
Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Experimental Environment
2.5. Determining the Target Vein
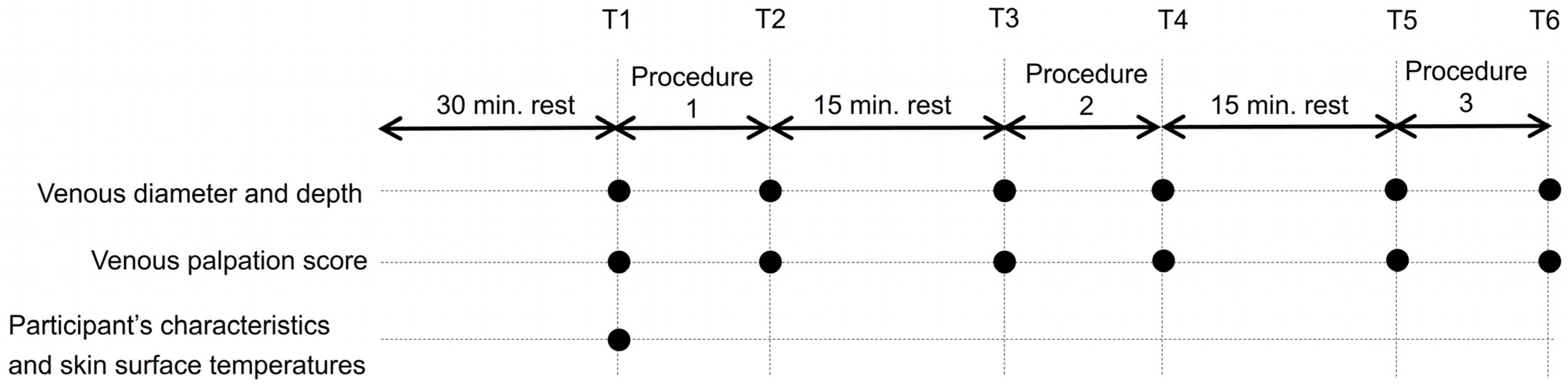
2.6. Experimental Procedure
2.6.1. Tourniquet Application
2.6.2. Tapping the Vein
2.6.3. Massaging the Forearm
2.7. Data Collection
2.7.1. Participants’ Characteristics
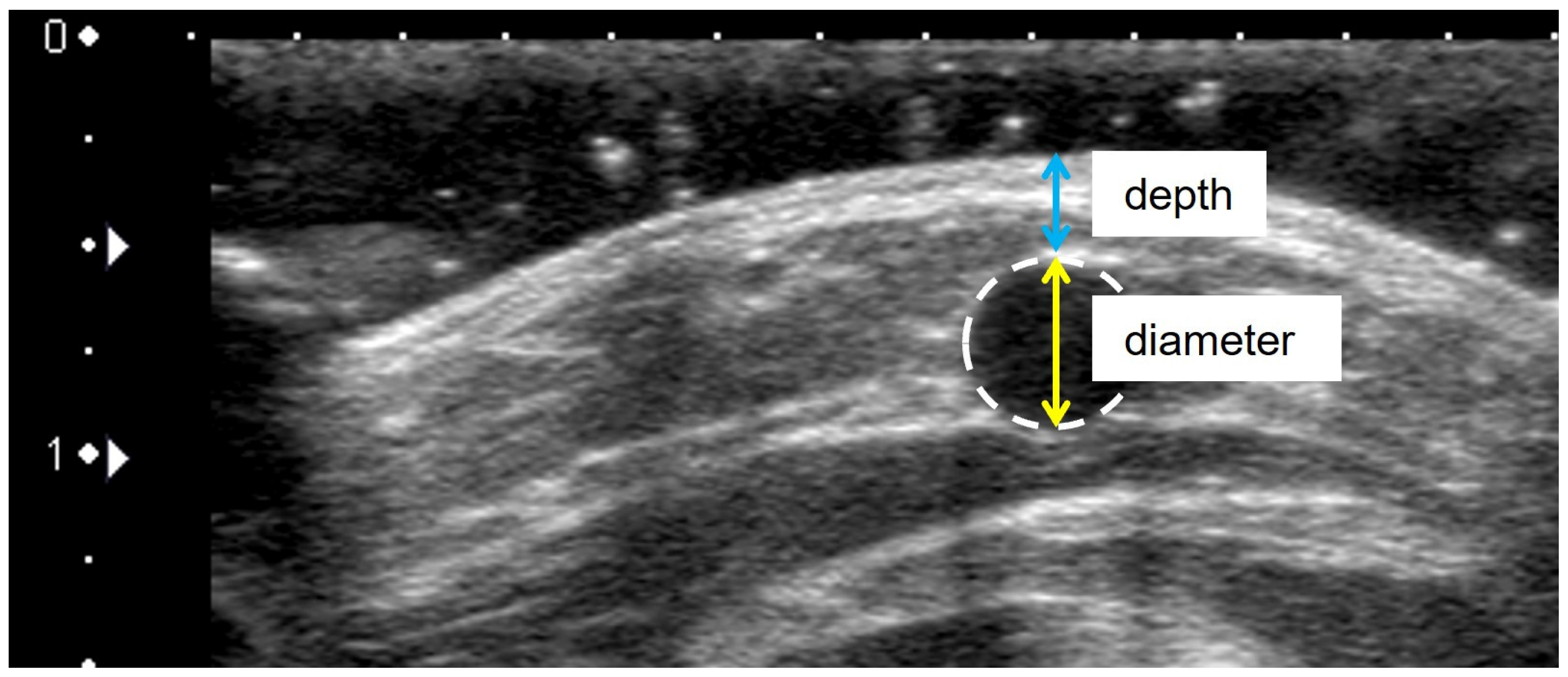
2.7.2. Venous Diameter and Depth
2.7.3. Skin Surface Temperature
2.7.4. Venous Palpation Score
2.8. Data Analysis
2.9. Ethical Considerations
3. Results
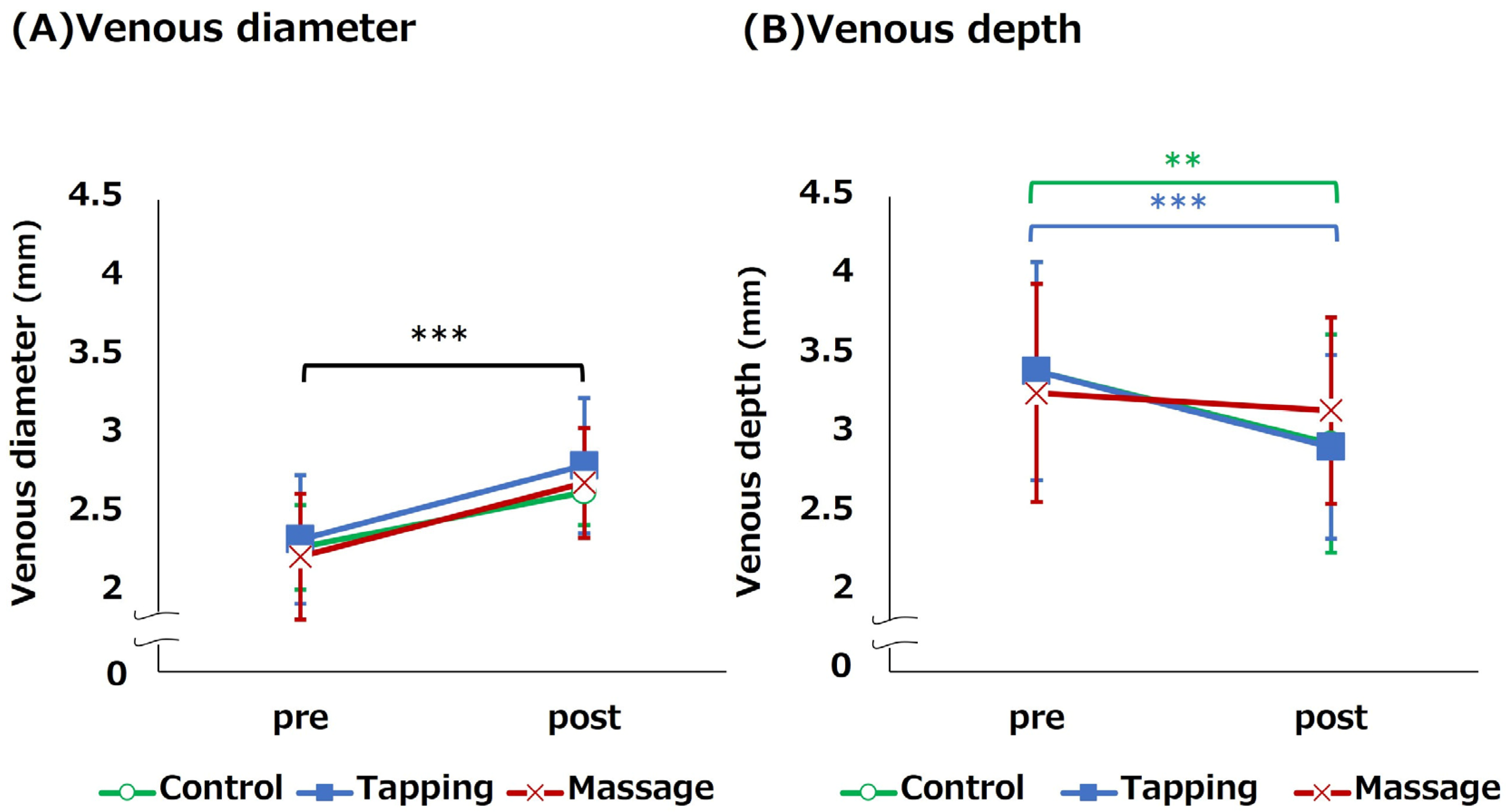
3.1. Change in Venous Diameter and Depth for Each Venous Dilation Procedure
3.2. Venous Palpitation Score and Associated Change
3.3. Subgroup Analysis: Venous Dilation Effect of Each Procedure in the Thin Vein Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alexandrou, E.; Ray-Barruel, G.; Carr, P.J.; Frost, S.A.; Inwood, S.; Higgins, N.; Lin, F.; Alberto, L.; Mermel, L.; Rickard, C.M.; et al. Use of short peripheral intravenous catheters: Characteristics, management, and outcomes worldwide. J. Hosp. Med. 2018, 13, E1–E7. [Google Scholar] [CrossRef]
- Hadaway, L.C.; Millam, D.A. On the road to successful I.V. starts. Nursing 2005, 35, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ingram, P.; Lavery, I. Peripheral intravenous cannulation: Safe insertion and removal technique. Nurs. Stand. 2007, 22, 44–47. [Google Scholar] [CrossRef]
- Gagne, P.; Sharma, K. Relationship of Common Vascular Anatomy to Cannulated Catheters. Int. J. Vasc. Med. 2017, 2017, 5157914. [Google Scholar] [CrossRef] [PubMed]
- Lapostolle, F.; Catineau, J.; Garrigue, B.; Monmarteau, V.; Houssaye, T.; Vecci, I.; Tréoux, V.; Hospital, B.; Crocheton, N.; Adnet, F. Prospective evaluation of peripheral venous access difficulty in emergency care. Intensive Care Med. 2007, 33, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Sabri, A.; Sazalas, J.; Holmes, K.S.; Labib, L.; Mussivand, T. Failed attempts and improvement strategies in peripheral intravenous catheterization. Biomed. Mater. Eng. 2013, 23, 93–108. [Google Scholar] [CrossRef]
- Carr, P.J.; Rippey, J.C.R.; Cooke, M.L.; Trevenen, M.L.; Higgins, N.S.; Foale, A.S.; Rickard, C.M. Factors associated with peripheral intravenous cannulation first-time insertion success in the emergency department. A multicentre prospective cohort analysis of patient, clinician and product characteristics. BMJ Open 2019, 9, e022278. [Google Scholar] [CrossRef]
- Marsh, N.; Larsen, E.N.; Takashima, M.; Kleidon, T.; Keogh, S.; Ullman, A.J.; Mihala, G.; Chopra, V.; Rickard, C.M. Peripheral intravenous catheter failure: A secondary analysis of risks from 11,830 catheters. Int. J. Nurs. Stud. 2021, 124, 104095. [Google Scholar] [CrossRef]
- Infusion Nursing Society. Infusion nursing standards of practice. J. Infus. Nurs. 2016, 34, S65–S74. [Google Scholar]
- Dougherty, L. Peripheral cannulation. Nurs. Stand. 2018, 22, 49–56. [Google Scholar] [CrossRef]
- Masamoto, T.; Yano, R. Characteristics of expert nurses’ assessment of insertion sites for peripheral venous catheters in elderly adults with hard-to-find veins. Jpn. J. Nurs. Sci. 2020, 18, e12379. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Mark, L.K.F.; Fatimah, L. Management of difficult intravenous access: A qualitative review. World J. Emerg. Med. 2022, 13, 467–478. [Google Scholar] [CrossRef]
- van Loon, F.H.J.; van Hooff, L.W.E.; de Boer, H.D.; Koopman, S.S.H.A.; Buise, M.P.; Korsten, H.H.M.; Dierick-van Daele, A.T.M.; Bouwman, A.R.A. The Modified A-DIVA Scale as a predictive tool for prospective identification of adult patients at risk of a difficult intravenous access: A multicenter validation study. J. Clin. Med. 2019, 8, 144. [Google Scholar] [CrossRef]
- Panebianco, N.L.; Fredette, J.M.; Szyld, D.; Sagalyn, E.B.; Pines, J.M.; Dean, A.J. What you see (sonographically) is what you get: Vein and patient characteristics associated with successful ultrasound-guided peripheral intravenous placement in patients with difficult access. Acad. Emerg. Med. 2009, 16, 1298–1303. [Google Scholar] [CrossRef]
- Potter, P.; Perry, A.; Stockert, P.; Hall, A. Fundamentals of Nursing: Concepts, Process, and Practice, 9th ed.; Elsevier Mosby: St. Louis, MI, USA, 2017. [Google Scholar]
- Santos-Costa, P.; Paiva-Santos, F.; Sousa, L.B.; Bernardes, R.A.; Ventura, F.; Fearnley, W.D.; Salgueiro-Oliveira, A.; Parreira, P.; Vieira, M.; Graveto, J. Nurses’ Practices in the Peripheral Intravenous Catheterization of Adult Oncology Patients: A Mix-Method Study. J. Pers. Med. 2022, 12, 151. [Google Scholar] [CrossRef] [PubMed]
- Lenhardt, R.; Seybold, T.; Kimberger, O.; Stoiser, B.; Sessler, D.I. Local warming and insertion of peripheral venous cannulas: Single blinded prospective randomised controlled trial and single blinded randomised crossover trial. BMJ 2002, 325, 409–410. [Google Scholar] [CrossRef] [PubMed]
- Bayram, B.S.; Caliskan, N. Effects of local heat application before intravenous catheter insertion in chemotherapy patients. J. Clin. Nurs. 2016, 25, 1740–1747. [Google Scholar] [CrossRef] [PubMed]
- Roberge, R.J. Venodilatation techniques to enhance venepuncture and intravenous cannulation. J. Emerg. Med. 2004, 27, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Masamoto, T.; Yano, R. Characteristics of Observations and Procedures Followed by Expert Nurses for the Selection of the Intravenous Insertion Site for a Short Peripheral Catheter. Jpn. J. Nurs. Art Sci. 2018, 17, 104–113. (In Japanese) [Google Scholar] [CrossRef]
- Lu, D.; Kassab, G.S. Role of shear stress and stretch in vascular mechanobiology. J. R. Soc. Interface 2011, 8, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.H.; Hsiao, S.S. Fundamentals of sensory systems. In Fundamental Neuroscience, 4th ed.; Squire, L., Berg, D., Bloom, F.E., Du Lac, S., Ghosh, A., Spitzer, N.C., Eds.; Academic Press: New York, NY, USA, 2013; pp. 499–511. [Google Scholar]
- Ichimura, M.; Sasaki, S.; Mori, M.; Ogino, T. Tapping but not massage enhances vasodilation and improves venous palpation of cutaneous veins. Acta Med. Okayama 2015, 69, 79–85. [Google Scholar] [CrossRef]
- Yasuda, K.; Sato, S.; Okada, K.; Yano, R. The venous dilation effects of tapping versus massaging for venipuncture. Jpn. J. Nurs. Sci. 2019, 16, 491–499. [Google Scholar] [CrossRef]
- Yamagami, Y.; Tomita, K.; Tsujimoto, T.; Inoue, T. Tourniquet application after local forearm warming to improve venous dilation for peripheral intravenous cannulation in young and middle-aged adults: A single-blind prospective randomized controlled trial. Int. J. Nurs. Stud. 2017, 72, 1–7. [Google Scholar] [CrossRef]
- Chen, M.; Li, X. Role of TRPV4 channel in vasodilation and neovascularization. Microcirculation 2021, 10, e12703. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Ichimura, M.; Murakami, N.; Matsumura, Y.; Mori, M.; Ogino, T. Effects of hot compress on superficial vein of forearm for venipuncture. Jpn. J. Nurs. Art Sci. 2014, 12, 14–23. (In Japanese) [Google Scholar] [CrossRef]
- Young, C.N.; Stillabower, M.E.; DiSabatino, A.; Farquhar, W.B. Venous smooth muscle tone and responsiveness in older adults. J. Appl. Physiol. 1985, 101, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Yamagami, Y.; Inoue, T. Patient position affects venous dilation for peripheral intravenous cannulation. Biol. Res. Nurs. 2019, 22, 226–233. [Google Scholar] [CrossRef]
- Kimori, K.; Sugama, J. Investigation of vasculature characteristics to improve venepuncture techniques in hospitalized elderly patients. Int. J. Nurs. Prac. 2016, 22, 300–306. [Google Scholar] [CrossRef]
- Ortega, R.; Sekhar, P.; Song, M.; Hansen, C.J.; Peterson, L. Videos in clinical medicine. Peripheral intravenous cannulation. N. Engl. J. Med. 2008, 359, e26. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Sasaki, S.; Murakami, N.; Matsumura, Y.; Ichimura, M.; Mori, M. Relationship between tourniquet pressure and a cross-section area of superficial vein of forearm. Acta Med. Okayama 2012, 66, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, M.; Sasaki, S.; Ogino, T. Tapping enhances vasodilation for venipuncture even in individuals with veins that are relatively difficult to palpate. Clin. Anat. 2020, 33, 440–445. [Google Scholar] [CrossRef]
- Sharp, R.; Childs, J.; Bulmer, A.C.; Esterman, A. The effect of oral hydration and localised heat on peripheral vein diameter and depth: A randomised controlled trial. Appl. Nurs. Res. 2018, 42, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Kato, A.; Mori, M. The effect of tension of venipuncture tourniquet on overswelling of the vein, and physical factors that influence overswelling. Jpn. J. Nurs. Art Sci. 2009, 8, 42–47. (In Japanese) [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Davey, M.; Eglin, C.; House, J.; Tipton, M. The contribution of blood flow to the skin temperature responses during a cold sensitivity test. Eur. J. Appl. Physiol. 2013, 113, 2411–2417. [Google Scholar] [CrossRef]
- Ungvari, Z.; Tarantini, S.; Donato, A.J.; Galvan, V.; Csiszar, A. Mechanisms of Vascular Aging. Circ. Res. 2018, 123, 849–867. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) | Mean (SD) |
|---|---|---|
| Sex | ||
| Men | 15 (50.0) | - |
| Women | 15 (50.0) | - |
| Dominant forearm | ||
| Right | 26 (86.7) | - |
| Left | 4 (13.3) | - |
| Target vein | ||
| Cephalic | 12 (40.0) | - |
| Median | 17 (56.7) | - |
| Basilic | 1 (3.3) | - |
| Age (years) | - | 22.47 (1.25) |
| BMI (kg/m2) | - | 21.44 (2.29) |
| Body fat percentage (%) | - | 21.16 (7.84) |
| Body temperature (°C) | - | 36.40 (0.29) |
| Pulse (beats/min) | - | 60.73 (9.13) |
| Systolic BP (mmHg) | - | 108.87 (11.14) |
| Diastolic BP (mmHg) | - | 58.60 (9.13) |
| Skin surface temperature on forearm (°C) | - | 33.07 (1.04) |
| Skin surface temperature on palm (°C) | - | 33.55 (1.81) |
| Venous diameter | - | |
| Cephalic venous diameter at T1 (mm, n = 12) | 2.53 (0.59) | |
| Median and basilic venous diameter at T1 (mm, n = 18) | 2.67 (0.31) | |
| Venous depth | - | |
| Cephalic venous diameter at T1 (mm, n = 12) | 3.91 (1.77) | |
| Median and basilic venous diameter at T1 (mm, n = 18) | 3.04 (1.19) |
| Pre | Post | p | Change Ratio | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Venous diameter (mm) | ||||
| Control condition | 2.60 (0.43) | 3.32 (0.60) | <0.001 a | 128.45 (16.78) |
| Tapping condition | 2.63 (0.52) | 3.25 (0.50) | <0.001 a | 126.41 (22.48) |
| Massage condition | 2.61 (0.64) | 3.13 (0.61) | <0.001 a | 124.36 (31.23) |
| p | 0.980 b | 0.432 b | ||
| Partial η2 | <0.001 | 0.019 | ||
| Venous depth (mm) | ||||
| Control condition | 3.41 (1.46) | 3.03 (1.27) | <0.001 a | 89.96 (10.37) |
| Tapping condition | 3.41 (1.48) | 3.00 (1.27) | <0.001 a | 90.38 (15.31) |
| Massage condition | 3.29 (1.39) | 3.23 (1.34) | 0.528 a | 99.95 (15.48) |
| p | 0.926 b | 0.743 b | ||
| Partial η2 | <0.001 | <0.001 | ||
| Venous Palpation Score | Pre | Post | χ2/p df | |
|---|---|---|---|---|
| n (%) | ||||
| Control condition | 0: impalpable | 14 (46.67) | 0 (0.00) | 35.40/<0.001 a df-2 |
| 1: slightly palpable | 16 (53.33) | 10 (33.33) | ||
| 2: sufficiently palpable | 0 (0.00) | 20 (66.67) | ||
| Taping condition | 0: impalpable | 15 (50.00) | 1 (3.33) | 30.44/<0.001 a df-2 |
| 1: slightly palpable | 15 (50.00) | 11 (36.67) | ||
| 2: sufficiently palpable | 0 (0.00) | 18 (60.00) | ||
| Massage condition | 0: impalpable | 17 (56.67) | 2 (6.67) | 32.39/<0.001 a df-2 |
| 1: slightly palpable | 13 (43.33) | 9 (30.00) | ||
| 2: sufficiently palpable | 0 (0.00) | 19 (63.33) | ||
| χ2/p | 0.623/0.733 a | 2.305/0.680 a | ||
| df | df-2 | df-4 | ||
| Characteristic | Thin Vein Group (n = 9) | Thick Vein Group (n = 21) | p | φ |
|---|---|---|---|---|
| n (%) | ||||
| Sex | ||||
| Men | 3 (33.33) | 12 (57.14) | 0.427 a | 0.220 |
| Women | 6 (66.67) | 9 (42.86) | ||
| Venous palpation score post Control condition | ||||
| 0: impalpable | 0 (0.0) | 0 (0.0) | 0.431 a | 0.154 |
| 1: slightly palpable | 4 (44.44) | 6 (28.57) | ||
| 2: sufficiently palpable | 5 (55.56) | 15 (71.43) | ||
| Mean (SD) | p | d | ||
| BMI (kg/m2) | 20.88 (1.39) | 21.69 (2.57) | 0.382 b | 0.354 |
| Body fat percentage (%) | 21.73 (6.56) | 20.92 (8.47) | 0.800 b | 0.102 |
| Body temperature (°C) | 36.36 (0.22) | 36.41 (0.33) | 0.629 b | 0.195 |
| Pulse (beats/min) | 61.89 (8.75) | 60.24 (9.45) | 0.671 b | 0.178 |
| Systolic BP (mmHg) | 103.78 (8.74) | 111.05 (11.62) | 0.102 b | 0.673 |
| Diastolic BP (mmHg) | 61.89 (7.46) | 57.19 (10.41) | 0.232 b | 0.486 |
| Skin surface temperature on the forearm (°C) | 32.61 (1.13) | 33.28 (0.95) | 0.110 b | 0.658 |
| Skin surface temperature on the palm (°C) | 32.59 (2.36) | 33.96 (1.40) | 0.056 b | 0.796 |
| Venous diameter at post Control condition (mm) | 2.64 (0.28) | 3.61 (0.44) | <0.001 b | 1.805 |
| Venous depth at post Control condition (mm) | 3.23 (1.26) | 2.94 (1.29) | 0.574 b | 0.226 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasuda, K.; Okada, K.; Sugimura, N.; Yano, R. Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study. Healthcare 2023, 11, 522. https://doi.org/10.3390/healthcare11040522
Yasuda K, Okada K, Sugimura N, Yano R. Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study. Healthcare. 2023; 11(4):522. https://doi.org/10.3390/healthcare11040522
Chicago/Turabian StyleYasuda, Kae, Kazunori Okada, Naotaka Sugimura, and Rika Yano. 2023. "Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study" Healthcare 11, no. 4: 522. https://doi.org/10.3390/healthcare11040522
APA StyleYasuda, K., Okada, K., Sugimura, N., & Yano, R. (2023). Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study. Healthcare, 11(4), 522. https://doi.org/10.3390/healthcare11040522