; Choi, J.-Y.; Rhee, Y. The diagnostic value of phase angle, an integrative bioelectrical marker, for identifying individuals with dysmobility syndrome: The Korean Urban-Rural Elderly study. Osteoporos. Int. 2020, 32, 939–949. [Google Scholar] [CrossRef]
- Uemura, K.; Yamada, M.; Okamoto, H. Association of bioimpedance phase angle and prospective falls in older adults. Geriatr. Gerontol. Int. 2019, 19, 503–507. [Google Scholar] [CrossRef]
- Uemura, K.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Kim, M.; Kurita, S.; Ishii, H.; Shimada, H. Predictivity of bioimpedance phase angle for incident disability in older adults. J. Cachex-Sarcopenia Muscle 2019, 11, 46–54. [Google Scholar] [CrossRef]
- Mertz, K.H.; Reitelseder, S.; Bechshoeft, R.; Bulow, J.; Højfeldt, G.; Jensen, M.; Schacht, S.R.; Lind, M.V.; Rasmussen, M.A.; Mikkelsen, U.R.; et al. The effect of daily protein supplementation, with or without re-sistance training for 1 year, on muscle size, strength, and function in healthy older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2021, 113, 790–800. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intervention (n = 10) | Control (n = 10) | p | |
|---|---|---|---|
| Age (years) | 75.0 ± 6.5 | 74.2 ± 6.8 | 0.792 |
| Sex (male/female) | 1/9 | 2/8 | 0.531 |
| Height (cm) | 163.0 ± 8.3 | 162.6 ± 6.8 | 0.907 |
| Body weight (kg) | 60.4 ± 6.9 | 62.2 ± 15.0 | 0.735 |
| BMI (kg/m2) | 22.9 ± 4.0 | 23.5 ± 5.9 | 0.792 |
| RMR (kcal/d) | 1198 ± 99 | 1232 ± 174 | 0.604 |
| MNA (score) | 21.4 ± 2.4 | 20.9 ± 1.3 | 0.575 |
| Mobility aids (yes/no) | 4/6 | 4/6 | 1.000 |
| Medical diagnosis for admission (n) | 0.819 | ||
| Arthrosis | 1 | 1 | |
| Diseases of the musculoskeletal system | 2 | 1 | |
| Lower limb injuries | 7 | 8 |
| Intervention (n = 10) Mean ± SD | p Time (t2 − t1) Intervention | Control (n = 10) Mean ± SD | p Time (t2 − t1) Control | p Time Both Groups | p Group t1 and t2 | p Interaction Time × Group | |
|---|---|---|---|---|---|---|---|
| Body weight t1 (kg) | 60.4 ± 6.9 | 0.039 * | 62.2 ± 15.0 | 0.375 | 0.038 * | 0.762 | 0.487 |
| Body weight t2 (kg) | 61.3 ± 6.3 | 62.6 ± 14.9 | |||||
| Hand-grip strength t1 (kg) | 20.7 ± 9.9 | 0.746 | 18.3 ± 5.5 | 0.444 | 0.398 | 0.516 | 0.652 |
| Hand-grip strength t2 (kg) | 20.9 ± 9.1 | 18.9 ± 4.3 | |||||
| Prealbumin t1 (mg/dL) | 21.1 ± 8.1 | 0.070 # | 23.8 ± 6.1 | 0.634 | 0.230 | 0.739 | 0.092 † |
| Prealbumin t2 (mg/dL) | 23.6 ± 8.9 | 23.9 ± 7.1 | |||||
| Fat-free mass t1 (kg) | 43.7 ± 7.1 | 0.327 | 42.6 ± 7.9 | 0.647 | 0.537 | 0.862 | 0.257 |
| Fat-free mass t2 (kg) | 43.0 ± 6.8 | 42.8 ± 8.6 | |||||
| Body cell mass t1 (kg) | 16.2 ± 6.0 | 0.881 | 16.4 ± 3.4 | 0.698 | 0.982 | 0.991 | 0.765 |
| Body cell mass t2 (kg) | 16.4 ± 3.7 | 16.2 ± 4.1 | |||||
| Fat mass t1 (kg) | 17.2 ± 7.8 | 0.050 * | 19.2 ± 10.0 | 0.923 | 0.182 | 0.705 | 0.110 |
| Fat mass t2 (kg) | 18.1 ± 7.3 | 19.2 ± 9.9 | |||||
| Phase angle t1 (°) | 3.8 ± 1.0 | 0.958 | 3.9 ± 0.6 | 0.521 | 0.757 | 0.769 | 0.853 |
| Phase angle t2 (°) | 3.8 ± 0.5 | 3.8 ± 0.6 | |||||
| HAQ score t1 | 0.42 ± 0.32 | 0.135 | 0.59 ± 0.28 | 0.589 | 0.241 | 0.256 | 0.879 |
| HAQ score t2 | 0.28 ± 0.27 | 0.48 ± 0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strasser, B.; Grote, V.; Bily, W.; Nics, H.; Riedl, P.; Jira, I.; Fischer, M.J. Short-Term Effects of Dietary Protein Supplementation on Physical Recovery in Older Patients at Risk of Malnutrition during Inpatient Rehabilitation: A Pilot, Randomized, Controlled Trial. Healthcare 2023, 11, 2317. https://doi.org/10.3390/healthcare11162317
Strasser B, Grote V, Bily W, Nics H, Riedl P, Jira I, Fischer MJ. Short-Term Effects of Dietary Protein Supplementation on Physical Recovery in Older Patients at Risk of Malnutrition during Inpatient Rehabilitation: A Pilot, Randomized, Controlled Trial. Healthcare. 2023; 11(16):2317. https://doi.org/10.3390/healthcare11162317
Chicago/Turabian StyleStrasser, Barbara, Vincent Grote, Walter Bily, Helena Nics, Patricia Riedl, Ines Jira, and Michael J. Fischer. 2023. "Short-Term Effects of Dietary Protein Supplementation on Physical Recovery in Older Patients at Risk of Malnutrition during Inpatient Rehabilitation: A Pilot, Randomized, Controlled Trial" Healthcare 11, no. 16: 2317. https://doi.org/10.3390/healthcare11162317
APA StyleStrasser, B., Grote, V., Bily, W., Nics, H., Riedl, P., Jira, I., & Fischer, M. J. (2023). Short-Term Effects of Dietary Protein Supplementation on Physical Recovery in Older Patients at Risk of Malnutrition during Inpatient Rehabilitation: A Pilot, Randomized, Controlled Trial. Healthcare, 11(16), 2317. https://doi.org/10.3390/healthcare11162317