
A Single-Center, Randomized Controlled Trial to Test the Efficacy of Nurse-Led Motivational Interviewing for Enhancing Self-Care in Adults with Heart Failure

 , , , , ,
, , , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Setting
2.3. Participants
2.4. Experimental Arms
2.5. Standard of Care and Control Group
2.6. Procedures
2.7. Randomization
2.8. Measurements
Outcomes
2.9. Sample Size
2.10. Treatment Fidelity
2.11. Timeline
2.12. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Self-Care Maintenance (Primary Endpoint), Management, and Confidence at the First Follow-Up (T1, 3 Months)
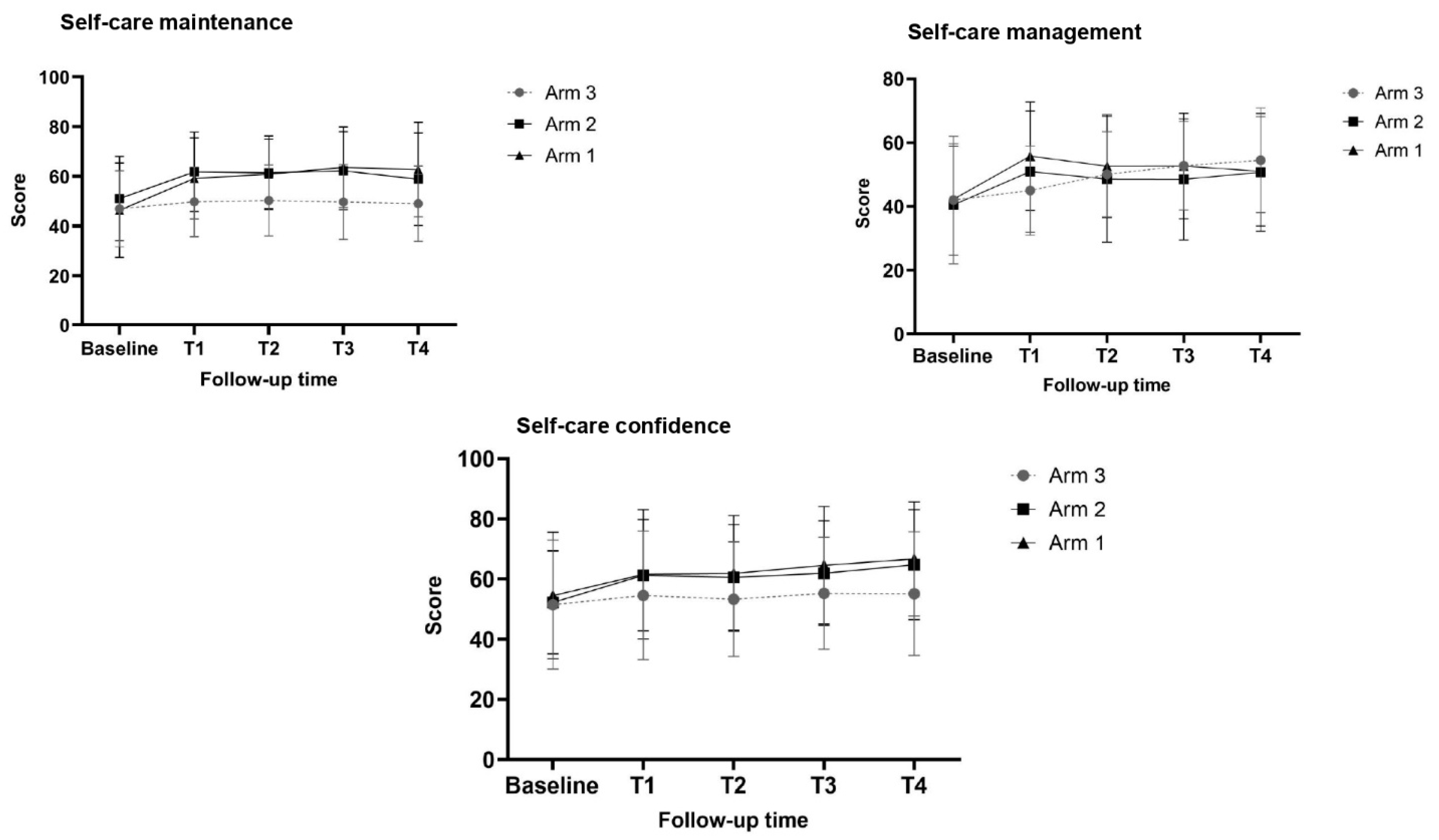
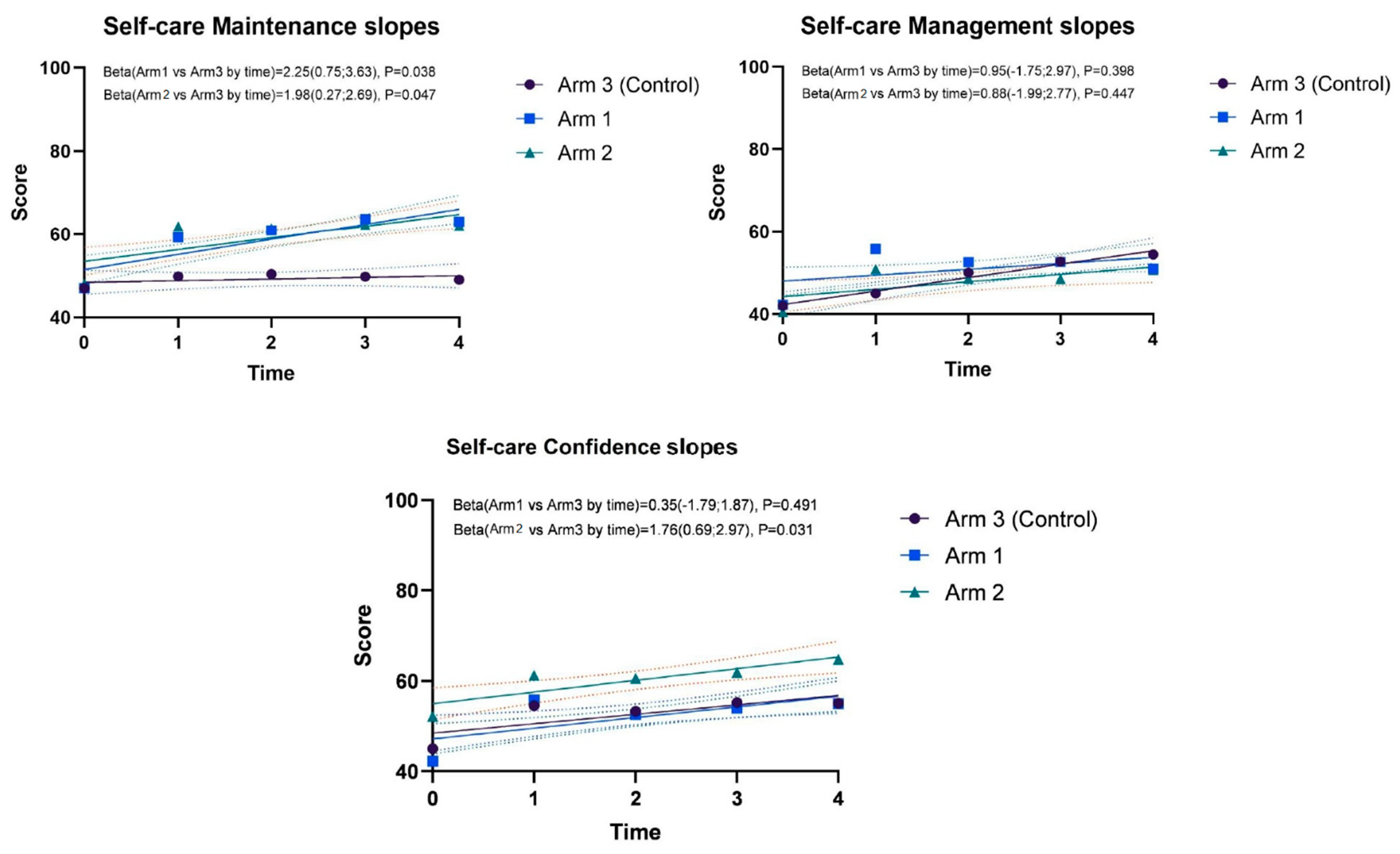
3.3. Changes in Self-Care Maintenance, Management, and Confidence over Follow-Up Times
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.A.; Hayden, K.A.; Raffin Bouchal, S.; King-Shier, K. Self-Care Practices of Patients with Heart Failure Using Wearable Electronic Devices: A Systematic Review. J. Cardiovasc. Nurs. Epub ahead of print. 2022. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.C.; Liljeroos, M.; Dwyer, A.A.; Jaques, C.; Girard, J.; Strömberg, A.; Hullin, R.; Schäfer-Keller, P. Symptom Perception in Heart Failure—Interventions and Outcomes: A Scoping Review. Int. J. Nurs. Stud. 2021, 116, 103524. [Google Scholar] [CrossRef]
- Kim, E.Y.; Oh, S.; Son, Y.-J. Caring Experiences of Family Caregivers of Patients with Heart Failure: A Meta-Ethnographic Review of the Past 10 Years. Eur. J. Cardiovasc. Nurs. 2020, 19, 473–485. [Google Scholar] [CrossRef]
- Sokalski, T.; Hayden, K.A.; Raffin Bouchal, S.; Singh, P.; King-Shier, K. Motivational Interviewing and Self-Care Practices in Adult Patients with Heart Failure: A Systematic Review and Narrative Synthesis. J. Cardiovasc. Nurs. 2020, 35, 107–115. [Google Scholar] [CrossRef]
- Dellafiore, F.; Conte, G.; Baroni, I.; Magon, A.; Pittella, F.; Casole, L.; Caruso, R. Gender Differences in Heart Failure Self-Care Behaviors: Do We Know Enough? Minerva Med. 2018, 109, 401–403. [Google Scholar] [CrossRef]
- Trenta, A.M.; Ausili, D.; Caruso, R.; Arrigoni, C.; Moro, M.; Nania, T.; Vellone, E.; Dellafiore, F. Living with Heart Failure during the COVID-19 Pandemic: An Interpretative Phenomenological Analysis. Clin. Nurs. Res. 2021, 30, 1071–1078. [Google Scholar] [CrossRef]
- Westland, H.; Page, S.D.; van Rijn, M.; Aryal, S.; Freedland, K.E.; Lee, C.; Strömberg, A.; Vellone, E.; Wiebe, D.J.; Jaarsma, T.; et al. Self-Care Management of Bothersome Symptoms as Recommended by Clinicians for Patients with a Chronic Condition: A Delphi Study. Heart Lung 2022, 56, 40–49. [Google Scholar] [CrossRef]
- Yang, Y.-F.; Hoo, J.-X.; Tan, J.-Y.; Lim, L.-L. Multicomponent Integrated Care for Patients with Chronic Heart Failure: Systematic Review and Meta-Analysis. ESC Heart Fail. 2022. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, T.; Chair, S.Y. Effectiveness of Nurse-Led Self-Care Interventions on Self-Care Behaviors, Self-Efficacy, Depression and Illness Perceptions in People with Heart Failure: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2022, 132, 104255. [Google Scholar] [CrossRef]
- Liu, S.; Li, J.; Wan, D.-Y.; Li, R.; Qu, Z.; Hu, Y.; Liu, J. Effectiveness of EHealth Self-Management Interventions in Patients With Heart Failure: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2022, 24, e38697. [Google Scholar] [CrossRef]
- Riegel, B.; Jaarsma, T.; Strömberg, A. A Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riegel, B.; Dickson, V.V.; Faulkner, K.M. The Situation-Specific Theory of Heart Failure Self-Care: Revised and Updated. J. Cardiovasc. Nurs. 2016, 31, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Rebora, P.; Spedale, V.; Occhino, G.; Luciani, M.; Alvaro, R.; Vellone, E.; Riegel, B.; Ausili, D. Effectiveness of Motivational Interviewing on Anxiety, Depression, Sleep Quality and Quality of Life in Heart Failure Patients: Secondary Analysis of the MOTIVATE-HF Randomized Controlled Trial. Qual. Life Res. 2021, 30, 1939–1949. [Google Scholar] [CrossRef]
- Vellone, E.; Rebora, P.; Ausili, D.; Zeffiro, V.; Pucciarelli, G.; Caggianelli, G.; Masci, S.; Alvaro, R.; Riegel, B. Motivational Interviewing to Improve Self-care in Heart Failure Patients (MOTIVATE-HF): A Randomized Controlled Trial. ESC Heart Fail. 2020, 7, 1309–1318. [Google Scholar] [CrossRef]
- Chew, H.S.J.; Cheng, H.Y.; Chair, S.Y. The Suitability of Motivational Interviewing versus Cognitive Behavioural Interventions on Improving Self-Care in Patients with Heart Failure: A Literature Review and Discussion Paper. Appl. Nurs. Res. 2019, 45, 17–22. [Google Scholar] [CrossRef]
- Kent, B.; Cull, E.; Phillips, N.M. A Systematic Review of the Effectiveness of Current Interventions to Assist Adults with Heart Failure to Comply with Therapy and Enhance Self-Care Behaviours. JBI Libr. Syst. Rev. 2011, 9, 2572–2626. [Google Scholar] [CrossRef] [PubMed]
- Poudel, N.; Kavookjian, J.; Scalese, M.J. Motivational Interviewing as a Strategy to Impact Outcomes in Heart Failure Patients: A Systematic Review. Patient 2020, 13, 43–55. [Google Scholar] [CrossRef]
- Barrett, S.; Begg, S.; O’Halloran, P.; Kingsley, M. Integrated Motivational Interviewing and Cognitive Behaviour Therapy for Lifestyle Mediators of Overweight and Obesity in Community-Dwelling Adults: A Systematic Review and Meta-Analyses. BMC Public Health 2018, 18, 1160. [Google Scholar] [CrossRef] [Green Version]
- Judice Jones, N.; Richard, A. Implementing Evidence-Based Motivational Interviewing Strategies in the Care of Patients with Heart Failure. Crit. Care Nurs. Clin. N. Am. 2022, 34, 191–204. [Google Scholar] [CrossRef]
- Wu, J.; Yu, Y.; Xu, H. Influence of Targeted Motivational Interviewing on Self-Care Level and Prognosis during Nursing Care of Chronic Heart Failure. Am. J. Transl. Res. 2021, 13, 6576–6583. [Google Scholar]
- Miller, W.R.; Rollnick, S. Ten Things That Motivational Interviewing Is Not. Behav. Cogn. Psychother. 2009, 37, 129–140. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Chang, Y.-P. The Effect of Nurse-Led Motivational Interviewing on Medication Adherence in Patients With Bipolar Disorder: The Effect of Nurse-Led Motivational Interviewing on Medication Adherence in Patients With Bipolar Disorder. Perspect. Psychiatr. Care 2015, 51, 36–44. [Google Scholar] [CrossRef]
- Ehrlich, O.; Brandoff, D.; Gorman, D.P.; Berry, D.L. Nurse-Led Motivational Interviewing for Setting Functional Cancer Pain Goals. Pain Manag. Nurs. 2021, 22, 716–723. [Google Scholar] [CrossRef]
- Ghizzardi, G.; Arrigoni, C.; Dellafiore, F.; Vellone, E.; Caruso, R. Efficacy of Motivational Interviewing on Enhancing Self-Care Behaviors among Patients with Chronic Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Heart Fail. Rev. 2022, 27, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE Approach in Systematic Reviews and Guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Mollica, G.; Caruso, R.; Conte, G.; Ambrogi, F.; Boveri, S. Analysing Researchers’ Engagement in Research Hospitals: A Pilot Study in IRCCS-Italian Research Hospitals. Healthcare 2022, 10, 2458. [Google Scholar] [CrossRef]
- Frigiola, A.; Moussaidi, N.; Giamberti, A.; Pomé, G.; Isgrò, G.; Youssef, T.; Reali, M.; Varrica, A.; Nuri, H.A.; Cirri, S.; et al. International Cooperation in Healthcare: Model of IRCCS Policlinico San Donato and Bambini Cardiopatici Nel Mondo Association for Congenital Heart Diseases. Eur. Heart J. Suppl. 2016, 18, E72–E78. [Google Scholar] [CrossRef] [Green Version]
- Vellone, E.; Riegel, B.; Cocchieri, A.; Barbaranelli, C.; D’Agostino, F.; Antonetti, G.; Glaser, D.; Alvaro, R. Psychometric Testing of the Self-care of Heart Failure Index Version 6.2. Res. Nurs. Health 2013, 36, 500–511. [Google Scholar] [CrossRef] [Green Version]
- Callahan, C.M.; Unverzagt, F.W.; Hui, S.L.; Perkins, A.J.; Hendrie, H.C. Six-Item Screener to Identify Cognitive Impairment among Potential Subjects for Clinical Research. Med. Care 2002, 40, 771–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment: MOCA: A Brief Screening Tool for Mci. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Dellafiore, F.; Arrigoni, C.; Palpella, F.; Diazzi, A.; Orrico, M.; Magon, A.; Pittella, F.; Caruso, R. Effects of Mutuality, Anxiety, and Depression on Quality of Life of Patients with Heart Failure: A Cross-Sectional Study. Create. Nurs. 2021, 27, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Moyers, T.B.; Martin, T.; Manuel, J.K.; Hendrickson, S.M.L.; Miller, W.R. Assessing Competence in the Use of Motivational Interviewing. J. Subst. Abus. Treat. 2005, 28, 19–26. [Google Scholar] [CrossRef]
- Kwak, S.G.; Kim, J.H. Central Limit Theorem: The Cornerstone of Modern Statistics. Korean J. Anesth. 2017, 70, 144. [Google Scholar] [CrossRef] [Green Version]
- Kraft, M.A. Interpreting Effect Sizes of Education Interventions. Educ. Res. 2020, 49, 241–253. [Google Scholar] [CrossRef]
- Flores, P.V.P.; Rocha, P.A.; Figueiredo, L. da S.; Guimarães, T.M.L.; Velasco, N.S.; Cavalcanti, A.C.D. Effect of motivational interviewing on self-care of people with heart failure: A randomized clinical trial. Rev. Esc. Enferm. USP 2020, 54, e03634. [Google Scholar] [CrossRef]
- Paranjpe, R.; Vadhariya, A.; Choi, J.; Essien, E.J.; Esse, T.W.; Gallardo, E.; Serna, O.; Abughosh, S. Evaluating Trajectories of Statin Adherence after a Motivational Interviewing Intervention. J. Am. Pharm. Assoc. 2020, 60, 892–898. [Google Scholar] [CrossRef]
- Masterson Creber, R.; Patey, M.; Lee, C.S.; Kuan, A.; Jurgens, C.; Riegel, B. Motivational Interviewing to Improve Self-Care for Patients with Chronic Heart Failure: MITI-HF Randomized Controlled Trial. Patient Educ. Couns. 2016, 99, 256–264. [Google Scholar] [CrossRef] [Green Version]
- Celano, C.M.; Freedman, M.E.; Harnedy, L.E.; Park, E.R.; Januzzi, J.L.; Healy, B.C.; Huffman, J.C. Feasibility and Preliminary Efficacy of a Positive Psychology-Based Intervention to Promote Health Behaviors in Heart Failure: The REACH for Health Study. J. Psychosom. Res. 2020, 139, 110285. [Google Scholar] [CrossRef]
- Beckwith, V.Z.; Beckwith, J. Motivational Interviewing: A Communication Tool to Promote Positive Behavior Change and Optimal Health Outcomes. NASN Sch. Nurse 2020, 35, 344–351. [Google Scholar] [CrossRef]
- Tooley, E.M.; Kolahi, A. Motivating Behavioral Change. Med. Clin. N. Am. 2022, 106, 627–639. [Google Scholar] [CrossRef]
- Budhwani, H.; Naar, S. Training Providers in Motivational Interviewing to Promote Behavior Change. Pediatr. Clin. N. Am. 2022, 69, 779–794. [Google Scholar] [CrossRef]
- Wilson, A.M.M.M.; de Almeida, G.S.M.; Santos, B. de C.F. dos; Nakahara-Melo, M.; Conceição, A.P. da; Cruz, D. de A.L.M. da Fatores Associados à Contribuição Dos Cuidadores Para o Autocuidado Na Insuficiência Cardíaca. Rev. Lat. Am. Enferm. 2022, 30, e3632. [Google Scholar] [CrossRef]
- Vellone, E.; D’Agostino, F.; Buck, H.G.; Fida, R.; Spatola, C.F.; Petruzzo, A.; Alvaro, R.; Riegel, B. The Key Role of Caregiver Confidence in the Caregiver’s Contribution to Self-Care in Adults with Heart Failure. Eur. J. Cardiovasc. Nurs. 2015, 14, 372–381. [Google Scholar] [CrossRef] [Green Version]
- Vellone, E.; Biagioli, V.; Durante, A.; Buck, H.G.; Iovino, P.; Tomietto, M.; Colaceci, S.; Alvaro, R.; Petruzzo, A. The Influence of Caregiver Preparedness on Caregiver Contributions to Self-Care in Heart Failure and the Mediating Role of Caregiver Confidence. J. Cardiovasc. Nurs. 2020, 35, 243–252. [Google Scholar] [CrossRef]
- Cajita, M.I.; Cajita, T.R.; Han, H.-R. Health Literacy and Heart Failure: A Systematic Review. J. Cardiovasc. Nurs. 2016, 31, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.B.; Ayatollahi, Y.; Yamashita, T.; Jaradat, M.; Shen, J.J.; Kim, S.J.; Lee, Y.-J.; Hwang, J.; Yeom, H.; Upadhyay, S.; et al. Health Literacy and Mortality in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Res. Gerontol. Nurs. 2019, 12, 99–108. [Google Scholar] [CrossRef]
- Fabbri, M.; Murad, M.H.; Wennberg, A.M.; Turcano, P.; Erwin, P.J.; Alahdab, F.; Berti, A.; Manemann, S.M.; Yost, K.J.; Finney Rutten, L.J.; et al. Health Literacy and Outcomes Among Patients with Heart Failure: A Systematic Review and Meta-Analysis. JACC Heart Fail. 2020, 8, 451–460. [Google Scholar] [CrossRef]
- Riegel, B.; Dickson, V.V.; Vellone, E. The Situation-Specific Theory of Heart Failure Self-Care: An Update on the Problem, Person, and Environmental Factors Influencing Heart Failure Self-Care. J. Cardiovasc. Nurs. 2022, 37, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, T.; Hill, L.; Bayes-Genis, A.; La Rocca, H.-P.B.; Castiello, T.; Čelutkienė, J.; Marques-Sule, E.; Plymen, C.M.; Piper, S.E.; Riegel, B.; et al. Self-Care of Heart Failure Patients: Practical Management Recommendations from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Riccardi, M.; Sammartino, A.M.; Piepoli, M.; Adamo, M.; Pagnesi, M.; Rosano, G.; Metra, M.; von Haehling, S.; Tomasoni, D. Heart Failure: An Update from the Last Years and a Look at the near Future. ESC Heart Fail. 2022, 9, 3667–3693. [Google Scholar] [CrossRef]
- Vellone, E.; Fida, R.; D’Agostino, F.; Mottola, A.; Juarez-Vela, R.; Alvaro, R.; Riegel, B. Self-Care Confidence May Be the Key: A Cross-Sectional Study on the Association between Cognition and Self-Care Behaviors in Adults with Heart Failure. Int. J. Nurs. Stud. 2015, 52, 1705–1713. [Google Scholar] [CrossRef] [Green Version]
- Caruso, R.; Rebora, P.; Dellafiore, F.; Fabrizi, D.; Riegel, B.; Ausili, D.; Di Mauro, S. Clinical and Socio-Demographic Determinants of Inadequate Self-Care in Adults with Type 1 Diabetes Mellitus: The Leading Role of Self-Care Confidence. Acta Diabetol. 2019, 56, 151–161. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Arm 1: MI Only for Patients (n = 61) | Arm 2: MI for Patients and Caregivers (n = 60) | Arm 3: Usual Care for Patients and Caregivers (n = 61) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Variables | ||||||||
| Sex | ||||||||
| Males | 33 | 54.1 | 33 | 55.0 | 32 | 52.5 | 0.960 | |
| Age | ||||||||
| Years (mean; SD) | 68.39 | 12.14 | 69.44 | 6.71 | 71.08 | 12.95 | 0.403 | |
| Marital status | ||||||||
| Single | 8 | 13.1 | 10 | 16.7 | 9 | 14.8 | 0.374 | |
| Married | 33 | 54.1 | 27 | 45.0 | 23 | 37.7 | ||
| Divorced | 8 | 13.1 | 10 | 16.7 | 7 | 11.5 | ||
| Widower | 12 | 19.7 | 13 | 21.7 | 22 | 36.1 | ||
| Education | ||||||||
| High schools or higher | 17 | 27.9 | 15 | 25.0 | 16 | 26.2 | 0.937 | |
| Employment | ||||||||
| Retired | 50 | 82.0 | 48 | 80.0 | 45 | 73.8 | 0.423 | |
| Income | ||||||||
| More than necessary to live | 6 | 9.8 | 8 | 13.3 | 10 | 16.4 | 0.264 | |
| The necessary to live | 46 | 75.4 | 44 | 73.4 | 49 | 80.3 | ||
| Not necessary to live | 9 | 14.8 | 8 | 13.3 | 2 | 3.3 | ||
| Time with HF | ||||||||
| Months (median; IQR) | 48.00 | 24.00–70.00 | 47.50 | 26.75–60.00 | 46.50 | 27.00–67.00 | 0.315 | |
| BMI | ||||||||
| Kg/m2 (median; IQR) | 24.36 | 22.00–27.92 | 25.00 | 22.75–26.5 | 25.71 | 22.00–28.31 | 0.585 | |
| MoCA | ||||||||
| Score (median; IQR) | 28.00 | 18.00–30.00 | 25.00 | 19.00–29.00 | 25.00 | 21.00–28.00 | 0.456 | |
| NYHA Class | ||||||||
| II | 36 | 59.00 | 38 | 63.3 | 42 | 68.9 | 0.595 | |
| III | 21 | 34.4 | 18 | 30.0 | 18 | 29.5 | ||
| IV | 4 | 6.6 | 4 | 6.7 | 1 | 1.6 | ||
| CCI | ||||||||
| Score (median; IQR) | 2 | 2.0–5.0 | 2 | 2.0–4.0 | 2 | 1.0–4.0 | 0.877 | |
| EF | ||||||||
| HFpEF | 31 | 50.8 | 32 | 53.3 | 34 | 55.7 | 0.855 | |
| HFmrEF | 14 | 23.0 | 10 | 16.7 | 13 | 21.3 | ||
| HFrEF | 16 | 26.2 | 18 | 30.0 | 14 | 23.0 | ||
| Self-care maintenance | ||||||||
| Inadequate (score < 70) | 54 | 88.5 | 53 | 88.3 | 57 | 93.4 | 0.564 | |
| Self-care management ¥ | ||||||||
| Inadequate (score < 70) | 47 | 95.9 | 51 | 98.1 | 34 | 94.40 | 0.657 | |
| Self-care confidence | ||||||||
| Inadequate (score < 70) | 44 | 72.1 | 48 | 80.00 | 52 | 85.2 | 0.200 | |
| Self-care maintenance | ||||||||
| Score (0–100) (median; IQR) | 46.66 | 29.56–63.33 | 53.33 | 35.83–63.33 | 46.66 | 36.67–56.66 | 0.162 | |
| Self-care management ¥ | ||||||||
| Score (0–100) (median; IQR) | 41.00 | 29.00–55.25 | 41.28 | 25.00–57.50 | 45.11 | 28.75–55.00 | 0.566 | |
| Self-care confidence | ||||||||
| Score (0–100) (median; IQR) | 50.04 | 45.56–71.20 | 52.41 | 37.82–67.24 | 51.00 | 38.92–66.72 | 0.687 | |
| Arm 1: MI Only for Patients (n = 61) | Arm 2: MI for Patients and Caregivers (n = 60) | Arm 3: Usual Care for Patients and Caregivers (n = 61) | Arm 1 vs. Arm 3 Cohen’s d (p-Value) | Arm 2 vs. Arm 3 Cohen’s d (p-Value) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Mean | SD | Mean | SD | ||||
| Δ in Self-care maintenance scores | ||||||||||
| T1 | 182 | 12.84 | 11.50 | 10.81 | 13.05 | 2.78 | 10.33 | 0.92 (<0.001) | 0.68 (<0.001) | |
| T2 | 182 | 14.60 | 11.92 | 10.39 | 12.01 | 3.34 | 11.57 | 0.96 (<0.001) | 0.60 (<0.001) | |
| T3 | 182 | 17.31 | 14.71 | 11.23 | 13.68 | 2.73 | 14.59 | 0.99 (<0.001) | 0.60 (0.001) | |
| T4 | 182 | 16.37 | 17.95 | 7.82 | 13.89 | 2.02 | 11.91 | 0.94 (<0.001) | 0.45 (0.015) | |
| Δ in Self-care management scores | ||||||||||
| T1 | 114 | 14.26 | 19.29 | 11.50 | 28.61 | 10.12 | 23.06 | 0.20 (0.788) | 0.05(0.586) | |
| T2 | 107 | 11.65 | 20.41 | 8.51 | 20.26 | 9.4 | 17.88 | 0.12 (0.672) | 0.05 (0.427) | |
| T3 | 108 | 11.12 | 18.64 | 7.79 | 20.40 | 9.2 | 16.72 | 0.11 (0.663) | 0.07 (0.382) | |
| T4 | 101 | 11.50 | 18.16 | 12.04 | 19.10 | 12.57 | 23.36 | 0.05 (0.421) | 0.03 (0.462) | |
| Δ in Self-care confidence scores | ||||||||||
| T1 | 182 | 7.11 | 14.22 | 9.04 | 6.84 | 3.06 | 12.84 | 0.31 (0.101) | 0.58 (0.002) | |
| T2 | 182 | 7.40 | 16.06 | 8.36 | 9.78 | 1.79 | 17.54 | 0.24 (0.183) | 0.37 (0.043) | |
| T3 | 182 | 10.08 | 17.71 | 9.69 | 9.07 | 3.75 | 16.55 | 0.37 (0.044) | 0.32 (0.079) | |
| T4 | 182 | 12.13 | 13.47 | 12.56 | 10.13 | 3.60 | 18.55 | 0.53 (0.004) | 0.60 (0.001) | |
| Arm 1 vs. Arm 3 (p-Value) | Arm 2 vs. Arm 3 (p-Value) | |||||||||
| Patients adequate in self-care maintenance (scores ≥ 70) | ||||||||||
| N | % | N | % | N | % | |||||
| T1 | 19 | 31.1 | 26 | 43.3 | 4 | 6.6 | 1.000 | 0.626 | ||
| T2 | 21 | 34.4 | 19 | 31.7 | 4 | 6.6 | 0.134 | 0.297 | ||
| T3 | 29 | 47.5 | 21 | 35.0 | 14 | 23.0 | 0.313 | 0.751 | ||
| T4 | 23 | 37.7 | 23 | 38.3 | 19 | 31.3 | 0.507 | 0.872 | ||
| Patients adequate in self-care management (scores ≥ 70) | ||||||||||
| N | % | N | % | N | % | |||||
| T1 | 14 | 30.4 | 11 | 21.6 | 6 | 14.3 | 1.000 | 0.295 | ||
| T2 | 11 | 24.4 | 10 | 20.0 | 3 | 8.6 | 0.342 | 0.545 | ||
| T3 | 11 | 25.6 | 8 | 17.0 | 5 | 12.8 | 0.454 | 0.269 | ||
| T4 | 7 | 15.9 | 10 | 22.7 | 7 | 21.2 | 0.342 | 0.330 | ||
| Patients adequate in self-care confidence (scores ≥ 70) | ||||||||||
| N | % | N | % | N | % | |||||
| T1 | 19 | 31.1 | 17 | 28.3 | 10 | 16.4 | 0.261 | 0.003 | ||
| T2 | 18 | 29.5 | 19 | 31.7 | 9 | 14.8 | 0.015 | 0.023 | ||
| T3 | 20 | 32.8 | 21 | 35.0 | 12 | 19.7 | 0.046 | 0.011 | ||
| T4 | 27 | 44.3 | 23 | 38.3 | 14 | 23.0 | <0.001 | <0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dellafiore, F.; Ghizzardi, G.; Vellone, E.; Magon, A.; Conte, G.; Baroni, I.; De Angeli, G.; Vangone, I.; Russo, S.; Stievano, A.; et al. A Single-Center, Randomized Controlled Trial to Test the Efficacy of Nurse-Led Motivational Interviewing for Enhancing Self-Care in Adults with Heart Failure. Healthcare 2023, 11, 773. https://doi.org/10.3390/healthcare11050773
Dellafiore F, Ghizzardi G, Vellone E, Magon A, Conte G, Baroni I, De Angeli G, Vangone I, Russo S, Stievano A, et al. A Single-Center, Randomized Controlled Trial to Test the Efficacy of Nurse-Led Motivational Interviewing for Enhancing Self-Care in Adults with Heart Failure. Healthcare. 2023; 11(5):773. https://doi.org/10.3390/healthcare11050773
Chicago/Turabian StyleDellafiore, Federica, Greta Ghizzardi, Ercole Vellone, Arianna Magon, Gianluca Conte, Irene Baroni, Giada De Angeli, Ida Vangone, Sara Russo, Alessandro Stievano, and et al. 2023. "A Single-Center, Randomized Controlled Trial to Test the Efficacy of Nurse-Led Motivational Interviewing for Enhancing Self-Care in Adults with Heart Failure" Healthcare 11, no. 5: 773. https://doi.org/10.3390/healthcare11050773
APA StyleDellafiore, F., Ghizzardi, G., Vellone, E., Magon, A., Conte, G., Baroni, I., De Angeli, G., Vangone, I., Russo, S., Stievano, A., Arrigoni, C., & Caruso, R. (2023). A Single-Center, Randomized Controlled Trial to Test the Efficacy of Nurse-Led Motivational Interviewing for Enhancing Self-Care in Adults with Heart Failure. Healthcare, 11(5), 773. https://doi.org/10.3390/healthcare11050773