

Torture and Maltreatment in Prison: A Medico-Legal Perspective
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Physical Abuse
3.1.1. Blunt Force Trauma
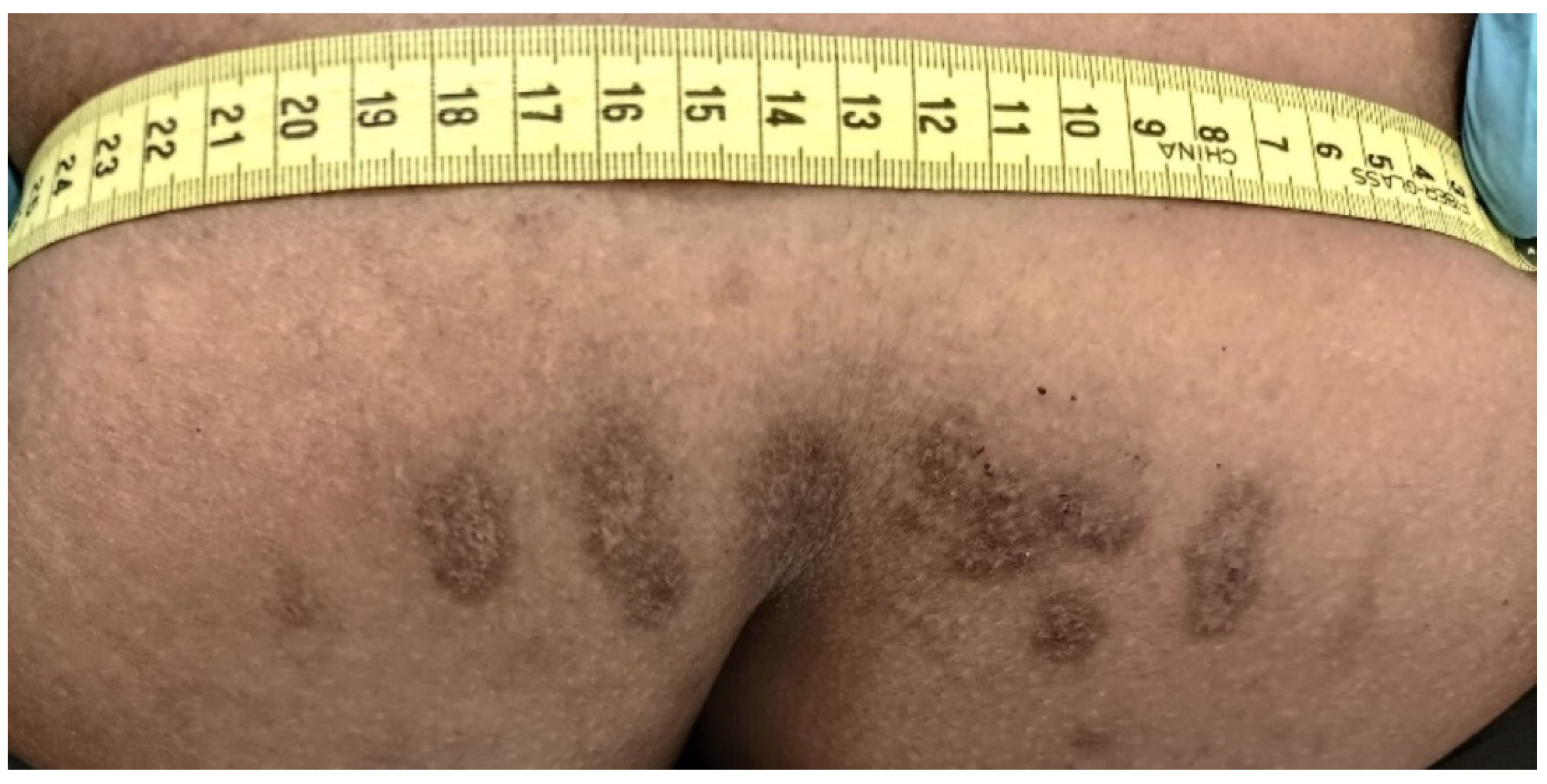
3.1.2. Electric Injuries
3.1.3. Asphyxiation
3.1.4. Forced Positions and Suspension
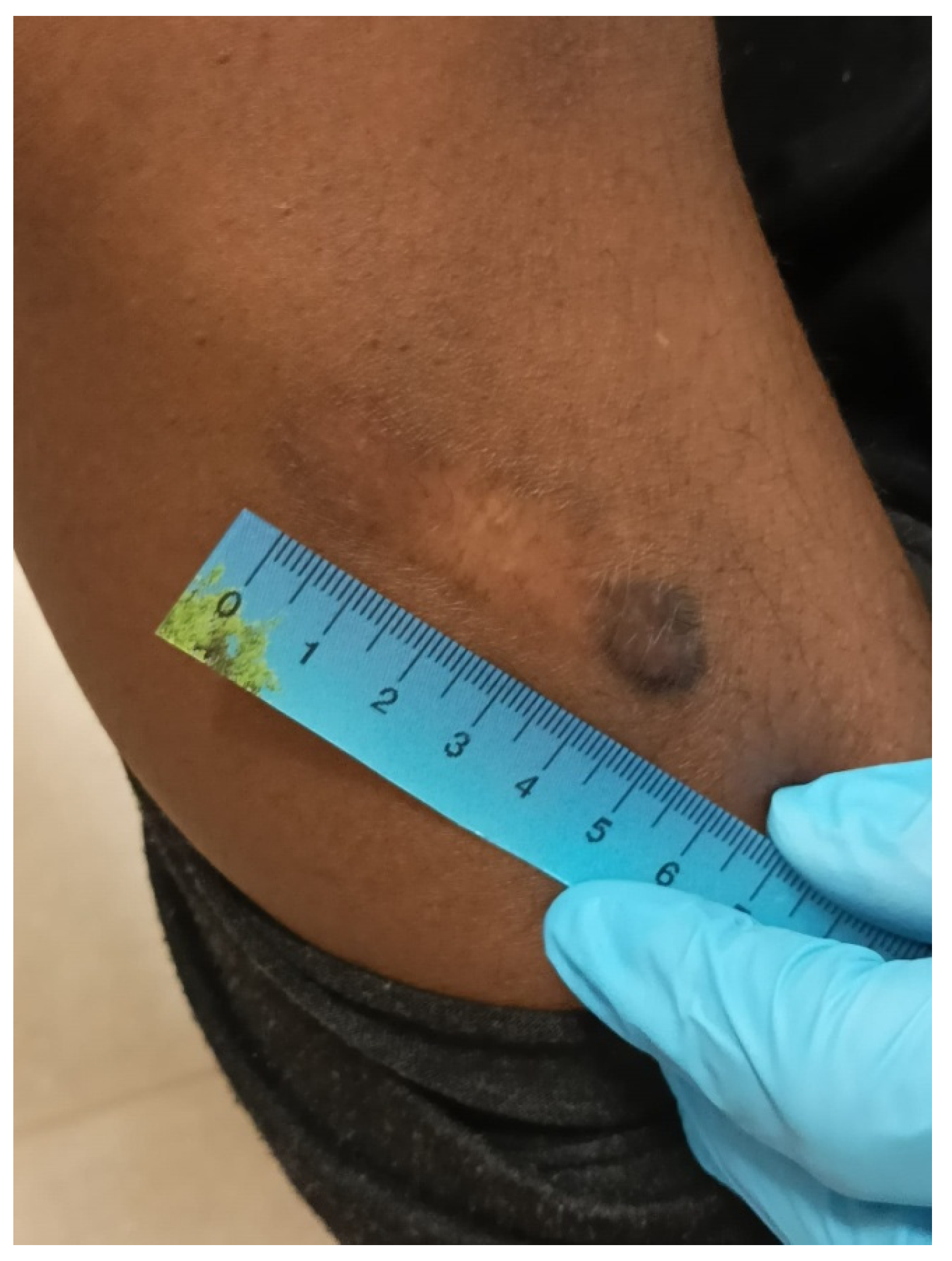
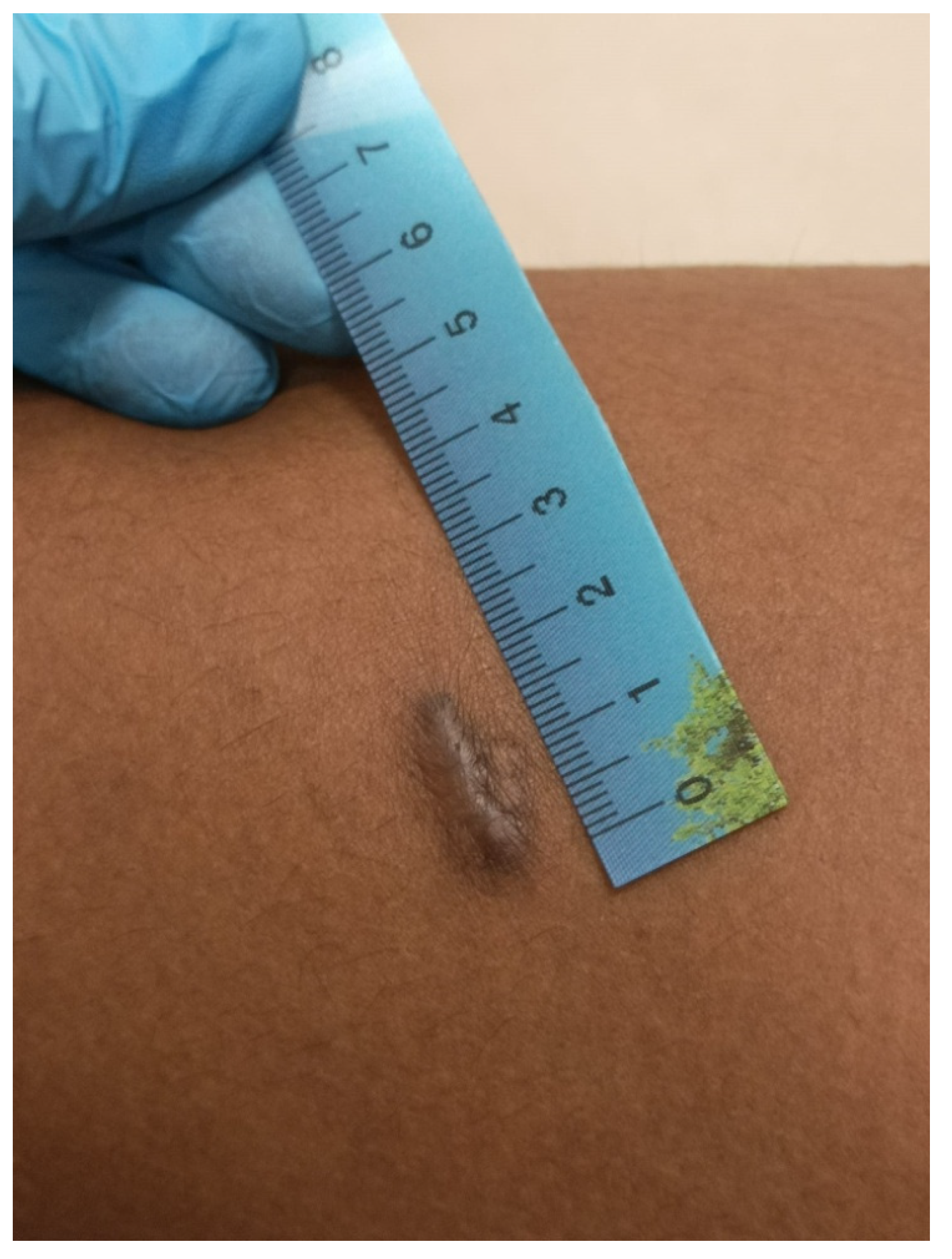
3.1.5. Thermal Injuries
3.2. Sexual Abuse
3.3. Psychological Abuse and Mental Health
3.4. Victimization of Prisoners with Mental Illnesses
3.5. Prison Torture and Autopsy Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torture and Ill Treatment. Available online: http://www.apt.ch/en/knowledge-hub/detention-focus-database/treatment/torture-and-ill-treatment (accessed on 25 November 2022).
- Mcdonald, G.K.; Swaak-Goldman, O. Declaration on the Protection of All Persons from Being Subjected to Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment: General Assembly Resolution 3452 (XXX) 9 December 1975. In Substantive and Procedural Aspects of International Criminal Law; Brill: Leiden, The Netherlands, 2000; pp. 217–218. [Google Scholar]
- Pounder, D.J. The medical contribution to assessing allegations of torture in international fact-finding missions. Forensic Sci. Int. 2011, 208, 143–148. [Google Scholar] [CrossRef] [PubMed]
- European Convention for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment; European Treaty Series No. 126; Council of Europe: Strasbourg, France, 1987; Available online: http://www.cpt.coe.int/en/documents/ecpt.htm (accessed on 25 November 2022).
- The United Nations Commission on Human Rights Resolution 1985/33. Available online: http://www.wunrn.com/news/2008/02_08/02_11_08/021108_un3.htm (accessed on 25 November 2022).
- Optional Protocol to the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, General Assembly of the United Nations Resolution A/RES/57/199. 2002. Available online: http://www2.ohchr.org/english/law/cat-one.htm (accessed on 25 November 2022).
- Bowker, L.H. Prison Victimization; Elsevier: New York, NY, USA, 1980. [Google Scholar]
- Steiner, B.; Ellison, J.M.; Butler, H.D.; Cain, C.M. The Impact of Inmate and PrisonCharacteristics on PrisonerVictimization. TraumaViolence Abus. 2017, 18, 17–36. [Google Scholar]
- Teasdale, B.; Daigle, L.E.; Hawk, S.R.; Daquin, J.C. ViolentVictimization in the PrisonContext: An Examination of the GenderedContexts of Prison. Int. J. Offender Ther. Comp. Criminol. 2016, 60, 995–1015. [Google Scholar] [CrossRef] [PubMed]
- Reidy, T.J.; Sorensen, J.R.; Bonner, H.S. PrisonHomicide: An Extension of ViolentCriminal Careers? J. Interpers. Violence 2020, 35, 5676–5690. [Google Scholar] [CrossRef] [PubMed]
- Stephan, J.J.; Karberg, J.C. Census of State and Federal Correctional Facilities 2000; Bureau of Justice Statistics, U.S. Department of Justice: Washington, DC, USA, 2003.
- Manual on the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (Istanbul Protocol); Professional Training Series No.8; United Nations Office of the High Commissioner for Human Rights: Geneva, Switzerland, 2004; Available online: www.ohchr.org/Documents/Publications/training8Rev1en.pdf (accessed on 25 November 2022).
- Crisanti, A.S.; Frueh, B.C. Risk of trauma exposure among persons with mental illness in jails and prisons: What do we really know? Curr. Opin. Psychiatry 2011, 24, 431–435. [Google Scholar] [CrossRef]
- Pounder, D.J. Torture: Physical findings. In Encyclopedia of Forensic and Legal Medicine; Byard, R., Payne-James, J., Corey, T., Henderson, C., Eds.; Elsevier Academic Press: Amsterdam, The Netherlands, 2005; p. 297302. [Google Scholar]
- Edston, E. The epidemiology of falanga—Incidence among Swedish asylum seekers. Torture 2009, 19, 27–32. [Google Scholar]
- Woldu, S.; Brasholt, M. Suspension torture and its physical sequelae. J. Forensic Leg. Med. 2021, 80, 102155. [Google Scholar] [CrossRef]
- Morentin, B.; Idoyaga, M.I.; Callado, L.F.; Meana, J.J. Prevalence and methods of torture claimed in the Basque Country (Spain) during 1992–1993. Forensic Sci. Int. 1995, 76, 151–158. [Google Scholar] [CrossRef]
- Vogel, H. Allegations of maltreatment in custody. J. Forensic Leg. Med. 2017, 45, 8–16. [Google Scholar] [CrossRef]
- Saukko, P.; Knight, B. Knight’s Forensic Pathology, 3rd ed.; Arnold: London, UK, 2004; pp. 235–244. [Google Scholar]
- Moreno, A.; Grodin, M.A. Torture and its neurological sequelae. Spinal Cord 2002, 40, 213–223. [Google Scholar] [CrossRef]
- Ozkalipci, O.; Unuvar, U.; Sahin, U.; Irencin, S.; Fincanci, S.K. A significant diagnostic method in torture investigation: Bone scintigraphy. Forensic Sci. Int. 2013, 226, 142–145. [Google Scholar] [CrossRef]
- Ozkalipci, O.; Sahin, U.; Baykal, T.; Fincanci, S.; Akhan, O.; Öztop, F.; Lök, V. Atlas of Torture: Use of Medical and Diagnostic Examination Results in Medical Assessment of Torture; Human Right Foundation of Turkey: Ankara, Turkey, 2010. [Google Scholar]
- Mannix, D.P. The History of Torture; Sutton Publishing: Stroud, UK, 2003; p. 46. [Google Scholar]
- Di Mizio, G.; Bolcato, M.; Rivellini, G.; Di Nunzio, M.; Falvo, V.; Nuti, M.; Enrichens, F.; Lucania, L.; Di Nunno, N.; Clerici, M. Protection of Prisoners with Mental Health Disorders in Italy: Lights and Shadows after the Abolition of Judicial Psychiatric Hospitals. Int. J. Environ. Res. Public Health 2022, 19, 9984. [Google Scholar] [CrossRef]
- Neal, T.; Clements, C.B. Prison rape and psychological sequelae: A call for research. Psychol. Public Policy Law 2010, 16, 284. [Google Scholar] [CrossRef]
- Noll, T. Sexualviolence in prison. Int. J. Offender Ther. Comp. Criminol. 2008, 52, 251–252. [Google Scholar] [CrossRef]
- Human Rights Watch. No Escape: Male Rape in US Prisons. 2006. Available online: www.hrw.org/reports/2001/prison/report.html (accessed on 25 November 2022).
- Struckman-Johnson, C.; Struckman-Johnson, D. Sexualcoercionreported by women in threemidwesternprisons. J. Sex Res. 2002, 39, 217–227. [Google Scholar]
- Human Rights Watch. Nowhere to Hide: Retaliation against Women in Michigan State Prisons; Human Rights Watch: New York, NY, USA, 1998. [Google Scholar]
- Burton, D.; Erdman, E.; Hamilton, G.; Muse, K. Women in Prison: Sexual Misconduct by Correctional Staff; US General Accounting Office, General Government Division: Washington, DC, USA, 1999.
- Phelps, M.J. Officers Having Sex with Inmates; Corrections Technology & Management: Wilmette, IL, USA, 1999; Volume 3, pp. 12–20. [Google Scholar]
- Lunde, I.; Ortmann, J. “Sexual Torture and The Treatment of Its Consequences”, Torture and Its Consequences, Current Treatment Approaches; Başoglu, M., Ed.; Cambridge University Press: Cambridge, UK, 1992; pp. 310–331. [Google Scholar]
- Hiday, V.A.; Swanson, J.W.; Swartz, M.S.; Borum, R.; Wagner, H. Victimization: A link between mental illness and violence? Int. J. Law Psychiatry 2001, 24, 559–572. [Google Scholar] [CrossRef]
- Wolff, N.; Blitz, C.L.; Shi, J.; Bachman, R.; Siegel, J.A. Sexual violence inside prisons: Rates of victimization. J. Urban Health 2006, 83, 835–848. [Google Scholar] [CrossRef] [Green Version]
- Dumond, R.W.; Dumond, D.A. The treatment for sexual assault victims. In Prison Sex, Practice and Policy; Hensley, C., Ed.; Rienner Publishers: London, UK, 2002; pp. 67–88. [Google Scholar]
- Fishman, J.F. Crucibles of Crime: The Shocking Story of the American Jail; Patterson Smith: Montclair, NJ, USA, 1968. [Google Scholar]
- Fleisher, M. Warehousing Violence; Sage Publications: Newbury Park, CA, USA, 1989. [Google Scholar]
- Herman, J.L. Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. J. Trauma. Stress 1992, 5, 377–391. [Google Scholar] [CrossRef]
- Turner, S. Surviving Sexual Assault and Sexual Torture. In Male Victims of Sexual Assault; Oxford University Press: New York, NY, USA, 1992; pp. 75–86. [Google Scholar]
- Punamäki, R.L.; Qouta, S.R.; Sarraj, E.E. Nature of torture, PTSD, and somatic symptoms among political ex-prisoners. J. Trauma. Stress 2010, 23, 532–536. [Google Scholar] [CrossRef]
- Başoğlu, M.; Livanou, M.; Crnobarić, C. Torture vs. other cruel, inhuman, and degrading treatment: Is the distinction real or apparent? Arch. Gen. Psychiatry 2007, 64, 277–285. [Google Scholar] [CrossRef]
- Ehlers, A.; Maercker, A.; Boos, A. Posttraumatic stress disorder following political imprisonment: The role of mental defeat, alienation, and perceived permanent change. J. Abnorm. Psychol. 2000, 109, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Emmelkamp, J.; Komproe, I.H.; Van Ommeren, M.; Schagen, S. The relation between coping, social support and psychologicaland somatic symptoms among torture survivors in Nepal. Psychol. Med. 2002, 32, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Komproe, I.H.; Thapa, S.B.; Jordans, M.; Sharma, B.; De Jong, J.T.V.M. Disability associated with psychiatric symptoms among torture survivors in rural Nepal. J. Nerv. Ment. Dis. 2007, 195, 463–469. [Google Scholar] [CrossRef] [PubMed]
- El Sarraj, E.; Punamäki, R.-L.; Salmi, S.; Summer-Field, D. Experiences of torture and ill treatment and posttraumatic stress disorder symptoms among Palestinian political prisoners. J. Trauma. Stress 1996, 9, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Kanninen, K.; Punamäki, R.-L.; Qouta, S. The relation of appraisal, coping efforts, and acuteness of trauma to PTS symptoms among former political prisoners. J. Trauma. Stress 2002, 15, 245–253. [Google Scholar] [CrossRef]
- Silove, D.; Steel, Z.; McGorry, P.; Miles, V.; Drobny, J. The impact of torture on post-traumatic stress symptoms in war-affected Tamil refugees and immigrants. Compr. Psychiatry 2002, 43, 49–55. [Google Scholar] [CrossRef]
- Shrestha, N.M.; Sharma, B.; Van Ommeren, M.; Regmi, S.; Makaju, R.; Komproe, I.; Shrestha, G.B.; de Jong, J.T.V.M. Impact of torture on refugees displaced within the developing world: Symptomatology among Bhutanese refugees in Nepal. JAMA 1998, 280, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Blaauw, E. Bullying and suicides in prison. In Bullying among Prisoners: Innovations in Theory and Research; Ireland, J.L., Ed.; Willan: Portland, OR, USA, 2005; pp. 44–61. [Google Scholar] [CrossRef]
- Cooper, C.; Berwick, S. Factors affecting psychological well-being of three groups of suicide-prone prisoners. Curr. Psychol. 2001, 20, 169–182. [Google Scholar] [CrossRef]
- Hochstetler, A.; Murphy, D.S.; Simons, R.L. Damaged goods: Exploringpredictors of distress in prison inmates. Crime Delinquency 2004, 50, 436–457. [Google Scholar] [CrossRef]
- Wolff, N.; Shi, J. Contextualization of physical and sexual assault in male prisons: Incidents and their aftermath. J. Correct. Health Care 2009, 15, 58–77. [Google Scholar] [CrossRef]
- Dumond, R.W. Inmate sexual assault: The plague that persists. Prison. J. 2000, 80, 407–414. [Google Scholar] [CrossRef]
- First, M.B.; France, A.; Pincus, H.A. DSM-IV-TR Guidebook; American Psychiatric Publishing, Inc.: Washington, DC, USA, 2004. [Google Scholar]
- Boeschen, L.E.; Sales, B.D.; Koss, M.P. Rape trauma experts in thecourtroom. Psychol. Public PolicyLaw 1998, 4, 414–432. [Google Scholar] [CrossRef]
- Kilpatrick, D.G. Rape-related PTSD: Issues and interventions. Psychiatr. Times 2007, 24, 50–54. [Google Scholar]
- Young, C. Assault behind bars: How big a problem is prison rape—And what can be done about it? Reason 2007, 39, 17–19. [Google Scholar]
- Sivakumaran, S. Male/male rape and the “taint” of homosexuality. Hum. Rights Q. 2005, 27, 1274–1306. [Google Scholar] [CrossRef]
- Atkeson, B.M.; Calhoun, K.S.; Resick, P.A.; Ellis, E.M. Victims of rape:Repeated assessment of depressive symptoms. J. Consult. Clin. Psychol. 1982, 50, 96–102. [Google Scholar] [CrossRef]
- Fields, R.M. The neurobiological consequences of psychological torture. In The Trauma of Psychological Torture; Ojeda, A.E., Ed.; Praeger: Westport, CT, USA, 2008; pp. 155–162. [Google Scholar]
- Başoğlu, M. A multivariate contextual analysis of torture and cruel, inhuman, and degrading treatments: Implications for an evidence-based definition of torture. Am. J. Orthopsychiatry 2009, 79, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Taghaddosinejad, F.; Sheikhazadi, A.; Yaghmaei, A.; Vakili, V.; Saberi, S.M.; Behnoush, B. A survey of self-mutilation from forensic medicine viewpoint. Am. J. Forensic Med. Pathol. 2009, 30, 313–317. [Google Scholar] [CrossRef]
- Beck, A.J.; Harrison, P.M. Bureau of Justice Statistics Special Report: Prison Rape Elimination Act of 2003–Sexual Victimization in State and Federal Prisons Reported by Inmates, 2007; Report no.: NCJ219414; US Department of Justice: Office of Justice Programs: Washington, DC, USA, 2008.
- Wolff, N.; Frueh, B.C.; Shi, J.; Gerardi, D.; Fabrikant, N.; Schumann, B.E. Trauma exposure and mental health characteristics of incarcerated females self-referred to specialty PTSD treatment. Psychiatr. Serv. 2011, 62, 954–958. [Google Scholar] [CrossRef]
- Wolff, N.; Blitz, C.L.; Shi, J. Rates of sexual victimization in prison for inmates with and without mental disorders. Psychiatr. Serv. 2007, 58, 1087–1094. [Google Scholar] [CrossRef]
- Austin, J.; Fabelo, T.; Gunter, A.; McGinnis, K. Sexual Violence in the Texas Prison System; JFA Institute: Washington, DC, USA, 2006. [Google Scholar]
- Steadman, H.J.; Osher, F.C.; Robbins, P.C.; Case, B.; Samuels, S. Prevalence of serious mental illness among jail inmates. Psychiatr. Serv. 2009, 60, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Silver, E.; Arseneault, L.; Langley, J.; Caspi, A.; Moffitt, T.E. Mental disorder and violent victimization in a total birth cohort. Am. J. Public Health 2005, 95, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Marley, J.A.; Buila, S. Crimes against people with mental illness: Types, perpetrators, and influencing factors. Soc. Work 2001, 46, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Hiday, V.A. The social context of mental illness and violence. J. Health Soc. Behav. 1995, 36, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Goodman, L.A.; Dutton, M.A.; Harris, M. The relationship between violence dimensions and symptom severity among homeless, mentally ill women. J. Trauma. Stress 1997, 10, 51–70. [Google Scholar] [CrossRef]
- Cusack, K.J.; Frueh, B.C.; Brady, K.T. Trauma history screening in a community mental health center. Psychiatr. Serv. 2004, 55, 157–162. [Google Scholar] [CrossRef]
- Grubaugh, A.L.; Zinzow, H.M.; Paul, L.; Egede, L.E.; Frueh, B.C. Trauma exposure and posttraumatic stress disorder in adults with severe mental illness: A critical review. Clin. Psychol. Rev. 2011, 31, 883–899. [Google Scholar] [CrossRef] [Green Version]
- Fineschi, V.; Dell’Erba, A.S.; Di Paolo, M.; Procaccianti, P. Typical homicide ritual of the Italian Mafia (incaprettamento). Am. J. Forensic Med. Pathol. 1998, 19, 87–92. [Google Scholar] [CrossRef]
- Maglietta, F.; Sessa, F.; Albano, G.D.; Bertozzi, G.; Giugliano, P.; Vacchiano, G.; Salerno, M. Italian mafia: A focus on Apulia mafia with a literature review. Acta Medica Mediterranea 2017, 6, 947–952. [Google Scholar]
- Pollanen, M.S. A variant of incaprettamento (ritual ligature strangulation) in East Timor. Am. J. Forensic Med. Pathol. 2003, 24, 51–54. [Google Scholar] [CrossRef]
- Pollanen, M.S. Fatal rhabdomyolysis after torture by reverse hanging. Forensic Sci. Med. Pathol. 2016, 12, 170–173. [Google Scholar] [CrossRef]
- Meel, B.L. Fatal pulmonary thromboembolism following physical torture. J. Clin. Forensic Med. 2003, 10, 259–262. [Google Scholar] [CrossRef]
- Maslen, S. The Minnesota Protocol on the investigation of potentially unlawful death (2016). In Forensic Science International; Elsevier: Clare, Ireland, 2017; Volume 277, p. 142. [Google Scholar]
- ICRC. Guidelines for Investigating Deaths in Custody; International Committee for the Red Cross: Geneva, Switzerland, 2013. [Google Scholar]
- International Rehabilitation Council for Torture Victims Medical Physical Examination of Alleged Torture Victims. A Practical Guide to The Istanbul Protocol—For Medical Doctors. 2009. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjHqYi-6pb9AhUPdt4KHfJZBfoQFnoECAgQAQ&url=https%3A%2F%2Fflyktning.net%2Fmedia%2Fistanbulprotokollen-manual-for-dokumentasjon-av-torturskader.pdf&usg=AOvVaw0SlLziopedmSIK_d18Rz5B (accessed on 25 November 2022).
- Pollanen, M.S. The pathology of torture. Forensic Sci. Int. 2018, 284, 85–96. [Google Scholar] [CrossRef]
- Byard, R.W.; Singh, B. Falanga torture: Characteristic features and diagnostic issues. Forensic Sci. Med. Pathol. 2012, 8, 320–322. [Google Scholar] [CrossRef]
- Aborisade, R.A.; Obileye, A.A. Systematic brutality, torture and abuse of human rights by the Nigerian Police: Narratives of inmates in Ogun State prisons. Niger. J. Sociol. Anthropol. 2017, 15, 2. [Google Scholar] [CrossRef]
- Heisler, M.; Moreno, A.; De Monner, S.; Keller, A.; Iacopino, V. Assessment of torture and ill treatment of detainees in Mexico: Attitudesand experiences of forensic physicians. JAMA 2003, 289, 2135–2143. [Google Scholar] [CrossRef]
- Busch, J.; Hansen, S.H.; Hougen, H.P. Geographical distribution of torture: An epidemiological study of torture reported by asylum applicants examined at the Department of Forensic Medicine, University of Copenhagen. Torture 2015, 25, 12–21. [Google Scholar] [CrossRef]
- Bolcato, M.; Fiore, V.; Casella, F.; Babudieri, S.; Lucania, L.; Di Mizio, G. Health in Prison: Does Penitentiary Medicine in Italy Still Exist? Healthcare 2021, 9, 1511. [Google Scholar] [CrossRef]
- Lo Re, G.; Argo, A.; Midiri, M.; Cattaneo, C. Radiology in Forensic Medicine: From Identification to Post-Mortem Imaging; Springer: Berlin/Heidelberg, Germany, 2019; pp. 1–301. [Google Scholar]
- Serraino, S.; Milone, L.; Picone, D.; Salerno, S.; Midiri, M. Imaging for Ballistic Trauma: Other Applications of Forensic Imaging in the Living. In Radiology in Forensic Medicine: From Identification to Post-Mortem Imaging; Springer: Berlin/Heidelberg, Germany, 2019; pp. 169–180. [Google Scholar]
- Camarda, L.; D’Arienzo, A.; Grassedonio, E.; Zerbo, S.; Argo, A.; D’Arienzo, M. Self-inflicted long bone fractures for insurance fraud. Int. J. Legal. Med. 2019, 133, 1083–1088. [Google Scholar] [CrossRef]
- Lo Re, G.; Salerno, M.; Terranova, M.C.; Argo, A.; LoCasto, A.; Zerbo, S.; Lagalla, R. Virtopsy and Living Individuals Evaluation Using Computed Tomography in Forensic Diagnostic Imaging. Semin. Ultrasound CT MRI 2019, 40, 67–78. [Google Scholar] [CrossRef]
- Esposito, M.; Salerno, M.; Di Nunno, N.; Ministeri, F.; Liberto, A.; Sessa, F. The Risk of COVID-19 Infection in Prisons and Prevention Strategies: A Systematic Review and a New Strategic Protocol of Prevention. Healthcare 2022, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Rogan, M. Prison Inspection and Monitoring: The Need to Reform European Law and Policy. Eur. J. Crim.Policy Res. 2021, 27, 285–305. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maltreatment Method | Common Findings |
|---|---|
| Blunt impact trauma | Physical injuries are often nonspecific, but hits with batons, electric cables, and sticks commonly leave classic “track” bruises that can leave permanent hypo- or hyperpigmented scars. |
| Falanga | Superficial hemorrhage occurs in the soles of the feet, with a possible extension in the dorsum of the feet. Large bruises on the feet, with deformity, are rare. |
| Electric injury | Electric marks are reddish-brown in color, with inflamed margins, before they darken, resolve completely, or leave thin white scars, which are punctiform when a wire end has been used. These might be partially circumferential, wrapping around a finger, if the wire was wrapped around it. Clusters of punctiform scars (picana) in unusual locations, including the toes or the foreskin, are strongly suggestive and typical of maltreatment using electric current. They are small and, therefore, they may remain undetected unless explicitly pointed out by the detainee. |
| Asphyxiation | It usually leaves no marks, and recovery is rapid. Only in rare cases can it result in fractures of the larynx or softtissue scarring. |
| Stress position | All forms of suspension or ligature involving limb ligation can cause scars and ligature marks of specific types and in specific locations.Musculoskeletal and nerve injuries can also occur. |
| Thermal injuries | Cigarette burns often leave 5 to 10 mm-long circular or ovoid macular scars. They may have a hyper- or hypopigmented center and a hyperpigmented, relatively indistinct periphery. Burning with hot objects produces markedly atrophic scars that reflect the shape of the tool and are sharply demarcated by hypertrophic or hyperpigmented marginal areas that relate to the initial zone of inflammation. The burn may result in hypertrophic or keloid scars, as in the case of a burn caused by burning rubber. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, G.D.; Guadagnino, D.; Midiri, M.; La Spina, C.; Tullio, V.; Argo, A.; Zerbo, S. Torture and Maltreatment in Prison: A Medico-Legal Perspective. Healthcare 2023, 11, 576. https://doi.org/10.3390/healthcare11040576
Albano GD, Guadagnino D, Midiri M, La Spina C, Tullio V, Argo A, Zerbo S. Torture and Maltreatment in Prison: A Medico-Legal Perspective. Healthcare. 2023; 11(4):576. https://doi.org/10.3390/healthcare11040576
Chicago/Turabian StyleAlbano, Giuseppe Davide, Daniela Guadagnino, Mauro Midiri, Corinne La Spina, Valeria Tullio, Antonina Argo, and Stefania Zerbo. 2023. "Torture and Maltreatment in Prison: A Medico-Legal Perspective" Healthcare 11, no. 4: 576. https://doi.org/10.3390/healthcare11040576
APA StyleAlbano, G. D., Guadagnino, D., Midiri, M., La Spina, C., Tullio, V., Argo, A., & Zerbo, S. (2023). Torture and Maltreatment in Prison: A Medico-Legal Perspective. Healthcare, 11(4), 576. https://doi.org/10.3390/healthcare11040576