Fusion’s Location and Quality within the Fixated Segment Following Transforaminal Interbody Fusion (TLIF)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
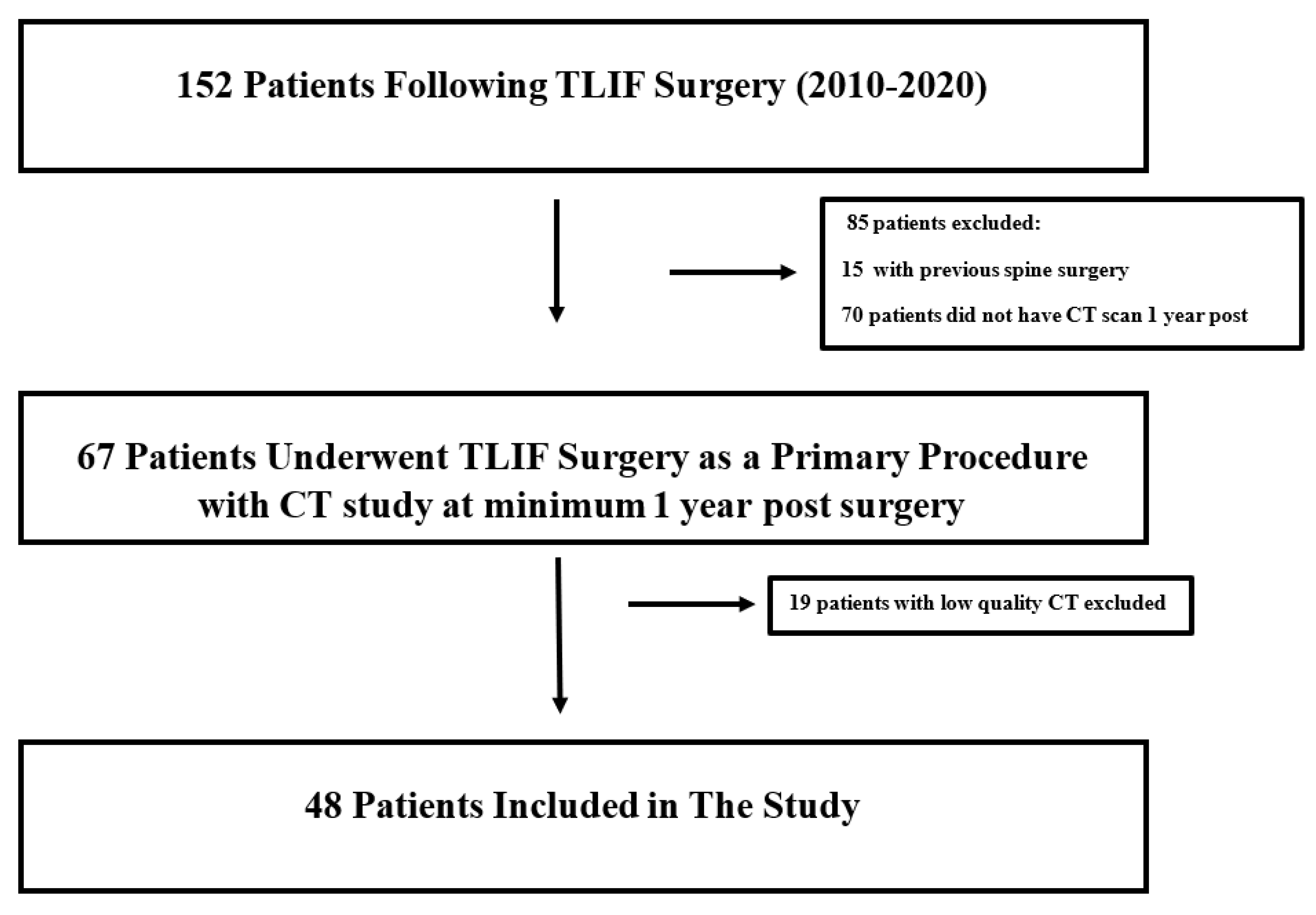
2.2. Study Eligibility
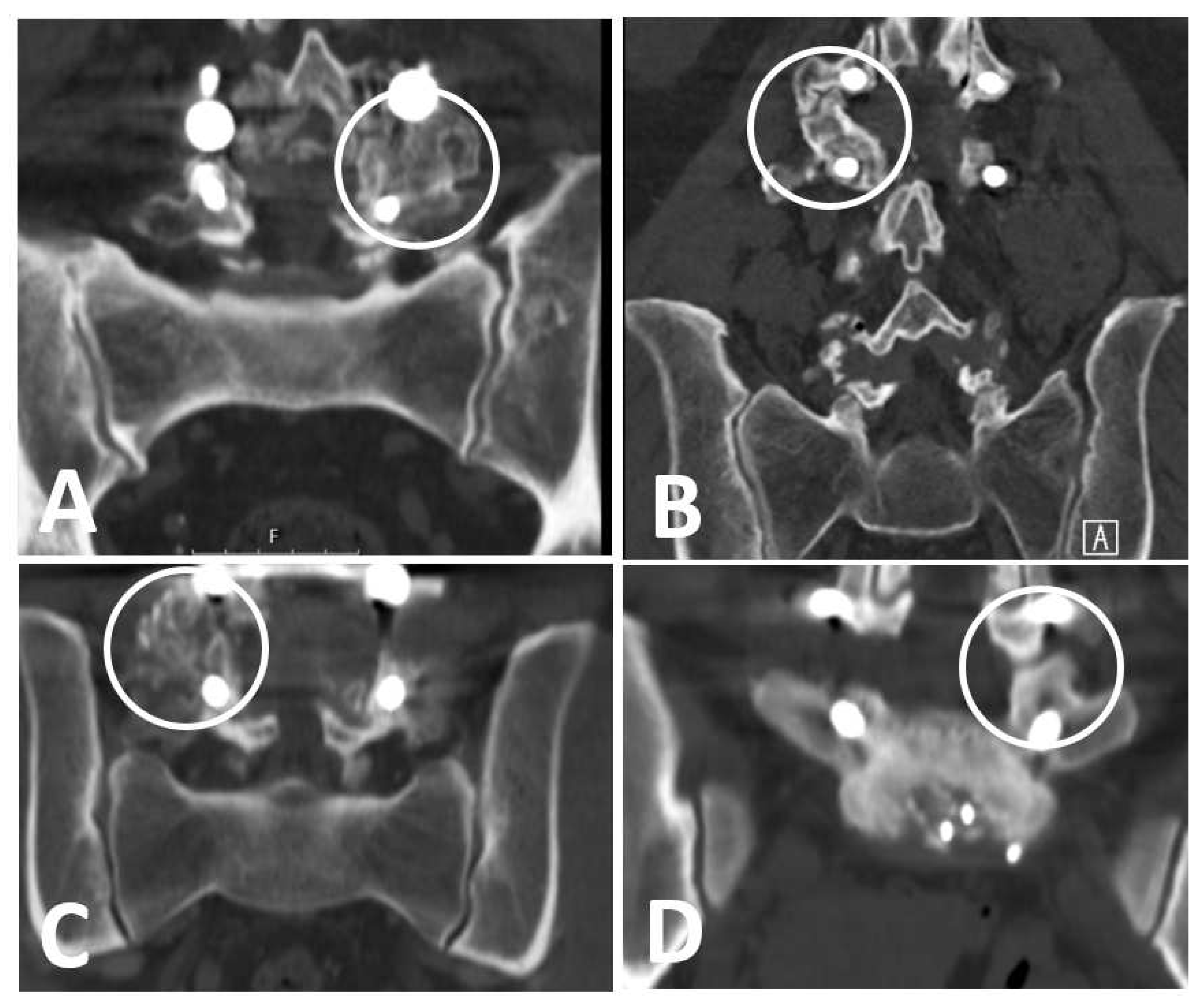
2.3. Patients’ Imaging Assessment
2.4. Patients’ Exposure
2.5. Outcomes
- (1)
- Definitive fusion: definitive bony trabecular bridging across the graft–host interface.
- (2)
- Probable fusion: no definitive bony trabecular crossing but with no gap at the graft–host interface.
- (3)
- Possible arthrosis: no bony trabecular crossing with identifiable gap at the graft–host interface.
- (4)
- Definite pseudarthrosis: no traversing trabecular bone with definitive gap.
2.6. Background Covariates
Statistical Analysis
3. Results
3.1. Patients’ Characteristics
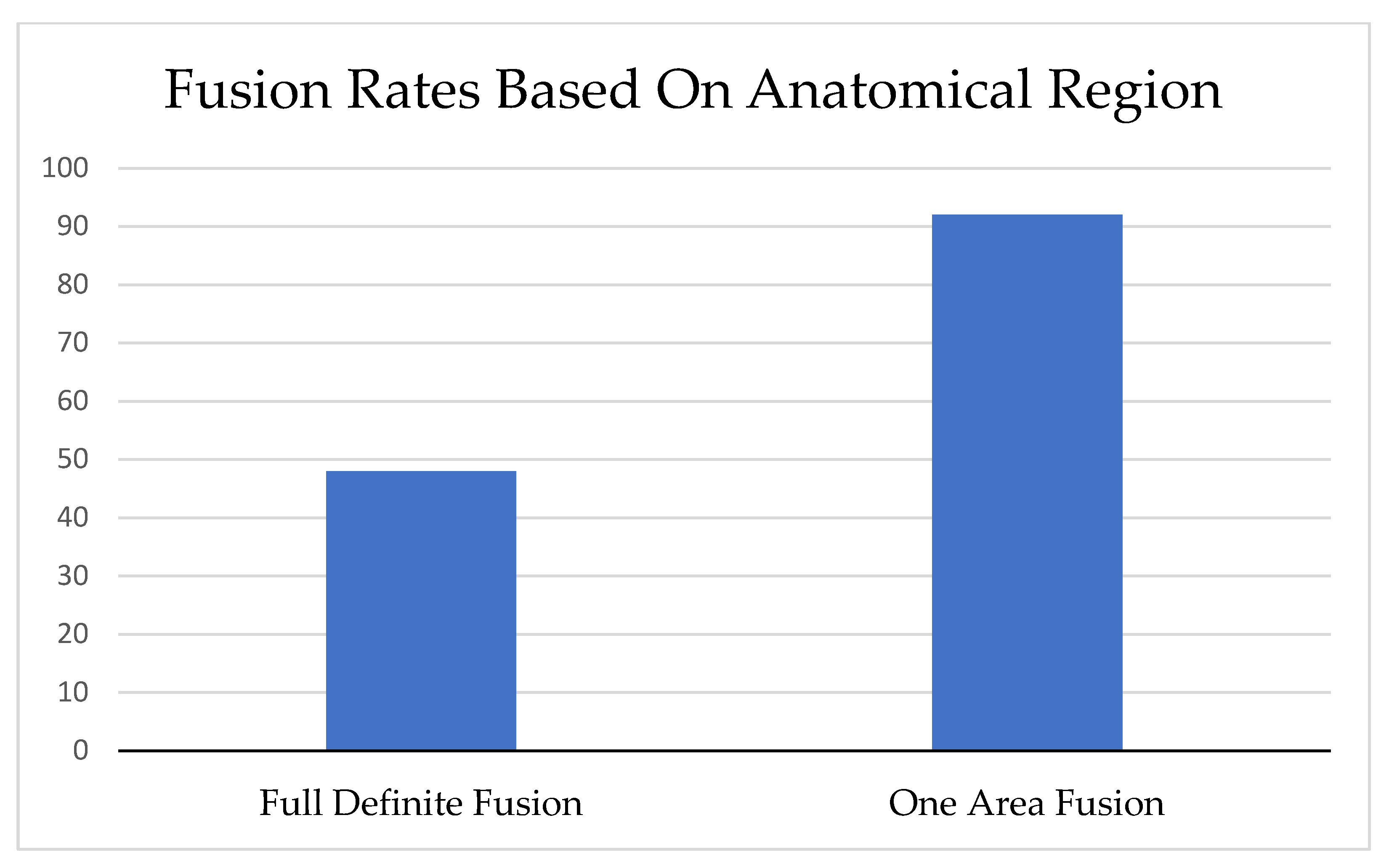
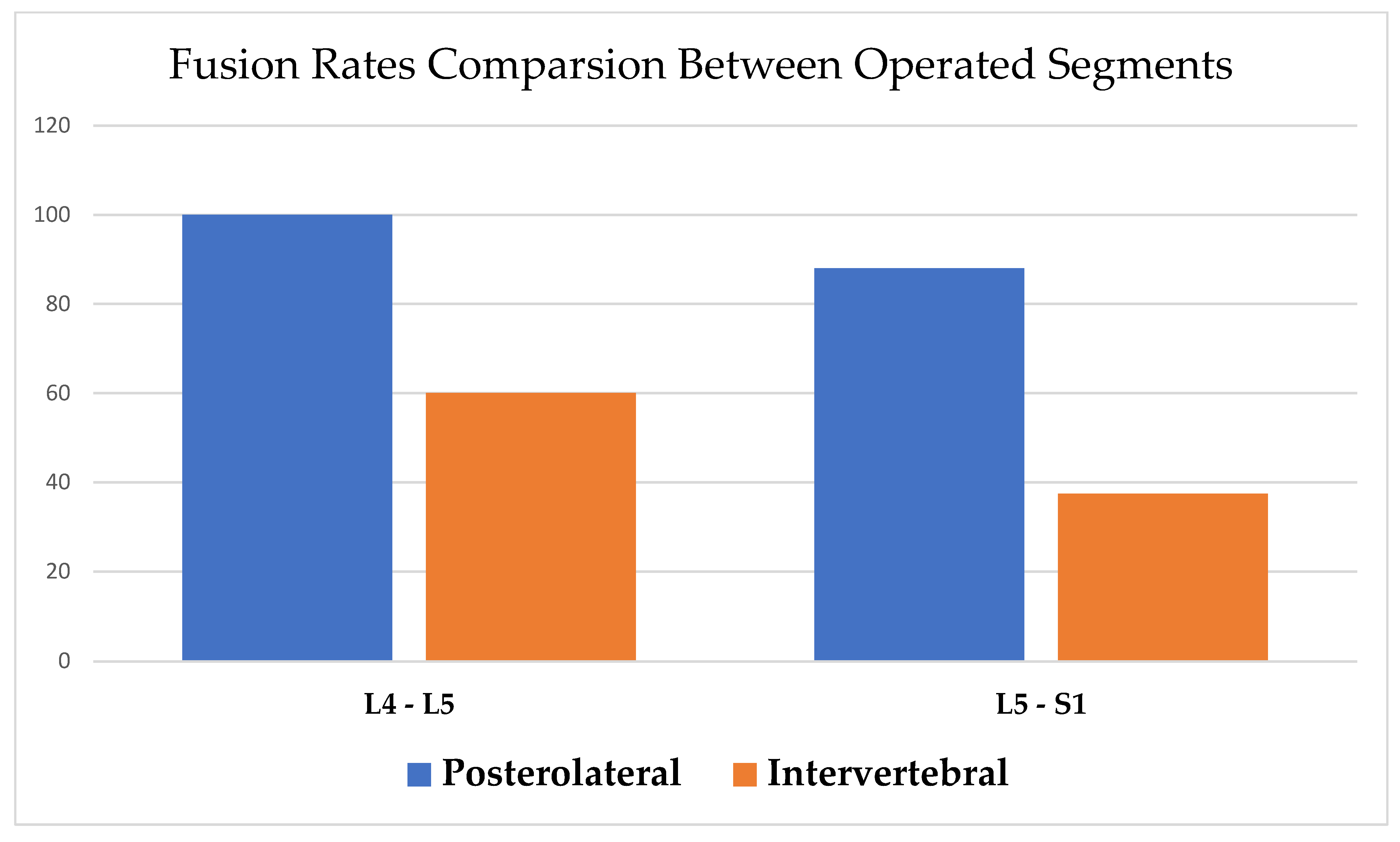
3.2. Fusion Rate and Quality
4. Discussion
4.1. Limitation
4.2. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| TLIF | Transforaminal lumbar interbody fusion with posterolateral fusion |
| CT | Computed tomography |
| SD | Statistical deviation |
| PLF | Posterolateral fusion |
| QALY | Quality-adjusted life year |
| HQRoL | Health-related quality of life |
| ODI | Oswestry disability index |
| PACS | Picture archiving and communication system |
| MM | Millimeters |
| OR | Odds ratio |
| CI | Confidence interval |
References
- Çaçan, M.A.; Uçar, B.Y. What every spine surgeon should know about transforaminal lumbar interbody fusion surgery for herniated discs. Int. Orthop. 2019, 43, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Zdeblick, T.A.; Phillips, F.M. Interbody cage devices. Spine 2003, 28, S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.X.; Liu, H.N.; Chen, M.T.; Lin, Y.P.; Wang, H.S.; Chen, B.L. Meta-analysis of the clinical efficacy and safety of oblique lateral interbody fusion and transforaminal interbody fusion in the treatment of degenerative lumbar spondylolisthesis. EFORT Open Rev. 2022, 7, 663–670. [Google Scholar] [CrossRef]
- Yuan, C.; Liu, C.; Shen, J.; Tian, H.; Zheng, W.; Zhang, C.; Pan, Y.; Huang, B.; Jiang, T.; Zhang, Z.; et al. Clinical evaluation of minimally invasive transforaminal lumbar interbody fusion for severe lumbar spinal stenosis. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2019, 33, 801–806. [Google Scholar] [CrossRef]
- Park, Y.; Ha, J.W.; Lee, Y.T.; Sung, N.Y. Minimally invasive transforaminal lumbar interbody fusion for spondylolisthesis and degenerative spondylosis: 5-year results. Clin. Orthop. Relat. Res. 2014, 472, 1813–1823. [Google Scholar] [CrossRef]
- Rouben, D.; Casnellie, M.; Ferguson, M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: A clinical and radiographic follow-up. J. Spinal Disord. Tech. 2011, 24, 288–296. [Google Scholar] [CrossRef]
- Qin, R.; Liu, B.; Zhou, P.; Yao, Y.; Hao, J.; Yang, K.; Xu, T.L.; Zhang, F.; Chen, X. Minimally Invasive Versus Traditional Open Transforaminal Lumbar Interbody Fusion for the Treatment of Single-Level Spondylolisthesis Grades 1 and 2: A Systematic Review and Meta-Analysis. World Neurosurg. 2019, 122, 180–189. [Google Scholar] [CrossRef]
- Kim, M.C.; Chung, H.T.; Kim, D.J.; Kim, S.H.; Jeon, S.H. The clinical and radiological outcomes of minimally invasive transforaminal lumbar interbody single level fusion. Asian Spine J. 2011, 5, 111–116. [Google Scholar] [CrossRef]
- Virk, S.; Qureshi, S.; Sandhu, H. History of Spinal Fusion: Where We Came from and Where We Are Going. HSS J. 2020, 16, 137–142. [Google Scholar] [CrossRef]
- de Kunder, S.L.; Rijkers, K.; Caelers, I.; de Bie, R.A.; Koehler, P.J.; van Santbrink, H. Lumbar Interbody Fusion: A Historical Overview and a Future Perspective. Spine 2018, 43, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Briggs, H.; Milligan, P.R. Chip Fusion of the Low Back Following Exploration of the Spinal Canal. JBJS 1944, 26, 125–130. [Google Scholar]
- Kepler, C.K.; Vaccaro, A.R.; Hilibrand, A.S.; Anderson, D.G.; Rihn, J.A.; Albert, T.J.; Radcliff, K.E. National trends in the use of fusion techniques to treat degenerative spondylolisthesis. Spine 2014, 39, 1584–1589. [Google Scholar] [CrossRef] [PubMed]
- Hackenberg, L.; Halm, H.; Bullmann, V.; Vieth, V.; Schneider, M.; Liljenqvist, U. Transforaminal lumbar interbody fusion: A safe technique with satisfactory three to five year results. Eur. Spine J. 2005, 14, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Ha, K.Y.; Rhyu, K.W.; Park, H.Y.; Cho, C.H.; Kim, H.C.; Lee, H.J.; Kim, S.I. Lumbar Interbody Fusion: Techniques, Pearls and Pitfalls. Asian Spine J. 2020, 14, 730–741. [Google Scholar] [CrossRef] [PubMed]
- Kakadiya, D.G.; Gohil, D.K.; Soni, D.Y.; Shakya, D.A. Clinical, radiological and functional results of transforaminal lumbar interbody fusion in degenerative spondylolisthesis. N. Am. Spine Soc. J. 2020, 2, 100011. [Google Scholar] [CrossRef]
- Sudo, H.; Oda, I.; Abumi, K.; Ito, M.; Kotani, Y.; Minami, A. Biomechanical study on the effect of five different lumbar reconstruction techniques on adjacent-level intradiscal pressure and lamina strain. J. Neurosurg. Spine 2006, 5, 150–155. [Google Scholar] [CrossRef]
- Rosenberg, W.S.; Mummaneni, P.V. Transforaminal lumbar interbody fusion: Technique, complications, and early results. Neurosurgery 2001, 48, 569–574, discussion 574–565. [Google Scholar] [CrossRef]
- Levin, J.M.; Tanenbaum, J.E.; Steinmetz, M.P.; Mroz, T.E.; Overley, S.C. Posterolateral fusion (PLF) versus transforaminal lumbar interbody fusion (TLIF) for spondylolisthesis: A systematic review and meta-analysis. Spine J. 2018, 18, 1088–1098. [Google Scholar] [CrossRef]
- Kim, E.; Chotai, S.; Stonko, D.; Wick, J.; Sielatycki, A.; Devin, C.J. A retrospective review comparing two-year patient-reported outcomes, costs, and healthcare resource utilization for TLIF vs. PLF for single-level degenerative spondylolisthesis. Eur. Spine J. 2018, 27, 661–669. [Google Scholar] [CrossRef]
- Høy, K.; Bünger, C.; Niederman, B.; Helmig, P.; Hansen, E.S.; Li, H.; Andersen, T. Transforaminal lumbar interbody fusion (TLIF) versus posterolateral instrumented fusion (PLF) in degenerative lumbar disorders: A randomized clinical trial with 2-year follow-up. Eur. Spine J. 2013, 22, 2022–2029. [Google Scholar] [CrossRef] [PubMed]
- Rathbone, J.; Rackham, M.; Nielsen, D.; Lee, S.M.; Hing, W.; Riar, S.; Scott-Young, M. A systematic review of anterior lumbar interbody fusion (ALIF) versus posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF), posterolateral lumbar fusion (PLF). Eur. Spine J. 2023, 32, 1911–1926. [Google Scholar] [CrossRef] [PubMed]
- Park, D.K.; Roberts, R.; Arnold, P.; Kim, D.H.; Sasso, R.; Baker, K.C.; Fischgrund, J.S. Lumbar Spine Fusion Rates With Local Bone in Posterolateral and Combined Posterolateral and Interbody Approaches. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2019, 3, e018. [Google Scholar] [CrossRef] [PubMed]
- Rickert, M.; Fennema, P.; Wehner, D.; Rahim, T.; Hölper, B.; Eichler, M.; Makowski, M.; Meurer, A.; Brenneis, M. Postoperative cage migration and subsidence following TLIF surgery is not associated with bony fusion. Sci. Rep. 2023, 13, 12597. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Lee, J.S.; Moon, K.P.; Kim, S.J.; Suh, K.T. Posterior lumbar interbody fusion and posterior instrumentation in the surgical management of lumbar tuberculous spondylitis. J. Bone Joint Surg. Br. 2007, 89, 210–214. [Google Scholar] [CrossRef]
- Lauber, S.; Schulte, T.L.; Liljenqvist, U.; Halm, H.; Hackenberg, L. Clinical and radiologic 2-4-year results of transforaminal lumbar interbody fusion in degenerative and isthmic spondylolisthesis grades 1 and 2. Spine 2006, 31, 1693–1698. [Google Scholar] [CrossRef]
- Dantas, F.; Dantas, F.L.R.; Botelho, R.V. Effect of interbody fusion compared with posterolateral fusion on lumbar degenerative spondylolisthesis: A systematic review and meta-analysis. Spine J. 2022, 22, 756–768. [Google Scholar] [CrossRef]
- Schmoelz, W.; Keiler, A. Intervertebral cages from a biomechanical point of view. Orthopade 2015, 44, 132–137. [Google Scholar] [CrossRef]
- Polly, D.W., Jr.; Klemme, W.R.; Cunningham, B.W.; Burnette, J.B.; Haggerty, C.J.; Oda, I. The biomechanical significance of anterior column support in a simulated single-level spinal fusion. J. Spinal Disord. 2000, 13, 58–62. [Google Scholar] [CrossRef]
- Closkey, R.F.; Parsons, J.R.; Lee, C.K.; Blacksin, M.F.; Zimmerman, M.C. Mechanics of interbody spinal fusion. Analysis of critical bone graft area. Spine 1993, 18, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.S.; Bailey, C.S.; Dvorak, M.F.; Fisher, C.G.; Oxland, T.R. Interbody device shape and size are important to strengthen the vertebra-implant interface. Spine 2005, 30, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Alkalay, R.N.; Adamson, R.; Groff, M.W. The effect of interbody fusion cage design on the stability of the instrumented spine in response to cyclic loading: An experimental study. Spine J. 2018, 18, 1867–1876. [Google Scholar] [CrossRef] [PubMed]
- Challier, V.; Boissiere, L.; Obeid, I.; Vital, J.M.; Castelain, J.E.; Bénard, A.; Ong, N.; Ghailane, S.; Pointillart, V.; Mazas, S.; et al. One-Level Lumbar Degenerative Spondylolisthesis and Posterior Approach: Is Transforaminal Lateral Interbody Fusion Mandatory?: A Randomized Controlled Trial with 2-Year Follow-Up. Spine 2017, 42, 531–539. [Google Scholar] [CrossRef]
- Tavares, W.M.; de França, S.A.; Paiva, W.S.; Teixeira, M.J. A systematic review and meta-analysis of fusion rate enhancements and bone graft options for spine surgery. Sci. Rep. 2022, 12, 7546. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, Y.; Zou, D.; Yuan, B.; Ke, H.Z.; Li, W. Therapeutics for enhancement of spinal fusion: A mini review. J. Orthop. Translat. 2021, 31, 73–79. [Google Scholar] [CrossRef]
- Hubbell, P.J.; Roth, B.; Block, J.E. Comparative Evaluation of Mineralized Bone Allografts for Spinal Fusion Surgery. J. Funct. Biomater. 2023, 14, 384. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, W.; Zuo, R.; Zhou, Y. Biomechanical Stability before and after Graft Fusion with Unilateral and Bilateral Pedicle Screw Fixation: Finite Element Study. World Neurosurg. 2019, 123, e228–e234. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.S.; Min, S.H.; Yoon, S.H. Fusion rate according to mixture ratio and volumes of bone graft in minimally invasive transforaminal lumbar interbody fusion: Minimum 2-year follow-up. Eur. J. Orthop. Surg. Traumatol. 2015, 25 (Suppl. 1), S183–S189. [Google Scholar] [CrossRef]
- Abou-Madawi, A.M.; Ali, S.H.; Abdelmonem, A.M. Local Autograft Versus Iliac Crest Bone Graft PSF-Augmented TLIF in Low-Grade Isthmic and Degenerative Lumbar Spondylolisthesis. Global Spine J. 2022, 12, 70–78. [Google Scholar] [CrossRef]
- Phani Kiran, S.; Sudhir, G. Minimally invasive transforaminal lumbar interbody fusion—A narrative review on the present status. J. Clin. Orthop. Trauma. 2021, 22, 101592. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, A.G.; Carandang, G.; Ghanayem, A.J.; Havey, R.M.; Cunningham, B.; Voronov, L.I.; Phillips, F.M. Compressive preload improves the stability of anterior lumbar interbody fusion cage constructs. J. Bone Joint Surg. Am. 2003, 85, 1749–1756. [Google Scholar] [CrossRef]
- Xu, S.; Zang, L.; Lu, Q.; Zhao, P.; Wu, Q.; Chen, X. Characteristics of interbody bone graft fusion after transforaminal lumbar interbody fusion according to intervertebral space division. Front. Surg. 2022, 9, 1004230. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pseudoarthrosis n (%) | Possible n (%) | Probable n (%) | Definitive n (%) | Region\Lee’s Criteria |
|---|---|---|---|---|
| - | - | 4 (8) | 44 (92) | Posterolateral area |
| - | 3 (6) | 20 (42) | 25 (52) | Intervertebral body area |
| 95% Confidence Interval | Odds Ratio | |
|---|---|---|
| 1.02 to 247.3 | 15.9 | Fusion area (PL) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Essa, A.; Shehade, M.; Rabau, O.; Smorgick, Y.; Mirovsky, Y.; Anekstein, Y. Fusion’s Location and Quality within the Fixated Segment Following Transforaminal Interbody Fusion (TLIF). Healthcare 2023, 11, 2814. https://doi.org/10.3390/healthcare11212814
Essa A, Shehade M, Rabau O, Smorgick Y, Mirovsky Y, Anekstein Y. Fusion’s Location and Quality within the Fixated Segment Following Transforaminal Interbody Fusion (TLIF). Healthcare. 2023; 11(21):2814. https://doi.org/10.3390/healthcare11212814
Chicago/Turabian StyleEssa, Ahmad, Munder Shehade, Oded Rabau, Yossi Smorgick, Yigal Mirovsky, and Yoram Anekstein. 2023. "Fusion’s Location and Quality within the Fixated Segment Following Transforaminal Interbody Fusion (TLIF)" Healthcare 11, no. 21: 2814. https://doi.org/10.3390/healthcare11212814
APA StyleEssa, A., Shehade, M., Rabau, O., Smorgick, Y., Mirovsky, Y., & Anekstein, Y. (2023). Fusion’s Location and Quality within the Fixated Segment Following Transforaminal Interbody Fusion (TLIF). Healthcare, 11(21), 2814. https://doi.org/10.3390/healthcare11212814