

Clinical Predictors for Upper Limb Recovery after Stroke Rehabilitation: Retrospective Cohort Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Intervention
2.2.1. Technology Devices
2.2.2. Conventional Therapy
2.2.3. Occupational Therapy
2.3. Clinical Data, Assessment and Outcome Measure
2.4. Sample Size
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabil. Neural Repair 2017, 31, 793–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, S.C. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann. Neurol. 2008, 63, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Smania, N.; Gandolfi, M.; Aglioti, S.M.; Girardi, P.; Fiaschi, A.; Girardi, F. How long is the recovery of global aphasia? Twenty-five years of follow-up in a patient with left hemisphere stroke. Neurorehabil. Neural Repair 2010, 24, 871–875. [Google Scholar] [CrossRef]
- McCabe, J.; Monkiewicz, M.; Holcomb, J.; Pundik, S.; Daly, J.J. Comparison of robotics, functional electrical stimulation, and motor learning methods for treatment of persistent upper extremity dysfunction after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 981–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, N.S.; Brander, F.; Kelly, K. Intensive upper limb neurorehabilitation in chronic stroke: Outcomes from the Queen Square programme. J. Neurol. Neurosurg. Psychiatry 2019, 90, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Salvalaggio, S.; Kiper, P.; Pregnolato, G.; Baldan, F.; Agostini, M.; Maistrello, L.; Turolla, A. Virtual Feedback for Arm Motor Function Rehabilitation after Stroke: A Randomized Controlled Trial. Healthcare 2022, 10, 1175. [Google Scholar] [CrossRef]
- Coupar, F.; Pollock, A.; Rowe, P.; Weir, C.; Langhorne, P. Predictors of upper limb recovery after stroke: A systematic review and meta-analysis. Clin. Rehabil. 2012, 26, 291–313. [Google Scholar] [CrossRef]
- Kiaer, C.; Lundquist, C.B.; Brunner, I. Knowledge and application of upper limb prediction models and attitude toward prognosis among physiotherapists and occupational therapists in the clinical stroke setting. Top Stroke Rehabil. 2021, 28, 135–141. [Google Scholar] [CrossRef]
- D’Imperio, D.; Romeo, Z.; Maistrello, L.; Durgoni, E.; Della Pietà, C.; De Filippo De Grazia, M.; Meneghello, F.; Turolla, A.; Zorzi, M. Sensorimotor, Attentional, and Neuroanatomical Predictors of Upper Limb Motor Deficits and Rehabilitation Outcome after Stroke. Neural Plast. 2021, 2021, 8845685. [Google Scholar] [CrossRef]
- Wondergem, R.; Pisters, M.F.; Wouters, E.J.; Olthof, N.; de Bie, R.A.; Visser-Meily, J.M.; Veenhof, C. The Course of Activities in Daily Living: Who Is at Risk for Decline after First Ever Stroke? Cerebrovasc. Dis. 2017, 43, 1–8. [Google Scholar] [CrossRef] [PubMed]
- VanGilder, J.L.; Hooyman, A.; Peterson, D.S.; Schaefer, S.Y. Post-stroke cognitive impairments and responsiveness to motor rehabilitation: A review. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Marwaa, M.N.; Kristensen, H.K.; Guidetti, S.; Ytterberg, C. Physiotherapists’ and occupational therapists’ perspectives on information and communication technology in stroke rehabilitation. PLoS ONE 2020, 15, e0236831. [Google Scholar] [CrossRef] [PubMed]
- Hayward, K.S.; Kramer, S.F.; Dalton, E.J.; Hughes, G.R.; Brodtmann, A.; Churilov, L.; Cloud, G.; Corbett, D.; Jolliffe, L.; Kaffenberger, T.; et al. Timing and Dose of Upper Limb Motor Intervention After Stroke: A Systematic Review. Stroke 2021, 52, 3706–3717. [Google Scholar] [CrossRef] [PubMed]
- Kundert, R.; Goldsmith, J.; Veerbeek, J.M.; Krakauer, J.W.; Luft, A.R. What the Proportional Recovery Rule Is (and Is Not): Methodological and Statistical Considerations. Neurorehabil. Neural Repair 2019, 33, 876–887. [Google Scholar] [CrossRef] [Green Version]
- Stinear, C.M.; Byblow, W.D.; Ackerley, S.J.; Smith, M.C.; Borges, V.M.; Barber, P.A. PREP2: A biomarker-based algorithm for predicting upper limb function after stroke. Ann. Clin. Transl. Neurol. 2017, 4, 811–820. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Baldan, F.; Turolla, A.; Rimini, D.; Pregnolato, G.; Maistrello, L.; Agostini, M.; Jakob, I. Robot-assisted rehabilitation of hand function after stroke: Development of prediction models for reference to therapy. J. Electromyogr. Kinesiol. 2021, 57, 102534. [Google Scholar] [CrossRef]
- Rimini, D.; Salvalaggio, S.; Pregnolato, G.; Alhelou, M.; Berlingieri, C.; Mascotto, E.; Turolla, A.; Ariano, P.; Celadon, N.; Ahmed, D. SEMG-biofeedback armband for hand motor rehabilitation in stroke patients: A preliminary pilot longitudinal study. In Proceedings of the IEEE Medical Measurements and Applications, MeMeA 2020, Virtual, 1 June–1 July 2020. [Google Scholar]
- Luque-Moreno, C.; Kiper, P.; Solis-Marcos, I.; Agostini, M.; Polli, A.; Turolla, A.; Oliva-Pascual-Vaca, A. Virtual Reality and Physiotherapy in Post-Stroke Functional Re-Education of the Lower Extremity: A Controlled Clinical Trial on a New Approach. J. Pers. Med. 2021, 11, 1210. [Google Scholar] [CrossRef]
- Beghi, E.; Gervasoni, E.; Pupillo, E.; Bianchi, E.; Montesano, A.; Aprile, I.; Agostini, M.; Rovaris, M.; Cattaneo, D.; Group, N. Prediction of Falls in Subjects Suffering from Parkinson Disease, Multiple Sclerosis, and Stroke. Arch. Phys. Med. Rehabil. 2018, 99, 641–651. [Google Scholar] [CrossRef] [PubMed]
- IRCCS San Camillo; IRCCS San Raffaele; Istituti Clinici Scientifici Maugeri SpA; IRCCS National Neurological Institute “C. Mondino” Foundation; I.R.C.C.S. Fondazione Santa Lucia. Sensor-Based Assessment and Rehabilitation of Balance in Neurological Diseases; IRCCS San Camillo: Venice, Italy, 2019. [Google Scholar]
- Fusco, A.; Giovannini, S.; Castelli, L.; Coraci, D.; Gatto, D.M.; Reale, G.; Pastorino, R.; Padua, L. Virtual Reality and Lower Limb Rehabilitation: Effects on Motor and Cognitive Outcome-A Crossover Pilot Study. J. Clin. Med. 2022, 11, 2300. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Dasi, F.; Navarro-Garcia, M.M.; Jimenez-Heredia, M.; Magraner, J.; Vina, J.R.; Pallardo, F.V.; Cervantes, A.; Morcillo, E. Evaluation of the quality of publications on randomized clinical trials using the Consolidated Standards of Reporting Trials (CONSORT) statement guidelines in a Spanish tertiary hospital. J. Clin. Pharmacol. 2012, 52, 1106–1114. [Google Scholar] [CrossRef]
- Mancuso, M.; Demeyere, N.; Abbruzzese, L.; Damora, A.; Varalta, V.; Pirrotta, F.; Antonucci, G.; Matano, A.; Caputo, M.; Caruso, M.G.; et al. Using the Oxford Cognitive Screen to Detect Cognitive Impairment in Stroke Patients: A Comparison with the Mini-Mental State Examination. Front. Neurol. 2018, 9, 101. [Google Scholar] [CrossRef] [Green Version]
- Gaskin, C.J.; Happell, B. Power, effects, confidence, and significance: An investigation of statistical practices in nursing research. Int. J. Nurs. Stud. 2014, 51, 795–806. [Google Scholar] [CrossRef]
- Page, S.J.; Fulk, G.D.; Boyne, P. Clinically important differences for the upper-extremity Fugl-Meyer Scale in people with minimal to moderate impairment due to chronic stroke. Phys. Ther. 2012, 92, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Beninato, M.; Gill-Body, K.M.; Salles, S.; Stark, P.C.; Black-Schaffer, R.M.; Stein, J. Determination of the minimal clinically important difference in the FIM instrument in patients with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 32–39. [Google Scholar] [CrossRef]
- Subramanian, S.K.; Banina, M.C.; Turolla, A.; Levin, M.F. Reaching performance scale for stroke—Test-retest reliability, measurement error, concurrent and discriminant validity. PM R. 2022, 14, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.M.; Chen, C.C.; Hsueh, I.P.; Huang, S.L.; Hsieh, C.L. Test-retest reproducibility and smallest real difference of 5 hand function tests in patients with stroke. Neurorehabil. Neural Repair 2009, 23, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Kumle, L.; Vo, M.L.; Draschkow, D. Estimating power in (generalized) linear mixed models: An open introduction and tutorial in R. Behav. Res. Methods 2021, 53, 2528–2543. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- McFadden, D. Quantitative Methods for Analyzing Travel Behaviour of Individuals: Some Recent Developments; Cowles Foundation for Research in Economics, Yale University: New Haven, CT, USA, 1977. [Google Scholar]
- Brier, G.W. Verification of Forecasts Expressed in Terms of Probability. Mon. Weather. Rev. 1950, 78, 1–3. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Hosmer, T.; Le Cessie, S.; Lemeshow, S. A comparison of goodness-of-fit tests for the logistic regression model. Stat. Med. 1997, 16, 965–980. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Tofthagen, C. Threats to validity in retrospective studies. J. Adv. Pract. Oncol. 2012, 3, 181–183. [Google Scholar]


{kind=link}
| Patients (N = 35) | |
|---|---|
| Age, years, mean ± SD | 65.26 ± 16.2 |
| Diagnosis, ischemic/hemorrhagic, n (%) | 25 (71%)/10 (29%) |
| Lesion Side, right/left, n (%) | 24 (69%)/11 (31%) |
| Time from stroke, months, mean ± SD | 26.72 ± 67.1 |
| Aphasia, yes/no, n (%) | 14 (40%)/20 (60%) |
| Apraxia, yes/no, n (%) | 2 (6%)/31 (94%) |
| TOT, mean ± SD | 80.57 ± 30.1 |
| TOT-UL, mean ± SD | 13.4 ± 14.19 |
| TOT-NUL, mean ± SD | 5.34 ± 9.5 |
| CT, mean ± SD | 64.03 ± 23.46 |
| Outcome Measure (N = 35) | T0 | T1 | Within Group p-Value | Effect Size (Cohen’s d) | ||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | |||
| FMA-UE | 31.60 ± 24.4 | 34 (46.5) | 37.20 ± 23.2 | 45 (45) | 0.005 * | 0.45 |
| FMA-sens | 18.29 ± 7.3 | 22 (12) | 19.11 ± 6.1 | 23 (11.5) | 0.501 | 0.15 |
| FIM | 86.17 ± 29.7 | 88 (58) | 97.69 ± 26.8 | 109 (40) | 0.005 * | 0.6 |
| BBT | 16.60 ± 17.7 | 14 (32) | 24.63 ± 20.5 | 29 (43) | < 0.001 * | 0.59 |
| MAS-BicBrach | 0.91 ± 0.9 | 1 (2) | ||||
| Outcome Measure (N = 18) | T0 Mean ± SD |
|---|---|
| Hearts | 44.83 ± 6.5 |
| Recall | 2.78 ± 1.2 |
| Shift | 1.72 ± 4 |
| Outcome Measure (N = 35) | Responders/Non-Responders n (%) |
|---|---|
| FMA-UE | 12 (34%)/23 (66%) |
| FIM | 8 (23%)/27 (77%) |
| BBT | 17 (49%)/18 (51%) |
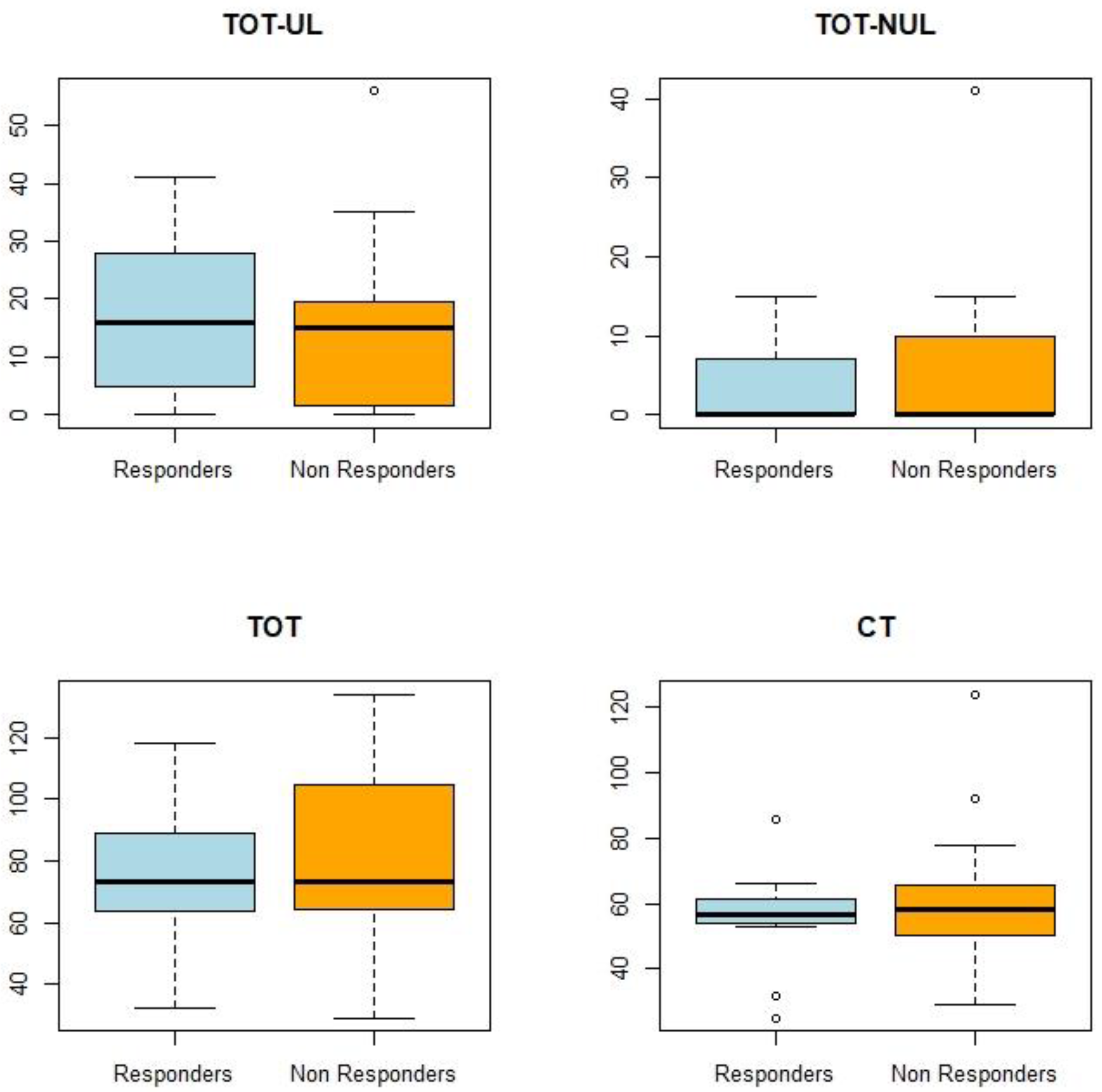
| Dose for Each Outcome Measure | Responders | Non-Responder | Between Groups | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | ||
| FMA-UE | n = 12 | n = 23 | n = 23 | ||
| TOT-UL | 17.17 ± 14.06 | 16 (18.5) | 11.43 ± 14.16 | 15 (17) | p = 0.607 |
| TOT-NUL | 3.67 ± 6.64 | 0 (3.5) | 6.22 ± 10.77 | 0 (10) | p = 0.221 |
| TOT | 76.33 ± 22.71 | 73.5 (21.25) | 82.78 ± 33.55 | 72 (40.5) | p = 0.524 |
| CT | 72.5 ± 33.7 | 56.5 (26) | 56.26 ± 12.17 | 58 (13.5) | p = 0.300 |
| FIM | N = 8 | N = 27 | |||
| TOT-UL | 12.00 ±12.68 | 10.5 (19.25) | 13.82 ± 14.81 | 14 (20) | p = 0.841 |
| TOT-NUL | 1.88 ± 5.30 | 0 (0) | 6.37 ± 10.32 | 0 (12) | p = 0.193 |
| TOT | 61.25 ± 14.96 | 63.5 (13) | 86.29 ± 31.21 | 75 (44) | p = 0.031 * |
| BBT | N = 17 | N = 18 | |||
| TOT-UL | 12.29 ± 15.79 | 6.0 (20) | 14.44 ± 12.88 | 15.5 (19) | p = 0.511 |
| TOT-NUL | 4.94 ± 8.33 | 0 (8) | 5.72 ± 10.77 | 0 (11.25) | p = 0.934 |
| TOT | 82.94 ± 38.34 | 70 (53) | 78.33 ± 20.37 | 74 (23.25) | p = 0.591 |
| Regression Model | β ± SE | Pseudo-R2 | sBS | AUC | PHL |
|---|---|---|---|---|---|
| Intercept FIM TOT | 0.06 ± 1.66 −0.03 ± 0.02 0.02 ± 0.02 | 0.20 | 0.26 | 0.79 | p = 0.33 |
| Intercept Heart * (p = 0.06) | 7.34 ± 4.25 −0.18 ± 0.09 | 0.18 | 0.24 | 0.70 | p = 0.47 |
| Intercept TOT * (p = 0.09) Hearts | 7.06 ± 4.8 0.04 ± 0.02 −0.25 ± 0.12 | 0.36 | 0.42 | 0.87 | p = 0.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvalaggio, S.; Cacciante, L.; Maistrello, L.; Turolla, A. Clinical Predictors for Upper Limb Recovery after Stroke Rehabilitation: Retrospective Cohort Study. Healthcare 2023, 11, 335. https://doi.org/10.3390/healthcare11030335
Salvalaggio S, Cacciante L, Maistrello L, Turolla A. Clinical Predictors for Upper Limb Recovery after Stroke Rehabilitation: Retrospective Cohort Study. Healthcare. 2023; 11(3):335. https://doi.org/10.3390/healthcare11030335
Chicago/Turabian StyleSalvalaggio, Silvia, Luisa Cacciante, Lorenza Maistrello, and Andrea Turolla. 2023. "Clinical Predictors for Upper Limb Recovery after Stroke Rehabilitation: Retrospective Cohort Study" Healthcare 11, no. 3: 335. https://doi.org/10.3390/healthcare11030335
APA StyleSalvalaggio, S., Cacciante, L., Maistrello, L., & Turolla, A. (2023). Clinical Predictors for Upper Limb Recovery after Stroke Rehabilitation: Retrospective Cohort Study. Healthcare, 11(3), 335. https://doi.org/10.3390/healthcare11030335