

Effectiveness of a Standardized Nursing Process Using NANDA International, Nursing Interventions Classification and Nursing Outcome Classification Terminologies: A Systematic Review
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Information
2.2. Search Methods
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Quality Appraisal
2.6. Data Extraction
2.7. Data Synthesis
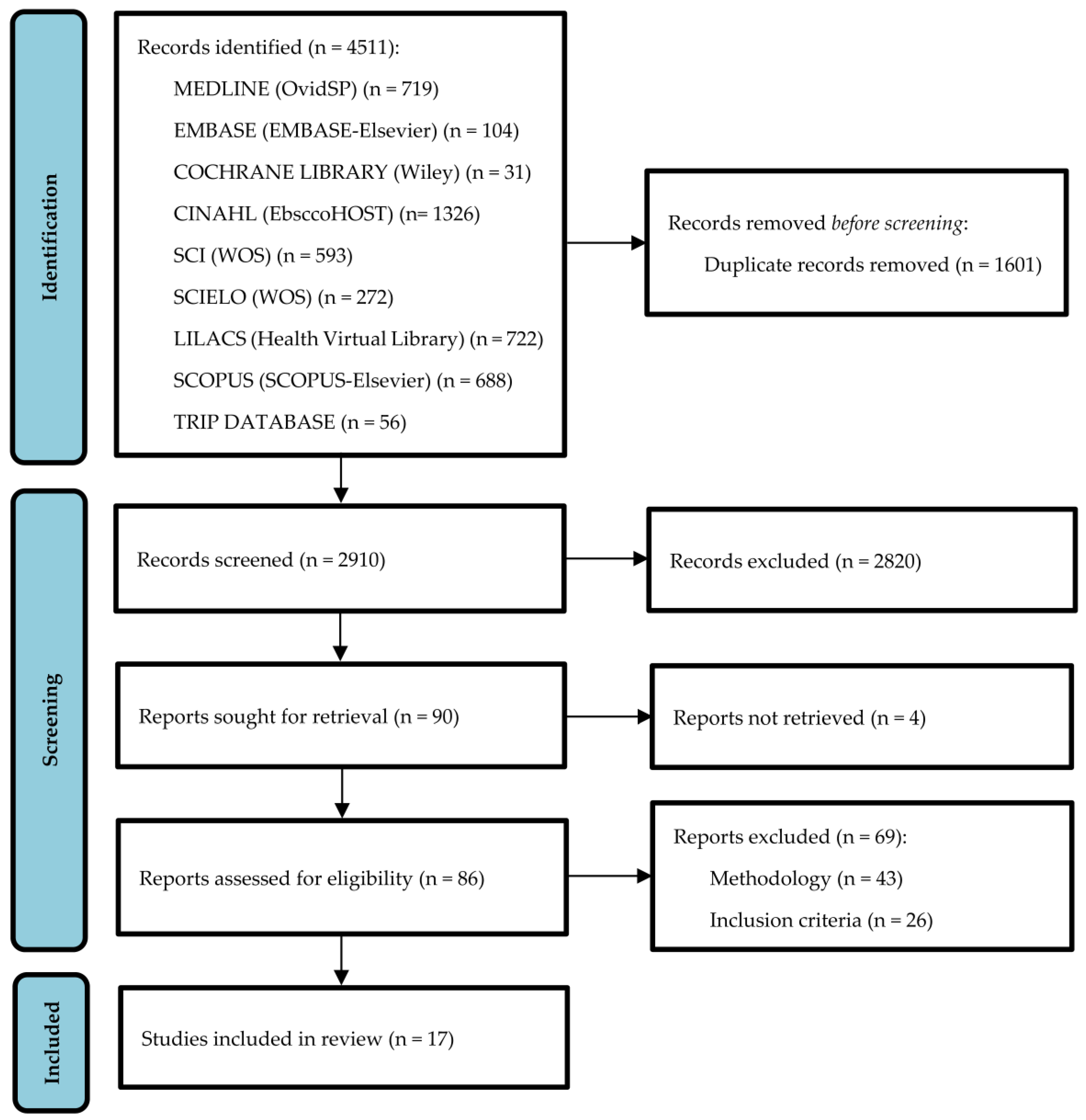
3. Results
3.1. Diagnostic Etiological Association and Accuracy of Defining Characteristics
3.2. People’s Health Outcomes

{kind=link}
| Author (Year) | Country | Methods | n | Study Period | Age |
|---|---|---|---|---|---|
| Corcoles et al. (2021) [12] | Spain | RCT | 109 | 4 months | >65 years |
| Guerra et al. (2021) [13] | Brazil | RCT | 118 | 10 months | >65 and <75 years |
| Lemos et al. (2020) [25] | Brazil | Quasi-experimental | 28 | 9 months | Non-specific |
| Rembold et al. (2020) [26] | Brazil | Case control | 239 | 6 years | >18 years |
| Silva et al. (2020) [16] | Brazil | Cohort | 93 | 1 year | >18 years |
| Bjorklund-Lima et al. (2019) [24] | Brazil | Cohort | 50 | 3 months | Non-specific |
| Pascoal et al. (2019) [17] | Brazil | Cohort | 136 | 6–10 days | <5 years |
| Silva et al. (2019) [18] | Brazil | Quasi-experimental | 101 | 1 year | >18 years |
| Vázquez-Sánchez et al. (2019) [27] | Spain | RCT | 106 | 4 months | >18 years |
| Gencbas et al. (2018) [14] | Turkey | Pseudo RCT | 62 | Non-specific | Women (non-specific) |
| Sampaio et al. (2018) [15] | Portugal | RCT | 74 | 6 months | >18 and <65 years |
| Pascoal et al. (2016) [19] | Brazil | Cohort | 163 | 6–10 days | Children (non-specific) |
| Reis and Jesus (2015) [20] | Brazil | Cohort | 271 | 5 months | Institutionalized elder patients (non-specific) |
| Pascoal et al.(2014) [21] | Brazil | Cohort | 136 | 10 days | <5 years |
| Laguna-Parras et al. (2013) [28] | Spain | Quasi-experimental | 291 | 14 months | >18 years |
| Cárdenas-Valladolid et al. (2012) [22] | Spain | Cohort | 23,488 | 2 years | Non-specific |
| Müller-Staub et al. (2008) [23] | Switzerland | RCT | 444 | 17 months | Non-specific |
| Author (Year) | Diagnostic Label | Related/Risk Factors | Effect Measures of Related/Risk Factors |
|---|---|---|---|
| Rembold et al. (2020) [26] | Risk of delayed surgical recovery (00246) | Pain | OR: 3.7 (CI: 2.04–6.65); p < 0.001 |
| Malnutrition | OR: 8 (CI: 1.96–32.60); p = 0.004 | ||
| Emotional responses recorded by nurses | OR: 5.2 (CI: 1.26–21.45); p = 0.020 | ||
| Impaired mobility | OR: 2.6 (CI: 1.42–4.71); p = 0.002 | ||
| Surgical wound infection | OR: 4.6 (CI: 2.03–10.47); p < 0.001 | ||
| Preoperative infection of surgical wound | OR: 7.6 (CI: 2.82–20.69); p < 0.001 | ||
| Prolonged surgical procedure | OR: 2.9 (CI: 1.61–5.20); p < 0.001 | ||
| Postoperative psychological disorders | OR: 6.4 (CI: 1.23–34.27); p = 0.023 | ||
| Extensive surgical procedure | OR: 1.8 (CI: 1.04–3.20); p = 0.036 | ||
| Interoperative complications | OR: 4.81 (CI: 1.55–14.92); p = 0.006 | ||
| Transfusion | OR: 4.25 (CI: 1.90–9.49); p < 0.001 | ||
| Anaemia | OR: 3.13 (CI: 1.65–5.93); p < 0.001 | ||
| Advanced cancer | OR: 2.87 (CI: 1.06–7.77); p = 0.032 | ||
| Silva et al. (2020) [16] | Dysfunctional ventilatory response to weaning (00034) | Water balance | (Pre) M: 1.64; SD: 13.04. |
| (Post) M: 13.04 SD: 13.14 | |||
| OR: 1.08 (CI: 1.03–1.12); p = 0.000 | |||
| Quantity of antibiotics administered | (Pre) M: 1.02; SD: 1.00 | ||
| (Post) M: 2.20; SD: 1.17 | |||
| OR: 2.56 (CI not reported); p = 0.000 | |||
| Age | (Pre) M: 56.85; SD: 18.48 | ||
| (Post) M: 65.76; SD: 18.53 | |||
| OR: 1.03 (CI: 1.00–1.05); p = 0.027 | |||
| Edema MI | (Pre) M: 1.02; SD: 0.94 | ||
| (Post) M: 2.39; SD: 1.56 | |||
| OR: 2.21 (CI: 1.53–3.19); p = 0.000 | |||
| Edema MS | (Pre) M: 1.23; SD: 1.02 | ||
| (Post) M: 2.34; SD: 1.56 | |||
| OR: 1.89 (CI: 1.34–2.66); p = 0.000 | |||
| Heart rate | (Pre) M: 85.73; SD: 18.07 | ||
| (Post) M: 96.42 SD: 16.40 | |||
| OR: 1.04 (CI: 1.01–1.06); p = 0.007 | |||
| Hemodialysis | (Pre) n = 8 (28.6%) | ||
| (Post) n = 20 (71.4%) | |||
| OR: 5.24 (CI: 1.98–13.83); p = 0.000 | |||
| Hyperthermia | (Pre) n = 5 (22.7%) | ||
| (Post) n = 17 (77.3%) | |||
| OR: 6.66 (CI: 2.19–20.24); p = 0.000 | |||
| Oliguria | (Pre) n = 5 (16.1%) | ||
| (Post) n = 26 (83.9%) | |||
| OR: 16.29 (CI: 5.32–49.93); p = 0.000 | |||
| Clinical severity on admission to ICU (SAPS 3) | (Pre) M: 54.52; SD: 13.13 | ||
| (Post) M: 64.39; SD: 17.06 | |||
| OR: 1.04 (CI: 1.01–1.08); p = 0.004 | |||
| Use of NIV (non-invasive ventilation) after extubation | (Pre) n = 10 (32.3%) | ||
| (Post) n = 21 (67.7%) | |||
| OR: 4.41 (CI: 1.75–11.09); p = 0.002 | |||
| Reis and Jesus (2015) [20] | Risk of falls (00155) | History of falls | (Fall) n = 59 (85.51%) |
| (No fall) n = 145 (71.78%) | |||
| OR: 2.32 (CI: 1.11–4.85); p = 0.025 | |||
| Foot problems | (Fall) n = 26 (37.68%) | ||
| (No fall) n = 40 (19.8%) | |||
| OR: 2.45 (CI: 1.35–4.44); p = 0.003 | |||
| Polypathology | (Fall) n = 19 (25.54%) | ||
| (No fall) n = 24 (11.88%) | |||
| OR: 2.82 (CI: 1.43–5.56); p = 0.002 | |||
| Wandering | (Fall) n = 46 (66.67%) | ||
| (No fall) n = 100 (49.5%) | |||
| OR: 2.04 (CI: 1.15–3.61); p = 0.014 | |||
| Cerebrovascular accident (CVA) | (Fall) n = 25 (36.23%) | ||
| (No fall) n = 48 (23.76%) | |||
| OR: 1.82 (CI: 1.01–3.28); p = 0.045 |
| Author (Year) | Diagnostic Label | Defining Characteristics | Effect Measures of the Defining Characteristics |
|---|---|---|---|
| Pascoal et al. (2019) [17] | Impaired gas exchange (00030) | Abnormal skin color | RR: 1.54 (CI: 1.08–2.20); p = 0.016 |
| Hypoxemia | RR: 135.7 (CI: 75.10–245.19); p < 0.001 | ||
| Pascoal et al. (2016) [19] | Ineffective airway clearance (00031) | Change in respiratory rate | OR: 2.88 (CI: 1.34–6.19); p = 0.007 |
| Cyanosis | OR: 0.03 (CI: 0.006–0.19); p < 0.001 | ||
| Difficulty vocalizing | OR: 10.04 (CI: 2.38–42.35); p = 0.002 | ||
| Open eyes | OR: 68.73 (CI: 1.53–3086.70); p < 0.001 | ||
| Adventitious lung sounds | OR: 300.58 (CI: 43.67–2068.86); p < 0.001 | ||
| Reduced breathing sounds | OR: 9.008 (CI: 2.75–29.48); p < 0.001 | ||
| Ineffective cough | OR: 129.53 (CI: 33.40–502.19); p < 0.001 | ||
| Pascoal et al. (2014) [21] | Ineffective respiratory pattern (00032) | Altered respiratory depth | OR: 73.32 (CI: 15.45–347.79); p < 0.001 |
| Anteroposterior diameter increase | OR: 31.56 (CI: 7.20–138.34); p < 0.001 | ||
| Altered chest movements | OR: 259.14 (CI: 31.41–2137.92); p < 0.001 | ||
| Orthopnea | OR: 30.14 (CI: 4.49–202.43); p < 0.001 | ||
| Tachypnea | OR: 5.89 (CI: 2.02–17.11); p = 0.001 | ||
| Use of accessory muscles for breathing | OR: 2595.06 (CI: 343.88–19,583.3); p < 0.001 |
| Author (year) | General Aspect Assessed | Indicator of Effectiveness | Effect Measures |
|---|---|---|---|
| Cárdenas-Valladolid et al. (2012) [22] | Care planning using NNN | Reduction in DAT in the IG | N: 4354 (Initial) M:76; SD: 10 (Final) M: 75; SD: 9 (Difference) M: −1.45; SD: 11 (AE) M: −0.33; IC: −0.63–0.04; p = 0.02 |
| Reduction in HbA1c (<7%) in the IG | Initial: 47.6% 24 months: 55.2% Change: 7.6% p < 0.01 | ||
| Reduction in SAT (<130 mmhg) in the CG | Initial: 31.6% 24 months: 35.5% Change: 3.9% p < 0.01 | ||
| Müller-Staub et al. (2008) [23] | Nurses’ clinical reasoning | NANDA-I | Pre (IG) M: 2.69; SD: 0.9 Post (IG) M: 3.7; SD: 0.54 p < 0.0001 |
| Pre (CG) M: 3.13; SD: 0.89 Post (CG) M: 2.97: SD: 0.8 p = 0.17 | |||
| NIC | Pre (IG) M: 2.33: SD: 0.93 Post (IG) M: 3.88; SD: 0.35 p < 0.0001 | ||
| Pre (CG) M: 2.7; SD: 0.88 Post (CG) M: 2.46; SD: 0.95 p = 0.05 | |||
| NOC | Pre (IG) M: 1.53; SD: 1.08 Post (IG) M: 3.77; SD: 0.53 p < 0.0001 | ||
| Pre (CG) M: 2.02; SD: 1.27 Post (CG) M: 1.94; SD: 1.06 p = 0.62 |
| Author (Year) | NNN Interrelationship | Indicator of Effectiveness | Effect Measure |
|---|---|---|---|
| Corcoles et al. (2021) [12] | NANDA-I Functional urinary incontinence (00020) NIC Urinary habit training (0600) NOC Urinary continence (0502) | 3 months: Continence | No: 25.5% (IG) and 47.2% (CG) Yes: 74.5% (IG) and 52.8% (CG) RR = 0.54 (CI: 0.31–0.94); p = 0.022; NNT: 5 |
| 3 months: Diurnal incontinence episodes | (CG) M: 1.54; SD: 2.26 (IG) M: 0.31; SD: 0.76 p = 0.002 | ||
| 3 months: Nocturnal incontinence episodes | (CG) M: 0.79; SD: 1.29 (IG) M: 0.21; SD: 0.5 p = 0.012 | ||
| 6 months: Continence | No: 25.5% (IG) and 49% (CG) Yes: 74.5% (IG) and 51% (CG) RR = 0.52 (CI: 0.3–0.9); p = 0.014; NNT: 4 | ||
| 6 months: Diurnal incontinence episodes | (CG) M: 1.8; SD: 2.51 (IG) M: 0.54; SD: 1.46 p = 0.007 | ||
| 6 months: Nocturnal incontinence episodes | (CG) M: 0.9; SD: 1.47 (IG) M: 0.35; SD: 0.86 p = 0.016 | ||
| Guerra et al. (2021) [13] | NANDA-I Risk of falls (00155) NIC Fall prevention (6490) | Decreased incidence of falls |
|
| Cause of fall: difficulty walking | (IG) 0.0% versus (CG) 10.0%; p = 0.013 | ||
| Place where fall occurred: living room | (IG) 0.0% versus (CG) 13.3%; p = 0.004 | ||
| Lemos et al. (2020) [25] | NANDA-I Ineffective health management (00078) NIC
| Knowledge: heart failure management | (1st assessment) M: 2.05; SD: 0.28 (2nd assessment) M: 2.54; SD: 0.30 (Difference) M: 0.48; SD: 0.21 p = 0.002 |
| Knowledge: diabetes management | (1st assessment) M: 2.61; SD: 0.55 (2nd assessment) M: 3.21; SD: 0.57 (Difference) M: 0.59; SD: 0.20 p = 0.000 | ||
| Bjorklund-Lima et al. (2019) [24] | NANDA-I Risk of perioperative postural injury (00087) NOC
| Measurement at five timepoints: mean scores in most NOCs decreased at timepoint 2 (T2-assessment in the operating room at the end of surgery) compared with timepoint 1 (T1-preoperative) | Most NOC showed improvement (p < 0.001) in postoperative time score (T3, T4 and T5) compared with T2 |
| NOC Consequences of immobility: physiological (0204) | T1 (M: 5.0; SD: 0.0), T2 (M: 4.0; SD: 0.0), T3 (M: 4.24; SD: 0.06), T4 (M: 4.80; SD: 0.05), T5 (M: 4.86; SD: 0.04); p < 0.001 | ||
| NOC Severity of blood loss (0413) | T1 (M: 4.59; SD: 0.04), T2 (M: 4.59; SD: 0.07), T3 (M: 4.58; SD: 0.09), T4 (M: 4.32 (SD: 4.32; SD: 0.10) T5 (M: 4.45; SD: 0.08); p = 0.014 | ||
| NOC Circulatory status (0401) | T1 (M: 4.59: SD: 0.06), T2 (M: 4.68; SD: 0.04), T3 (M: 4.41; SD: 0.07), T4 (M: 4.65; SD: 0.06), T5 (M: 4.43; SD: 0.08); p = 0.002 | ||
| NOC Tissue perfusion: cellular (0416) | T1 (M: 4.94; SD: 0.02), T2 (M: 4.68; SD: 0.05), T3 (M: 4.67; SD: 0.05), T4 (M: 4.68; SD: 0.04), T5 (M: 4.70; SD: 0.04); p < 0.001 | ||
| NOC Tissue perfusion: peripheral (0407) | T1 (M: 4.92; SD: 0.03), T2 (M: 4.31; SD: 0.09), T3 (M: 4.42; SD: 0.08), T4 (M: 4.58; SD: 0.06), T5 (M: 4.58; SD: 0.08); p < 0.001 | ||
| NOC Thermoregulation (0800) | T1 (M: 4.69; SD: 0.05), T2 (M: 4.69; SD: 0.05), T3 (M: 4.45; SD: 0.08), T4 (M: 4.86; SD: 0.03), T5 (M: 4.73; SD: 0.05); p < 0.001 | ||
| NOC Neurological status: peripheral (0917) | T1 (M: 4.96; SD: 0.03), T2 (M: 3.98; SD: 0.18), T3 (M: 4.39; SD: 0.15), T4 (M: 4.65; SD: 0.12), T5 (M: 4.76; SD: 0.11); p < 0.001 | ||
| NOC Tissue integrity: skin and mucous membranes (1101) | T1 (M: 4.93; SD: 0.02), T2 (M: 4.30; SD: 0.05), T3 (M: 4.50; SD: 0.05), T4 (M: 4.69; SD: 0.04), T5 (M: 4.71; SD: 0.04); p < 0.001 | ||
| Silva et al. (2019) [18] | NANDA-I Ineffective airway clearance (00031) NIC
Respiratory status (0415) | NIC Cough enhancement (3250): Respiratory rate | PR = 0.39 (CI: 0.81–0.98); p = 0.005 |
| NIC Cough enhancement (3250): Adventitious respiratory sounds | PR = 2.20 (CI: 2.55–8.11); p = 0.021 | ||
| NIC Cough enhancement (3250): Thoracic surgery patients: improvement in ability to eliminate secretions | PR = 4.55 (CI: 1.13–20.87); p = 0.0001 | ||
| NIC Cough enhancement (3250): Thoracic surgery patients: increase in ability to cough | PR = 4.75 (CI: 2.55–8.11); p = 0.024 | ||
| NIC Cough enhancement (3250): Abdominal surgery patients: reduction in the presence of dyspnea in mild exertion | PR = 0.38 (CI: 0.62–0.90); p = 0.022 | ||
| NIC Cough enhancement (3250): Abdominal surgery patients: decrease in changes in respiratory rate | PR = 0.25 (CI: 0.10–0.60); p = 0.001 | ||
| NIC Cough enhancement (3250): Abdominal surgery patients: decrease in nasal flaring | PR = 0.06 (CI: 0.006–0.74); p = 0.040 | ||
| NIC Cough enhancement (3250): Abdominal surgery patients: decrease in inspiration depth | PR = 0.45 (CI: 0.21–0.92); p = 0.028 | ||
| NIC Cough enhancement (3250): Abdominal surgery patients: improvement in adventitious respiratory sounds | PR = 2.82 (CI: 1.06–7.49); p = 0.031 | ||
| NIC Ventilation support (3390): Improvement in ability to eliminate secretions | PR = 0.14 (CI: 0.35–0.58); p = 0.009 | ||
| NIC Ventilation support (3390): Improvement in respiratory rate | PR = 0.43 (CI: 0.19–0.95); p = 0.034 | ||
| Ventilation support (3390): Improvement in inspiration depth | PR = 0.44 (CI: 0.20–0.97); p = 0.040 | ||
| NIC Ventilation support (3390): Abdominal surgery patients: decrease in use of accessory muscles | PR = 0.41 (CI: 0.16–1.007); p = 0.046 | ||
| NIC Airway management (3140): Decrease in accumulation of sputum | PR = 0.15 (CI: 0.30–0.76); p = 0.036 | ||
| NIC Airway management (3140): Improvement in adventitious respiratory sounds | PR = 0.14 (CI: 0.24–0.90); p = 0.047 | ||
| Vázquez-Sánchez et al. (2019) [27] | NANDA-I Nutritional imbalance: lower than body needs (00002) NIC Nutritional assessment (5246) NOC
| NIC increased NOC indicator score: prescribed diet | IG: 1.57 vs. CG: 0.22; p < 0.001 |
| NOC indicator: prescribed diet | Correlated with BMI (r = −0.34; p = 0.001), with Barthel index score (r = 0.50; p < 0.001) and with MUST questionnaire score (r = 0.28; p = 0.007) | ||
| Intervention increased NOC indicator score NOC: select foods and liquids compatible with prescribed diet. | IG: 1.20 vs. CG: 0.26; p < 0.001 | ||
| NOC indicator: select foods and liquids compatible with prescribed diet | Correlated with BMI score (r = 0.34; p = 0.001), with Barthel index score (r = 0.27; p = 0.008) and with MUST questionnaire score (r = −0.22; p = 0.018) | ||
| Gencbas et al. (2018) [14] | NANDA-I Impaired urinary elimination (00016) NIC
| In the IG, NIC had the effect of improving all NOC scores following the intervention | |
| NIC Urinary bladder training (0570) (n = 7) | NOC Urinary continence (Pre) M: 2.93; SD: 3.72 (Post) M: 4.41; SD: 0.24 (Difference) M: 1.48 | ||
| NOC Urinary elimination (Pre) M: 3.04; SD: 0.41 (Post) M: 4.49; SD: 0.22 (Difference) M: 1.45 | |||
| NIC Urinary elimination management (0590) (n = 32) | NOC Self-care: use of the toilet: Pre (M: 3.01; SD: 1.09); Post (M: 4.08; SD: 1.41); Difference M: 1.07 | ||
| NOC Urinary continence: Pre (M: 3.24; SD: 0.44); Post (M: 4.44; SD: 0.37); Difference M: 1.2 | |||
| NOC Urinary elimination: Pre (M: 3.23; SD: 0.46); Post (M: 4.59; SD: 0.22); Difference M: 1.36 | |||
| NIC Urinary habit training (0600) (n = 31) | NOC Urinary continence: Pre (M: 3.24; SD: 0.45); Post M: 4.45; SD: 0.37); Difference M: 1.21 | ||
| NOC Urinary elimination: Pre (M: 3.22; SD: 0.46); Post (M: 4.58; SD: 0.22); Difference M: 1.36 | |||
| NIC Help with self-care: urination/defecation (1804) (n = 29) | NOC Self-care: use of the toilet: Pre (M: 3.32; SD: 0.49); Post (M: 4.50; SD: 0.49); Difference M: 1.18 | ||
| NOC Urinary continence: Pre (M: 3.20; SD: 0.44); Post (M: 4.43; SD: 0.37); Difference M: 1.23 | |||
| NIC Environmental management (6480) (n = 29) | NOC Self-care: use of the toilet: Pre (M: 3.32; SD: 0.49); Post (M: 4.50; SD: 0.49); Difference M: 1.18 | ||
| NOC Urinary continence: Pre (M: 3.20; SD: 0.44); Post (M: 4.43; SD: 0.37); Difference M: 1.23 | |||
| NOC Urinary elimination: Pre (M: 3.17; SD: 0.44); Post (M: 4.57; SD: 0.22); Difference M: 1.4 | |||
| NIC Pelvic floor exercises (0560) (n = 32) | NOC Urinary continence: Pre (M: 3.24; SD: 0.44); Post (M: 4.44; SD: 0.37); Difference M: 1.2 | ||
| NOC Urinary elimination: Pre (M: 3.23; SD: 0.46); Post (M: 4.59; SD: 0.22); Difference M: 1.36 | |||
| NIC Urinary incontinence care (0610) (n = 32) | NOC Urinary continence: Pre (M: 3.24; SD: 0.44); Post (M: 4.44; SD: 0.37); Difference M: 1.2 | ||
| NOC Urinary elimination: Pre (M: 3.23; SD: 0.46); Post (M: 4.59; SD: 0.22); Difference M: 1.36 | |||
| NOC Tissue integrity: skin and mucous membranes: Pre (M: 4.10; SD: 0.75); Post M: 4.93; SD: 0.06); Difference M: 0.83 | |||
| NIC Teaching: prescribed medication (5616) (n = 7) | NOC Response to medication: Pre (M: 4.19; SD: 0.81); Post (M: 4.89; SD: 0.90); Difference M: 0.70 | ||
| NIC Urinary retention care (0620) (n = 7) | NOC Urinary continence: Pre (M: 3.12; SD: 0.26); Post (M: 4.48; SD: 0.21); Difference M: 1.36 | ||
| Sampaio et al. (2018) [15] | NANDA-I Anxiety (00146) NIC
| Favorable effect of the NIC on the NOC score | NOC Level of anxiety (d = 1.11) NOC Self-control of anxiety (d = 1.65) |
| Being part of the IG predicts level of anxiety | 22.8% (R2 adjusted: 0.228) Posttest (F (1.58) = 18.40); p < 0.001 | ||
| Moderate positive association between the variable “group” and the NOC Level of anxiety total score (1211) (posttest) | Β = 0.49 | ||
| Being part of the IG predicts self-control of anxiety | 40% (R2 adjusted = 0.400) Posttest (F (1.58) = 40.27; p < 0.001) | ||
| Moderate positive association between the variable “group” and total score in NOC Self-control of anxiety (posttest) | Β = 0.64 | ||
| NOC Level of anxiety (1211): mean differences by groups pre and post intervention |
| ||
| NOC Self-control of anxiety (1402): Mean differences by groups pre and post intervention |
| ||
| Laguna-Parras et al. (2013) [28] | NANDA-I Sleep pattern disorder (00198) NIC Sleep improvement (1850) NOC Sleep (0004) | Oviedo Sleep Questionnaire: Satisfaction with sleep | (Admission) M: 3.27; SD: 1.51 (Discharge) M: 5.19; SD: 1.3 (Difference) M: 1.921; SD: 1.781; (CI: 1.71–2.12) p < 0.0001 |
| Oviedo Sleep Questionnaire: Insomnia | (Admission) M: 23.52; SD: 9.05 (Discharge) M: 15.93; SD: 8.25 (Difference) M: −7.59; SD: 10.95 (CI: 6.31–8.86) p < 0.0001 | ||
| Oviedo Sleep Questionnaire: Hypersomnia | (Admission) M: 5.97; SD: 3.76 (Discharge) M: 4.49; SD: 2.55 (Difference) M: −1.479; SD: 3.82 (CI: 1.03–1.92) p < 0.0001 | ||
| NOC Sleep (0004) | (Admission) M: 1.36; SD: 0.56 (Discharge) M: 3.84; SD: 0.68 (Difference) M: 2.48; SD: 0.84 (CI: 2.38–2.58) p < 0.0001 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanson, G.; Vellone, E.; Kangasniemi, M.; Alvaro, R.; D’Agostino, F. Impact of nursing diagnoses on patient and organisational outcomes: A systematic literature review. J. Clin. Nurs. 2017, 26, 3764–3783. [Google Scholar] [CrossRef]
- Ramírez Elías, A. Proceso de enfermería; lo que sí es y lo que no es. Enfermería Univ. 2016, 13, 71–72. [Google Scholar] [CrossRef]
- Hakverdioğlu Yönt, G.; Korhan, E.A.; Erdemir, F.; Müller-Staub, M. Nursing Diagnoses Determined by First Year Students: A Vignette Study. Int. J. Nurs. Knowl. 2014, 25, 39–42. [Google Scholar] [CrossRef]
- D’Agostino, F.; Zeffiro, V.; Vellone, E.; Ausili, D.; Belsito, R.; Leto, A.; Alvaro, R. Cross-Mapping of Nursing Care Terms Recorded in Italian Hospitals into the Standardized NNN Terminology. Int. J. Nurs. Knowl. 2020, 31, 4–13. [Google Scholar] [CrossRef]
- Herdman, T.; Kamitsuru, S.; Takáo Lopes, C. NANDA International Nursing Diagnoses. Definitions and Classification, 2021–2023, 12th ed.; Thieme: New York, NY, USA, 2021. [Google Scholar]
- Butcher, H.K.; Bulechek, G.M.; Dochterman, J.M.; Wagner, C.M. Clasificación de Intervenciones de Enfermería (NIC), 7th ed.; Elsevier España, S.L.U.: Barcelona, Spain, 2019. [Google Scholar]
- Moorhead, S.; Swanson, E.A.; Johnson, M.; Maas, M. Nursing Outcomes Classification (NOC): Measurement of Health Outcomes; Elsevier: St Louis, MO, USA, 2018. [Google Scholar]
- Tastan, S.; Linch, G.C.; Keenan, G.M.; Stifter, J.; McKinney, D.; Fahey, L.; Lopez, K.D.; Yao, Y.; Wilkie, D.J. Evidence for the existing American Nurses Association-recognized standardized nursing terminologies: A systematic review. Int. J. Nurs. Stud. 2014, 51, 1160–1170. [Google Scholar] [CrossRef]
- Chae, S.; Oh, H.; Moorhead, S. Effectiveness of Nursing Interventions using Standardized Nursing Terminologies: An Integrative Review. West. J. Nurs. Res. 2020, 42, 963–973. [Google Scholar] [CrossRef]
- Zhang, T.; Wu, X.; Peng, G.; Zhang, Q.; Chen, L.; Cai, Z.; Ou, H. Effectiveness of Standardized Nursing Terminologies for Nursing Practice and Healthcare Outcomes: A Systematic Review. Int. J. Nurs. Knowl. 2021, 32, 220–228. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Córcoles-Jiménez, M.-P.; Candel-Parra, E.; del Egido-Fernández, M.; Villada-Munera, A.; Moreno-Moreno, M.; Piña-Martínez, A.-J.; Jiménez-Sánchez, M.-D.; Azor-García, R.-J. Preventing Functional Urinary Incontinence in Hip-Fractured Older Adults Through Patient Education: A Randomized Controlled Trial. J. Appl. Gerontol. 2021, 40, 890–901. [Google Scholar] [CrossRef]
- Guerra, F.V.G.; Moreira, R.P.; Ferreira, G.d.O.; Felício, J.F.; Cavalcante, T.F.; de Araujo, T.L.; de Araujo, M.F.M. Effectiveness of the fall prevention intervention in older adults with arterial hypertension: Randomized clinical trial. Geriatr. Nurs. 2021, 42, 27–32. [Google Scholar] [CrossRef]
- Gencbas, D.; Bebis, H.; Cicek, H. Evaluation of the Efficiency of the Nursing Care Plan Applied Using NANDA, NOC, and NIC Linkages to Elderly Women with Incontinence Living in a Nursing Home: A Randomized Controlled Study. Int. J. Nurs. Knowl. 2018, 29, 217–226. [Google Scholar] [CrossRef]
- Sampaio, F.M.C.; Araújo, O.; Sequeira, C.; Lluch Canut, M.T.; Martins, T. A randomized controlled trial of a nursing psychotherapeutic intervention for anxiety in adult psychiatric outpatients. J. Adv. Nurs. 2018, 74, 1114–1126. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.C.R.; da Tonelli, I.S.; Oliveira, R.C.C.; Lemos, P.L.; Matos, S.S.; de Chianca, T.C.M. Clinical study of Dysfunctional Ventilatory Weaning Response in critically ill patients. Rev. Lat. Am. Enferm. 2020, 28, e3334. [Google Scholar] [CrossRef]
- Pascoal, L.M.; Lopes, M.V.d.O.; Chaves, D.B.R.; Beltrão, B.A.; Nunes, M.M.; da Silva, V.M.; Freire, V.E.C.d.S. Impaired Gas Exchange: Prognostic Clinical Indicators of Short-Term Survival in Children with Acute Respiratory Infection. Int. J. Nurs. Knowl. 2019, 30, 87–92. [Google Scholar] [CrossRef]
- Da Silva, L.F.M.; Pascoal, L.M.; Nunes, S.F.L.; Freire, V.E.C.D.S.; Almeida, A.G.A.; Gontijo, P.V.C.; Neto, M.S. Ineffective Airway Clearance in Surgical Patients: Evaluation of Nursing Interventions and Outcomes. Int. J. Nurs. Knowl. 2019, 30, 251–256. [Google Scholar] [CrossRef]
- Pascoal, L.M.; Lopes, M.V.d.O.; da Silva, V.M.; Beltrão, B.A.; Chaves, D.B.R.; Herdman, T.H.; Lira, A.L.B.d.C.; Teixeira, I.X.; Costa, A.G.d.S. Clinical indicators of ineffective airway clearance in children with acute respiratory infection. J. Child. Health Care 2016, 20, 324–332. [Google Scholar] [CrossRef]
- dos Reis, K.M.C.; de Jesus, C.A.C. Cohort study of institutionalized elderly people: Fall risk factors from the nursing diagnosis. Rev. Lat. Am. Enferm. 2015, 23, 1130–1138. [Google Scholar] [CrossRef]
- Pascoal, L.M.; Lopes, M.V.d.O.; da Silva, V.M.; Beltrão, B.A.; Chaves, D.B.R.; de Santiago, J.M.V.; Herdman, T.H. Ineffective Breathing Pattern: Defining Characteristics in Children With Acute Respiratory Infection. Int. J. Nurs. Knowl. 2014, 25, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas-Valladolid, J.; Salinero-Fort, M.A.; Gómez-Campelo, P.; de Burgos-Lunar, C.; Abánades-Herranz, J.C.; Arnal-Selfa, R.; Andrés, A.L. Effectiveness of Standardized Nursing Care Plans in Health Outcomes in Patients with Type 2 Diabetes Mellitus: A Two-Year Prospective Follow-Up Study. Dasgupta K, editor. PLoS ONE 2012, 7, e43870. [Google Scholar] [CrossRef]
- Müller-Staub, M.; Needham, I.; Odenbreit, M.; Lavin, M.A.; van Achterberg, T. Implementing nursing diagnostics effectively: Cluster randomized trial. J. Adv. Nurs. 2008, 63, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Bjorklund-Lima, L.; Müller-Staub, M.; E Cardozo, M.C.; Bernardes, D.S.; Rabelo-Silva, E.R. Clinical indicators of nursing outcomes classification for patient with risk for perioperative positioning injury: A cohort study. J. Clin. Nurs. 2019, 28, 4367–4378. [Google Scholar] [CrossRef]
- Lemos, D.M.P.; Saldanha, P.F.; Vieira, L.F.; Azzolin, K.d.O. Nursing taxonomies in hospital discharge planning: A quasi-experimental study. Rev. Bras. Enferm. 2020, 73, e20180896. [Google Scholar] [CrossRef] [PubMed]
- Rembold, S.M.; Santana, R.F.; Oliveira Lopes, M.V.; Melo, U.G. Nursing Diagnosis Risk for Delayed Surgical Recovery (00246) in Adult and Elderly: A Case-Control Study. Int. J. Nurs. Knowl. 2020, 31, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Sánchez, M.Á.; Valero-Cantero, I.; Carrión-Velasco, Y.; Castro-López, P.; Suárez-Cadenas, E.; Casals, C. Applicability and Clinical Validity of Nursing Outcomes Classification in a Nursing Intervention of Nutritional Counseling for Patients With Malnutrition. Int. J. Nurs. Knowl. 2019, 30, 168–172. [Google Scholar] [CrossRef]
- Laguna-Parras, J.M.; Jerez-Rojas, M.R.; García-Fernández, F.P.; Carrasco-Rodríguez, M.D.; Nogales-Vargas-Machuca, I. Effectiveness of the ‘sleep enhancement’ nursing intervention in hospitalized mental health patients. J. Adv. Nurs. 2013, 69, 1279–1288. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Müller-Staub, M.; Lavin, M.A.; Needham, I.; van Achterberg, T. Nursing diagnoses, interventions and outcomes? application and impact on nursing practice: Systematic review. J. Adv. Nurs. 2006, 56, 514–531. [Google Scholar] [CrossRef]
- Freire, V.E.S.; Lopes, M.V.; Keenan, G.M.; Lopez, K.D. Nursing students’ diagnostic accuracy using a computer-based clinical scenario simulation. Nurse Educ. Today 2018, 71, 240–246. [Google Scholar] [CrossRef]
- Collins, A. Effect of Continuing Nursing Education on Nurses’ Attitude Toward and Accuracy of Nursing Diagnosis. Int. J. Nurs. Knowl. 2013, 24, 122–128. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Suárez, C.-A.; González-de la Torre, H.; Hernández-De Luis, M.-N.; Fernández-Gutiérrez, D.-Á.; Martínez-Alberto, C.-E.; Brito-Brito, P.-R. Effectiveness of a Standardized Nursing Process Using NANDA International, Nursing Interventions Classification and Nursing Outcome Classification Terminologies: A Systematic Review. Healthcare 2023, 11, 2449. https://doi.org/10.3390/healthcare11172449
Rodríguez-Suárez C-A, González-de la Torre H, Hernández-De Luis M-N, Fernández-Gutiérrez D-Á, Martínez-Alberto C-E, Brito-Brito P-R. Effectiveness of a Standardized Nursing Process Using NANDA International, Nursing Interventions Classification and Nursing Outcome Classification Terminologies: A Systematic Review. Healthcare. 2023; 11(17):2449. https://doi.org/10.3390/healthcare11172449
Chicago/Turabian StyleRodríguez-Suárez, Claudio-Alberto, Héctor González-de la Torre, María-Naira Hernández-De Luis, Domingo-Ángel Fernández-Gutiérrez, Carlos-Enrique Martínez-Alberto, and Pedro-Ruymán Brito-Brito. 2023. "Effectiveness of a Standardized Nursing Process Using NANDA International, Nursing Interventions Classification and Nursing Outcome Classification Terminologies: A Systematic Review" Healthcare 11, no. 17: 2449. https://doi.org/10.3390/healthcare11172449
APA StyleRodríguez-Suárez, C.-A., González-de la Torre, H., Hernández-De Luis, M.-N., Fernández-Gutiérrez, D.-Á., Martínez-Alberto, C.-E., & Brito-Brito, P.-R. (2023). Effectiveness of a Standardized Nursing Process Using NANDA International, Nursing Interventions Classification and Nursing Outcome Classification Terminologies: A Systematic Review. Healthcare, 11(17), 2449. https://doi.org/10.3390/healthcare11172449