
Strength and Bioelectrical Activity of the Pelvic Floor Muscles and Sexual Function in Women with and without Stress Urinary Incontinence: An Observational Cross-Sectional Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Period of Study
2.3. Population
2.4. Eligibility Criteria
2.5. Sampling
2.6. Sample
2.7. Data Collection and Variables
2.8. Primary Outcomes
2.9. Secondary Outcomes
2.10. Level of Strength of the PFM
2.11. Bioelectrical Activity of the PFM
2.12. Sexual Function
2.13. Severity of Urinary Loss and Impact on Daily Life
2.14. Impact of SUI on Quality of Life
2.15. Statistical Analysis
3. Results
3.1. Comparison among the Control and SUI groups
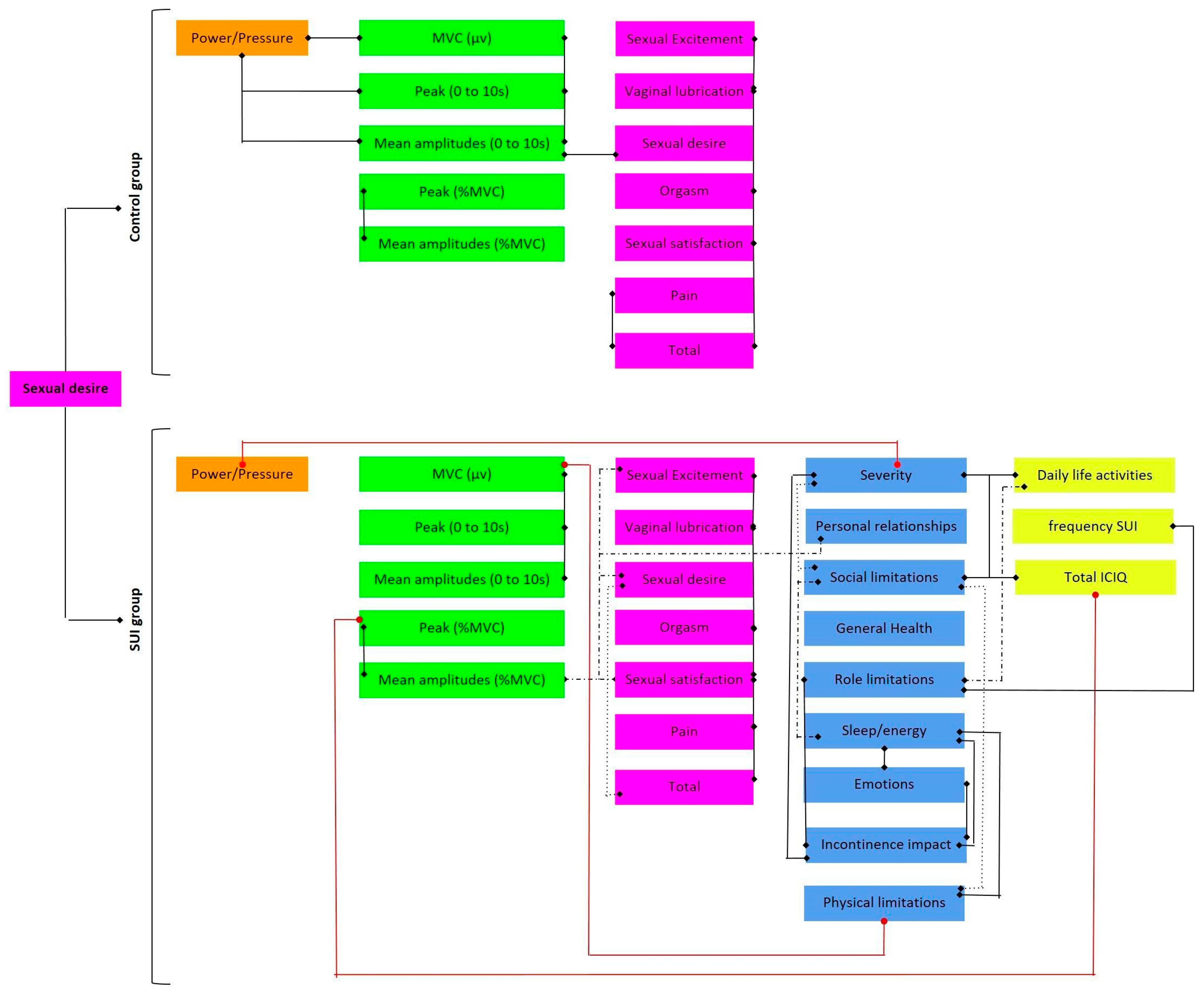
3.2. Correlations among Variables in the Control Group
3.3. Correlations among Variables in the SUI Group
4. Discussion
5. Limitation of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aoki, Y.; Brown, H.W.; Brubaker, L.; Cornu, J.N.; Daly, J.O.; Cartwright, R. Urinary incontinence in women. Nat. Rev. Dis. Prim. 2017, 3, 17042. [Google Scholar] [CrossRef] [Green Version]
- Mazur-Bialy, A.I.; Kołomańska-Bogucka, D.; Nowakowski, C.; Tim, S. Urinary incontinence in women: Modern methods of physiotherapy as a support for surgical treatment or independent therapy. J. Clin. Med. 2020, 9, 1211. [Google Scholar] [CrossRef] [Green Version]
- Lim, R.; Liong, M.L.; Leong, W.S.; Khan, N.A.K.; Yuen, K.H. Effect of stress urinary incontinence on the sexual function of couples and the quality of life of patients. J. Urol. 2016, 196, 153–158. [Google Scholar] [CrossRef]
- Preda, A.; Moreira, S. Stress urinary incontinence and female sexual dysfunction: The role of pelvic floor rehabilitation. Acta Med. Port. 2019, 32, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Pizzol, D.; Demurtas, J.; Celotto, S.; Maggi, S.; Smith, L.; Angiolelli, G.; Trott, M.; Yang, L.; Veronese, N. Urinary incontinence and quality of life: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 25–35. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Kucab–Klich, K.; Błaszczak, E.; Kwaśna, K.; Smykla, A.; Hudziak, D.; Dolibog, P. Electromyographic characteristics of pelvic floor muscles in women with stress urinary incontinence following sEMG-assisted biofeedback training and Pilates exercises. PLoS ONE 2019, 14, e0225647. [Google Scholar] [CrossRef] [Green Version]
- Laycock, J.; Jerwood, D. Pelvic floor muscle assessment: The PERFECT scheme. Physiotherapy 2001, 87, 631–642. [Google Scholar] [CrossRef]
- Sch, B.; Laycock, J.; Norton, P.A.; Stanton, S.L. Pelvic Floor Re-Education: Principles and Practice; Springer Science & Business Media: Berlin/Heidelberg, Germany, 1994. [Google Scholar]
- Chevalier, F.; Fernandez-Lao, C.; Cuesta-Vargas, A.I. Normal reference values of strength in pelvic floor muscle of women: A descriptive and inferential study. BMC Women’s Health 2014, 14, 143. [Google Scholar] [CrossRef] [Green Version]
- Madill, S.J.; McLean, L. Quantification of abdominal and pelvic floor muscle synergies in response to voluntary pelvic floor muscle contractions. J. Electromyogr. Kinesiol. 2008, 18, 955–964. [Google Scholar] [CrossRef]
- Thiel, R.D.; Dambros, M.; Palma, P.C.R.; Thiel, M.; Riccetto, C.L.Z.; Ramos, M.d.F. Tradução para português, adaptação cultural e validação do Female Sexual Function Index. Rev. Bras. Ginecol. Obs. 2008, 30, 504–510. [Google Scholar] [CrossRef]
- Tamanini, J.T.N.; Dambros, M.; D’Ancona, C.A.L.; Palma, P.C.R.; Netto, R., Jr. Validação para o português do “International Consultation on Incontinence Questionnaire-Short form” (ICIQ-SF). Rev. Saude Publica 2004, 38, 438–444. [Google Scholar] [CrossRef] [Green Version]
- Silva, V.A.; D’Elboux, M.J. Factors associated with urinary incontinence in elderly individuals who meet frailty criteria. Texto Contexto-Enferm. 2012, 21, 338–347. [Google Scholar] [CrossRef]
- Fonseca, E.S.M.; Camargo, A.L.M.; Castro, R.d.A.; Sartori, M.G.F.; Fonseca, M.C.M.; Lima, G.R.d.; Girão, M.J. Validação do questionário de qualidade de vida (King’s Health Questionnaire) em mulheres brasileiras com incontinência urinária. Rev. Bras. Ginecol. Obs. 2005, 27, 235–242. [Google Scholar] [CrossRef] [Green Version]
- de Luccas Batista, N.M.T.; de Oliveira, A.N.; Nunes, E.F.C.; Latorre, G.F.S. Força e coordenação motora da musculatura do assoalho pélvico e a função sexual feminina. IJHE-Interdiscip. J. Health Educ. 2017, 2. [Google Scholar] [CrossRef]
- Oleksy, Ł.; Mika, A.; Sulowska-Daszyk, I.; Rosłoniec, E.; Kielnar, R.; Stolarczyk, A. The Reliability of Pelvic Floor Muscle Bioelectrical Activity (sEMG) Assessment Using a Multi-Activity Measurement Protocol in Young Women. Int. J. Environ. Res. Public Health 2021, 18, 765. [Google Scholar] [CrossRef]
- Ribeiro, A.M.; Mateus-Vasconcelos, E.C.L.; Silva TDd Brito, L.G.d.O.; Oliveira, H.F.d. Functional assessment of the pelvic floor muscles by electromyography: Is there a normalization in data analysis? A systematic review. Fisioter. Pesqui. 2018, 25, 88–99. [Google Scholar] [CrossRef] [Green Version]
- Vieira, G.F.; Saltiel, F.; Miranda-Gazzola, A.P.G.; Kirkwood, R.N.; Figueiredo, E.M. Pelvic floor muscle function in women with and without urinary incontinence: Are strength and endurance the only relevant functions? A cross-sectional study. Physiotherapy 2020, 109, 85–93. [Google Scholar] [CrossRef]
- Eisen, A. Electromyography in disorders of muscle tone. Can. J. Neurol. Sci. 1987, 14 (Suppl 3), 501–505. [Google Scholar] [CrossRef] [Green Version]
- Guler, U.; Sen, D.; Costanzo, I.M.; Tufan, T.B.; Rhein, L. Sensors for Neonatal Monitoring. 2022. Available online: https://www.sciencedirect.com/science/article/pii/B9780128225486001047 (accessed on 20 September 2022).
- Wiegel, M.; Meston, C.; Rosen, R. The female sexual function index (FSFI): Cross-validation and development of clinical cutoff scores. J. Sex Marital Ther. 2005, 31, 1–20. [Google Scholar] [CrossRef]
- Bilgic, D.; Kizilkaya Beji, N. How do urinary incontinence types affect sexual function and quality of life for Turkish women? LUTS: Low. Urin. Tract Symptoms 2020, 12, 253–259. [Google Scholar] [CrossRef]
- Felippe, M.R.; Zambon, J.P.; Girotti, M.E.; Burti, J.S.; Hacad, C.R.; Cadamuro, L.; Almeida, F. What is the real impact of urinary incontinence on female sexual dysfunction? A case control study. Sex. Med. 2017, 5, e54–e60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zincir, H.; Demir, G.; Ozen, B. Sexual dysfunction in married women with urinary incontinence. Urol. J. 2018, 15, 193–198. [Google Scholar]
- Burzyński, B.; Kwiatkowska, K.; Sołtysiak-Gibała, Z.; Bryniarski, P.; Przymuszała, P.; Wlaźlak, E.; Przymski, P. Impact of stress urinary incontinence on female sexual activity. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 643–653. [Google Scholar] [PubMed]
- Gomes, T.A.; de Arruda Faber, M.; Botta, B.; Brito, L.G.O.; Juliato, C.R.T. Severity of urinary incontinence is associated with prevalence of sexual dysfunction. Int. Urogynecol. J. 2020, 31, 1669–1674. [Google Scholar] [CrossRef]
- Mota, R.L. Female urinary incontinence and sexuality. Int. Braz. J. Urol. 2017, 43, 20–28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
|
G1 (n = 16) |
G2 (n = 17) | t or U | p | |
|---|---|---|---|---|
| Power (pressure) | 3.00 (2.16; 3.46) | 3.00 (2.59; 3.75) | 114.00 | 0.414 |
| sEMG | ||||
| MVC (µv) | 34.69 (30.07; 47.97) | 32.53 (24.80; 48.02) | 117.00 | 0.494 |
| Peak (0 to 10 s) | 34.14 (29.99; 49.13) | 26.86 (23.15; 45.98) | 99.00 | 0.183 |
| Peak (%MCV) | 102.48 ± 12.90 | 96.36 ± 19.25 | 1.079 | 0.290 |
| Mean amplitudes (0 to 10 s) | 25.08 (20.74; 34.49) | 18.44 (15.59; 31.03) | 98.00 | 0.171 |
| Mean amplitudes (%MVC) | 71.98 ± 13.75 | 65.94 ± 13.58 | 1.269 | 0.214 |
| FSFI | ||||
| Sexual desire | 3.86 ± 0.87 | 3.13 ± 0.98 | 2.23 | 0.033 |
| Sexual excitement | 4.05 ± 1.46 | 3.32 ± 1.81 | 1.28 | 0.210 |
| Vaginal lubrication | 4.65 (3.35; 5.12) | 3.90 (2.50; 4.95) | 132.00 | 0.884 |
| Orgasm | 4.07 ± 1.61 | 3.38 ± 2.39 | 0.973 | 0.339 |
| Sexual satisfaction | 3.95 ± 1.63 | 4.05 ± 1.70 | −0.167 | 0.868 |
| Pain | 4.20 (3.10; 4.73) | 4.40 (2.29; 4.81) | 133.00 | 0.914 |
| Total | 24.09 ± 6.71 | 21.17 ± 10.48 | 0.960 | 0.346 |
| Variables | rs | p | |
|---|---|---|---|
| Power (pressure) | MVC (µv) | 0.652 | 0.006 |
| Peak (0 to 10 s) | 0.653 | 0.006 | |
| Mean amplitudes (0 to 10 s) | 0.653 | 0.017 | |
| MVC (µv) | Peak (0 to 10 s) | 0.985 | <0.0001 |
| Mean amplitudes (0 to 10 s) | 0.909 | <0.0001 | |
| Peak (0 to 10 s) | Mean amplitudes (0 to 10 s) | 0.909 | <0.0001 |
| Peak (%MCV) | Mean amplitudes (%MVC) | 0.833 | <0.0001 |
| Mean amplitudes (%MVC) | Sexual desire (FSFI) | 0.534 | 0.033 |
| Sexual excitement (FSFI) | Vaginal lubrication (FSFI) | 0.885 | <0.0001 |
| Orgasm (FSFI) | 0.766 | 0.001 | |
| Sexual satisfaction (FSFI) | 0.763 | 0.001 | |
| Total (FSFI) | 0.908 | <0.0001 | |
| Vaginal lubrication (FSFI) | Orgasm (FSFI) | 0.736 | 0.001 |
| Sexual satisfaction (FSFI) | 0.517 | 0.040 | |
| Total (FSFI) | 0.859 | <0.0001 | |
| Orgasm (FSFI) | Sexual satisfaction (FSFI) | 0.668 | 0.005 |
| Total (FSFI) | 0.850 | <0.0001 | |
| Sexual satisfaction (FSFI) | Total (FSFI) | 0.797 | <0.0001 |
| Pain (FSFI) | Total (FSFI) | 0.644 | 0.007 |
| Variables | rs | p | |
|---|---|---|---|
| Power (pressure) | KHQ Severity measures | −0.491 | 0.045 |
| MVC (µv) | Peak (0 to 10 s) | 0.961 | <0.0001 |
| Mean amplitudes (0 to 10 s) | 0.954 | <0.0001 | |
| KHQ Physical limitations | −0.483 | 0.049 | |
| Peak (0 to 10 s) | Mean amplitudes (0 to 10 s) | 0.978 | <0.0001 |
| Peak (%MCV) | Mean amplitudes (%MVC) | 0.855 | <0.0001 |
| ICIQ Total | −0.486 | 0.048 | |
| Mean amplitudes (%MVC) | Sexual desire (FSFI) | 0.556 | 0.020 |
| Sexual excitement (FSFI) | 0.500 | 0.041 | |
| Sexual satisfaction (FSFI) | 0.533 | 0.028 | |
| Personal relationships (KHQ) | 0.748 | 0.001 | |
| Total (ICIQ) | Daily life activities (ICIQ) | 0.895 | <0.0001 |
| Social limitations (KHQ) | 0.482 | 0.050 | |
| Severity measures (KHQ) | 0.579 | 0.015 | |
| Frequency SUI (ICIQ) | Role limitations (KHQ) | 0.578 | 0.015 |
| Daily life activities (ICIQ) | Role limitations (KHQ) | 0.578 | 0.015 |
| Social limitations (KHQ) | 0.485 | 0.048 | |
| Severity measures (KHQ) | 0.515 | 0.035 | |
| Sexual desire (FSFI) | Sexual excitement (FSFI) | 0.711 | 0.001 |
| Sexual satisfaction (FSFI) | 0.625 | 0.007 | |
| Total (FSFI) | 0.628 | 0.007 | |
| General health perception (KHQ) | −0.579 | 0.015 | |
| Sexual excitement (FSFI) | Vaginal lubrication (FSFI) | 0.870 | <0.0001 |
| Orgasm (FSFI) | 0.803 | <0.0001 | |
| Sexual satisfaction (FSFI) | 0.860 | <0.0001 | |
| Pain (FSFI) | 0.782 | <0.0001 | |
| Total (FSFI) | 0.943 | <0.0001 | |
| Vaginal lubrication (FSFI) | Orgasm (FSFI) | 0.781 | <0.0001 |
| Sexual satisfaction (FSFI) | 0.747 | 0.001 | |
| Pain (FSFI) | 0.919 | <0.0001 | |
| Total (FSFI) | 0.936 | <0.0001 | |
| Orgasm (FSFI) | Sexual satisfaction (FSFI) | 0.794 | <0.0001 |
| Pain (FSFI) | 0.792 | <0.0001 | |
| Total (FSFI) | 0.902 | <0.0001 | |
| Sexual satisfaction (FSFI) | Pain | 0.734 | 0.001 |
| Total (FSFI) | 0.892 | <0.0001 | |
| Pain (FSFI) | Total (FSFI) | 0.917 | <0.0001 |
| Incontinence impact (KHQ) | Role limitations (KHQ) | 0.535 | 0.027 |
| Emotions (KHQ) | 0.756 | <0.0001 | |
| Sleep/energy (KHQ) | 0.689 | 0.002 | |
| Severity measures (KHQ) | 0.413 | 0.100 | |
| Physical limitations (KHQ) | Social limitations (KHQ) | 0.691 | 0.002 |
| Sleep/energy (KHQ) | 0.603 | 0.010 | |
| Social limitations (KHQ) | Sleep/energy (KHQ) | 0.615 | 0.009 |
| Severity measures (KHQ) | 0.535 | 0.027 | |
| Emotions (KHQ) | Sleep/energy (KHQ) | 0.487 | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, C.R.G.; Soares, W.M.; da Costa Priante, C.H.; de Souza Duarte, N.; Soares, C.O.; Bittencourt, K.C.; Melo, G.S.; Nunes, E.F.C.; de Campos Gomes, F.; De Melo Neto, J.S.; et al. Strength and Bioelectrical Activity of the Pelvic Floor Muscles and Sexual Function in Women with and without Stress Urinary Incontinence: An Observational Cross-Sectional Study. Healthcare 2023, 11, 181. https://doi.org/10.3390/healthcare11020181
Ferreira CRG, Soares WM, da Costa Priante CH, de Souza Duarte N, Soares CO, Bittencourt KC, Melo GS, Nunes EFC, de Campos Gomes F, De Melo Neto JS, et al. Strength and Bioelectrical Activity of the Pelvic Floor Muscles and Sexual Function in Women with and without Stress Urinary Incontinence: An Observational Cross-Sectional Study. Healthcare. 2023; 11(2):181. https://doi.org/10.3390/healthcare11020181
Chicago/Turabian StyleFerreira, Clicia Raiane Galvão, Wenderk Martins Soares, Caren Heloise da Costa Priante, Natália de Souza Duarte, Cleuma Oliveira Soares, Kayonne Campos Bittencourt, Giovana Salomão Melo, Erica Feio Carneiro Nunes, Fabiana de Campos Gomes, João Simão De Melo Neto, and et al. 2023. "Strength and Bioelectrical Activity of the Pelvic Floor Muscles and Sexual Function in Women with and without Stress Urinary Incontinence: An Observational Cross-Sectional Study" Healthcare 11, no. 2: 181. https://doi.org/10.3390/healthcare11020181
APA StyleFerreira, C. R. G., Soares, W. M., da Costa Priante, C. H., de Souza Duarte, N., Soares, C. O., Bittencourt, K. C., Melo, G. S., Nunes, E. F. C., de Campos Gomes, F., De Melo Neto, J. S., & Rodrigues, C. N. C. (2023). Strength and Bioelectrical Activity of the Pelvic Floor Muscles and Sexual Function in Women with and without Stress Urinary Incontinence: An Observational Cross-Sectional Study. Healthcare, 11(2), 181. https://doi.org/10.3390/healthcare11020181