
Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy in Korea: A Population-Based Cross-Sectional Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
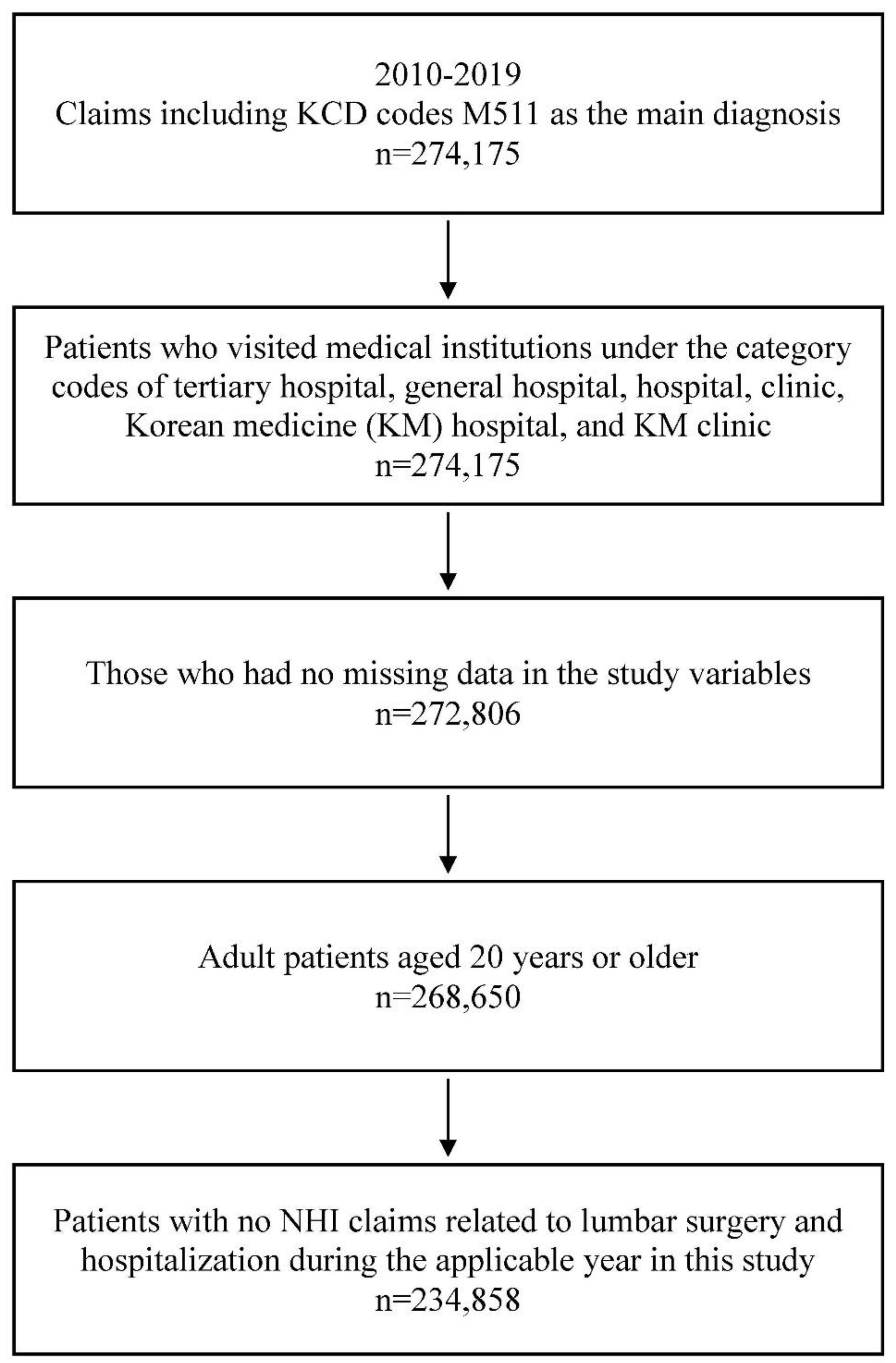
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Patients
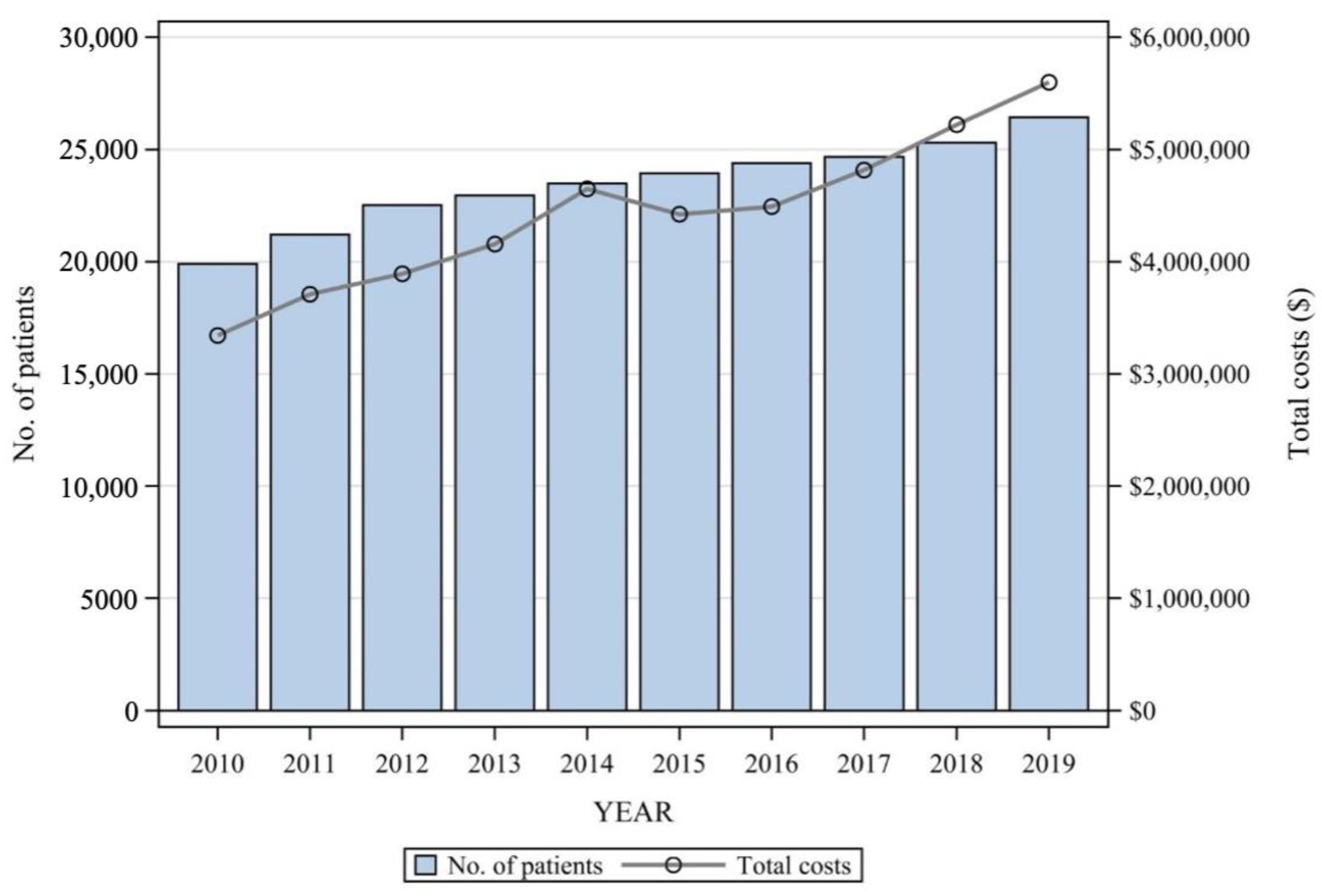
3.2. Use of Medical Services
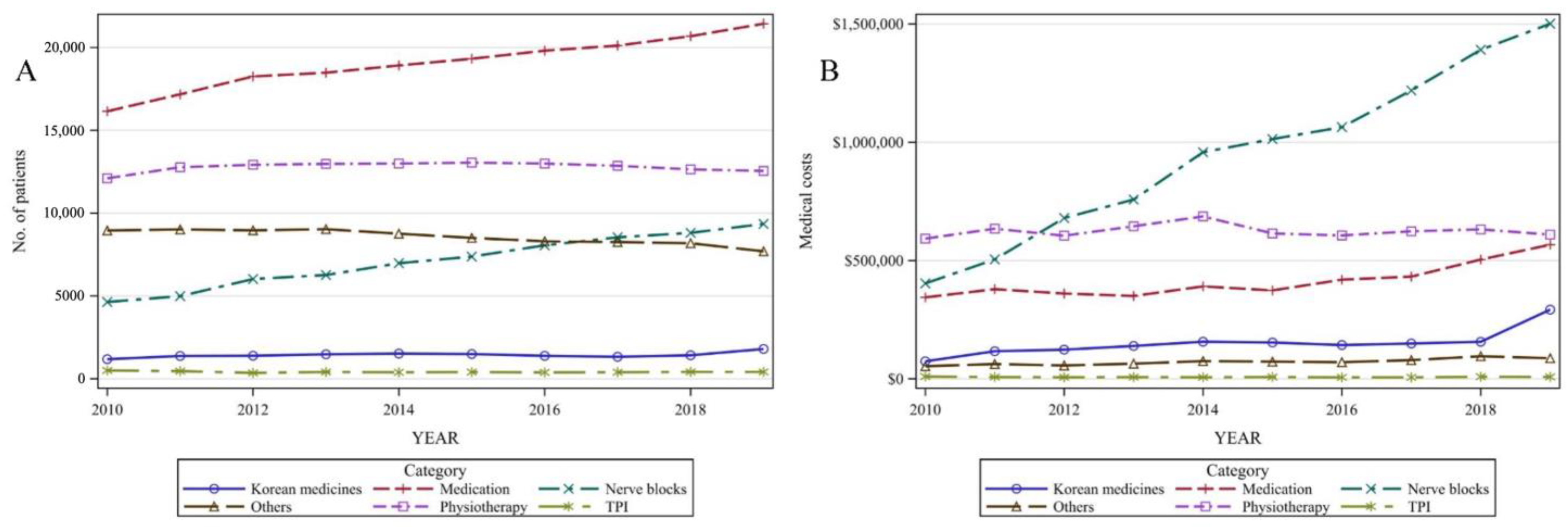
3.3. Non-surgical Treatment
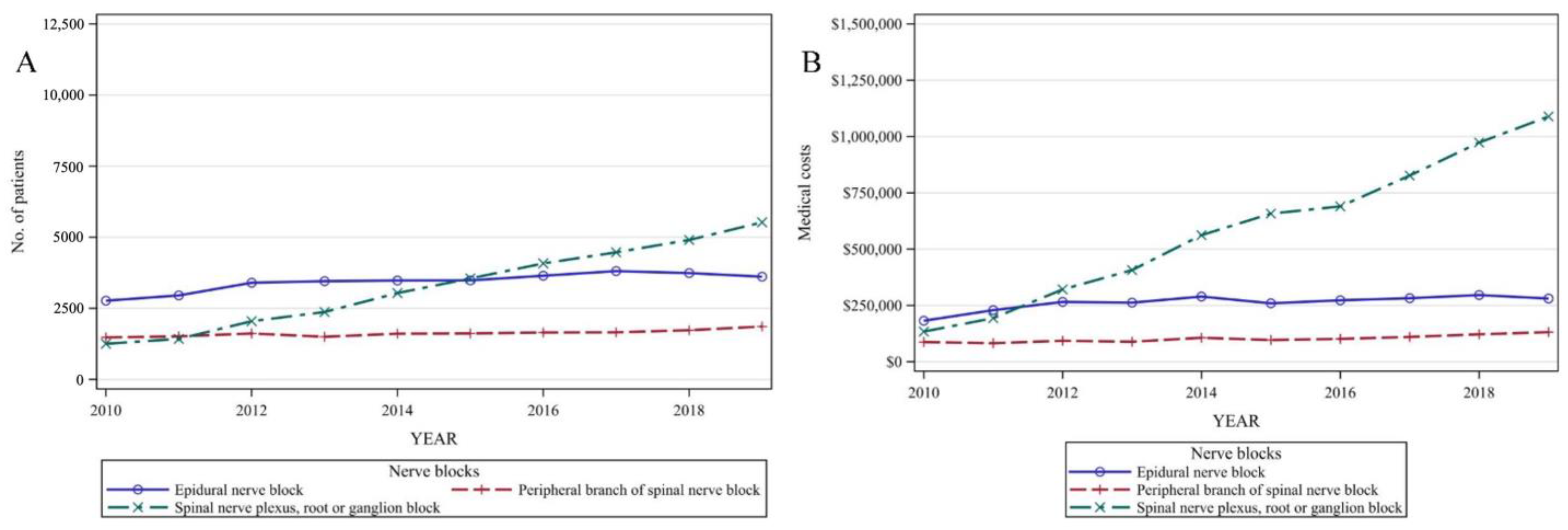
3.4. Nerve Blocks
3.5. Medication
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanaan, T.; Abusaleh, R.; Abuasbeh, J.; Al Jammal, M.; Al-Haded, S.; Al-Rafaiah, S.; Kanaan, A.; Alnaimat, F.; Khreesha, L.; Al Hadidi, F.; et al. The Efficacy of Therapeutic Selective Nerve Block in Treating Lumbar Radiculopathy and Avoiding Surgery. J. Pain Res. 2020, 13, 2971–2978. [Google Scholar] [CrossRef]
- Gugliotta, M.; da Costa, B.R.; Dabis, E.; Theiler, R.; Jüni, P.; Reichenbach, S.; Landolt, H.; Hasler, P. Surgical versus conservative treatment for lumbar disc herniation: A prospective cohort study. BMJ Open 2016, 6, e012938. [Google Scholar] [CrossRef]
- Hahne, A.J.; Ford, J.J.; McMeeken, J.M. Conservative management of lumbar disc herniation with associated radiculopathy: A systematic review. Spine 2010, 35, E488–E504. [Google Scholar] [CrossRef]
- Bruggeman, A.J.; Decker, R.C. Surgical Treatment and Outcomes of Lumbar Radiculopathy. Phys. Med. Rehabil. Clin. N Am. 2011, 22, 161–177. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, K.; Hider, S.L.; Jordan, J.L.; Lewis, M.; Dunn, K.M.; Hay, E.M. The impact of low back-related leg pain on outcomes as compared with low back pain alone: A systematic review of the literature. Clin. J. Pain 2013, 29, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.-L.; Guo, J.-B.; Zhang, H.-W.; Zhang, Y.-J.; Zhu, Y.; Zhang, J.; Hu, H.-Y.; Zheng, Y.-L.; Wang, X.-Q. Surgical versus non-operative treatment for lumbar disc herniation: A systematic review and meta-analysis. Clin. Rehabil. 2017, 32, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Li, X.; Liu, Z.; Bai, M.; Zhao, Z.; Wang, J. The study on the clinical effectiveness and safety of traditional Chinese medicine acupoint catgut embedding guided by musculoskeletal ultrasound in the treatment of nerve root sciatica: A protocol for systematic review and meta-analysis of randomized controlled trials. Medicine 2021, 100, e25387. [Google Scholar] [PubMed]
- Ahn, Y.-J.; Shin, J.-S.; Lee, J.; Lee, Y.J.; Kim, M.-R.; Park, K.B.; Lee, J.-H.; Shin, K.-M.; Ha, I.-H. Evaluation of use and cost of medical care of common lumbar disorders in Korea: Cross-sectional study of Korean Health Insurance Review and Assessment Service National Patient Sample data. BMJ Open 2016, 6, e012432. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, K.H.; Kang, S.; Kim, D.H.; Kim, D.H.; Kim, B.R.; Kim, W.; Kim, J.H.; Do, K.H.; Do, J.G.; et al. Nonsurgical treatments for patients with radicular pain from lumbosacral disc herniation. Spine J. 2019, 19, 1478–1489. [Google Scholar] [CrossRef]
- Latka, D.; Miekisiak, G.; Jarmuzek, P.; Lachowski, M.; Kaczmarczyk, J. Treatment of lumbar disc herniation with radiculopathy. Clinical practice guidelines endorsed by The Polish Society of Spinal Surgery. Neurol. I Neurochir. Pol. 2016, 50, 101–108. [Google Scholar] [CrossRef]
- Koltsov, J.C.; Smuck, M.W.; Zagel, A.; Alamin, T.F.; Wood, K.B.; Cheng, I.; Hu, S.S. Lumbar epidural steroid injections for herniation and stenosis: Incidence and risk factors of subsequent surgery. Spine J. 2019, 19, 199–205. [Google Scholar] [CrossRef]
- Bozzao, A.; Gallucci, M.; Masciocchi, C.; Aprile, I.; Barile, A.; Passariello, R. Lumbar disk herniation: MR imaging assessment of natural history in patients treated without surgery. Radiology 1992, 185, 135–141. [Google Scholar] [CrossRef]
- Ma, Z.; Yu, P.; Jiang, H.; Li, X.; Qian, X.; Yu, Z.; Zhu, Y.; Liu, J. Conservative Treatment for Giant Lumbar Disc Herniation: Clinical Study in 409 Cases. Pain Physician 2021, 24, E639–E648. [Google Scholar] [PubMed]
- Postacchini, F.; Postacchini, R. Operative Management of Lumbar Disc Herniation: The Evolution of Knowledge and Surgical Techniques in the Last Century; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Zaina, F.; Tomkins-Lane, C.; Carragee, E.; Negrini, S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Jacobs, W.C.; van Tulder, M.; Arts, M.; Rubinstein, S.M.; van Middelkoop, M.; Ostelo, R.; Verhagen, A.; Koes, B.; Peul, W.C. Surgery versus conservative management of sciatica due to a lumbar herniated disc: A systematic review. Eur. Spine J. 2011, 20, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Choi, Y.; Chung, C.K.; Kim, K.-J.; Shin, D.A.; Park, Y.-K.; Kwon, W.-K.; Yang, S.H.; Lee, C.H.; Park, S.B.; et al. Nonsurgical treatment outcomes for surgical candidates with lumbar disc herniation: A comprehensive cohort study. Sci. Rep. 2021, 11, 3931. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Hebert, J.J.; Abraham, E.; Vandewint, A.; Bigney, E.; Richardson, E.; El-Mughayyar, D.; Attabib, N.; Wedderkopp, N.; Kingwell, S.; et al. Postoperative recovery patterns following discectomy surgery in patients with lumbar radiculopathy. Sci. Rep. 2022, 12, 11146. [Google Scholar] [CrossRef]
- Brötz, D.; Maschke, E.; Burkard, S.; Engel, C.; Mänz, C.; Ernemann, U.; Wick, W.; Weller, M. Is there a role for benzodiazepines in the management of lumbar disc prolapse with acute sciatica? Pain 2010, 149, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Pangarkar, S.S.; Kang, D.G.; Sandbrink, F.; Bevevino, A.; Tillisch, K.; Konitzer, L.; Sall, J. VA/DoD Clinical Practice Guideline: Diagnosis and Treatment of Low Back Pain. J. Gen. Intern. Med. 2019, 34, 2620–2629. [Google Scholar] [CrossRef]
- Kim, L.; Kim, J.-A.; Kim, S. A guide for the utilization of Health Insurance Review and Assessment Service National Patient Samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef]
- Cohen, S.P.; Furman, M.B.; Weber, N.H.; Singh, J.R. Single Versus Two-Level Transforaminal Epidural Steroid Injection for Treating Lumbosacral Radicular Pain: What is the Evidence? PM&R 2015, 7, 883–888. [Google Scholar]
- Lee, S.M.; Han, S.K.; Kim, J.H.; Jang, B.H.; Jeong, C.R.; Sohn, H.J.; Choi, H.J.; Park, S.Y.; Jeong, C.K.; Shin, G.M.; et al. Pain release effects of injection therapy on chronic back pain-the status of Korea back pain patients and injection treatment and the long-term effects of repetitive injection treatment. Natl. Evid. Based Healthc. Collab. Agency (NECA) Res. Rep. 2009, 1, 1–231. [Google Scholar]
- Albrecht, D.S.; Ahmed, S.U.; Kettner, N.W.; Borra, R.J.; Cohen-Adad, J.; Deng, H.; Houle, T.T.; Opalacz, A.; Roth, S.A.; Melo, M.F.V.; et al. Neuroinflammation of the spinal cord and nerve roots in chronic radicular pain patients. Pain 2018, 159, 968–977. [Google Scholar] [CrossRef]
- Yu, J.; Shin, B.-C.; Kim, H.; Hyun, E.; Lee, J.-H.; Kim, M.-R.; Lim, B. The process of National Health Insurance coverage for Chuna Manual Therapy in Korea: A qualitative study. Integr. Med. Res. 2021, 11, 100746. [Google Scholar] [CrossRef]
- Berry, J.A.; Elia, C.; Saini, H.S.; Miulli, D.E. A Review of Lumbar Radiculopathy, Diagnosis, and Treatment. Cureus 2019, 11, e5934. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kim, W.; Kong, H.H.; Do, K.H.; Choi, K.H. Epidural steroid injection versus conservative treatment for patients with lumbosacral radicular pain: A meta-analysis of randomized controlled trials. Medicine 2020, 99, e21283. [Google Scholar] [CrossRef]
- Cohen, S.P.; Hanling, S.; Bicket, M.C.; White, R.L.; Veizi, E.; Kurihara, C.; Zhao, Z.; Hayek, S.; Guthmiller, K.B.; Griffith, S.R.; et al. Epidural steroid injections compared with gabapentin for lumbosacral radicular pain: Multicenter randomized double blind comparative efficacy study. BMJ 2015, 350, h1748. [Google Scholar] [CrossRef]
- Buchner, M.; Zeifang, F.; Brocai, D.R.; Schiltenwolf, M. Epidural Corticosteroid Injection in the Conservative Management of Sciatica. Clin. Orthop. Relat. Res. 2000, 375, 149–156. [Google Scholar] [CrossRef]
- Dincer, U.; Kiralp, M.Z.; Cakar, E.; Yasar, E.; Dursan, H. Caudal epidural injection versus non-steroidal anti-inflammatory drugs in the treatment of low back pain accompanied with radicular pain. Jt. Bone Spine 2007, 74, 467–471. [Google Scholar] [CrossRef]
- Horasanli, E.; Gamli, M.; Pala, Y.; Erol, M.; Sahin, F.; Dikmen, B. A Comparison of Epidural Anesthesia and Lumbar Plexus-Sciatic Nerve Blocks for Knee Surgery. Clinics 2010, 65, 29–34. [Google Scholar] [CrossRef]
- Harvey, N.R.; Wolf, B.J.; Bolin, E.D.; Wilson, S.H. Comparison of analgaesia with lumbar epidurals and lumbar plexus nerve blocks in patients receiving multimodal analgaesics following primary total hip arthroplasty: A retrospective analysis. Int. Orthop. 2017, 41, 2229–2235. [Google Scholar] [CrossRef] [PubMed]
- Jayabalan, P.; Bergman, R.B.; Huang, K.D.; Maas, M.; Welty, L. Relationship Between Socioeconomic Status and the Outcome of Lumbar Epidural Steroid Injections for Lumbar Radiculopathy. Am. J. Phys. Med. Rehabil. 2022, 102, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, A.; Miller, J.; Lubelski, D.; Nowacki, A.S.; Wells, B.J.; Milinovich, A.; Edward, C.B.; Thomas, E.M.; Michael, P.S. The Impact of Socioeconomic Status on the Utilization of Spinal Imaging. Neurosurgery 2015, 77, 746–753; discussion 753–754. [Google Scholar] [CrossRef]
- Kwon, M.A.; Shim, W.S.; Kim, M.H.; Gwak, M.S.; Hahm, T.S.; Kim, G.S.; Kim, C.S.; Choi, Y.H.; Park, J.H.; Cho, H.S.; et al. A Correlation between Low Back Pain and Associated Factors: A Study Involving 772 Patients who Had Undergone General Physical Examination. J. Korean Med Sci. 2006, 21, 1086–1091. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Lee, I.-S.; Kim, S.-Y.; Lee, H.; Park, H.-J.; Lee, H.; Kim, S.-H.; Chae, Y. Identification of determinants of the utilisation of acupuncture treatment using Andersen’s behavioural model. Acupunct. Med. 2015, 33, 129–135. [Google Scholar] [CrossRef]
- Singh, J.A.; Cleveland, J.D. Socioeconomic status and healthcare access are associated with healthcare utilization after knee arthroplasty: A U.S. national cohort study. Jt. Bone Spine 2020, 87, 157–162. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Patients | Percentage |
|---|---|---|
| Total | 234,858 | 100.00 |
| Age | ||
| 20–29 | 14,465 | 6.16 |
| 30–39 | 27,561 | 11.74 |
| 40–49 | 40,229 | 17.13 |
| 50–59 | 57,343 | 24.42 |
| 60–69 | 50,121 | 21.34 |
| ≥70 | 45,139 | 19.22 |
| Sex | ||
| Male | 97,219 | 41.39 |
| Female | 137,639 | 58.61 |
| Payer type * | ||
| NHI | 221,055 | 94.12 |
| Medicaid | 13,655 | 5.81 |
| Others | 148 | 0.06 |
| Year | 2010 | 2011 | 2012 | 2013 | 2014 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Category | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs |
| Opioids | 6468 (32.49%) | USD 47,991 | 6796 (32.04%) | USD 58,008 | 7423 (32.96%) | USD 60,484 | 7573 (32.99%) | USD 62,775 | 7726 (32.88%) | USD 77,725 |
| Non-opioid analgesics | 14,057 (70.61%) | USD 237,719 | 14,814 (69.84%) | USD 260,964 | 15,699 (69.71%) | USD 235,957 | 15,889 (69.21%) | USD 236,299 | 16,099 (68.52%) | USD 268,784 |
| Anesthetics | 3976 (19.97%) | USD 3522 | 4407 (20.78%) | USD 4495 | 5352 (23.76%) | USD 4754 | 5724 (24.93%) | USD 4921 | 6254 (26.62%) | USD 5258 |
| Gastrointestinal | 12,616 (63.37%) | USD 124,552 | 13,429 (63.31%) | USD 136,958 | 14,390 (63.89%) | USD 132,835 | 14,685 (63.97%) | USD 140,187 | 15,007 (63.88%) | USD 159,086 |
| Antipsychotic | 2716 (13.64%) | USD 15,247 | 2664 (12.56%) | USD 18,991 | 2597 (11.53%) | USD 15,358 | 2472 (10.77%) | USD 19,303 | 2430 (10.34%) | USD 26,598 |
| Antibiotics | 789 (3.96%) | USD 13,786 | 787 (3.71%) | USD 12,240 | 786 (3.49%) | USD 10,874 | 837 (3.65%) | USD 11,469 | 864 (3.68%) | USD 12,538 |
| Steroids | 4425 (22.23%) | USD 6553 | 4963 (23.40%) | USD 7407 | 5718 (25.39%) | USD 7050 | 5715 (24.89%) | USD 5578 | 5700 (24.26%) | USD 5813 |
| Others | 8626 (43.33%) | USD 164,106 | 8873 (41.83%) | USD 174,297 | 9485 (42.11%) | USD 155,872 | 9847 (42.89%) | USD 164,890 | 10,362 (44.10%) | USD 184,074 |
| Year | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
| Category | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs | No. of Patients (%) | Medical Costs |
| Opioids | 7762 (32.42%) | USD 75,213 | 7967 (32.65%) | USD 75,318 | 7978 (32.33%) | USD 78,781 | 8244 (32.57%) | USD 94,459 | 8705 (32.92%) | USD 104,940 |
| Non-opioid analgesics | 16,399 (68.49%) | USD 247,407 | 16,872 (69.14%) | USD 267,065 | 17,037 (69.05%) | USD 289,043 | 17,560 (69.39%) | USD 323,767 | 18,322 (69.29%) | USD 377,972 |
| Anesthetics | 6689 (27.94%) | USD 5107 | 7367 (30.19%) | USD 5318 | 7880 (31.94%) | USD 5917 | 8309 (32.83%) | USD 6249 | 8911 (33.70%) | USD 6711 |
| Gastrointestinal | 15,262 (63.74%) | USD 149,845 | 15,652 (64.14%) | USD 158,084 | 15,973 (64.73%) | USD 168,681 | 16,329 (64.52%) | USD 186,856 | 17,090 (64.63%) | USD 201,417 |
| Antipsychotics | 2334 (9.75%) | USD 24,539 | 2062 (8.45%) | USD 28,057 | 1937 (7.85%) | USD 27,529 | 1907 (7.54%) | USD 28,564 | 1833 (6.93%) | USD 34,020 |
| Antibiotics | 849 (3.55%) | USD 10,516 | 827 (3.39%) | USD 13,511 | 739 (2.99%) | USD 11,259 | 777 (3.07%) | USD 10,016 | 681 (2.58%) | USD 8926 |
| Steroids | 5956 (24.88%) | USD 4977 | 6361 (26.07%) | USD 5536 | 6766 (27.42%) | USD 5465 | 6899 (27.26%) | USD 5875 | 7342 (27.77%) | USD 5280 |
| Others | 10,655 (44.50%) | USD 167,309 | 11,416 (46.78%) | USD 187,091 | 11,778 (47.73%) | USD 198,196 | 12,195 (48.19%) | USD 228,621 | 11,157 (42.19%) | USD 249,625 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, S.; Lim, Y.-C.; Kim, E.-J.; Park, Y.; Ha, I.-H.; Lee, Y.-S.; Lee, Y.J. Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy in Korea: A Population-Based Cross-Sectional Study. Healthcare 2023, 11, 2353. https://doi.org/10.3390/healthcare11162353
Cho S, Lim Y-C, Kim E-J, Park Y, Ha I-H, Lee Y-S, Lee YJ. Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy in Korea: A Population-Based Cross-Sectional Study. Healthcare. 2023; 11(16):2353. https://doi.org/10.3390/healthcare11162353
Chicago/Turabian StyleCho, Sohyun, Yu-Cheol Lim, Eun-Jung Kim, Yeoncheol Park, In-Hyuk Ha, Ye-Seul Lee, and Yoon Jae Lee. 2023. "Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy in Korea: A Population-Based Cross-Sectional Study" Healthcare 11, no. 16: 2353. https://doi.org/10.3390/healthcare11162353
APA StyleCho, S., Lim, Y. -C., Kim, E. -J., Park, Y., Ha, I. -H., Lee, Y. -S., & Lee, Y. J. (2023). Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy in Korea: A Population-Based Cross-Sectional Study. Healthcare, 11(16), 2353. https://doi.org/10.3390/healthcare11162353