
An Integrated Model for Evaluating the Sustainability of Gamified Mobile Health Apps: An Instrument Development and Validation

 ,
,
Abstract
:1. Introduction
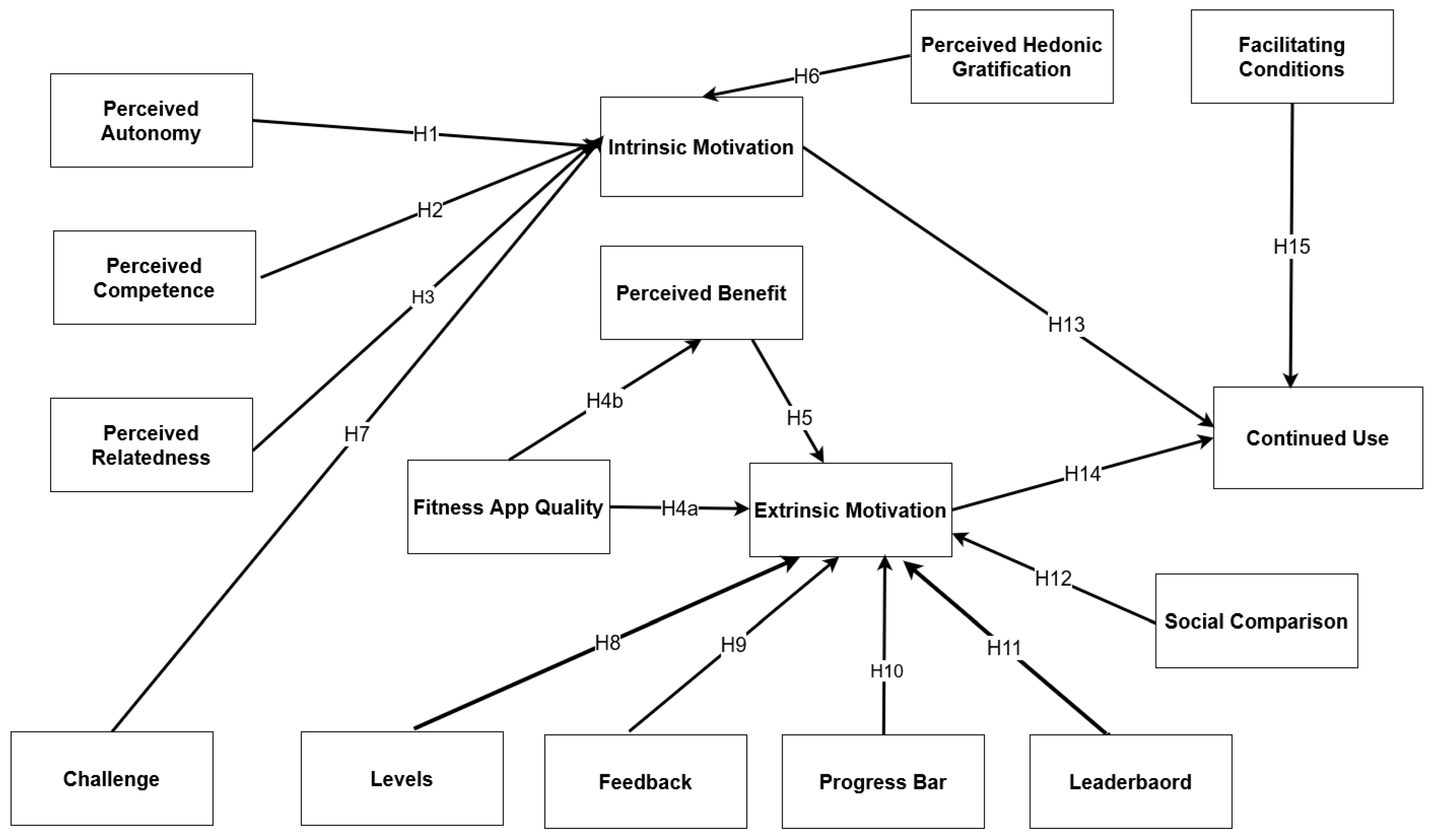
2. Research Model and Hypotheses Development
2.1. Self-Determination Theory
2.2. Social Comparison Theory
2.3. Perceived Autonomy (PA)
2.4. Perceived Competence (PC)
2.5. Perceived Relatedness (PR)
2.6. Fitness App Quality (FAQ)
2.7. Perceived Benefits (PB)
2.8. Perceived Hedonic Gratification (PHG)
2.9. Challenge (CH)
2.10. Levels (LV)
2.11. Feedback (FB)
2.12. Progress Bars (PGB)
2.13. Leaderboards (LB)
2.14. The Effect of Social Comparison (SC)
2.15. Intrinsic Motivation (IM)
2.16. Extrinsic Motivation (EM)
2.17. Facilitating Conditions (FC)
3. Instrument Development

{kind=link}
| Construct | Definition | Source |
|---|---|---|
| Facilitating Conditions (FC) | The conditions that facilitate the use of fitness apps for exercise. | [25] |
| Social Comparison (SC) | The degree to which users self-evaluate their exercise performance with others. | [25] |
| Perceived Autonomy (PA) | The need for a user to feel that they can choose their actions without pressure. | [39] |
| Perceived Competence (PC) | The need to successfully achieve desired results and avoid unwanted outcomes. | [39] |
| Perceived Relatedness (PR) | The need to feel connected with others and be valued by them. | [39] |
| Intrinsic Motivation (IM) | The degree to which an individual is driven to use a mHealth for internal rewards. | [39] |
| Perceived Benefits (PB) | The degree to which the user perceives the mHealth will enhance their performance. | [54] |
| Perceived Hedonic Gratification (PHG) | The degree to which the process of using mHealth is perceived to be pleasant. | [77] |
| Fitness App Quality (FAQ) | The degree to which the fitness app is easy to use, reliable, functional, and efficient. | [78] |
| Feedback (FB) | Personalized real-time updates about users’ performance. | [79] |
| Challenge (CH) | A task that requires considerable effort to solve. | [79] |
| Progress Bars (PGB) | A visual representation of users’ progress toward a goal. | [79] |
| Leaderboards (LB) | Visual display of users’ rankings based on their achievements. | [79] |
| Level (LV) | Indication of user’s progress over time. | [79] |
| Extrinsic Motivation (EM) | The degree to which an individual is driven to use a mHealth for external rewards. | [80] |
| Continued Use (CU) | The degree to which a user intends to continue using mHealth. | [81] |
Construct Conceptualization
4. Methodology
4.1. Study Design, Sampling Population, and Sample Size
4.2. Inclusion Criteria
4.3. Survey Instrument: Questionnaire
4.4. Data Collection
4.5. Data Analysis
4.6. Study Ethics
5. Results
5.1. Analysis
5.2. Face Validity
5.3. Content Validity
5.4. Reliability
6. Discussion
7. Conclusions
Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Constructs | Statements |
| Perceived Autonomy (PA) | PA1: My fitness apps usage is consistent with my preferences and interests. |
| PA2: I have several options when deciding how to use my fitness app. | |
| PA3: I feel free to decide what activities to do in my fitness app. | |
| PA4: I have the opportunity to make choices and set goals on my fitness app. | |
| Perceived Competence (PC) | PC1: I feel I have made a lot of progress in relation to the goal I want to achieve using my fitness app. |
| PC2: I think that I am good enough when I use my fitness app. | |
| PC3: I am satisfied with my performance when using my fitness app. | |
| PC4: I often feel that I am competent when using my fitness app. | |
| Perceived Relatedness (PR) | PR1: When I use my fitness app, I feel like other people care what I do. |
| PR2: I really like the people in my fitness app social network. | |
| PR3: The people in my fitness app social network are friendly towards me. | |
| Fitness App Quality (FAQ) | FAQ1: The functionality of my fitness app allows me to complete my activities. |
| FAQ2: Overall, my fitness app is highly reliable. | |
| FAQ3: My fitness app is efficient in allowing me to complete my exercise. | |
| Perceived Benefits (PB) | PB1: My fitness app helps improves the quality of my life. |
| PB2: My fitness app helps me enhance my physical fitness. | |
| PB3: My fitness app increases my productivity in doing exercises. | |
| Perceived Hedonic Gratification (PHG) | PHG1: I find using my fitness app to be enjoyable. |
| PHG2: I have fun interacting with my fitness app. | |
| PHG3: I find the experience of the exercise and the related fitness app use pleasant. | |
| PHG4: I find the experience of the exercise and the related fitness app use exciting. | |
| Perceived Competitive Climate (PCC) | PCC1: The amount of recognition I get within my social network in this fitness app depends on how my rank on leaderboard compares to others. |
| PCC2: My friends within this fitness app frequently compare their results of physical activity performance with mine. | |
| PCC3: Others within this fitness app frequently compare their results of physical activity performance with mine. | |
| Social Comparison (SC) | SC1: I often compare my performance with others. |
| SC2: The amount of recognition I get within my social network in my fitness app depends on how my rank on leaderboard compared to others. | |
| SC3: My friends within my fitness app network frequently compare their results of physical activity performance with mine. | |
| SC4: Other fitness app users frequently compare their results of physical activity performance with mine. | |
| Facilitating Conditions (FC) | FC1: My social network (e.g., family, friends, colleagues) encourages me to exercise more and keep fit. |
| FC2: My fitness apps are well-matched with other technologies that I use. | |
| FC3: My fitness apps promote physical activities. | |
| Intrinsic Motivation (IM) | IM1: I use my fitness app because it is fun. |
| IM2: I use my fitness app because it is interesting. | |
| IM3: I use my fitness app because I like it. | |
| Extrinsic Motivation (EM) | EM1: I use my fitness app because I will feel bad about myself when I do not carry out physical activities. |
| EM2: I feel under pressure from my friends/family to be physically active. | |
| EM3: I use my fitness app because other people say I should. | |
| EM4: I use my fitness app because I feel guilty when I do not exercise. | |
| Continued Use (CU) | CU1: I intend to continue using my fitness apps rather than discontinue their use |
| CU2: In my opinion, it is desirable to continue using fitness apps. | |
| CU3: I plan to continue using my fitness app. | |
| CU4: I think that continuously using my fitness app for exercise is a good idea. |
References
- Woessner, M.N.; Tacey, A.; Levinger-Limor, A.; Parker, A.G.; Levinger, P.; Levinger, I. The Evolution of Technology and Physical Inactivity: The Good, the Bad, and the Way Forward. Front. Public Health 2021, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Institute for Public Health (NIH); Ministry of Health Malaysia. Health and Morbidity Survey (NHMS) 2019: NCDs—Non-Communicable Diseases: Risk Factors and Other Health Problems; Ministry of Health Malaysia: Putrajaya, Malaysia, 2020; Volume 1, ISBN 9789671815922.
- Ferdowsy, F.; Rahi, K.S.A.; Jabiullah, M.I.; Habib, M.T. A Machine Learning Approach for Obesity Risk Prediction. Curr. Res. Behav. Sci. 2021, 2, 100053. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Brellenthin, A.G.; Lee, D.C.; Bennie, J.A.; Sui, X.; Blair, S.N. Resistance Exercise, Alone and in Combination with Aerobic Exercise, and Obesity in Dallas, Texas, US: A Prospective Cohort Study. PLoS Med. 2021, 18, e287. [Google Scholar] [CrossRef] [PubMed]
- Tate, E.B.; Spruijt-Metz, D.; O’Reilly, G.; Jordan-Marsh, M.; Gotsis, M.; Pentz, M.A.; Dunton, G.F. MHealth Approaches to Child Obesity Prevention: Successes, Unique Challenges, and next Directions. Transl. Behav. Med. 2013, 3, 406–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. MHealth: Use of Appropriate Digital Technologies for Public Health: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2018; Volume 10. [Google Scholar]
- Spring, B.; Champion, K.E.; Acabchuk, R.; Hennessy, E.A. Self-Regulatory Behaviour Change Techniques in Interventions to Promote Healthy Eating, Physical Activity, or Weight Loss: A Meta-Review. Health Psychol. Rev. 2021, 15, 508–539. [Google Scholar] [CrossRef]
- Albahri, A.S.; Zaidan, A.A.; Albahri, O.S.; Zaidan, B.B.; Alsalem, M.A. Real-Time Fault-Tolerant MHealth System: Comprehensive Review of Healthcare Services, Opens Issues, Challenges and Methodological Aspects. J. Med. Syst. 2018, 42, 137. [Google Scholar] [CrossRef]
- Lunney, A.; Cunningham, N.R.; Eastin, M.S. Wearable Fitness Technology: A Structural Investigation into Acceptance and Perceived Fitness Outcomes. Comput. Hum. Behav. 2016, 65, 114–120. [Google Scholar] [CrossRef]
- Bardus, M.; Awada, N.; Ghandour, L.A.; Fares, E.J.; Gherbal, T.; Al-Zanati, T.; Stoyanov, S.R. The Arabic Version of the Mobile App Rating Scale: Development and Validation Study. JMIR Mhealth Uhealth 2020, 8, e16956. [Google Scholar] [CrossRef]
- Wasil, A.R.; Gillespie, S.; Schell, T.; Lorenzo-Luaces, L.; DeRubeis, R.J. Estimating the Real-World Usage of Mobile Apps for Mental Health: Development and Application of Two Novel Metrics. World Psychiatry 2021, 20, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C. MHealth Market Revenue Worldwide 2017–2025; Statista: Hamburg, Germany, 2021. [Google Scholar]
- Bhuvan, K.C.; Alrasheedy, A.A.; Goh, B.H.; Blebil, A.; Bangash, N.S.A.; Ibrahim, M.I.M.; Rehman, I.U. The Types and Pattern of Use of Mobile Health Applications among the General Population: A Cross-Sectional Study from Selangor, Malaysia. Patient Prefer. Adherence 2021, 15, 1755–1762. [Google Scholar] [CrossRef]
- Murnane, E.L.; Huffaker, D.; Kossinets, G. Mobile Health Apps: Adoption, Adherence, and Abandonment. In Proceedings of the UbiComp ISWC 2015—Proceedings of the 2015 ACM International Joint Conference on Pervasive Ubiquitous Computing and Proceedings of the 2015 ACM International Symposium Wearable Computers, Osaka, Japan, 7–11 September 2015; pp. 261–264. [Google Scholar] [CrossRef]
- Marston, H.R.; Hall, A.K. Gamification: Applications for Health Promotion and Health Information Technology Engagement. In Handbook of Research on Holistic Perspectives Gamification for Clinical Practice; Igi Global: Hershey, PA, USA, 2015; pp. 78–104. [Google Scholar] [CrossRef]
- Deterding, S.; O’Hara, K.; Sicart, M.; Dixon, D.; Nacke, L. Gamification: Using Game Design Elements in Non-Gaming Contexts. In Proceedings of the CHI’11 Extended Abstracts on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 2425–2428. [Google Scholar] [CrossRef]
- Wu, X.; Santana, S. Impact of Intrinsic and Extrinsic Gaming Elements on Online Purchase Intention. Front. Psychol. 2022, 13, 885619. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.; Edney, S.; Maher, C. Engagement, Compliance and Retention with a Gamified Online Social Networking Physical Activity Intervention. Transl. Behav. Med. 2017, 7, 702–708. [Google Scholar] [CrossRef] [Green Version]
- Woldaregay, A.Z.; Issom, D.Z.; Henriksen, A.; Marttila, H.; Mikalsen, M.; Pfuhl, G.; Sato, K.; Lovis, C.; Hartvigsen, G. Motivational Factors for User Engagement with MHealth Apps. Stud. Health Technol. Inform. 2018, 249, 151–157. [Google Scholar] [CrossRef]
- Cho, J. The Impact of Post-Adoption Beliefs on the Continued Use of Health Apps. Int. J. Med. Inform. 2016, 87, 75–83. [Google Scholar] [CrossRef]
- Müller-Török, R.; Prosser, A. The Corona Warning App of the German Federal Government–How Perceived Data Protection Issues Hindered Any Effectiveness. Smart Cities Reg. Dev. J. 2021, 5, 23–31. [Google Scholar]
- Landers, R.N.; Bauer, K.N.; Callan, R.C. Gamification of Task Performance with Leaderboards: A Goal Setting Experiment. Comput. Hum. Behav. 2017, 71, 508–515. [Google Scholar] [CrossRef]
- Wu, Y.; Kankanhalli, A.; Huang, K.W. Gamification in Fitness Apps: How Do Leaderboards Influence Exercise? In Proceedings of the 2015 International Conference of Information Systems: Exploring the Information Frontier ICIS 2015, Fort Worth, TX, USA, 13–16 December 2015; pp. 1–12. [Google Scholar]
- Seaborn, K.; Fels, D.I. Gamification in Theory and Action: A Survey. Int. J. Hum. Comput. Stud. 2015, 74, 14–31. [Google Scholar] [CrossRef]
- Mazeas, A.; Duclos, M.; Pereira, B.; Chalabaev, A. Evaluating the Effectiveness of Gamification on Physical Activity: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e26779. [Google Scholar] [CrossRef]
- Galli, F.; Chirico, A.; Mallia, L.; Alivernini, F.; Manganelli, S.; Zelli, A.; Hagger, M.S.; Lucidi, F. Identifying Determinants of Neuro-Enchancement Substance Use in Students Application of an Integrated Theoretical Model. Eur. J. Health Psychol. 2022, 30, 29–39. [Google Scholar] [CrossRef]
- Hagger, M.S.; Hamilton, K. Changing Behavior Using Integrated Theories. In Handbook of Behavior Change; Cambridge University Press: Cambridge, UK, 2020; pp. 208–224. [Google Scholar] [CrossRef]
- Hagger, M.S. Theoretical Integration in Health Psychology: Unifying Ideas and Complementary Explanations. Br. J. Health Psychol. 2009, 14, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory an Introduction and Overview; Guilford Press: New York, NY, USA, 2017; ISBN 9781462538966. [Google Scholar]
- Festinger, L. A Theory of Social Comparison Process. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Hagger, M.S.; Weed, M. DEBATE: Do Interventions Based on Behavioral Theory Work in the Real World? Int. J. Behav. Nutr. Phys. Act. 2019, 16, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, S.; Ma, W.; Kanthawala, S.; Peng, W. Keep Using My Health Apps: Discover Users’ Perception of Health and Fitness Apps with the UTAUT2 Model. Telemed. E-Health 2015, 21, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Zhang, R.; Zhu, X.; Liu, M. Factors Influencing Continued Usage Behavior on Mobile Health Applications. Healthcare 2022, 10, 208. [Google Scholar] [CrossRef]
- Yang, Y.; Asaad, Y.; Dwivedi, Y. Examining the Impact of Gamification on Intention of Engagement and Brand Attitude in the Marketing Context. Comput. Hum. Behav. 2017, 73, 459–469. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef]
- Ryan, R.M.; Rigby, C.S.; Przybylski, A. The Motivational Pull of Video Games: A Self-Determination Theory Approach. Motiv. Emot. 2006, 30, 347–363. [Google Scholar] [CrossRef]
- Bitrián, P.; Buil, I.; Catalán, S. Gamification in Sport Apps: The Determinants of Users’ Motivation. Eur. J. Manag. Bus. Econ. 2020, 29, 365–381. [Google Scholar] [CrossRef]
- Huschens, M.; Rothlauf, F.; Rothe, R. On the Role of Social Comparison Processes in Gamified Work Situations. In Proceedings of the Annual Hawaii International Conference on System Science Grand Wailea, Maui, HI, USA, 8–11 January 2019; pp. 1446–1455. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Williams, G.C.; Patrick, H.; Deci, E.L. Self-Determination Theory and Physical Activity: The Dynamics of Motivation in Development and Wellness. Hell. J. Psychol. 2009, 6, 107–124. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-Regulation and the Problem of Human Autonomy: Does Psychology Need Choice, Self-Determination, and Will? J. Pers. 2006, 74, 1557–1586. [Google Scholar] [CrossRef] [PubMed]
- Alexiou, A.; Schippers, M. Digital Game Elements, User Experience and Learning: A Conceptual Framework Content Courtesy of Springer Nature, Terms of Use Apply. Rights Reserved. Content Courtesy of Springer Nature, Terms of Use Apply. Rights Reserved. Educ. Inf. Technol. 2018, 23, 2545–2567. [Google Scholar] [CrossRef] [Green Version]
- Edmunds, J.; Ntoumanis, N.; Duda, J.L. A Test of Self-Determination Theory in the Exercise Domain. J. Appl. Soc. Psychol. 2006, 36, 2240–2265. [Google Scholar] [CrossRef]
- Ryan, R.M.; Patrick, H.; Deci, E.L.; Williams, G.C.; Ryan, R.M.; Patrick, H.; Deci, E.L.; Williams, G.C. Facilitating Health Behaviour Change and Its Maintenance: Interventions Based on Self-Determination Theory. Eur. Health Psychol. 2008, 10, 2–6. [Google Scholar]
- Markland, D.A. Self-Determination Moderates the Effects of Perceived Competence on Intrinsic Motivation in an Exercise Setting. J. Sport Exerc. Psychol. 1999, 21, 351–361. [Google Scholar] [CrossRef]
- Karlsson, V.; Danielsson, L. Motivators for Patients with Schizophrenia Spectrum Disorders to Start and Maintain Exercising: A Qualitative Interview Study. Eur. J. Physiother. 2022, 24, 30–38. [Google Scholar] [CrossRef]
- Khan, I.U.; Hameed, Z.; Yu, Y.; Islam, T.; Sheikh, Z.; Khan, S.U. Predicting the Acceptance of MOOCs in a Developing Country: Application of Task-Technology Fit Model, Social Motivation, and Self-Determination Theory. Telemat. Inform. 2018, 35, 964–978. [Google Scholar] [CrossRef]
- Tsai, T.H.; Chang, Y.S.; Chang, H.T.; Lin, Y.W. Running on a Social Exercise Platform: Applying Self-Determination Theory to Increase Motivation to Participate in a Sporting Event. Comput. Hum. Behav. 2021, 114, 106523. [Google Scholar] [CrossRef]
- Alaiad, A.; Alsharo, M.; Alnsour, Y. The Determinants of M-Health Adoption in Developing Countries: An Empirical Investigation. Appl. Clin. Inform. 2019, 10, 820–840. [Google Scholar] [CrossRef]
- Palos-Sanchez, P.; Saura, J.R.; Martin-Velicia, F. A Study of the Effects of Programmatic Advertising on Users’ Concerns about Privacy Overtime. J. Bus. Res. 2019, 96, 61–72. [Google Scholar] [CrossRef]
- Leung, Y. Encyclopedia of Behavioral Medicine; Springer: Cham, Switzerland, 2013; ISBN 9781441910059. [Google Scholar]
- McArthur, L.H.; Riggs, A.; Uribe, F.; Spaulding, T.J. Health Belief Model Offers Opportunities for Designing Weight Management Interventions for College Students. J. Nutr. Educ. Behav. 2018, 50, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Vinnikova, A.; Lu, L.; Xu, J. Understanding and Predicting the Adoption of Fitness Mobile Apps: Evidence from China. Health Commun. 2021, 36, 950–961. [Google Scholar] [CrossRef]
- Putri, M.F.; Hidayanto, A.N.; Negara, E.S.; Abidin, Z.; Utari, P.; Budi, N.F.A. Ranking of Game Mechanics for Gamification in Mobile Payment Using AHP-TOPSIS: Uses and Gratification Perspective. In Proceedings of the ICICOS 2019—3rd International Conference on Informatics and Computational Sciences: Accelerating Informatics and Computational Research for Smarter Society in The Era of Industry 4.0, Proceedings, Semarang, Indonesia, 29–30 October 2019. [Google Scholar]
- Costa, C.; Alvelos, H.; Teixeira, L. The Use of Moodle E-Learning Platform: A Study in a Portuguese University. Procedia Technol. 2012, 5, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Di Domenico, S.I.; Ryan, R.M. The Emerging Neuroscience of Intrinsic Motivation: A New Frontier in Self-Determination Research. Front. Hum. Neurosci. 2017, 11, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, A.S.; Ali, N.; Dhillon, J.S.; Alkawsi, G.; Baashar, Y. User Engagement and Abandonment of MHealth: A Cross-Sectional Survey. Healthcare 2022, 10, 221. [Google Scholar] [CrossRef]
- Lu, H.P.; Ho, H.C. Exploring the Impact of Gamification on Users’ Engagement for Sustainable Development: A Case Study in Brand Applications. Sustainability 2020, 12, 4169. [Google Scholar] [CrossRef]
- Werbach, K.; Hunter, D. For the Win: How Game Thinking Can Revolutionize Your Business; Wharton Digital Press: Philadelphia, PA, USA, 2012; p. 146. [Google Scholar]
- Zichermann, G.; Cunningham, C. Gamification by Design: Implementing Game Mechanics in Web and Mobile Apps; O’Reilly Media: Sebastopol, CA, USA, 2011; ISBN 9781449397678. [Google Scholar]
- Xi, N.; Hamari, J. The Relationship between Gamification, Brand Engagement and Brand Equity. In Proceedings of the 52nd Hawaii International Conferenceon System Sciences, Grand Wailea, HI, USA, 8–11 January 2019; pp. 812–821. [Google Scholar] [CrossRef] [Green Version]
- Kappen, D.L.; Mirza-Babaei, P.; Nacke, L.E. Gamification through the Application of Motivational Affordances for Physical Activity Technology. In Proceedings of the Annual Symposium on Computer-Human Interaction in Play, Amsterdam, The Netherlands, 15–18 October 2017; pp. 5–18. [Google Scholar] [CrossRef]
- Keepers, M.; Nesbit, I.; Romero, D.; Wuest, T. Current State of Research & Outlook of Gamification for Manufacturing. J. Manuf. Syst. 2022, 64, 303–315. [Google Scholar] [CrossRef]
- Holmes, B.J.; Schellenberg, M.; Schell, K.; Scarrow, G. How Funding Agencies Can Support Research Use in Healthcare: An Online Province-Wide Survey to Determine Knowledge Translation Training Needs. Implement. Sci. 2014, 9, 71. [Google Scholar] [CrossRef] [Green Version]
- Mekler, E.D.; Brühlmann, F.; Opwis, K.; Tuch, A.N. Do Points, Levels and Leaderboards Harm Intrinsic Motivation? An Empirical Analysis of Common Gamification Elements. In Proceedings of the First International Conference on Gameful Design, Research, and Applications, Toronto, ON, Canada, 2–4 October 2013; pp. 66–73. [Google Scholar] [CrossRef]
- Mazarakis, A.; Bräuer, P. Gamification of an Open Access Quiz with Badges and Progress Bars: An Experimental Study with Scientists. In Proceedings of the GamiFIN Conference 2020, Levi, Finland, 1–3 April 2020; pp. 62–71. [Google Scholar]
- Jia, Y.; Liu, Y.; Yu, X.; Voida, S. Designing Leaderboards for Gamification: Perceived Differences Based on User Ranking, Application Domain, and Personality Traits. In Proceedings of the 2017 CHI Conference on Human Factors in Computing System, Denver, CO, USA, 6–11 May 2017; pp. 1949–1960. [Google Scholar] [CrossRef] [Green Version]
- Altmeyer, M.; Lessel, P.; Sander, T.; Krüger, A. Extending a Gamified Mobile App with a Public Display to Encourage Walking. In Proceedings of the ACM International Conference Proceeding Series, Tempere, Finland, 10–11 October 2018; pp. 20–29. [Google Scholar] [CrossRef]
- Ingledew, D.K.; Markland, D.; Sheppard, K.E. Personality and Self-Determination of Exercise Behaviour. Pers. Individ. Dif. 2004, 36, 1921–1932. [Google Scholar] [CrossRef]
- Sweet, S.N.; Fortier, M.S.; Strachan, S.M.; Blanchard, C.M.; Boulay, P. Testing a Longitudinal Integrated Self-Efficacy and Self-Determination Theory Model for Physical Activity Post-Cardiac Rehabilitation. Health Psychol. Res. 2014, 2, 1008. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Fan, L.; Zheng, X.; Wang, W.; Liang, J.; An, K.; Ju, M.; Lei, J. The Impact of Gamification-Induced Users’ Feelings on the Continued Use of Mhealth Apps: A Structural Equation Model with the Self-Determination Theory Approach. J. Med. Internet Res. 2021, 23, e24546. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, Physical Activity, and Self-Determination Theory: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, A.; Limpo, T.; Castro, S.L. Acceptance of Mobile Health Applications: Examining Key Determinants and Moderators. Front. Psychol. 2019, 10, 2791. [Google Scholar] [CrossRef] [PubMed]
- Humpel, N.; Owen, N.; Leslie, E. Environmental Factors Associated with Adults’ Participation in Physical Activity. A Review. Am. J. Prev. Med. 2002, 22, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Shi, H.; Shen, M.; Ni, Y.; Zhang, X.; Pang, Y.; Yu, T.; Lian, X.; Yu, T.; Yang, X.; et al. The Effects of MHealth-Based Gamification Interventions on Participation in Physical Activity: Systematic Review. JMIR Mhealth Uhealth 2022, 10, e27794. [Google Scholar] [CrossRef]
- Gan, C.; Li, H. Understanding the Effects of Gratifications on the Continuance Intention to Use WeChat in China: A Perspective on Uses and Gratifications. Comput. Hum. Behav. 2018, 78, 306–315. [Google Scholar] [CrossRef]
- Yakubu, M.N.; Dasuki, S.I.; Abubakar, A.M.; Kah, M.M.O. Determinants of Learning Management Systems Adoption in Nigeria: A Hybrid SEM and Artificial Neural Network Approach. Educ. Inf. Technol. 2020, 25, 3515–3539. [Google Scholar] [CrossRef]
- Balci, S.; Secaur, J.M.; Morris, B.J. Comparing the Effectiveness of Badges and Leaderboards on Academic Performance and Motivation of Students in Fully versus Partially Gamified Online Physics Classes; Springer: New York, NY, USA, 2022; ISBN 1063902210983. [Google Scholar]
- Moustaka, F.C.; Vlachopoulos, S.P.; Vazou, S.; Kaperoni, M.; Markland, D.A. Initial Validity Evidence for the Behavioral Regulation in Exercise Questionnaire-2 among Greek Exercise Participants. Eur. J. Psychol. Assess. 2010, 26, 269–276. [Google Scholar] [CrossRef]
- Koivisto, J.; Hamari, J. Demographic Differences in Perceived Benefits from Gamification. Comput. Hum. Behav. 2014, 35, 179–188. [Google Scholar] [CrossRef]
- MacKenzie, S.B.; Podsakoff, P.M.; Podsakoff, N.P. Construct Measurement and Validation Procedures in MIS and Behavioral Research: Integrating New and Existing Techniques. MIS Q. Manag. Inf. Syst. 2011, 35, 293–334. [Google Scholar] [CrossRef]
- Straub, D.; Gefen, D. Validation Guidelines for IS Positivist Research. Commun. Assoc. Inf. Syst. 2004, 13, 24. [Google Scholar] [CrossRef]
- Alshammari, T.; Messom, C.; Cheung, Y. M-Government Continuance Intentions: An Instrument Development and Validation. Inf. Technol. Dev. 2022, 28, 189–209. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the Sample Size for a Pilot Randomised Trial to Minimise the Overall Trial Sample Size for the External Pilot and Main Trial for a Continuous Outcome Variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esmaeilzadeh, P. The Influence of Gamification and Information Technology Identity on Postadoption Behaviors of Health and Fitness App Users: Empirical Study in the United States. JMIR Serious Games 2021, 9, e28282. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an Acceptable Indicator of Content Validity? Appraisal and Recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Davis, L.L. Instrument Review: Getting the Most from a Panel of Experts. Appl. Nurs. Res. 1992, 5, 194–197. [Google Scholar] [CrossRef]
- Dean, E.; Caspar, R.; McAvinchey, G.; Reed, L.; Quiroz, R. Developing a Low-Cost Technique for Parallel Cross-Cultural Instrument Development: The Question Appraisal System (QAS-04). Int. J. Soc. Res. Methodol. 2007, 10, 227–241. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Hopkins, L.; Kuppelwieser, V.G. Partial Least Squares Structural Equation Modeling (PLS-SEM): An Emerging Tool in Business Research. Eur. Bus. Rev. 2014, 26, 106–121. [Google Scholar] [CrossRef]
- Arafat, S.; Chowdhury, H.; Qusar, M.; Hafez, M. Cross Cultural Adaptation and Psychometric Validation of Research Instruments: A Methodological Review. J. Behav. Health 2016, 5, 129. [Google Scholar] [CrossRef] [Green Version]
- Raykov, T. Alpha If Item Deleted: A Note on Loss of Criterion Validity in Scale Development If Maximizing Coefficient Alpha. Br. J. Math. Stat. Psychol. 2008, 61, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Che Md Ghazali, N.H. A Reliability and Validity of an Instrument to Evaluate the School-Based Assessment System: A Pilot Study. Int. J. Eval. Res. Educ. 2016, 5, 148–157. [Google Scholar] [CrossRef]
- Chiu, W.; Cho, H.; Chi, C.G. Consumers’ Continuance Intention to Use Fitness and Health Apps: An Integration of the Expectation–Confirmation Model and Investment Model. Inf. Technol. People 2020, 34, 978–998. [Google Scholar] [CrossRef]
- Taherdoost, H. Validity and Reliability of the Research Instrument; How to Test the Validation of a Questionnaire/Survey in a Research. SSRN Electron. J. 2018, 5, 28–36. [Google Scholar] [CrossRef]
- Yoo, C.; Kwon, S.; Na, H.; Chang, B. Factors Affecting the Adoption of Gamified Smart Tourism Applications: An Integrative Approach. Sustainability 2017, 9, 2162. [Google Scholar] [CrossRef] [Green Version]
- Sailer, M.; Hense, J.; Mandl, H.; Klevers, M. Fostering Development of Work Competencies and Motivation via Gamification. In Competence-Based Vocational and Professional Education; Springer International Publishing: New York, NY, USA, 2017; pp. 795–818. ISBN 9783319417134. [Google Scholar]
- Wu, B.; Chen, X. Continuance Intention to Use MOOCs: Integrating the Technology Acceptance Model (TAM) and Task Technology Fit (TTF) Model. Comput. Hum. Behav. 2017, 67, 221–232. [Google Scholar] [CrossRef]
- Wong, D.; Liu, H.; Meng-Lewis, Y.; Sun, Y.; Zhang, Y. Gamified Money: Exploring the Effectiveness of Gamification in Mobile Payment Adoption among the Silver Generation in China. Inf. Technol. People 2021, 35, 281–315. [Google Scholar] [CrossRef]
- Jahn, K.; Kordyaka, B.; Machulska, A.; Eiler, T.J.; Gruenewald, A.; Klucken, T.; Brueck, R.; Gethmann, C.F.; Niehaves, B. Individualized Gamification Elements: The Impact of Avatar and Feedback Design on Reuse Intention. Comput. Hum. Behav. 2021, 119, 106702. [Google Scholar] [CrossRef]
- Choi-Ki Wong, C.; Chi-Wai Kwok, R. The Effect of Gamified Mhealth App on Exercise Motivation and Physical Activity. In Proceedings of the Pacific Asia Conference on Information Systems (PACIS), Chiayi, Taiwan, 27 June–1 July 2016; p. 389. [Google Scholar]
- van Teijlingen, E.; Hundley, V. The Importance of Pilot Studies. Nurs. Stand. 2002, 16, 33–36. [Google Scholar] [CrossRef] [Green Version]

| Frequency | Percentage | |
|---|---|---|
| Gender | ||
| Male | 20 | 42 |
| Female | 28 | 58 |
| Age (Mean = 26.9) | ||
| 18–25 | 28 | 58 |
| 26–35 | 12 | 25 |
| 36–45 | 8 | 17 |
| Educational Level | ||
| High School | 5 | 10.5 |
| Diploma | 5 | 10.5 |
| Bachelors’ Degree | 24 | 50 |
| Masters’ Degree | 12 | 25 |
| PhD Degree | 2 | 4 |
| Monthly Household Income | ||
| Less than 2000 | 20 | 42 |
| 2999–4999 | 9 | 18.5 |
| 5000–7999 | 8 | 17 |
| 8000–9999 | 2 | 4 |
| Above 10,000 | 9 | 18.5 |
| Frequently Used Apps | ||
| MyFitnessPal | 7 | 25 |
| Strava | 6 | 21.4 |
| Samsung Health | 5 | 17.9 |
| RunKeeper | 5 | 17.9 |
| HealthifyMe | 5 | 17.9 |
| Construct | Item | No. of Items | Cronbach’s Alpha | Composite Reliability |
|---|---|---|---|---|
| Perceived Autonomy (PA) | PA1, PA2, PA3, PA4 | 4 | 0.929 | 0.949 |
| Perceived Competence (PC) | PC1, PC2, PC3, PC4 | 4 | 0.931 | 0.951 |
| Perceived Relatedness (PR) | PR1, PR2, PR4 (PR3 deleted) | 3 | 0.919 | 0.943 |
| Fitness App Quality (FAQ) | FAQ1, FAQ2, FAQ3 | 3 | 0.920 | 0.950 |
| Perceived Benefits (PB) | PB1, PB2, PB3 | 3 | 0.950 | 0.968 |
| Perceived Hedonic Gratification (PHG) | PHG1, PHG2, PHG3 | 4 | 0.938 | 0.955 |
| Leaderboard (LB) | LB1, LB2, LB3, LB4 | 4 | 0.884 | 0.916 |
| Levels (LV) | LV1, LV2, LV3, LV4 | 4 | 0. 868 | 0.908 |
| Feedback (FB) | FB1, FB2, FB3, FB4 | 4 | 0.849 | 0.906 |
| Progress Bar (PGB) | PGB1, PGB2, PGB3, PGB4 | 4 | 0.950 | 0.968 |
| Challenge (CH) | CH1, CH2, CH3, CH4 | 4 | 0.922 | 0.945 |
| Social Comparison (SC) | SC1, SC2, SC3, SC4 | 4 | 0.939 | 0.956 |
| Facilitating Condition (FC) | FC1, FC2, FC3 | 3 | 0.924 | 0.952 |
| Intrinsic Motivation (IM) | IM1, IM2, IM3 | 3 | 0.924 | 0.952 |
| Extrinsic Motivation (EM) | EM1, EM2, EM3, EM4 | 4 | 0.893 | 0.925 |
| Continued Use (CU) | CU1, CU2, CU3 | 4 | 0.949 | 0.963 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mustafa, A.S.; Ali, N.; Dhillon, J.S.; Sedera, D. An Integrated Model for Evaluating the Sustainability of Gamified Mobile Health Apps: An Instrument Development and Validation. Healthcare 2023, 11, 1051. https://doi.org/10.3390/healthcare11071051
Mustafa AS, Ali N, Dhillon JS, Sedera D. An Integrated Model for Evaluating the Sustainability of Gamified Mobile Health Apps: An Instrument Development and Validation. Healthcare. 2023; 11(7):1051. https://doi.org/10.3390/healthcare11071051
Chicago/Turabian StyleMustafa, Abdulsalam Salihu, Nor’ashikin Ali, Jaspaljeet Singh Dhillon, and Darshana Sedera. 2023. "An Integrated Model for Evaluating the Sustainability of Gamified Mobile Health Apps: An Instrument Development and Validation" Healthcare 11, no. 7: 1051. https://doi.org/10.3390/healthcare11071051
APA StyleMustafa, A. S., Ali, N., Dhillon, J. S., & Sedera, D. (2023). An Integrated Model for Evaluating the Sustainability of Gamified Mobile Health Apps: An Instrument Development and Validation. Healthcare, 11(7), 1051. https://doi.org/10.3390/healthcare11071051