
Effects of Different Protocols of Moderate-Intensity Intermittent Hypoxic Training on Mental Health and Quality of Life in Brazilian Adults Recovered from COVID-19: The AEROBICOVID Double-Blind Randomized Controlled Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
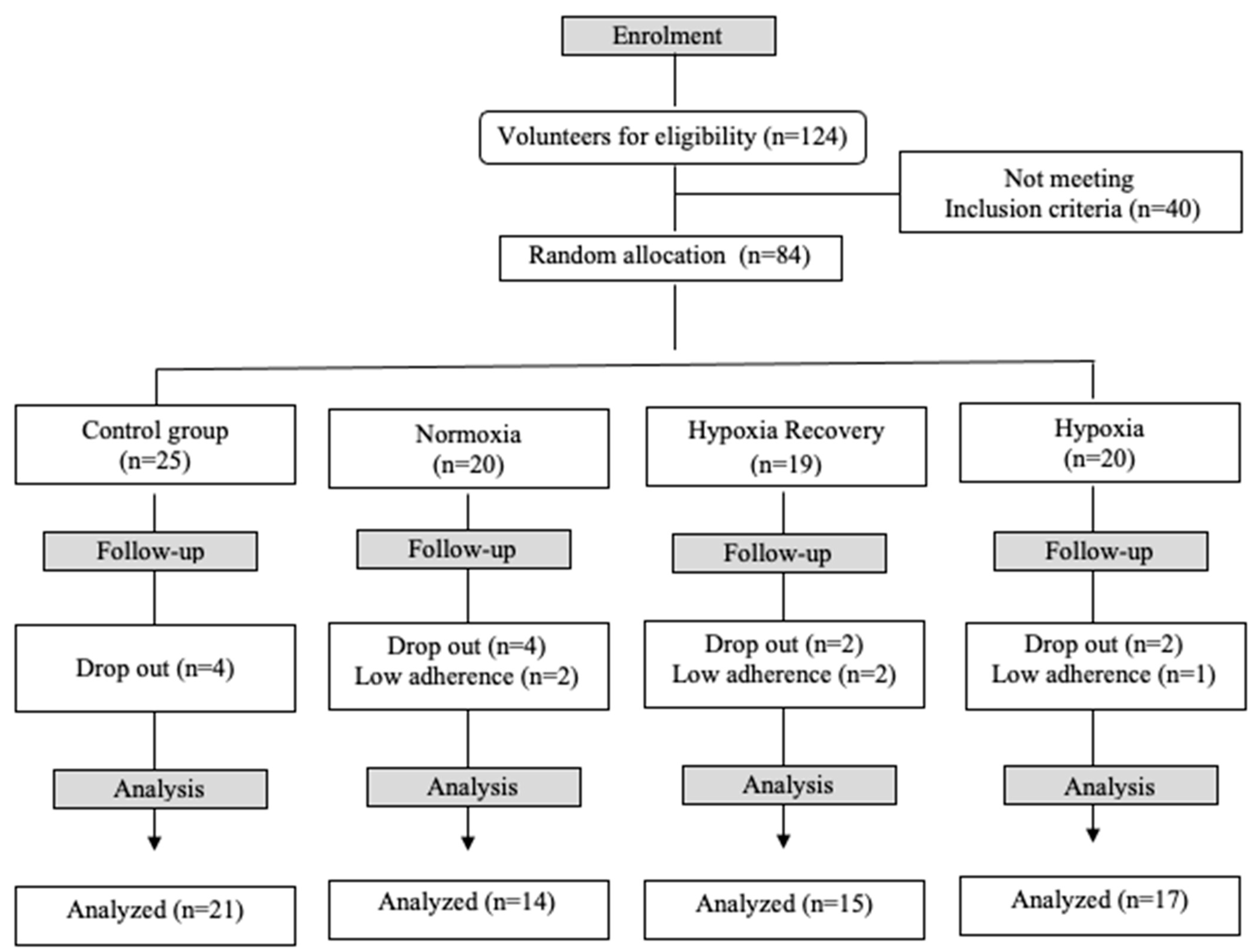
2.1. Participants
2.2. Intervention Protocol
2.3. Data Collection
2.3.1. PAR-Q and Anamnesis
2.3.2. Anthropometric Measurements
2.3.3. Questionnaires
2.3.4. Statistical Analysis
3. Results
3.1. Participant’s Characteristics
3.2. Quality of Life and Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronavirus COVID-19 (2019-nCoV). 2023. Available online: https://gisanddata.maps.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6 (accessed on 20 January 2023).
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Martínez, B.J.S.-A.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Chi, X.; Becker, B.; Yu, Q.; Willeit, P.; Jiao, C.; Huang, L.; Hossain, M.M.; Grabovac, I.; Yeung, A.; Lin, J.; et al. Prevalence and Psychosocial Correlates of Mental Health Outcomes Among Chinese College Students During the Coronavirus Disease (COVID-19) Pandemic. Front. Psychiatry 2020, 11, 803. [Google Scholar] [CrossRef]
- Bourmistrova, N.W.; Solomon, T.; Braude, P.; Strawbridge, R.; Carter, B. Long-term effects of COVID-19 on mental health: A systematic review. J. Affect. Disord. 2021, 299, 118–125. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Lardone, A.; Sorrentino, P.; Giancamilli, F.; Palombi, T.; Simper, T.; Mandolesi, L.; Lucidi, F.; Chirico, A.; Galli, F. Psychosocial variables and quality of life during the COVID-19 lockdown: A correlational study on a convenience sample of young Italians. PeerJ 2020, 8, e10611. [Google Scholar] [CrossRef]
- de Souza, I.M.; Machado-De-Sousa, J.P. Brazil: World leader in anxiety and depression rates. Rev. Bras. Psiquiatr. 2017, 39, 384. [Google Scholar] [CrossRef]
- Filgueiras, A.; Stults-Kolehmainen, M. Risk Factors for Potential Mental Illness Among Brazilians in Quarantine Due To COVID-19. Psychol. Rep. 2021, 125, 723–741. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Santamaría, G.; Sánchez-Serrano, N.; Caeiro, E.L.; Seco-Calvo, J. Efficacy of Therapeutic Exercise in Reversing Decreased Strength, Impaired Respiratory Function, Decreased Physical Fitness, and Decreased Quality of Life Caused by the Post-COVID-19 Syndrome. Viruses 2022, 14, 2797. [Google Scholar] [CrossRef]
- Alves, W.M.; Alves, T.G.; Ferreira, R.M.; Lima, T.A.; Pimentel, C.P.; Sousa, E.C.; Abrahin, O.; Alves, E.A. Strength training improves the respiratory muscle strength and quality of life of elderly with Parkinson disease. SSRN Electron. J. 2019, 59, 1756–1762. [Google Scholar] [CrossRef]
- Amini, A.; Vaezmousavi, M.; Shirvani, H. Comparing the effect of individual and group cognitive-motor training on reconstructing subjective well-being and quality of life in older males, recovered from the COVID-19. Cogn. Process. 2023, 24, 361–374. [Google Scholar] [CrossRef]
- Aryana, I.G.P.S.; Setiati, S.; Paulus, I.B.; Daniella, D. Appropriate Timing and Type of Physical Training in Patients with COVID-19 for Muscle Health and Quality of Life: A Systematic Review. J. Nutr. Metab. 2022, 2022, 6119593. [Google Scholar] [CrossRef]
- Schega, L.; Peter, B.; Törpel, A.; Mutschler, H.; Isermann, B.; Hamacher, D. Effects of Intermittent Hypoxia on Cognitive Performance and Quality of Life in Elderly Adults: A Pilot Study. Gerontology 2013, 59, 316–323. [Google Scholar] [CrossRef]
- Kleim, J.; Cooper, N.R.; VandenBerg, P.M. Exercise induces angiogenesis but does not alter movement representations within rat motor cortex. Brain Res. 2002, 934, 1–6. [Google Scholar] [CrossRef]
- Faulhaber, M.; Gröbner, K.; Rausch, L.; Gatterer, H.; Menz, V. Effects of Acute Hypoxia on Lactate Thresholds and High-Intensity Endurance Performance—A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 7573. [Google Scholar] [CrossRef]
- Rybnikova, E.; Vataeva, L.; Tyulkova, E.; Gluschenko, T.; Otellin, V.; Pelto-Huikko, M.; Samoilov, M.O. Mild hypoxia preconditioning prevents impairment of passive avoidance learning and suppression of brain NGFI-A expression induced by severe hypoxia. Behav. Brain Res. 2005, 160, 107–114. [Google Scholar] [CrossRef]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef]
- Glazachev, O.; Kopylov, P.; Susta, D.; Dudnik, E.; Zagaynaya, E. Adaptations following an intermittent hypoxia-hyperoxia training in coronary artery disease patients: A controlled study. Clin. Cardiol. 2017, 40, 370–376. [Google Scholar] [CrossRef]
- Burtscher, J.; Niedermeier, M.; Hüfner, K.; Burg, E.v.D.; Kopp, M.; Stoop, R.; Burtscher, M.; Gatterer, H.; Millet, G.P. The interplay of hypoxic and mental stress: Implications for anxiety and depressive disorders. Neurosci. Biobehav. Rev. 2022, 138, 104718. [Google Scholar] [CrossRef]
- Schega, L.; Peter, B.; Brigadski, T.; Leßmann, V.; Isermann, B.; Hamacher, D.; Törpel, A. Effect of intermittent normobaric hypoxia on aerobic capacity and cognitive function in older people. J. Sci. Med. Sport 2016, 19, 941–945. [Google Scholar] [CrossRef]
- Syrkin, A.L.; Glazachev, O.; Kopylov, F.Y.; Dudnik, E.; Zagaynaya, E.; Tuter, D.S. Adaptation to Intermittent Hypoxia-Hyperoxia in the Rehabilitation of Patients with Ischemic Heart Disease: Exercise Tolerance and Quality of Life. Kardiologiia 2017, 57, 10–16. [Google Scholar]
- Burtscher, J.; Mallet, R.T.; Burtscher, M.; Millet, G.P. Hypoxia and brain aging: Neurodegeneration or neuroprotection? Ageing Res. Rev. 2021, 68, 101343. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Chen, X.; Shan, J.; Yang, R.; Guo, Q.; Bi, X.; Xu, P.; Shi, X.; Chu, L.; Wang, L. Intermittent Hypoxic Preconditioning: A Potential New Powerful Strategy for COVID-19 Rehabilitation. Front. Pharmacol. 2021, 12, 643619. [Google Scholar] [CrossRef]
- Trapé, Á.A.; Camacho-Cardenosa, M.; Camacho-Cardenosa, A.; Merellano-Navarro, E.; Rodrigues, J.A.L.; Lizzi, E.A.d.S.; Sorgi, C.A.; Papoti, M.; Brazo-Sayavera, J. Effects of moderate-intensity intermittent hypoxic training on health outcomes of patients recovered from COVID-19: The AEROBICOVID study protocol for a randomized controlled trial. Trials 2021, 22, 534. [Google Scholar] [CrossRef]
- Hogg, R.; Tanis, E.; Zimmerman, D. Probability and Statistical Inference, 9th ed.; Publications, Inc.: Thousand Oaks, CA, USA, 2015. [Google Scholar] [CrossRef]
- de Carvalho, C.D.; Bertucci, D.R.; Ribeiro, F.A.; Costa, G.P.; Toro, D.M.; Camacho-Cardenosa, M.; Brazo-Sayavera, J.; Sorgi, C.A.; Papoti, M.; Trapé, Á.A. Effects of Moderate-Intensity Training Under Cyclic Hypoxia on Cardiorespiratory Fitness and Hematological Parameters in People Recovered From COVID-19: The AEROBICOVID Study. Sports Health A Multidiscip. Approach 2022, 15, 558–570. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshalm, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Maggiorini, M.; Müller, A.; Hofstetter, D.; Bärtsch, P.; Oelz, O. Assessment of acute mountain sickness by different score protocols in the Swiss Alps. Aviat. Space Environ. Med. 1998, 69, 1186–1192. [Google Scholar]
- Costa, G.P.; Camacho-Cardenosa, A.; Brazo-Sayavera, J.; Viliod, M.C.D.L.; Camacho-Cardenosa, M.; Foresti, Y.F.; de Carvalho, C.D.; Merellano-Navarro, E.; Papoti, M.; Trapé, A. Effectiveness, implementation, and monitoring variables of intermittent hypoxic bicycle training in patients recovered from COVID-19: The AEROBICOVID study. Front. Physiol. 2022, 13, 977519. [Google Scholar] [CrossRef]
- Galloway, J.B.; Norton, S.; Barker, R.D.; Brookes, A.; Carey, I.; Clarke, B.D.; Jina, R.; Reid, C.; Russell, M.D.; Sneep, R.; et al. A clinical risk score to identify patients with COVID-19 at high risk of critical care admission or death: An observational cohort study. J. Infect. 2020, 81, 282–288. [Google Scholar] [CrossRef]
- WHO. Consultation on Obesity (1999: Geneva, Switzerland) & World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. World Health Organization. 2000. Available online: https://apps.who.int/iris/handle/10665/42330 (accessed on 8 October 2023).
- Ferreira, M.G.; Valente, J.G.; Gonçalves-Silva, R.M.V.; Sichieri, R. Acurácia da circunferência da cintura e da relação cintura/quadril como preditores de dislipidemias em estudo transversal de doadores de sangue de Cuiabá, Mato Grosso, Brasil. Cad. Saude Publica 2006, 22, 307–314. [Google Scholar] [CrossRef]
- Matsudo, S.; Araújo, T.; Marsudo, V.; Andrade, D.; Andrade, E.; Braggion, G.J.R. Questionário Internacional De Atividade Física (Ipaq): Estupo De Validade E Reprodutibilidade No Brasil. Rev. Bras. Ativ. Fís. Saúde 2012, 6, 5–18. [Google Scholar] [CrossRef]
- Camelier, A.A. [UNIFESP]. Avaliação da Qualidade de vida Relacionada a Saúde em Pacientes com DPOC: Estudo de Base Populacional com o SF-12 na Cidade de São Paulo. 2004. Available online: https://repositorio.unifesp.br/handle/11600/20321 (accessed on 8 October 2023).
- Vignola, R.C.B.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed]
- Singhal, T. A Review of Coronavirus Disease—2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Gerth, A.M.J.; Hatch, R.A.; Young, J.D.; Watkinson, P.J. Changes in health-related quality of life after discharge from an intensive care unit: A systematic review. Anaesthesia 2019, 74, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.; Verges, S.; Hérengt, F. Effectiveness of pulmonary rehabilitation in COVID-19 respiratory failure patients post-ICU. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef] [PubMed]
- Baratto, C.; Caravita, S.; Faini, A.; Perego, G.B.; Senni, M.; Badano, L.P.; Parati, G. Impact of COVID-19 on exercise pathophysiology: A combined cardiopulmonary and echocardiographic exercise study. J. Appl. Physiol. 2021, 130, 1470–1478. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Jeffries, O.; Patterson, S.D.; Waldron, M. The effect of severe and moderate hypoxia on exercise at a fixed level of perceived exertion. Eur. J. Appl. Physiol. 2019, 119, 1213–1224. [Google Scholar] [CrossRef]
- Adams, M.A.; Frank, L.D.; Schipperijn, J.; Smith, G.; Chapman, J.; Christiansen, L.B.; Coffee, N.; Salvo, D.; du Toit, L.; Dygrýn, J.; et al. International variation in neighborhood walkability, transit, and recreation environments using geographic information systems: The IPEN adult study. Int. J. Health Geogr. 2014, 13, 43. [Google Scholar] [CrossRef]
- Chapman, R.F.; Stager, J.M.; Tanner, D.A.; Stray-Gundersen, J.; Levine, B.D. Impairment of 3000-m Run Time at Altitude Is Influenced by Arterial Oxyhemoglobin Saturation. Med. Sci. Sports Exerc. 2011, 43, 1649–1656. [Google Scholar] [CrossRef] [PubMed]
- Girard, O.; Girard, I.M.; Peeling, P. Hypoxic conditioning: A novel therapeutic solution for load-compromised individuals to achieve similar exercise benefits by doing less mechanical work! Br. J. Sports Med. 2020, 55, 944–945. [Google Scholar] [CrossRef]


{kind=link}
| Control (n = 21) | Normoxia (n = 14) | Hypoxia Recovery (n = 15) | Hypoxia (n = 17) | p | |
|---|---|---|---|---|---|
| Age (years) | 48.0 (10.7) | 50.4 (9.5) | 47.5 (9.9) | 48.1 (9.9) | 0.8 |
| BMI (kg/m2) | 29.6 (4.6) | 29.0 (4.2) | 29.2 (5.8) | 30.7 (3.9) | 0.6 |
| W/H ratio | 0.87 (0.09) | 0.90 (0.06) | 0.90 (0.10) | 0.92 (0.10) | 0.7 |
| Total PA/week (min) | 522.1 (464.3) | 405.4 (511.5) | 385.7 (376.8) | 390.3 (469.4) | 0.7 |
| Total seated time/week (min) | 2351.9 (1304.2) | 2777.0 (928) | 2234.0 (1023.1) | 2735.9 (833.5) | 0.3 |
| Sex a | |||||
| Male | 8 (38.1) | 3 (21.4) | 6 (40.0) | 7 (41.2) | 0.6 |
| Female | 13 (61.9) | 11 (78.6) | 9 (60.0) | 10 (58.8) | |
| Presence of diseases a | |||||
| Diabetes | 4 (19.1) | 2 (14.3) | 2 (13.3) | 4 (23.5) | 0.9 |
| Hypertension | 3 (14.3) | 5 (35.7) | 4 (26.7) | 3 (17.7) | 0.4 |
| Asthma | 0 (0.0) | 1 (7.1) | 1 (6.7) | 1 (5.9) | 0.6 |
| COVID-19 Severity a | 0.5 | ||||
| Mild | 5 (23.8) | 3 (21.4) | 3 (20.0) | 3 (17.7) | |
| Moderate | 11 (52.4) | 7 (50.0) | 10 (66.7) | 13 (76.5) | |
| Severe | 4 (19.1) | 2 (14.3) | 0 (0.0) | 1 (5.9) | |
| Critical | 1 (4.8) | 2 (14.3) | 2 (13.3) | 0 (0.0) | |
| Control Group (n = 21) | Normoxia (n = 14) | Hypoxia Recovery (n = 15) | Hypoxia (n = 17) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post | Δ% | Baseline | Post | Δ% | Baseline | Post | Δ% | Baseline | Post | Δ% | |
| SF-12 Physical score | 47.3 (7.9) | 47.1 (8.3) | −0.4 | 42.1 (11.0) | 48.7 (7.0) * | 15.7 | 45.2 (7.7) | 53.2 (3.8) *$ | 17.7 | 45.8 (9.2) | 51.1 (5.3) * | 11.6 |
| SF-12 Mental score | 47.4 (10.8) | 46.9 (11.3) | −1.1 | 48.8 (7.9) | 54.6 (4.6) *$ | 11.2 | 46.9 (11.8) | 53.5 (6.6) * | 14.1 | 46.5 (9.7) | 52.0 (9.9) * | 11.8 |
| DASS-21 Depression score | 7.9 (8.8) | 7.6 (7.7) | −3.8 | 9.3 (9.1) | 3.1 (3.8) * | −66.7 | 6.4 (6.1) | 4.4 (5.6) | −31.2 | 10.0 (10.4) | 6.9 (7.9) * | −31.0 |
| DASS-21 Anxiety score | 7.1 (5.1) | 6.8 (6.7) | −4.2 | 11.4 (11.7) | 6.1 (6.8) * | −46.5 | 7.2 (7.2) | 3.9 (3.9) * | −45.9 | 10.9 (9.6) | 6.6 (5.7) * | −39.5 |
| DASS-21 Stress score | 11.5 (9.4) α | 12.3 (9.6) | 6.9 | 15.3 (10.3) | 9.1 (6.7) * | −40.6 | 11.3 (8.7) α | 7.2 (5.7) *α | −36.3 | 18.1 (10.3) | 14.1 (9.4) * | −22.1 |
| Depression | Anxiety | Stress | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No Risk | Risk | p | No Risk | Risk | p | No Risk | Risk | p | |
| Control Group | |||||||||
| Baseline (%) | 13 (61.9) | 8 (38.1) | 0.999 | 10 (47.6) | 11 (52.4) | 0.758 | 10 (47.6) | 11 (52.4) | 0.999 |
| Post (%) | 12 (57.1) | 9 (42.9) | 12 (57.1) | 9 (42.9) | 10 (47.6) | 11 (52.4) | |||
| Normoxia | |||||||||
| Baseline (%) | 9 (64.3) | 5 (35.7) | 0.165 | 6 (42.9) | 8 (57.1) | 0.450 | 8 (57.1) | 6 (42.9) | 0.999 |
| Post (%) | 13 (92.9) | 1 (7.1) | 9 (64.3) | 5 (35.7) | 8 (57.1) | 6 (42.9) | |||
| Hypoxia Recovery | |||||||||
| Baseline (%) | 9 (60.0) | 6 (40.0) | 0.215 | 9 (60.0) | 6 (40.0) | 0.215 | 7 (46.7) | 8 (53.3) | 0.462 |
| Post (%) | 13 (86.7) | 2 (13.3) | 13 (86.7) | 2 (13.3) | 10 (66.7) | 5 (33.3) | |||
| Hypoxia | |||||||||
| Baseline (%) | 10 (58.8) | 7 (41.2) | 0.465 | 7 (41.2) | 10 (58.8) | 0.494 | 5 (29.4) | 12 (70.6) | 0.999 |
| Post (%) | 13 (76.5) | 4 (23.5) | 10 (58.8) | 7 (41.2) | 6 (35.3) | 11 (64.7) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merellano-Navarro, E.; Camacho-Cardenosa, M.; Costa, G.P.; Wiggers, E.; Marcolino Putti, G.; Evandro Nogueira, J.; Aparecida da Silva Lizzi, E.; Trapé, Á.A. Effects of Different Protocols of Moderate-Intensity Intermittent Hypoxic Training on Mental Health and Quality of Life in Brazilian Adults Recovered from COVID-19: The AEROBICOVID Double-Blind Randomized Controlled Study. Healthcare 2023, 11, 3076. https://doi.org/10.3390/healthcare11233076
Merellano-Navarro E, Camacho-Cardenosa M, Costa GP, Wiggers E, Marcolino Putti G, Evandro Nogueira J, Aparecida da Silva Lizzi E, Trapé ÁA. Effects of Different Protocols of Moderate-Intensity Intermittent Hypoxic Training on Mental Health and Quality of Life in Brazilian Adults Recovered from COVID-19: The AEROBICOVID Double-Blind Randomized Controlled Study. Healthcare. 2023; 11(23):3076. https://doi.org/10.3390/healthcare11233076
Chicago/Turabian StyleMerellano-Navarro, Eugenio, Marta Camacho-Cardenosa, Gabriel Peinado Costa, Ester Wiggers, Germano Marcolino Putti, Jonatas Evandro Nogueira, Elisangela Aparecida da Silva Lizzi, and Átila Alexandre Trapé. 2023. "Effects of Different Protocols of Moderate-Intensity Intermittent Hypoxic Training on Mental Health and Quality of Life in Brazilian Adults Recovered from COVID-19: The AEROBICOVID Double-Blind Randomized Controlled Study" Healthcare 11, no. 23: 3076. https://doi.org/10.3390/healthcare11233076
APA StyleMerellano-Navarro, E., Camacho-Cardenosa, M., Costa, G. P., Wiggers, E., Marcolino Putti, G., Evandro Nogueira, J., Aparecida da Silva Lizzi, E., & Trapé, Á. A. (2023). Effects of Different Protocols of Moderate-Intensity Intermittent Hypoxic Training on Mental Health and Quality of Life in Brazilian Adults Recovered from COVID-19: The AEROBICOVID Double-Blind Randomized Controlled Study. Healthcare, 11(23), 3076. https://doi.org/10.3390/healthcare11233076