
Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic?


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rizvi, R.F.; Craig, K.J.T.; Hekmat, R.; Reyes, F.; South, B.; Rosario, B.; Kassler, W.J.; Jackson, G.P. Effectiveness of non-pharmaceutical interventions related to social distancing on respiratory viral infectious disease outcomes: A rapid evidence-based review and meta-analysis. SAGE Open Med. 2021, 9, 20503121211022973. [Google Scholar] [CrossRef]
- Kucharski, A.J.; Klepac, P.; Conlan, A.J.K.; Kissler, S.M.; Tang, M.L.; Fry, H.; Gog, J.R.; Edmunds, W.J.; CMMID COVID-19 Working Group. Effectiveness of isolation, testing, contact tracing, and physical distancing on reducing transmission of SARS-CoV-2 in different settings: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Chan, J.F.; Yuen, K.Y. Viral lung infections: Epidemiology, virology, clinical features, and management of avian influenza A(H7N9). Curr. Opin. Pulm. Med. 2014, 20, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Sopena, N.; Sabrià, M.; Pedro-Botet, M.L.; Manterola, J.M.; Matas, L.; Domínguez, J.; Modol, J.M.; Tudela, P.; Ausina, V.; Foz, M. Prospective study of community-acquired pneumonia of bacterial etiology in adults. Eur. J. Clin. Microbiol. Infect. Dis. 1999, 18, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Park, J.Y.; Lim, I.S.; Chae, S.A.; Yun, S.W.; Lee, N.M.; Kim, S.Y.; Choi, B.S.; Yi, D.Y. Changes in the Occurrence of Gastrointestinal Infections after COVID-19 in Korea. J. Korean Med. Sci. 2021, 36, e180. [Google Scholar] [CrossRef] [PubMed]
- Ronald, A. The etiology of urinary tract infection: Traditional and emerging pathogens. Dis. Mon. 2003, 49, 71–82. [Google Scholar] [CrossRef]
- Tanislav, C.; Jacob, L.; Kostev, K. Consultations Decline for Stroke, Transient Ischemic Attack, and Myocardial Infarction during the COVID-19 Pandemic in Germany. Neuroepidemiology 2021, 55, 70–78. [Google Scholar] [CrossRef]
- Arafa, M.; Nesar, S.; Abu-Jabeh, H.; Jayme, M.O.R.; Kalairajah, Y. COVID-19 pandemic and hip fractures: Impact and lessons learned. Bone Jt. Open. 2020, 1, 530–540. [Google Scholar] [CrossRef]
- Magnusson, K.; Helgeland, J.; Grøsland, M.; Telle, K. Impact of the COVID-19 pandemic on emergency and elective hip surgeries in Norway. Acta Orthop. 2021, 92, 376–380. [Google Scholar] [CrossRef]
- Schoeneberg, C.; Eschbach, D.A.; Friess, T.; Lendemans, S.; Hoefer, C.; Ruchholtz, S. Effect of the COVID-19 Pandemic in German Trauma Centres and Geriatric Trauma Centres DGU. Z. Orthop. Unfall. 2021, 159, 209–215. [Google Scholar] [CrossRef]
- Ormeño, J.C.; Martínez, R.; Frías, C.; Von Plessing, C.; Quevedo, I. Impact of the COVID-19 pandemic on osteoporotic hip fractures in Chile. Arch. Osteoporos. 2022, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Tam, C.-C.F.; Cheung, K.-S.; Lam, S.; Wong, A.; Yung, A.; Sze, M.; Lam, Y.-M.; Chan, C.; Tsang, T.-C.; Tsui, M.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on ST-Segment-Elevation Myocardial Infarction Care in Hong Kong, China. Circ. Cardiovasc. Qual Outcomes 2020, 13, e006631. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child. Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef] [PubMed]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January 1, 2019–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, V.; Mahfoud, F.; Lauder, L.; Reith, W.; Behnke, S.; Smola, S.; Rissland, J.; Pfuhl, T.; Scheller, B.; Böhm, M.; et al. Decline of emergency admissions for cardiovascular and cerebrovascular events after the outbreak of COVID-19. Clin. Res. Cardiol. 2020, 109, 1500–1506. [Google Scholar] [CrossRef] [PubMed]
- Slagman, A.; Behringer, W.; Greiner, F.; Klein, M.; Weismann, D.; Erdmann, B.; Möckel, M.; On behalf of the German Forum of University Emergency Departments (FUN) and the AKTIN Emergency Department Registry. Medical Emergencies During the COVID-19 Pandemic. Dtsch. Arztebl. Int. 2020, 117, 545–552. [Google Scholar] [CrossRef]
- Tanislav, C.; Kostev, K. Investigation of the prevalence of non-COVID-19 infectious diseases during the COVID-19 pandemic. Public. Health 2022, 203, 53–57. [Google Scholar] [CrossRef]
- Marroquín, B.; Vine, V.; Morgan, R. Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Res. 2020, 293, 113419. [Google Scholar] [CrossRef]
- Cai, W.; Gao, Y.; Yang, W.; Cheng, F.; Tang, D.; Li, L. Physical Activity-Related Injury and Its Associated Factors among Middle School Students in Southern China. Int. J. Environ. Res. Public. Health. 2018, 15, 1244. [Google Scholar] [CrossRef] [PubMed]
- Rennie, L.; Court-Brown, C.M.; Mok, J.Y.; Beattie, T.F. The epidemiology of fractures in children. Injury 2007, 38, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.M.; Robertson, G.A.; Rennie, L.; Caesar, B.C.; Court-Brown, C.M. The epidemiology of sports-related fractures in adolescents. Injury 2010, 41, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Court-Brown, C.M.; Wood, A.M.; Aitken, S. The epidemiology of acute sports-related fractures in adults. Injury 2008, 39, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Moreland, B.; Kakara, R.; Henry, A. Trends in Nonfatal Falls and Fall-Related Injuries Among Adults Aged ≥65 Years—United States, 2012–2018. MMWR Morb Mortal Wkly Rep. 2020, 69, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.M.; Lentzner, H.R.; Weeks, J.D. Unmet need for personal assistance with activities of daily living among older adults. Gerontologist 2001, 41, 82–88. [Google Scholar] [CrossRef]
- Moreland, B.; Shakya, I.; Idaikkadar, N. Development and Evaluation of Syndromic Surveillance Definitions for Fall- and Hip Fracture-Related Emergency Department Visits Among Adults Aged 65 Years and Older, United States 2017-2018. J Public Health Manag Pract. 2023, 29, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Zhang, Y.; Song, K.; Kang, H.; Ye, D.; Li, F. What was the Epidemiology and Global Burden of Disease of Hip Fractures From 1990 to 2019? Results From and Additional Analysis of the Global Burden of Disease Study 2019. Clin. Orthop. Relat. Res. 2022, 481, 1209–1220. [Google Scholar] [CrossRef]
- Hernandez, I.; He, M.; Guo, J.; Tadrous, M.; Gabriel, N.; Swabe, G.; Gellad, W.F.; Essien, U.R.; Saba, S.; Benjamin, E.J.; et al. COVID-19 pandemic and trends in new diagnosis of atrial fibrillation: A nationwide analysis of claims data. PLoS ONE 2023, 18, e0281068. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Kohring, C.; Dammertz, L.; Heuer, J.; Below, M.; Bätzing, J.; Holstiege, J. The Effect of the COVID-19 Pandemic on Outpatient Antibiotic Prescription Rates in Children and Adolescents-A Claims-Based Study in Germany. Antibiotics 2022, 11, 1433. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|
| N | 47,459 | 48,487 | 50,084 | 46,227 | 46,467 |
| Mean age (standard deviation) | 60.8 (16.2) | 61.1 (16.1) | 61.5 (15.9) | 63.1 (14.6) | 63.3 (14.9) |
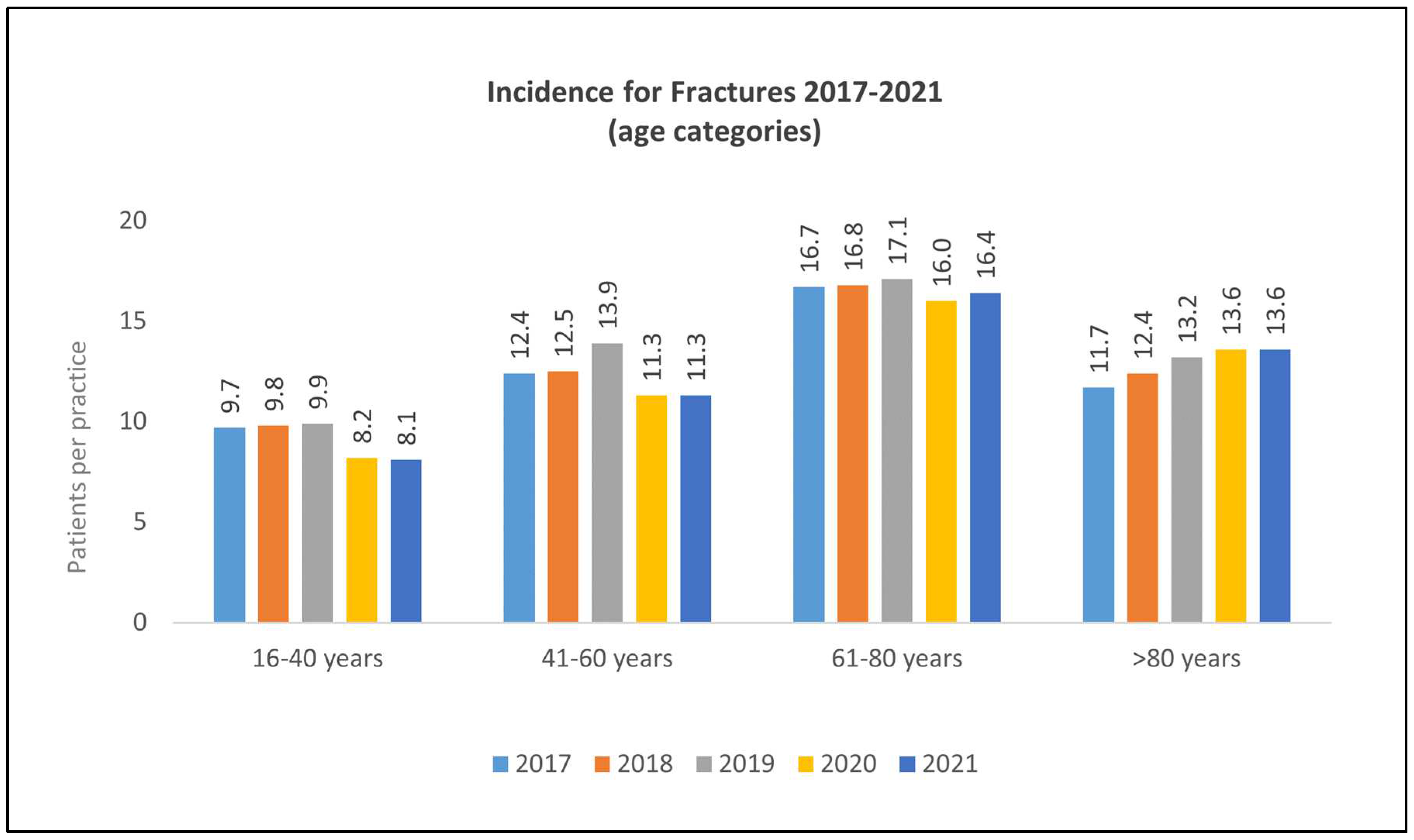
| 16–40 years (%) | 19.2 | 19.0 | 18.6 | 16.7 | 16.3 |
| 41–60 years (%) | 24.6 | 24.4 | 24.5 | 23.1 | 22.9 |
| 61–80 years (%) | 33.1 | 32.6 | 32.1 | 32.6 | 33.2 |
| >80 years (%) | 23.2 | 24.0 | 24.8 | 27.7 | 27.5 |
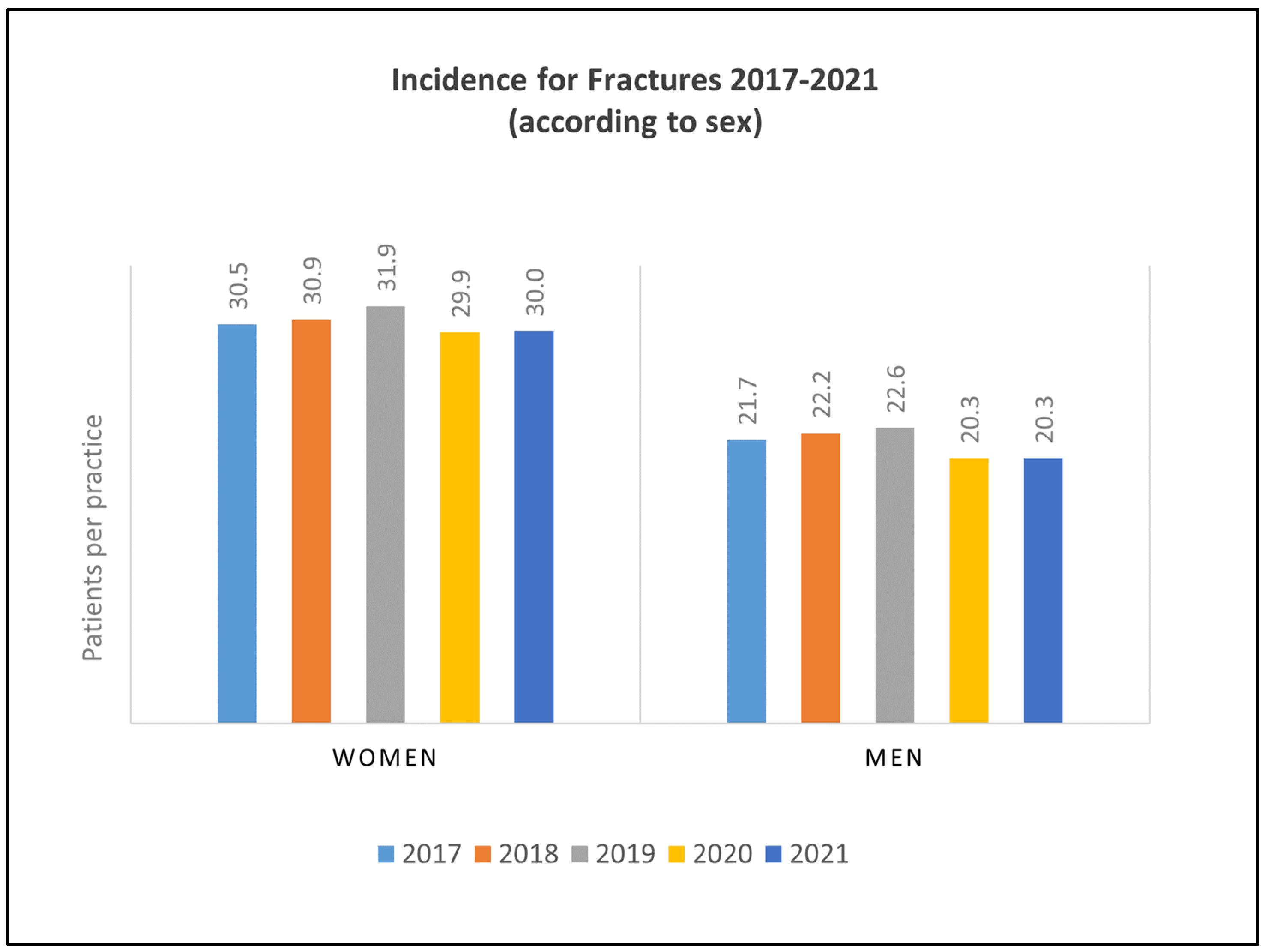
| Female (%) | 58.4 | 58.2 | 58.6 | 59.5 | 59.7 |
| Male (%) | 41.6 | 41.8 | 41.4 | 40.5 | 40.3 |
| Fractures by Age Group | Yearly Difference | ||||
|---|---|---|---|---|---|
| 2018–2017 | 2019–2018 | 2020–2019 | 2021–2020 | ||
| 16–40 years | Patients per practice | 9.8 − 9.7 = +0.1 | 9.9 − 9.8 = +0.1 | 8.2 − 9.9 = −1.7 | 8.1 − 8.2 = −0.1 |
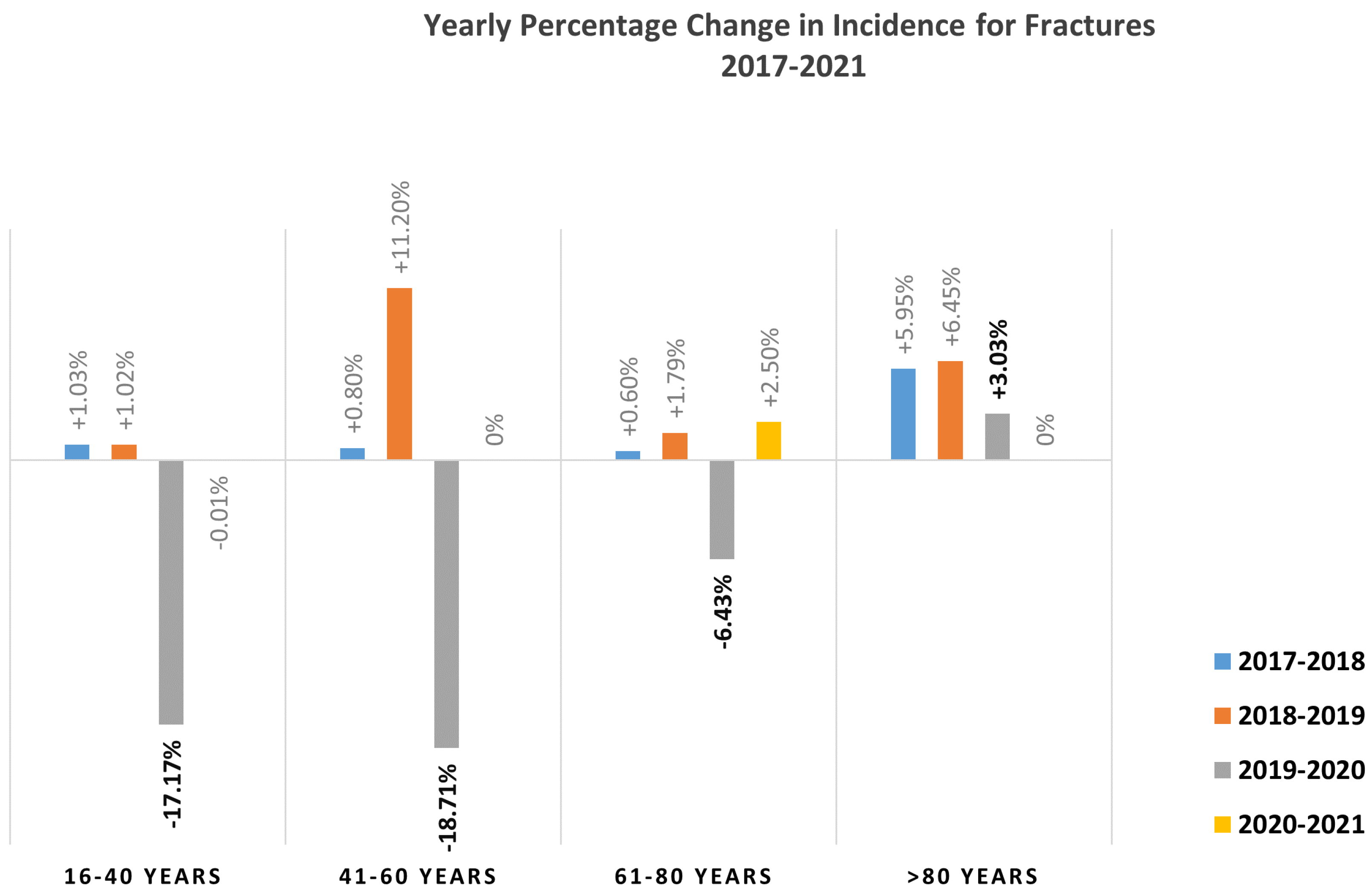
| Percentage | +1.03% | +1.02% | −17.17% | −1.22% | |
| 41–60 years | Patients per practice | 12.5 − 12.4 = +0.1 | 13.9 − 12.5 = +1.4 | 11.3 − 13.9 = −2.6 | 11.3 − 11.3 = 0 |
| Percentage | +0.80% | +11.2% | −18.71% | 0% | |
| 61–80 years | Patients per practice | 16.8 − 16.7 = +0.1 | 17.1 − 16.8 = +0.3 | 16.0 − 17.1 = −1.1 | 16.4 − 16.0 = +0.4 |
| Percentage | +0.60% | +1.79% | −6.43% | +2.5% | |
| >80 years | Patients per practice | 12.4 − 11.7 = +0.7 | 13.2 − 12.4 = +0.8 | 13.6 − 12.3 = +0.4 | 13.6 − 13.6 = 0 |
| Percentage | +5.98% | +6.45% | +3.03% | 0% | |
| Percentage Difference for Incidences during the First Year of the Pandemic (2020) in Comparison to the Pre-Pandemic Year (2019) | ||||
|---|---|---|---|---|
| Fracture Location | 16–40 Years | 41–60 Years | 61–80 Years | >80 Years |
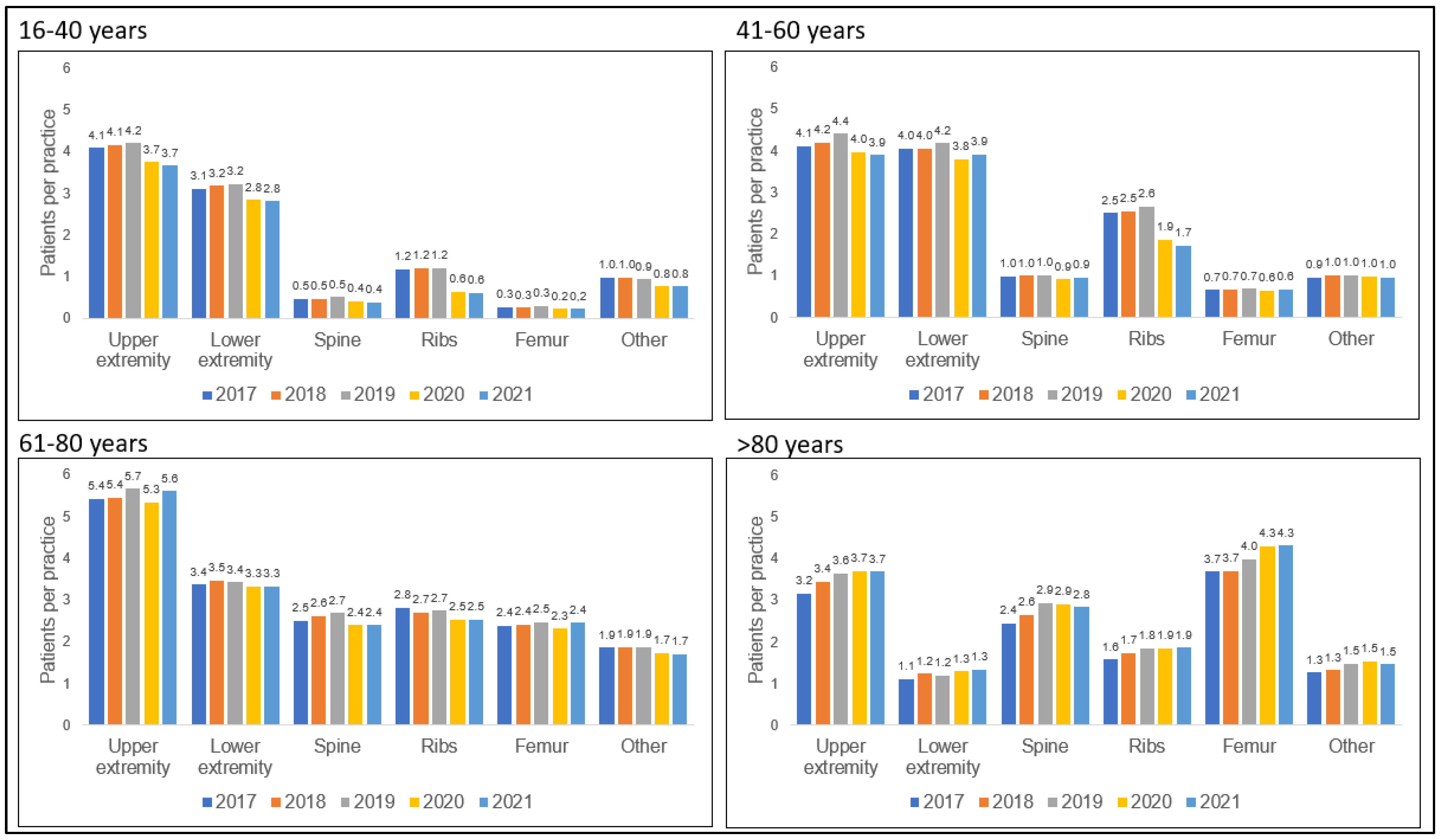
| Upper extremity | −11.9% | −9.1% | −7.0% | +2.8% |
| Lower extremity | −12.5% | −9.5% | −2.9% | +8.3% |
| Spine | −20.0% | −10.0% | −11.1% | ±0% |
| Ribs | −50.0% | −26.9% | −7.4% | +5.6% |
| Femur | −33.3% | −14.3% | −8.0% | +8.3% |
| Other | −11.1% | ±0% | −10.5% | ±0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemöller, U.; Tanislav, C.; Kostev, K. Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic? Healthcare 2023, 11, 2804. https://doi.org/10.3390/healthcare11202804
Niemöller U, Tanislav C, Kostev K. Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic? Healthcare. 2023; 11(20):2804. https://doi.org/10.3390/healthcare11202804
Chicago/Turabian StyleNiemöller, Ulrich, Christian Tanislav, and Karel Kostev. 2023. "Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic?" Healthcare 11, no. 20: 2804. https://doi.org/10.3390/healthcare11202804
APA StyleNiemöller, U., Tanislav, C., & Kostev, K. (2023). Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic? Healthcare, 11(20), 2804. https://doi.org/10.3390/healthcare11202804