
Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study


 , ,
, , 
 and
and 
Abstract
:1. Introduction
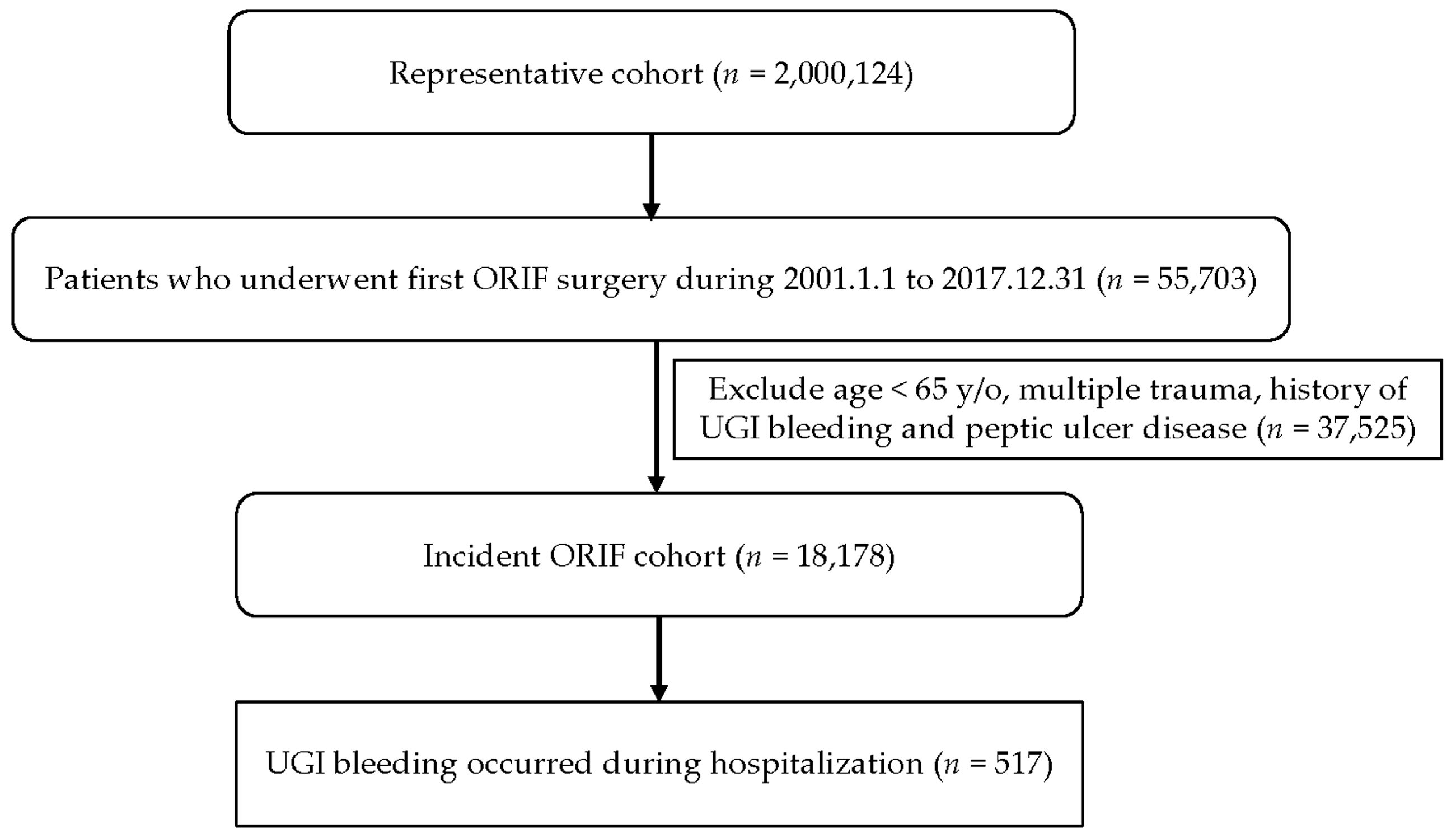
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Pilkington, K.B.; Wagstaff, M.J.D.; Greenwood, J.E. Prevention of gastrointestinal bleeding due to stress ulceration: A review of current literature. Anaesth. Intensive Care. 2012, 40, 253–259. [Google Scholar] [CrossRef]
- Alhazzani, W.; Alenezi, F.; Jaeschke, R.Z.; Moayyedi, P.; Cook, D.J. Proton pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in critically ill patients: A systematic review and meta-analysis. Crit. Care Med. 2013, 41, 693–705. [Google Scholar] [CrossRef]
- Rocos, B.; Whitehouse, M.R.; Kelly, M.B. Resuscitation in hip fractures: A systematic review. BMJ Open 2017, 7, e015906. [Google Scholar] [CrossRef]
- Hip Fracture: Management, Clinical Guideline [CG124]. 2011. Available online: https://www.nice.org.uk/guidance/cg124 (accessed on 28 June 2022).
- Liu, J.; Gupta, R.; Hay, K.; Pulle, C.; Rahman, T.; Pandy, S. Upper gastrointestinal bleeding in neck of femur fracture patients: A single tertiary centre experience. Intern. Med. J. 2018, 48, 731–735. [Google Scholar] [CrossRef]
- Chuene, M.A.; Pietrzak, J.R.T.; Sekeitto, A.R.; Mokete, L. Should we routinely prescribe proton pump inhibitors peri-operatively in elderly patients with hip fractures? A review of the literature. EFORT Open Rev. 2021, 6, 686–691. [Google Scholar] [CrossRef]
- Jantzen, C.; Madsen, C.M.; Abrahamsen, B.; Van Der Mark, S.; Duus, B.R.; Howland, J.; Lauritzen, J.B.; Jørgensen, H.L. Pre-fracture medication use as a predictor of 30-day mortality in hip fracture patients: An analysis of 141,201 patients. Hip Int. 2020, 30, 101–106. [Google Scholar] [CrossRef]
- Plummer, M.P.; Blaser, A.R.; Deane, A.M. Stress ulceration: Prevalence, pathology and association with adverse outcomes. Crit. Care 2014, 18, 213. [Google Scholar] [CrossRef]
- Ostermann, M.; Sprigings, D. Chapter 1. In Acute Medicine: A Practical Guide to the Management of Medical Emergencies, 5th ed.; Wiley-Blackwell: Oxford, UK, 2017. [Google Scholar]
- Sevransky, J.E.; Checkley, W.; Herrera, P.; Pickering, B.W.; Barr, J.; Brown, S.M.; Chang, S.Y.; Chong, D.; Kaufman, D.; Fremont, R.D.; et al. Protocols and hospital mortality in critically ill patients: The United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study. Crit. Care Med. 2015, 43, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Guyatt, G.; Alshahrani, M.; Deane, A.M.; Marshall, J.C.; Hall, R.; Muscedere, J.; English, S.W.; Lauzier, F.; Thabane, L.; et al. Withholding Pantoprazole for stress ulcer prophylaxis in critically ill patients: A plot randomized clinical trial and meta-analysis. Crit. Care Med. 2017, 45, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Ackland, G.; Grocott, M.P.W.; Mythen, M.G. Understanding gastrointestinal perfusion in critical care: So near, and yet so far. Crit. Care 2020, 4, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, A.; Chattopadhyay, R.; Mitra, S.; Crowe, S.E. Oxidative stress: An essential factor in the pathogenesis of gastrointestinal mucosal diseases. Physiol. Rep. 2014, 94, 329–354. [Google Scholar] [CrossRef]
- Cryer, B.; Mahaffey, K.W. Gastrointestinal ulcers, role of aspirin, and clinical outcomes: Pathobiology, diagnosis, and treatment. J. Multidiscip. Healthc. 2014, 7, 137–146. [Google Scholar] [CrossRef]
- Lalmohamed, A.; Vestergaard, P.; Javaid, M.K.; de Boer, A.; Leufkens, H.G.; van Staa, T.P.; de Vries, F. Risk of gastrointestinal bleeding in patients undergoing total hip or knee replacement compared with matched controls: A nationwide cohort study. Am. J. Gastroenterol. 2013, 108, 1277–1285. [Google Scholar] [CrossRef]
- Taha, A.S.; McCloskey, C.; Craigen, T.; Simpson, A.; Angerson, W.J. Occult vs. overt upper gastrointestinal bleeding: Inverse relationship and the use of mucosal damaging and protective drugs. Aliment. Pharmacol. Ther. 2015, 42, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Chan, F.K.L.; Ching, J.Y.L.; Tse, Y.K.; Lam, K.; Wong, G.L.H.; Ng, S.C.; Lee, V.; Au, K.W.L.; Cheong, P.K.; Suen, B.Y.; et al. Gastrointestinal safety of celecoxib versus naproxen in patients with cardiothrombotic diseases and arthritis after upper gastrointestinal bleeding (CONCERN): An industry-independent, double-blind, double-dummy, randomised trial. Lancet 2017, 389, 2375–2382. [Google Scholar] [CrossRef] [PubMed]
- Barkun, A.N.; Almadi, M.; Kuipers, E.J.; Laine, L.; Sung, J.; Tse, F.; Leontiadis, G.I.; Abraham, N.S.; Calvet, X.; Chan, F.K.L.; et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations From the International Consensus Group. Ann. Intern. Med. 2019, 171, 805–822. [Google Scholar] [CrossRef]
- Brozek, W.; Reichardt, B.; Zwerina, J.; Dimai, H.P.; Klaushofer, K.; Zwettler, E. Use of proton pump inhibitors and mortality after hip fracture in a nationwide study. Osteoporos. Int. 2017, 28, 1587–1595. [Google Scholar] [CrossRef]
- Kim, S.H.; Han, K.; Kang, G.; Lee, S.W.; Park, C.M.; Cho, J.; Choi, J.W.; Park, S.J.; Kang, M.; Kim, T.J.; et al. Risk of Postoperative Gastrointestinal Bleeding and Its Associated Factors: A Nationwide Population-Based Study in Korea. J. Pers. Med. 2021, 11, 1222. [Google Scholar] [CrossRef] [PubMed]
- Lv, H.; Yin, P.; Long, A.; Gao, Y.; Zhao, Z.; Li, J.; Zhang, L.; Zhang, L.; Tang, P. Clinical characteristics and risk factors of postoperative pneumonia after hip fracture surgery: A prospective cohort study. Osteoporos. Int. 2016, 27, 3001–3009. [Google Scholar] [CrossRef] [PubMed]
- Salarbaks, A.M.; Lindeboom, R.; Nijmeijer, W. Pneumonia in hospitalized elderly hip fracture patients: The effects on length of hospital-stay, in-hospital and thirty-day mortality and a search for potential predictors. Injury 2020, 51, 1846–1850. [Google Scholar] [CrossRef]
- Wang, X.; Dai, L.; Zhang, Y.; Lv, Y. Gender and low albumin and oxygen levels are risk factors for perioperative pneumonia in geriatric hip fracture patients. Clin. Interv. Aging 2020, 15, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.C.; Muo, C.H.; Wang, I.K.; Chang, C.T.; Chou, C.Y.; Liu, J.H.; Yen, T.H.; Huang, C.C.; Chung, C.J. Peptic ulcer disease risk in chronic kidney disease: Ten-year incidence, ulcer location, and ulcerogenic effect of medications. PLoS ONE 2014, 9, e87952. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.W.; Leu, H.B.; Luo, J.C.; Chan, W.L.; Hou, M.C.; Lin, H.C.; Lee, F.Y.; Kuan, Y.C. Different peptic ulcer bleeding risk in chronic kidney disease and end-stage renal disease patients receiving different dialysis. Dig. Dis. Sci. 2014, 59, 807–813. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Research Database. Data Subsets [Cited March 1 2018]. Available online: https://nhird.nhri.org.tw/en/Data_Subsets.html (accessed on 29 March 2019).
- Yoshioka, T.; Nishida, T.; Tsujii, M.; Kato, M.; Hayashi, Y.; Komori, M.; Yoshihara, H.; Nakamura, T.; Egawa, S.; Yoshio, T.; et al. Renal dysfunction is an independent risk factor for bleeding after gastric ESD. Endosc. Int. Open 2015, 3, E39–E45. [Google Scholar] [CrossRef]
- Dahiya, D.S.; Mandoorah, S.; Gangwani, M.K.; Ali, H.; Merza, N.; Aziz, M.; Singh, A.; Perisetti, A.; Garg, R.; Cheng, C.I.; et al. A Comparative Analysis of Bleeding Peptic Ulcers in Hospitalizations With and Without End-Stage Renal Disease. Gastroenterol. Res. 2023, 16, 17–24. [Google Scholar] [CrossRef]
- Peiffer, S.; Pelton, M.; Keeney, L.; Kwon, E.G.; Ofosu-Okromah, R.; Acharya, Y.; Chinchilli, V.M.; Soybel, D.I.; Oh, J.S.; Ssentongo, P. Risk factors of perioperative mortality from complicated peptic ulcer disease in Africa: Systematic review and meta-analysis. BMJ Open Gastroenterol. 2020, 7, e000350. [Google Scholar] [CrossRef]
- Sivaram, P.; Sreekumar, A. Preoperative factors influencing mortality and morbidity in peptic ulcer perforation. Eur. J. Trauma Emerg. Surg. 2018, 44, 251–257. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Atinga, A.; Shekkeris, A.; Fertleman, M.; Batrick, N.; Kashef, E.; Dick, E. Trauma in the elderly patient. Br. J. Radiol. 2018, 91, 20170739. [Google Scholar] [CrossRef]
- Buendgens, L.; Koch, A.; Tacke, F. Prevention of stress-related ulcer bleeding at the intensive care unit: Risks and benefits of stress ulcer prophylaxis. World J. Crit. Care Med. 2016, 5, 57–64. [Google Scholar] [CrossRef]
- Ye, Z.; Reintam Blaser, A.; Lytvyn, L.; Wang, Y.; Guyatt, G.H.; Mikita, J.S.; Roberts, J.; Agoritsas, T.; Bertschy, S.; Boroli, F.; et al. Gastrointestinal bleeding prophylaxis for critically ill patients: A clinical practice guideline. BMJ 2020, 368, l6722. [Google Scholar] [CrossRef] [PubMed]
- Yadlapati, R.; Gyawali, C.P.; Pandolfino, J.E.; CGIT GERD Consensus Conference Participants. AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review. Clin. Gastroenterol. Hepatol. 2022, 20, 984–994.e1. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, I.; Elgendy, I.Y.; Dicks, A.B.; Marchena, P.J.; Malý, R.; Francisco, I.; Pedrajas, J.M.; Font, C.; Hernández-Blasco, L.; Monreal, M.; et al. Comparison of Presentation, Treatment, and Outcomes of Venous Thromboembolism in Long-Term Immobile Patients Based on Age. J. Gen. Intern. Med. 2023, 38, 1877–1886. [Google Scholar] [CrossRef]
- Dahm, K.T.; Myrhaug, H.T.; Strømme, H.; Fure, B.; Brurberg, K.G. Effects of preventive use of compression stockings for elderly with chronic venous insufficiency and swollen legs: A systematic review and meta-analysis. BMC Geriatr. 2019, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, H.K.; Kim, B.S.; Han, K.D.; Park, J.B.; Lee, H.; Lee, S.P.; Kim, Y.J. Risk of upper gastrointestinal bleeding in patients on oral anticoagulant and proton pump inhibitor co-therapy. PLoS ONE 2021, 16, e0253310. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, S.I.; Nagarekha, D.; Hegade, G.; Marutheesh, M. Postoperative nausea and vomiting: A simple yet complex problem. Anesth. Essays Res. 2016, 10, 388–396. [Google Scholar] [CrossRef]
- Niedermeier, S.R.; Crouser, N.; Hidden, K.; Jain, S.A. Pain Management following Open Reduction and Internal Fixation of Distal Radius Fractures. J. Wrist Surg. 2021, 10, 27–30. [Google Scholar] [CrossRef]
- Kanno, T.; Moayyedi, P. Who Needs Gastroprotection in 2020? Curr. Treat. Options Gastroenterol. 2020, 18, 557–573. [Google Scholar] [CrossRef]
- Kamada, T.; Satoh, K.; Itoh, T.; Ito, M.; Iwamoto, J.; Okimoto, T.; Kanno, T.; Sugimoto, M.; Chiba, T.; Nomura, S.; et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2020. J. Gastroenterol. 2021, 56, 303–322. [Google Scholar] [CrossRef]
- Coxib and traditional NSAID Trialists’ (CNT) Collaboration; Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: Meta-analyses of individual participant data from randomised trials. Lancet 2013, 382, 769–779. [Google Scholar] [CrossRef]
- Ishii, M.; Kawai, T.; Tsujita, K.; Igarashi, A.; Suzuki, M.; Deguchi, H.; Fernandez, J. Cost-Effectiveness of Vonoprazan Compared With Proton Pump Inhibitors in Patients Taking Low-Dose Aspirin for Secondary Prevention of Cardiovascular Events in Japan. Circ. J. 2023, 87, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, K. Ethical Considerations in Trauma-Informed Care. Psychiatr. Clin. N. Am. 2021, 44, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Yüksel, I.; Usküdar, O.; Köklü, S.; Başar, O.; Gültuna, S.; Unverdi, S.; Oztürk, Z.A.; Sengül, D.; Arikök, A.T.; Yüksel, O.; et al. Inlet patch: Associations with endoscopic findings in the upper gastrointestinal system. Scand. J. Gastroenterol. 2008, 43, 910–914. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Male | Female | Total |
|---|---|---|---|
| N | 6162 | 12,016 | 18,178 |
| Age | 77.9 ± 7.5 | 77.4 ± 7.6 | 77.6 ± 7.5 |
| Age Group | - | - | - |
| 65–74 y/o | 2146 (34.8%) | 4598 (38.2%) | 6744 (37.1%) |
| 75–84 y/o | 2705 (43.9%) | 5019 (41.8%) | 7724 (42.5%) |
| ≥85 y/o | 1311 (21.3%) | 2399 (20.0%) | 3710 (20.4%) |
| Fracture site | - | - | - |
| Upper major limb | 1484 (24.1%) | 5275 (43.9%) | 6759 (37.2%) |
| Lower major limb | 4678 (75.9%) | 6741 (56.1%) | 11,419 (62.8%) |
| Hypertension (%) | 2929 (47.5%) | 6727 (56.0%) | 9656 (53.1%) |
| Diabetes mellitus (%) | 1288 (20.9%) | 3568 (29.7%) | 4856 (26.7%) |
| Dyslipidemia (%) | 703 (11.4%) | 2362 (19.7%) | 3065 (16.9%) |
| Coronary artery disease (%) | 980 (15.9%) | 1782 (14.8%) | 2762 (15.2%) |
| Cerebrovascular accident (%) | 1217 (19.8%) | 1843 (15.3%) | 3060 (16.8%) |
| Chronic liver disease (%) | 260 (4.2%) | 548 (4.6%) | 808 (4.4%) |
| Chronic renal disease (%) | 356 (5.8%) | 461 (3.8%) | 817 (4.5%) |
| Psychiatric disorders (%) | 1217 (19.8%) | 2866 (23.9%) | 4083 (22.5%) |
| Osteoporosis (%) | 300 (4.9%) | 1357 (11.3%) | 1657 (9.1%) |
| Peripheral vascular disease (%) | 433 (7.0%) | 700 (5.8%) | 1133 (6.2%) |
| Upper gastrointestinal bleeding (%) | 241 (3.9%) | 276 (2.3%) | 517 (2.8%) |
| Variables | Crude | Adjusted | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Age | 1.03 (1.02, 1.05) | <0.001 * | 1.02 (1.00, 1.03) | 0.008 * |
| Gender (Male vs. Female) | 1.73 (1.45, 2.06) | <0.001 * | 1.46 (1.21, 1.75) | <0.001 * |
| Fracture site (Lower major limb vs. Upper major limb) | 3.18 (2.51, 4.03) | <0.001 * | 2.65 (2.06, 3.41) | <0.001 * |
| Hypertension vs. None | 1.04 (0.87, 1.23) | 0.696 | 1.01 (0.84, 1.23) | 0.879 |
| Diabetes mellitus vs. None | 1.02 (0.84, 1.24) | 0.849 | 1.01 (0.81, 1.25) | 0.959 |
| Dyslipidemia vs. None | 0.85 (0.66, 1.08) | 0.184 | 0.98 (0.75, 1.27) | 0.875 |
| Coronary artery disease vs. None | 1.13 (0.90, 1.43) | 0.294 | 1.02 (0.80, 1.30) | 0.897 |
| Cerebrovascular accident vs. None | 1.06 (0.84, 1.33) | 0.636 | 0.92 (0.72, 1.16) | 0.479 |
| Chronic liver disease vs. None | 1.24 (0.84, 1.83) | 0.278 | 1.32 (0.89, 1.96) | 0.167 |
| Chronic renal disease vs. None | 2.41 (1.79, 3.25) | <0.001 * | 2.12 (1.56, 2.89) | <0.001 * |
| Psychiatric disorders vs. None | 0.99 (0.81, 1.23) | 0.989 | 0.98 (0.79, 1.21) | 0.826 |
| Osteoporosis vs. None | 0.95 (0.70, 1.29) | 0.742 | 0.99 (0.73, 1.36) | 0.984 |
| Peripheral vascular disease vs. None | 1.24 (0.89, 1.72) | 0.212 | 1.06 (0.75, 1.48) | 0.745 |
| Variables | Crude | Adjusted | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Age | 1.04 (1.03, 1.05) | <0.001 * | 1.02 (1.00, 1.03) | 0.017 * |
| Gender (Male vs. Female) | 1.87 (1.50, 2.34) | <0.001 * | 1.52 (1.21, 1.92) | <0.001 * |
| Fracture site (Lower major limb vs. Upper major limb) | 3.59 (2.67, 4.85) | <0.001 * | 2.91 (2.11, 4.00) | <0.001 * |
| Hypertension vs. None | 0.98 (0.78, 1.22) | 0.847 | 1.02 (0.80, 1.29) | 0.902 |
| Diabetes mellitus vs. None | 0.88 (0.68, 1.16) | 0.370 | 0.89 (0.66, 1.20) | 0.432 |
| Dyslipidemia vs. None | 0.72 (0.50, 1.02) | 0.068 | 0.92 (0.63, 1.34) | 0.655 |
| Chronic liver disease vs. None | 1.30 (0.79, 2.13) | 0.305 | 1.48 (0.89, 2.45) | 0.127 |
| Chronic renal disease vs. None | 2.72 (1.80, 4.12) | <0.001 * | 2.49 (1.63, 3.81) | <0.001 * |
| Psychiatric disorders vs. None | 1.03 (0.78, 1.36) | 0.846 | 1.02 (0.76, 1.35) | 0.915 |
| Osteoporosis vs. None | 0.87 (0.57, 1.33) | 0.525 | 0.91 (0.60, 1.40) | 0.676 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.-Y.; Wu, W.-T.; Lee, R.-P.; Chen, I.-H.; Yu, T.-C.; Wang, J.-H.; Yeh, K.-T. Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study. Healthcare 2023, 11, 2853. https://doi.org/10.3390/healthcare11212853
Chen G-Y, Wu W-T, Lee R-P, Chen I-H, Yu T-C, Wang J-H, Yeh K-T. Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study. Healthcare. 2023; 11(21):2853. https://doi.org/10.3390/healthcare11212853
Chicago/Turabian StyleChen, Guan-Yu, Wen-Tien Wu, Ru-Ping Lee, Ing-Ho Chen, Tzai-Chiu Yu, Jen-Hung Wang, and Kuang-Ting Yeh. 2023. "Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study" Healthcare 11, no. 21: 2853. https://doi.org/10.3390/healthcare11212853
APA StyleChen, G. -Y., Wu, W. -T., Lee, R. -P., Chen, I. -H., Yu, T. -C., Wang, J. -H., & Yeh, K. -T. (2023). Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study. Healthcare, 11(21), 2853. https://doi.org/10.3390/healthcare11212853