

Improving Well-Being and Fostering Health-Oriented Leadership among Leaders in Small and Medium-Sized Enterprises (SMEs): A Systematic Review

 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Work-Related Stress and Strain and Their Consequences
1.2. The Significant Role of Small and Medium-Sized Enterprises
1.3. Small and Medium-Sized Enterprises: Challenges and Opportunities
1.4. Psychological Demands among SME Leaders
1.5. Addressing Mental Health of SME Leaders
1.6. Research Aim
2. Methods
2.1. General Methodology and Selection Criteria
PICO Criteria
2.2. Data Sources and Search Strategy
2.3. Screening Procedure and Data Extraction
2.4. Quality Assessment
3. Results
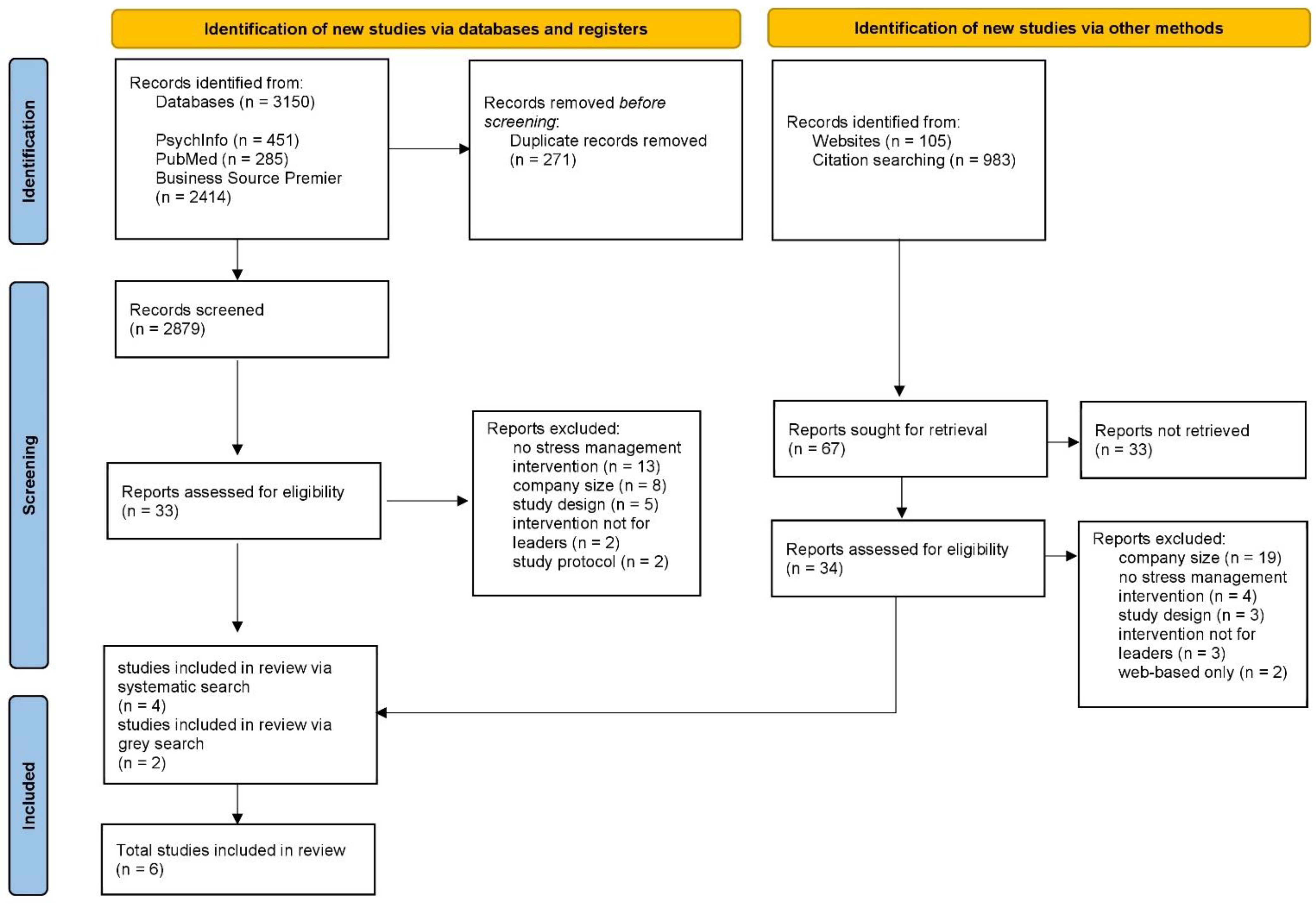
3.1. Study Selection
3.2. Study Characteristics
3.3. Detailed Description of Included Study Results
- Leadership- and well-being-oriented interventions
- Cognitive behavioural theory (CBT)-based and goal-oriented interventions
- Individualised coaching-based interventions
3.3.1. Well-Being- and Leadership-Oriented Interventions
3.3.2. CBT-Based and Goal-Oriented Interventions
3.3.3. Individualised Coaching-Based Intervention
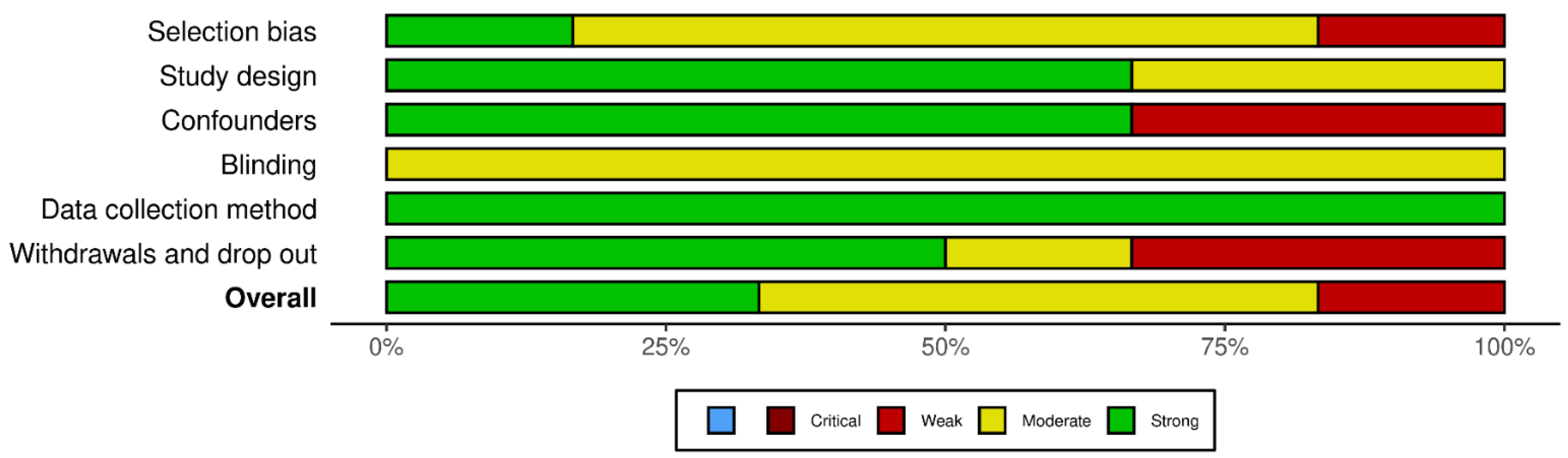
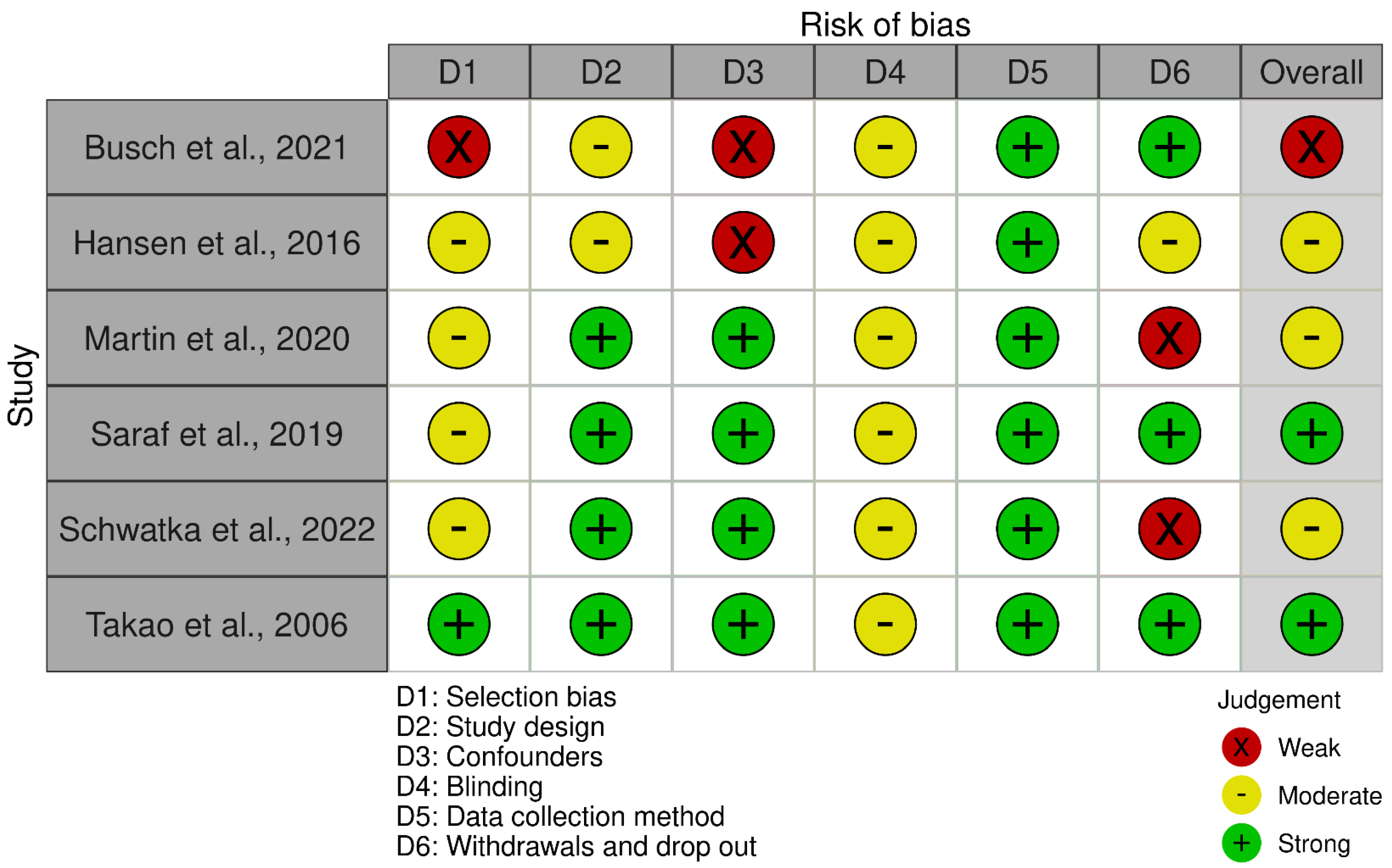
3.4. Risk of Bias in the Included Studies
4. Discussion
Strengths and Limitations
5. Conclusions
- Definition: As mentioned above, the definition of SMEs varies internationally and between organisations, which often makes it difficult to correctly identify types of businesses and their specific challenges [14].
- Limited research: There is a lack of research specifically focused on the mental health of SME leaders. Most studies on this topic tend to be limited in scope or are conducted on larger organisations, making it difficult to draw generalisations or make informed recommendations for SMEs [72].
- Sample size and representativeness: SMEs are a diverse group, and their leaders may have unique experiences and needs. However, the small sample sizes in most studies and the lack of diversity in the samples can make it difficult to generalise findings to the wider population of SME leaders.
- Access and recruitment: SMEs are often more difficult to access for research purposes than larger organisations as they may not have dedicated HR departments or may be more reluctant to participate in research. This can make it difficult to recruit participants, which may further limit the generalisability of the findings [32].
- Self-reporting bias: Mental health research often relies on self-reported data, which can be subject to biases such as social desirability or recall bias. This can make it difficult to accurately assess the mental health of SME leaders, particularly if they are reluctant to disclose mental health issues [73].
- Lack of resources and support: SMEs may have limited resources to devote to mental health initiatives, which can make it difficult to support the mental health of leaders and employees. In addition, SME leaders may feel a greater sense of responsibility for the success of their business, which can create additional stress and make it more difficult to prioritise their own mental health [32].
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Pech, E.; Rose, U.; Freude, G.; Pech, E.; Rose, U.; Freude, G. Zum Verständnis mentaler Gesundheit—Eine erweiterte Perspektive. Zent. Arb. Arb. Ergon. 2010, 60, 234–243. [Google Scholar] [CrossRef]
- Siegrist, J.; Wahrendorf, M. Work Stress and Health in a Globalized Economy; Springer Science and Business Media LLC: Dordrecht, The Netherlands, 2016. [Google Scholar] [CrossRef]
- Siegrist, J. Effort-Reward Imbalance at Work: Theory, Measurement and Evidence; Department of Medical Sociology, University Düsseldorf: Düsseldorf, Germany, 2012; Volume 19. [Google Scholar]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions at work. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Jarczok, M.; Mauss, D.; Koenig, J.; Li, J.; Herr, R.M.; Thayer, J.F. Autonomic nervous system activity and workplace stressors—A systematic review. Neurosci. Biobehav. Rev. 2013, 37, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Mulfinger, N.; Contributors of the SEEGEN Consortium; Sander, A.; Stuber, F.; Brinster, R.; Junne, F.; Limprecht, R.; Jarczok, M.N.; Seifried-Dübon, T.; Rieger, M.A.; et al. Cluster-randomised trial evaluating a complex intervention to improve mental health and well-being of employees working in hospital–A protocol for the SEEGEN trial. BMC Public Health 2019, 19, 1694. [Google Scholar] [CrossRef]
- Erschens, R.; Seifried-Dübon, T.; Stuber, F.; Rieger, M.A.; Zipfel, S.; Nikendei, C.; Genrich, M.; Angerer, P.; Maatouk, I.; Gündel, H.; et al. The association of perceived leadership style and subjective well-being of employees in a tertiary hospital in Germany. PLoS ONE 2022, 17, e0278597. [Google Scholar] [CrossRef]
- European Comission. SME definitionEuropean Comission. 2022. Available online: https://ec.europa.eu/growth/smes/sme-definition_en (accessed on 23 May 2023).
- Statistisches Bundesamt. 2023. Available online: https://www.destatis.de/DE/Themen/Branchen-Unternehmen/Unternehmen/Kleine-Unternehmen-Mittlere-Unternehmen/_inhalt.html (accessed on 23 May 2023).
- OECD. Financing SMEs and Entrepreneurs. Available online: https://www.oecd-ilibrary.org/docserver/e9073a0f-en.pdf?expires=1684859786&id=id&accname=ocid43023317a&checksum=213465B72F4E74BEBC7C44BBD4361196 (accessed on 23 May 2023).
- Office of the Untited States Trade Representative. Available online: https://ustr.gov/trade-agreements/free-trade-agreements/transatlantic-trade-and-investment-partnership-t-tip/t-tip-12 (accessed on 23 May 2023).
- O’Driscoll, M.P.; Brough, P.; Haar, J. The work-family nexus and small to medium sized enterprises: Implications for worker well-being. Occup. Health Saf. Small Medium Sized Enterp. 2011, 106–128. [Google Scholar] [CrossRef]
- Gonzales, E.; Hommes, M.; Mirmulstein, M.L. MSME Country Indicators 2014. Available online: https://smefinanceforum.org/sites/default/files/description%20note.pdf (accessed on 23 May 2023).
- Schreibauer, E.C.; Hippler, M.; Burgess, S.; Rieger, M.A.; Rind, E. Work-Related Psychosocial Stress in Small and Medium-Sized Enterprises: An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7446. [Google Scholar] [CrossRef]
- Dannheim, I.; Buyken, A.E.; Kroke, A. Work-related stressors and coping behaviors among leaders in small and medium-sized IT and technological services enterprises. BMC Public Health 2023, 23, 700. [Google Scholar] [CrossRef]
- Burns, W.B. Family-Owned and Non-Family-Owned Business: Stress and Coping; Iowa State University: Ames, IA, USA, 2000; Available online: https://lib.dr.iastate.edu/rtd/12313 (accessed on 23 May 2023).
- Visentin, D.C.; Cleary, M.; Minutillo, S. Small business ownership and mental health. Issues Ment. Health Nurs. 2020, 41, 460–463. [Google Scholar] [CrossRef]
- Wagner, A.; Werners, B.; Pieper, C.; Eilerts, A.-L.; Seifried-Dübon, T.; Grot, M.; Junne, F.; Weltermann, B.M.; Rieger, M.A.; Rind, E. Exploring Transfer Potentials of the IMPROVE job Intervention for Strengthening Workplace Health Management in Micro-, Small-, and Medium-Sized Enterprises in Germany: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 4067. [Google Scholar] [CrossRef]
- Encrenaz, G.; Laberon, S.; Lagabrielle, C.; Debruyne, G.; Pouyaud, J.; Rascle, N. Psychosocial risks in small enterprises: The mediating role of perceived working conditions in the relationship between enterprise size and workers’ anxious or depressive episodes. Int. J. Occup. Saf. Ergon. 2018, 25, 485–494. [Google Scholar] [CrossRef]
- Fernet, C.; Torrès, O.; Austin, S.; St-Pierre, J. The psychological costs of owning and managing an SME: Linking job stressors, occupational loneliness, entrepreneurial orientation, and burnout. Burn. Res. 2016, 3, 45–53. [Google Scholar] [CrossRef]
- Cubbon, L.; Darga, K.; Wisnesky, U.D.; Dennett, L.; Guptill, C. Depression among entrepreneurs: A scoping review. Small Bus. Econ. 2020, 57, 781–805. [Google Scholar] [CrossRef]
- Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Sanderson, K. Psychological distress and related work attendance among small-to-medium enterprise owner/managers: Literature review and research agenda. Int. J. Ment. Health Promot. 2012, 14, 219–236. [Google Scholar] [CrossRef]
- Barsade, S.G. The Ripple Effect: Emotional Contagion and its Influence on Group Behavior. Adm. Sci. Q. 2002, 47, 644–675. [Google Scholar] [CrossRef]
- Barsade, S.G.; Gibson, D.E. Why does affect matter in organizations? Acad. Manag. Perspect. 2007, 21, 36–59. [Google Scholar] [CrossRef]
- Janssen, O. Fairness Perceptions as a Moderator in the Curvilinear Relationships Between Job Demands, and Job Performance and Job Satisfaction. Acad. Manag. J. 2001, 44, 1039–1050. [Google Scholar] [CrossRef]
- Hägele, H.; Fertig, M. 1st Interim Report Evaluation of the Company- and Employee Surveys—Corrected Version; Geschäftsstelle der Nationalen Arbeitsschutzkonferenz c/o Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Berlin, Germany, 2018. [Google Scholar]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef] [PubMed]
- Bhui, K.S.; Dinos, S.; Stansfeld, S.A.; White, P.D. A Synthesis of the Evidence for Managing Stress at Work: A Review of the Reviews Reporting on Anxiety, Depression, and Absenteeism. J. Environ. Public Health 2012, 2012, 1–21. [Google Scholar] [CrossRef]
- Joyce, S.; Modini, M.; Christensen, H.; Mykletun, A.; Bryant, R.; Mitchell, P.B.; Harvey, S.B. Workplace interventions for common mental disorders: A systematic meta-review. Psychol. Med. 2015, 46, 683–697. [Google Scholar] [CrossRef]
- Martin, A.; Sanderson, K.; Cocker, F. Meta-analysis of the effects of health promotion intervention in the workplace on depression and anxiety symptoms. Scand. J. Work. Environ. Health 2008, 35, 7–18. [Google Scholar] [CrossRef]
- Dawkins, S.; Martin, A.; Kilpatrick, M.; Scott, J. Reasons for engagement: SME owner-manager motivations for engaging in a workplace mental health and wellbeing intervention. J. Occup. Environ. Med. 2018, 60, 917–927. [Google Scholar] [CrossRef]
- Moore, S.C.; Brennan, I.R.; Murphy, S.; Byrne, E.; Moore, S.N.; Shepherd, J.P.; Moore, L. The reduction of intoxication and disorder in premises licensed to serve alcohol: An exploratory randomised controlled trial. BMC Public Health 2010, 10, 607. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group*, t. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evidence-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- *Hansen, E.; Landstad, B.J.; Gundersen, K.T.; Vinberg, S. Leader-Based Workplace Health Interventions—A Before–After Study in Norwegian and Swedish Small-Scale Enterprises. Int. J. Disabil. Manag. 2016, 11, e5. [Google Scholar] [CrossRef]
- *Schwatka, N.V.; Dally, M.; Shore, E.; Tenney, L.; Brown, C.E.; Scott, J.G.; Dexter, L.; Newman, L.S. Small + Safe + Well: Lessons learned from a Total Worker Health® randomized intervention to promote organizational change in small business. BMC Public Health 2022, 22, 1039. [Google Scholar] [CrossRef]
- *Takao, S.; Tsutsumi, A.; Nishiuchi, K.; Mineyama, S.; Kawakami, N. Effects of the job stress education for supervisors on psychological distress and job performance among their immediate subordinates: A supervisor-based randomized controlled trial. J. Occup. Health 2006, 48, 494–503. [Google Scholar] [CrossRef] [PubMed]
- *Busch, C.; Dreyer, R.; Janneck, M. Blended recovery and burnout coaching for small-business copreneurs. Consult. Psychol. J. Pract. Res. 2021, 73, 65–87. [Google Scholar] [CrossRef]
- *Saraf, P.; Rahman, T.; Jamison, J.C. Group-Based Cognitive Behavioral Therapy (CBT) Training Improves Mental Health of SME Entrepreneurs: Experimental Evidence from Conflict-Affected Areas of Pakistan. In World Bank Policy Research Working Paper 2019; SSRN: Rochester, NY, USA, 2019; p. 8872. Available online: https://ssrn.com/abstract=3430478 (accessed on 23 May 2023).
- *Martin, A.; Kilpatrick, M.; Scott, J.; Cocker, F.; Dawkins, S.; Brough, P.; Sanderson, K. Protecting the Mental Health of Small-to-Medium Enterprise Owners: A Randomized Control Trial Evaluating a Self-Administered Versus Telephone Sup-ported Intervention. J. Occup. Environ. Med. 2020, 62, 503–510. [Google Scholar] [CrossRef] [PubMed]
- *Schwatka, N.V.; Dally, M.; Tenney, L.; Shore, E.; Brown, C.E.; Newman, L.S. Total Worker Health leadership and business strategies are related to safety and health climates in small business. Int. J. Environ. Res. Public Health 2020, 17, 2142. [Google Scholar] [CrossRef] [PubMed]
- Staehr, J.K. The use of well-being measures in primary health care-the DepCare project. In World Health Organization, Regional Office for Europe: Well-Being Measures in Primary Health Care-the DepCare Project; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Kawada, T.; Otsuka, T. Relationship between job stress, occupational position and job satisfaction using a brief job stress questionnaire (BJSQ). Work 2011, 40, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Huang, Y.-H.; Robertson, M.M.; Murphy, L.A.; Garabet, A.; Chang, W.-R. External validity of a generic safety climate scale for lone workers across different industries and companies. Accid. Anal. Prev. 2014, 63, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Zweber, Z.M.; Henning, R.A.; Magley, V.J. A practical scale for multi-faceted organizational health climate assessment. J. Occup. Health Psychol. 2016, 21, 250–259. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Enzmann, D.; Kleiber, D. Helfer-Leiden: Stress und Burnout in Psychosozialen Berufen; Asanger: Wien, Austria, 1989. [Google Scholar]
- Christensen, M. Building Engagement and Healthy Organisations: Validation of the Nordic Questionnaire on Positive Organisational Psychology (N-POP), the Third Report from the Nordic Project; Nordic Council of Ministers: Copenhagen, Denmark, 2012. [Google Scholar]
- Krohne, H.W.; Egloff, B.; Kohlmann, C.-W.; Tausch, A. Untersuchungen mit einer deutschen version der “positive and negative affect schedule” (PANAS). Diagnostica 1996, 42, 139–156. [Google Scholar]
- Chilcot, J.; Hudson, J.L.; Moss-Morris, R.; Carroll, A.; Game, D.; Simpson, A.; Hotopf, M. Screening for psychological distress using the Patient Health Questionnaire Anxiety and Depression Scale (PHQ-ADS): Initial validation of structural validity in dialysis patients. Gen. Hosp. Psychiatry 2018, 50, 15–19. [Google Scholar] [CrossRef]
- Sonnentag, S.; Fritz, C. The Recovery Experience Questionnaire: Development and validation of a measure for assessing recuperation and unwinding from work. J. Occup. Health Psychol. 2007, 12, 204–221. [Google Scholar] [CrossRef]
- Bringsén, Å.; Andersson, H.I.; Ejlertsson, G. Development and quality analysis of the Salutogenic Health Indicator Scale (SHIS). Scand. J. Public Health 2008, 37, 13–19. [Google Scholar] [CrossRef]
- Nilsson, P. Development and quality analysis of the Work Experience Measurement Scale (WEMS). Work 2010, 35, 153–161. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Greif, S. Putting goals to work in coaching: The complexities of implementation. In Beyond Goals; Routledge: London, UK, 2016; pp. 125–150. [Google Scholar]
- Storch, M. Resource-activating selfmanagement with the Zurich Resource Model (ZRM). Editor. Impressum 2 Clin. Exp. 2004, 5, 29–66. [Google Scholar]
- ENWHP. Luxembourg Declaration on Workplace Health Promotion in the European Union; ENWHP: Brussels, Belgium, 2007. [Google Scholar]
- Luthans, F.; Youssef, C.M.; Sweetman, D.S.; Harms, P.D. Meeting the Leadership Challenge of Employee Well-Being Through Relationship PsyCap and Health PsyCap. J. Leadersh. Organ. Stud. 2012, 20, 118–133. [Google Scholar] [CrossRef]
- Burke, M.J.; Signal, S.M. Workplace safety: A multilevel, interdisciplinary perspective. In Research in Personnel and Human Resources Management; Emerald Group Publishing Limited: London, UK, 2010; Volume 29, pp. 1–47. [Google Scholar] [CrossRef]
- Theorell, T.; Emdad, R.; Arnetz, B.; Weingarten, A.-M. Employee effects of an educational program for managers at an insurance company. Psychosom. Med. 2001, 63, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Tenney, L.; Dexter, L.; Shapiro, D.C.; Dally, M.; Brown, C.E.; Schwatka, N.V.; Huebschmann, A.G.; McMillen, J.; Newman, L.S. Impact of advising on total worker health implementation. J. Occup. Environ. Med. 2021, 63, 657. [Google Scholar] [CrossRef] [PubMed]
- Busch, C.; Dreyer, R. Gesundheitscoaching für Paare; Springer Science and Business Media LLC: Dordrecht, The Netherlands, 2020; ISBN 9783658298517. [Google Scholar] [CrossRef]
- McGuinness, L.; Higgins, J. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Kuehnl, A.; Seubert, C.; Rehfuess, E.; von Elm, E.; Nowak, D.; Glaser, J. Human resource management training of supervisors for improving health and well-being of employees. Emergencias 2019, 2019, CD010905. [Google Scholar] [CrossRef]
- Lamontagne, A.; Keegel, T.; Louie, A.; Ostry, A.; Landsbergis, P.A. A systematic review of the job-stress intervention evaluation literature, 1990–2005. Int. J. Occup. Environ. Health 2007, 13, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Shir, N.; Nikolaev, B.N.; Wincent, J. Entrepreneurship and well-being: The role of psychological autonomy, competence, and relatedness. J. Bus. Ventur. 2018, 34, 105875. [Google Scholar] [CrossRef]
- Yeh, W.-Y.; Yeh, C.-Y.; Chen, C.-J. Exploring the public-private and company size differences in employees’ work characteristics and burnout: Data analysis of a nationwide survey in Taiwan. Ind. Health 2018, 56, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Torrès, O.; Thurik, R. Small business owners and health. Small Bus. Econ. 2018, 53, 311–321. [Google Scholar] [CrossRef]
- Donaldson, S.I.; Grant-Vallone, E.J. Understanding self-report bias in organizational behavior research. J. Bus. Psychol. 2002, 17, 245–260. [Google Scholar] [CrossRef]
- Graen, G.B.; Uhl-Bien, M. Relationship-based approach to leadership: Development of leader-member exchange (LMX) theory of leadership over 25 years: Applying a multi-level multi-domain perspective. Leadersh. Q. 1995, 6, 219–247. [Google Scholar] [CrossRef]
- Bass, B.M. From transactional to transformational leadership: Learning to share the vision. Organ. Dyn. 1991, 18, 19–31. [Google Scholar] [CrossRef]
- Bass, B.M. Two Decades of Research and Development in Transformational Leadership. Eur. J. Work. Organ. Psychol. 1999, 8, 9–32. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PICO Criteria | Inclusion | Exclusion |
|---|---|---|
| Participants | Leaders of small and medium-sized enterprises (SMEs) Experienced in managing more than one follower | Studies conducted in hospitals or health-care settings Public sectors Retired leaders |
| Intervention | Interventions with direct impact on leaders’ outcomes Interventions with indirect impact on followers’ outcomes or targeting the leader–follower dyad (if available) Content: Stress management, stress reduction, reduction in anxiety and depressive symptoms, improvement of quality of life, leader–follower relationship (LMX), transformational/transactional leadership style, improvement of health behaviour Type of intervention: face-to-face or web-based/online interventions All intensities or durations | Interventions targeting solely followers Interventions without a coach/instructor |
| Comparator | Control group not mandatory | |
| Outcome | Subjectively assessed psychosocial outcomes (e.g., distress, anxiety, depression, resilience, coping, effort–reward imbalance, leader–follower relationship) Objectively assessed psychophysiological outcomes (e.g., heart rate variability, cortisol, alpha-amylase) Other objectively assessed measures (e.g., number of sick days, resignations) | Studies without health-related outcome measures |
| Studies (n = 6) | ||
|---|---|---|
| Sample size | Total (n) | 4063 |
| Minimum sample size (n) | 32 | |
| Maximum sample size (n) | 2785 | |
| Age | Mean age range (M) | 41.7–51 |
| Study design | RCT (n) | 4 |
| Quasi-experimental (n) | 1 | |
| Pre-post study (n) | 1 | |
| Instruments | Sub-syndromal | |
| Stress | BJSQ (n = 1) Kessler K-10 (n = 1) | |
| Well-being | Five-item scale by Staehr (n =1) SHIS (n = 1) REQ (n =1) WHO-5 (n = 1) | |
| Burn-out | MBI (n = 1) | |
| Affect | PANAS (n = 1) | |
| Syndromal | ||
| Anxiety and depression | PHQ-ADS (n = 1) | |
| Leadership | ||
| CTSS (n = 1) HCS (n = 1) N-POP (n = 1) WEMS (n =1) | ||
| Response rates (%) | 37–96 | |
| Country—context | ||
| Australia | (n = 1) | |
| Germany | (n = 1) | |
| Japan | (n = 1) | |
| Norway and Sweden | (n = 1) | |
| Pakistan | (n = 1) | |
| USA | (n = 1) | |
| First Author (Year of Publication), Country Implemented | Recipients of the Intervention | Number of Followers per Leader | Outcome Measures Available for (Follower/Leader/Both) | Format | Framework |
|---|---|---|---|---|---|
| Busch et al. (2021), Germany [42] | Dyads of small business owners and their respective spouses | Intervention group: on average, 6 followers. Control group: on average 13 followers | Leader | Blended: online and face-to-face | Rubicon phase model [59] Zurich Resource Model [60] |
| Hansen et al. (2016), Norway and Sweden [39] | SME leaders | <20 followers | Leader and follower | Face-to-face and telephone contacts | European Network for Workplace Health Promotion [61] |
| Martin et al. (2020), Australia [44] | SME leaders | 0–200 followers | Leader | Self-administered and telephone supported | Psychological capital: work-related hope, optimism, resilience, and self-efficacy [62] |
| Saraf et al. (2019), Pakistan [43] | SME leaders | On average, 10 followers | Leader | Face-to-face | Cognitive behavioural therapy core elements (stress management, problem solving, behavioural activation, strengthening support network, self-care) adapted for leaders working within fragility, conflict, and violence surroundings |
| Schwatka et al. (2022), United States of America [40] | SME leader and one additional organization member (safety manager or human resource manager) | <500 followers | Follower and leader | In-person and virtual components | Multi-level model of safety [63] |
| Takao et al. (2006), Japan [41] | SME leaders | On average, 5.5 follower | Follower | Face-to-face | Theoretic background by Theorell et al. [64] assuming that training programs to improve the psychosocial competence of managers reduce stressors among leaders and employees |
| Busch et al., 2021 | ||
|---|---|---|
| Bias Domain | Authors Judgement | Reasons for Assessment 1 |
| Selection bias | Weak | selection not described no response rate described |
| Study design | Moderate | quasi-experimental |
| Confounders | Weak | sample was limited to mainly male leaders different sizes of employees per leader in intervention and control group identified as relevant confounder; control for this confounder was not reported |
| Blinding | Moderate | it is not clear if the outcome assessors were aware of the intervention or status of the participants the participants were aware of the research question |
| Data collection method | Strong | tools for outcome measures were reliable and valid |
| Withdrawals and drop-out | Strong | 80–100% of the participants completed the study |
| Hansen et al., 2016 | ||
| Bias Domain | Authors Judgement | Reasons for Assessment |
| Selection bias | Moderate | selected individuals were very likely to be representative of the target population no response rate described |
| Study design | Moderate | cohort analytic (two intervention groups) |
| Confounders | Weak | control of confounders was not described |
| Blinding | Moderate | it is not clear if the outcome assessors were aware of the intervention or status of the participants the participants were aware of the research question |
| Data collection method | Strong | tools for outcome measures were reliable and valid |
| Withdrawals and drop-out | Moderate | 69% of the participants completed the study |
| Martin et al., 2020 | ||
| Bias Domain | Authors Judgement | Reasons for Assessment |
| Selection bias | Moderate | selected individuals were very likely to be representative of the target population no response rate described |
| Study design | Strong | RCT |
| Confounders | Strong | no important differences between the groups |
| Blinding | Moderate | blinding was not described |
| Data collection method | Strong | tools for outcome measures reliable and valid |
| Withdrawals and drop-out | Weak | 49.5% of the participants completed the study |
| Saraf et al., 2019 | ||
| Bias Domain | Authors Judgement | Reasons for Assessment |
| Selection bias | Moderate | response rate less than 80% |
| Study design | Strong | RCT |
| Confounders | Strong | relevant confounders controlled |
| Blinding | Moderate | blinding is not described |
| Data collection method | Strong | tools for outcome measures were reliable and valid |
| Withdrawals and drop-out | Strong | low drop-out rate |
| Schwatka et al., 2022 | ||
| Bias Domain | Authors Judgement | Reasons for Assessment |
| Selection bias | Moderate | selected individuals were very likely to be representative of the target population no response rate described |
| Study design | Strong | RCT |
| Confounders | Strong | relevant confounders controlled |
| Blinding | Moderate | blinding was not described |
| Data collection method | Strong | tools for outcome measures were reliable and valid |
| Withdrawals and drop out | Weak | 37% of the participants completed the study |
| Takao et al., 2006 | ||
| Bias Domain | Authors Judgement | Reasons for Assessment |
| Selection bias | Strong | Participation rate: 96% |
| Study design | Strong | RCT |
| Confounders | Strong | relevant confounders controlled |
| Blinding | Moderate | blinding was not described |
| Data collection method | Strong | tools for outcome measures were reliable and valid |
| Withdrawals and drop-out | Strong | low drop-out rate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erschens, R.; Adam, S.H.; Schröpel, C.; Diebig, M.; Rieger, M.A.; Gündel, H.; Zipfel, S.; Junne, F. Improving Well-Being and Fostering Health-Oriented Leadership among Leaders in Small and Medium-Sized Enterprises (SMEs): A Systematic Review. Healthcare 2024, 12, 486. https://doi.org/10.3390/healthcare12040486
Erschens R, Adam SH, Schröpel C, Diebig M, Rieger MA, Gündel H, Zipfel S, Junne F. Improving Well-Being and Fostering Health-Oriented Leadership among Leaders in Small and Medium-Sized Enterprises (SMEs): A Systematic Review. Healthcare. 2024; 12(4):486. https://doi.org/10.3390/healthcare12040486
Chicago/Turabian StyleErschens, Rebecca, Sophia Helen Adam, Carla Schröpel, Mathias Diebig, Monika A. Rieger, Harald Gündel, Stephan Zipfel, and Florian Junne. 2024. "Improving Well-Being and Fostering Health-Oriented Leadership among Leaders in Small and Medium-Sized Enterprises (SMEs): A Systematic Review" Healthcare 12, no. 4: 486. https://doi.org/10.3390/healthcare12040486
APA StyleErschens, R., Adam, S. H., Schröpel, C., Diebig, M., Rieger, M. A., Gündel, H., Zipfel, S., & Junne, F. (2024). Improving Well-Being and Fostering Health-Oriented Leadership among Leaders in Small and Medium-Sized Enterprises (SMEs): A Systematic Review. Healthcare, 12(4), 486. https://doi.org/10.3390/healthcare12040486