
Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample and Setting
2.3. Data Collection
2.3.1. Development of an Interview Guide
2.3.2. Focus Group Discussions
2.3.3. Individual Interviews
2.4. Data Analysis
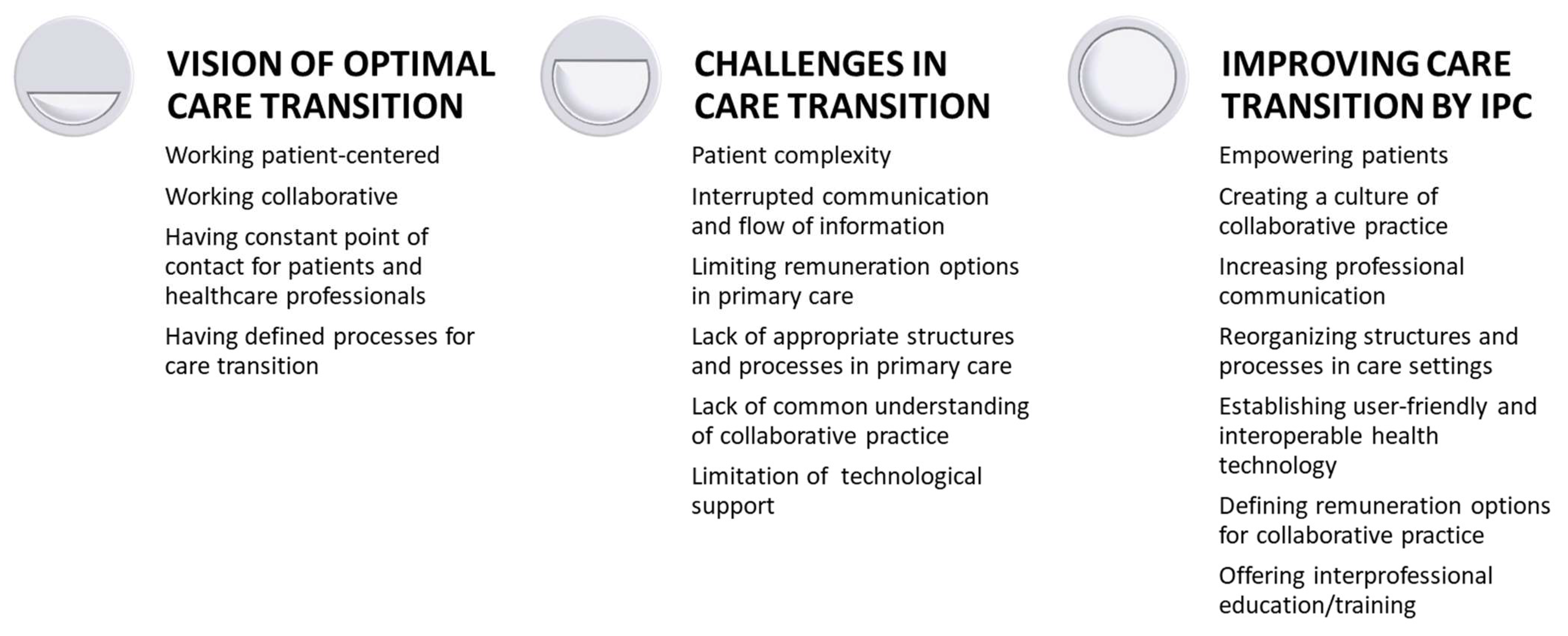
3. Results
3.1. Vision of Optimal Care Transition
‘The most important thing is that you can exchange information in person. That is the most effective and fastest form of communication and the best guarantee that information flows. And that is of course increasingly difficult in more operationalized systems today. I experience this, for example, with referrals to inpatient psychiatry hospitals. When I fill out a referral form, I can do it very meticulously, but it also takes me 1 to 2 h. Or I know whom I can call and that is much easier for someone who is locally well-connected. I know where and whom to call and it’s done in five minutes.’ (01_focus group discussion)
3.2. Challenges in Care Transition
‘The transition to a complex patient and its care provision can be very linear. (…) In palliative care, we know that when it is a palliative situation, it is usually relatively complex. However, there is an illness trajectory long before that, that shows, that it is or becomes complex, even though you don’t think about it, because you are busy with therapies all the time.’ (I04_individual)
‘(…) yes, that is how medical reporting works, due to its relevance for insurance billing. This and that should be included, but if you don’t want to extend the report to 4 pages, you leave out the rest (…) which then influences the quality of the report. The quality is catastrophic, the content is zero!’ (I04_individual).
‘(…) We are still perceived as assistant staff (psychologists), so according to the Swiss health insurance system we cannot reimburse services on the grounds of the basic insurance, the delegates (who receive a referral by medical doctors) can, but the self-employed cannot. (…) With the GPs, we (as self-employed psychologists) have found a common ground to collaborate; with psychiatrists, in contrast, it is partly difficult, due to their problems with the next generation (i.e., low number of psychiatrists and the number is further going down) and therefore they are under pressure.’ (I03_individual).
‘What I still notice professionally and institutionally is that only where someone works or what is relevant for them is just of interest. And it is just not enough patient-tailored or related to what is required (for a collaborative complex patient care transition). And I believe that this feels often like a battle (between healthcare professionals and institutions) and thus remains in these silos.’ (I06_individual)
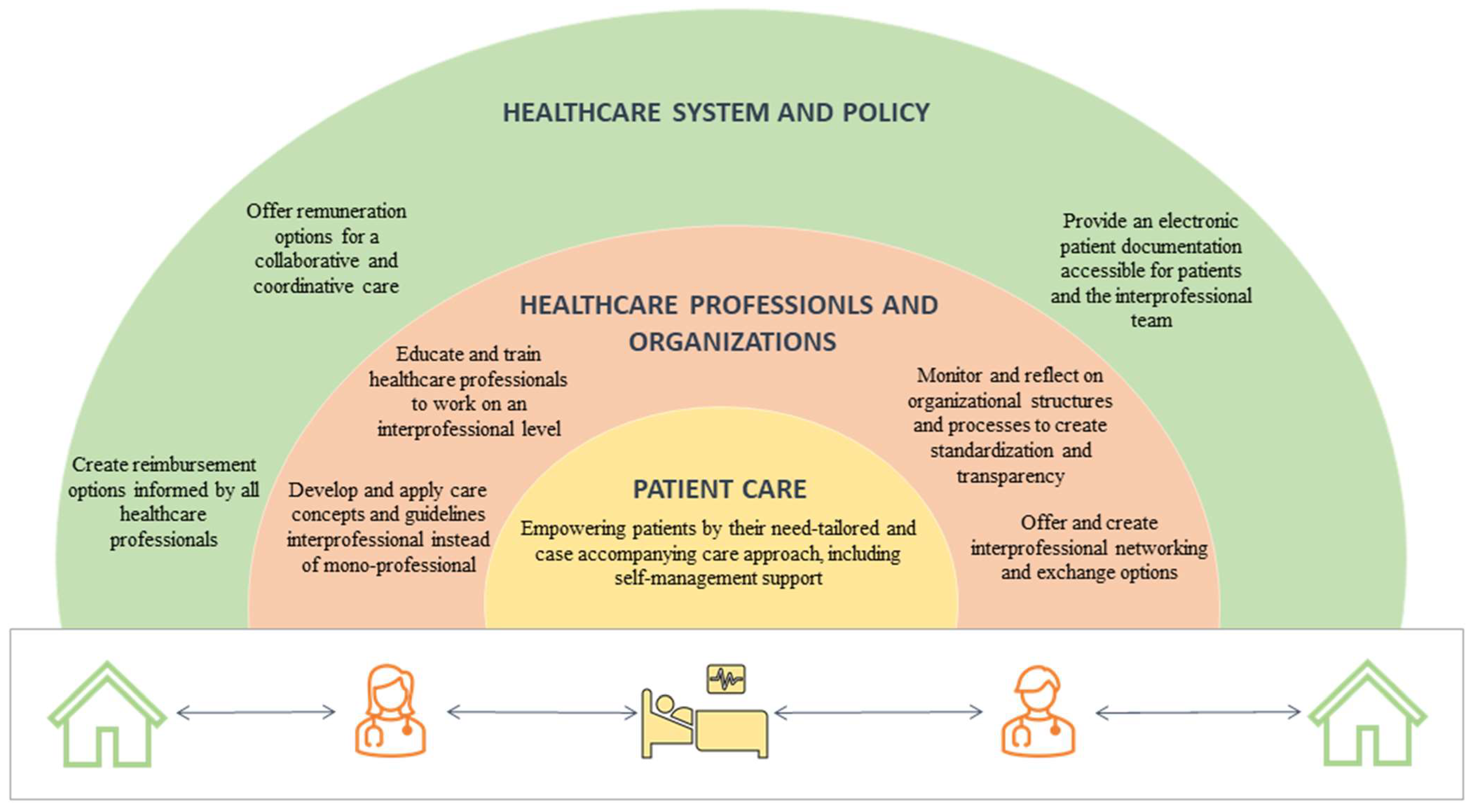
3.3. Improving Care Transition by Interprofessional Collaboration
‘Which information does the other healthcare provider need to continue providing care?’ (01_focus group discussion).
‘It was about caring for an 86-year-old woman. In some instances, she did not understand everything. Then she was embarrassed to ask the doctor again, because she was worried that people would think that she was an old woman and that she was already a bit stupid. (…) I always think that help is needed, which should be installed in the hospitals and so on (…) and stand by the side of those affected, for example through volunteers or peers.’ (01_focus group discussion)
‘This question of costs comes up again and again. And with the pressure to economize… it also helps, if you look at the issue the other way round and ask yourself, what will it cost if we (healthcare professionals) don’t do it? What if we don’t do it because of the cost? The follow-up costs that arise because of problems in the (complex patient) care transition and, if therapies are not provided… that will be much more expensive on average compared to investing in coordination services at the beginning. Nonetheless, after monitoring this alternative approach it can always be decided to change back to the old modus.’ (01_focus group discussion)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schaink, A.K.; Kuluski, K.; Lyons, R.F.; Fortin, M.; Jadad, A.R.; Upshur, R.; Wodchis, W.P. A scoping review and thematic classification of patient complexity: Offering a unifying framework. J. Comorb. 2012, 2, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. The European Health Report 2012—Charting the Way to Well-Being; World Health Organization: Geneva, Switzerland, 2012. Available online: https://apps.who.int/iris/handle/10665/326381 (accessed on 5 December 2022).
- Loeb, D.F.; Binswanger, I.A.; Candrian, C.; Bayliss, E.A. Primary Care Physician Insights Into a Typology of the Complex Patient in Primary Care. Ann. Fam. Med. 2015, 13, 451–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manning, E.; Gagnon, M. The complex patient: A concept clarification. Nurs. Health Sci. 2017, 19, 13–21. [Google Scholar] [CrossRef]
- Safford, M.M.; Allison, J.J.; Kiefe, C.I. Patient Complexity: More Than Comorbidity. The Vector Model of Complexity. J. Gen. Intern. Med. 2007, 22 (Suppl. 3), 382–390. [Google Scholar] [CrossRef] [Green Version]
- Eton, D.T.; Ramalho de Oliveira, D.; Egginton, J.S.; Ridgeway, J.L.; Odell, L.; May, C.R.; Montori, V.M. Building a measurement framework of burden of treatment in complex patients with chronic conditions: A qualitative study. Patient Relat. Outcome Meas. 2012, 3, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Shippee, N.D.; Shah, N.D.; May, C.R.; Mair, F.S.; Montori, V.M. Cumulative complexity: A functional, patient-centered model of patient complexity can improve research and practice. J. Clin. Epidemiol. 2012, 65, 1041–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zullig, L.L.; Whitson, H.E.; Hastings, S.N.; Beadles, C.A.; Kravchenko, J.; Akushevich, I.; Maciejewski, M.L. A Systematic Review of Conceptual Frameworks of Medical Complexity and New Model Development. J. Gen. Intern. Med. 2016, 31, 329–337. [Google Scholar] [CrossRef]
- Nicolaus, S.; Crelier, B.; Donzé, J.D.; Aubert, C.E. Definition of patient complexity in adults: A narrative review. J. Multimorb. Comorbidity 2022, 12, 26335565221081288. [Google Scholar] [CrossRef]
- Nardi, R.; Scanelli, G.; Corrao, S.; Iori, I.; Mathieu, G.; Amatrian, R.C. Co-morbidity does not reflect complexity in internal medicine patients. Eur. J. Intern. Med. 2007, 18, 359–368. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.; Hutchinson, A.M.; Brown, R.; Livingston, P.M. User experience and care for older people transitioning from hospital to home: Patients’ and carers’ perspectives. Health Expect. 2018, 21, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Mora, K.; Dorrejo, X.M.; Carreon, K.M.; Butt, S. Nurse practitioner-led transitional care interventions: An integrative review. J. Am. Assoc. Nurse Pract. 2017, 29, 773–790. [Google Scholar] [CrossRef]
- Monaco, A.; Palmer, K.; Marengoni, A.; Maggi, S.; Hassan, T.A.; Donde, S. Integrated care for the management of ageing-related non-communicable diseases: Current gaps and future directions. Aging Clin. Exp. Res. 2020, 32, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Rijken, M.; Hujala, A.; Van Ginneken, E.; Melchiorre, M.G.; Groenewegen, P.; Schellevis, F. Managing multimorbidity: Profiles of integrated care approaches targeting people with multiple chronic conditions in Europe. Health Policy 2018, 122, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lambert, S.D.; Harrison, J.D.; Smith, E.; Bonevski, B.; Carey, M.; Lawsin, C.; Paul, C.; Girgis, A. The unmet needs of partners and caregivers of adults diagnosed with cancer: A systematic review. BMJ Support. Palliat. Care 2012, 2, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Marengoni, A.; Forjaz, M.J.; Jureviciene, E.; Laatikainen, T.; Mammarella, F.; Muth, C.; Navickas, R.; Prados-Torres, A.; Rijken, M.; et al. Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy 2018, 122, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, B.F.Y.; Lee, J.X.Y.; Tam, W.W.S. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: A systematic review. Hum. Resour. Health 2017, 15, 63. [Google Scholar] [CrossRef]
- Barry, S.; Fhallúin, M.N.; Thomas, S.; Harnett, P.J.; Burke, S. Implementing Integrated Care in Practice—Learning from MDTs Driving the Integrated Care Programme for Older Persons in Ireland. Int. J. Integr. Care 2021, 21, 15. [Google Scholar] [CrossRef]
- Filliettaz, S.S.; Berchtold, P.; Kohler, D.; Peytremann-Bridevaux, I. Integrated care in Switzerland: Results from the first nationwide survey. Health Policy 2018, 122, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Mabire, C.; Büla, C.; Morin, D.; Goulet, C. Nursing discharge planning for older medical inpatients in Switzerland: A cross-sectional study. Geriatr. Nurs. 2015, 36, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 2017, CD000072. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice; World Health Organization: Geneva, Switzerland, 2010. Available online: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice (accessed on 5 December 2022).
- House, S.; Wilmoth, M.; Kitzmiller, R. Relational coordination and staff outcomes among healthcare professionals: A scoping review. J. Interprof. Care 2021, 36, 891–899. [Google Scholar] [CrossRef]
- Tsakitzidis, G.; Timmermans, O.; Callewaert, N.; Verhoeven, V.; Lopez-Hartmann, M.; Truijen, S.; Meulemans, H.; Van Royen, P. Outcome Indicators on Interprofessional Collaboration Interventions for Elderly. Int. J. Integr. Care 2016, 16, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xyrichis, A.; Reeves, S.; Zwarenstein, M. Examining the nature of interprofessional practice: An initial framework validation and creation of the InterProfessional Activity Classification Tool (InterPACT). J. Interprof. Care 2018, 32, 416–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitz, C.; Atzeni, G.; Berchtold, P. Challenges in interprofessionalism in Swiss health care: The practice of successful interprofessional collaboration as experienced by professionals. Swiss Med. Wkly. 2017, 147, w14525. [Google Scholar] [CrossRef] [Green Version]
- Wei, H.; Horns, P.; Sears, S.F.; Huang, K.; Smith, C.M.; Wei, T.L. A systematic meta-review of systematic reviews about interprofessional collaboration: Facilitators, barriers, and outcomes. J. Interprof. Care 2022, 36, 735–749. [Google Scholar] [CrossRef] [PubMed]
- Flick, U. Triangulation. In Handbuch Qualitative Forschung in der Psychologie; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2011. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The Use of Triangulation in Qualitative Research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Bundesamt für Gesundheit. Patientengruppen und Schnittstellen (Koordinierte Versorgung)—Patient Groups and Interfaces (Coordinated Care); Swiss Federal Office of Public Health: Liebefeld, Switzerland, 2018.
- De Wit, M.; Cooper, C.; Tugwell, P.; Bere, N.; Kirwan, J.; Conaghan, P.G.; Roberts, C.; Aujoulat, I.; Al-Daghri, N.; de Carvalho, I.A.; et al. Practical guidance for engaging patients in health research, treatment guidelines and regulatory processes: Results of an expert group meeting organized by the World Health Organization (WHO) and the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Aging Clin. Exp. Res. 2019, 31, 905–915. [Google Scholar] [CrossRef] [Green Version]
- Kallio, H.; Pietilä, A.-M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016, 72, 2954–2965. [Google Scholar] [CrossRef]
- Chan, A.K.; Pharm, B.; Wood, V. Preparing tomorrow’s healthcare providers for interprofessional collaborative patient-centred practice today. UBC Med. J. 2010, 1, 22–24. [Google Scholar]
- Körner, M.; Bütof, S.; Müller, C.; Zimmermann, L.; Becker, S.; Bengel, J. Interprofessional teamwork and team interventions in chronic care: A systematic review. J. Interprof. Care 2016, 30, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Tuzzio, L.; Berry, A.L.; Gleason, K.; Barrow, J.; Bayliss, E.A.; Gray, M.F.; Delate, T.; Bermet, Z.; Uratsu, C.S.; Grant, R.W.; et al. Aligning care with the personal values of patients with complex care needs. Health Serv. Res. 2021, 56, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Supper, I.; Catala, O.; Lustman, M.; Chemla, C.; Bourgueil, Y.; Letrilliart, L. Interprofessional collaboration in primary health care: A review of facilitators and barriers perceived by involved actors. J. Public Health 2014, 37, 716–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Flick, U.; von Kardorff, E.; Steinke, I. Qualitative Forschung. Ein Handbuch; Rowolth Taschenbuch Verlag: Reinebek bei Hamburg, Germany, 2009. [Google Scholar]
- Vindrola-Padros, C.; Johnson, G.A. Rapid Techniques in Qualitative Research: A Critical Review of the Literature. Qual. Health Res. 2020, 30, 1596–1604. [Google Scholar] [CrossRef]
- World Health Organization. Imbalances in Rural Primary Care: A Scoping Literature Review with an Emphasis on the WHO European Region; World Health Organization: Geneva, Switzerland, 2018. Available online: https://apps.who.int/iris/handle/10665/346351 (accessed on 5 December 2022).
- Chevillard, G.; Mousquès, J. Medically underserved areas: Are primary care teams efficient at attracting and retaining general practitioners? Soc. Sci. Med. 2021, 287, 114358. [Google Scholar] [CrossRef]
- Geese, F.; Molls, S.; Schucht, P.; Raabe, A.; Schmitt, K.-U. Evaluation of an APN service in acute inpatient care of patients with a malignant brain tumor: A qualitative study in a Swiss university hospital/Evaluation eines APN-Angebots in der akut-stationären Versorgung von Patienten und Patientinnen mit malignem Hirntumor: Eine qualitative Studie in einem Schweizer Universitätsspital. Int. J. Health Prof. 2022, 9, 1–12. [Google Scholar] [CrossRef]
- Karimi-Shahanjarini, A.; Shakibazadeh, E.; Rashidian, A.; Hajimiri, K.; Glenton, C.; Noyes, J.; Lewin, S.; Laurant, M.; Colvin, C.J. Barriers and facilitators to the implementation of doctor-nurse substitution strategies in primary care: A qualitative evidence synthesis. Cochrane Database Syst. Rev. 2019, 2019, CD010412. [Google Scholar] [CrossRef] [Green Version]
- Martin-Misener, R.; Harbman, P.; Donald, F.; Reid, K.; Kilpatrick, K.; Carter, N.; Bryant-Lukosius, D.; Kaasalainen, S.; Marshall, D.A.; Charbonneau-Smith, R.; et al. Cost-effectiveness of nurse practitioners in primary and specialised ambulatory care: Systematic review. BMJ Open 2015, 5, e007167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gysin, S.; Sottas, B.; Odermatt, M.; Essig, S. Advanced practice nurses’ and general practitioners’ first experiences with introducing the advanced practice nurse role to Swiss primary care: A qualitative study. BMC Fam. Pract. 2019, 20, 163. [Google Scholar] [CrossRef] [PubMed]
- Torrens, C.; Campbell, P.; Hoskins, G.; Strachan, H.; Wells, M.; Cunningham, M.; Bottone, H.; Polson, R.; Maxwell, M. Barriers and facilitators to the implementation of the advanced nurse practitioner role in primary care settings: A scoping review. Int. J. Nurs. Stud. 2020, 104, 103443. [Google Scholar] [CrossRef] [PubMed]
- Girard, M.-A. Interprofessional education and collaborative practice policies and law: An international review and reflective questions. Hum. Resour. Health 2021, 19, 9. [Google Scholar] [CrossRef]
- Boes, S.; Brach, M.; Kaufmann, C.; Mantwill, S.; Rubinelli, S.; Stucki, G. Swiss Learning Health System. Bull. Méd. Suisses 2017, 98, 1264–1268. [Google Scholar] [CrossRef]
- Schweizerische Akademien der Medizinischen Wissenschaften. Kommunikation im Medizinischen Alltag. Ein Leitfaden für die Praxis; Schweizerische Akademie der Medizinischen Wissenschaften: Basel, Switzerland, 2019; Available online: https://www.samw.ch/de/Publikationen/Leitfaden-fuer-die-Praxis.html (accessed on 5 December 2022).
- Dreier-Wolfgramm, A.; Homeyer, S.; Oppermann, R.F.; Hoffmann, W. A model of interprofessional problem-based learning for medical and nursing students: Implementation, evaluation and implications for future implementation. GMS J. Med. Educ. 2018, 35, Doc13. [Google Scholar] [CrossRef] [PubMed]
- Marion-Martins, A.D.; Pinho, D.L.M. Interprofessional simulation effects for healthcare students: A systematic review and meta-analysis. Nurse Educ. Today 2020, 94, 104568. [Google Scholar] [CrossRef]
- Kent, F.; Nankervis, K.; Johnson, C.; Hodgkinson, M.; Baulch, J.; Haines, T. ‘More effort and more time’. Considerations in the establishment of interprofessional education programs in the workplace. J. Interprof. Care 2018, 32, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.; Nguyen, H.; Groth, M.; Wang, K.; Ng, J.L. Time to change: A review of organisational culture change in health care organisations. J. Organ. Eff. People Perform. 2016, 3, 265–288. [Google Scholar] [CrossRef]
- Schadewaldt, V.; McInnes, E.; Hiller, J.E.; Gardner, A. Experiences of nurse practitioners and medical practitioners working in collaborative practice models in primary healthcare in Australia—A multiple case study using mixed methods. BMC Fam. Pract. 2016, 17, 99. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual. Res. Sport Exerc. Health 2020, 13, 201–216. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Focus Group Discussion (1) | Focus Group Discussion (2) | Individual Interviews | |
|---|---|---|---|
| Number of participants | n = 8 | n = 13 | n = 10 |
| Professional background |
|
|
|
| Represented care setting |
|
| |
| Organization/Association |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geese, F.; Schmitt, K.-U. Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis. Healthcare 2023, 11, 359. https://doi.org/10.3390/healthcare11030359
Geese F, Schmitt K-U. Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis. Healthcare. 2023; 11(3):359. https://doi.org/10.3390/healthcare11030359
Chicago/Turabian StyleGeese, Franziska, and Kai-Uwe Schmitt. 2023. "Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis" Healthcare 11, no. 3: 359. https://doi.org/10.3390/healthcare11030359
APA StyleGeese, F., & Schmitt, K. -U. (2023). Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis. Healthcare, 11(3), 359. https://doi.org/10.3390/healthcare11030359