
The Association of Hypertensive Disorders of Pregnancy with Infant Mortality, Preterm Delivery, and Small for Gestational Age

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
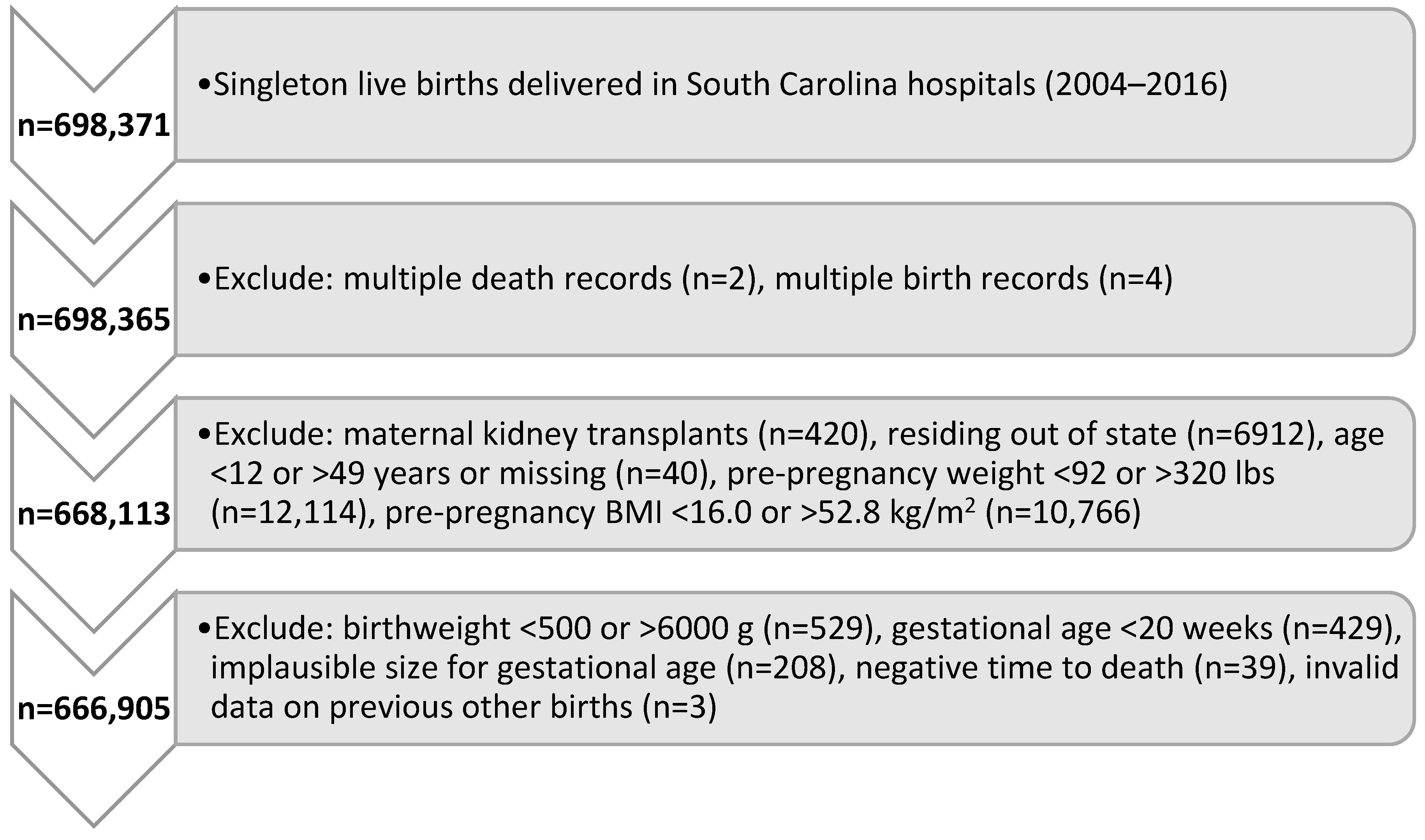
2.1. Cohort Selection
2.2. Exposures and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Association of Sociodemographic and Clinical Characteristics including Pregnancy and Delivery Complications with Infant Mortality
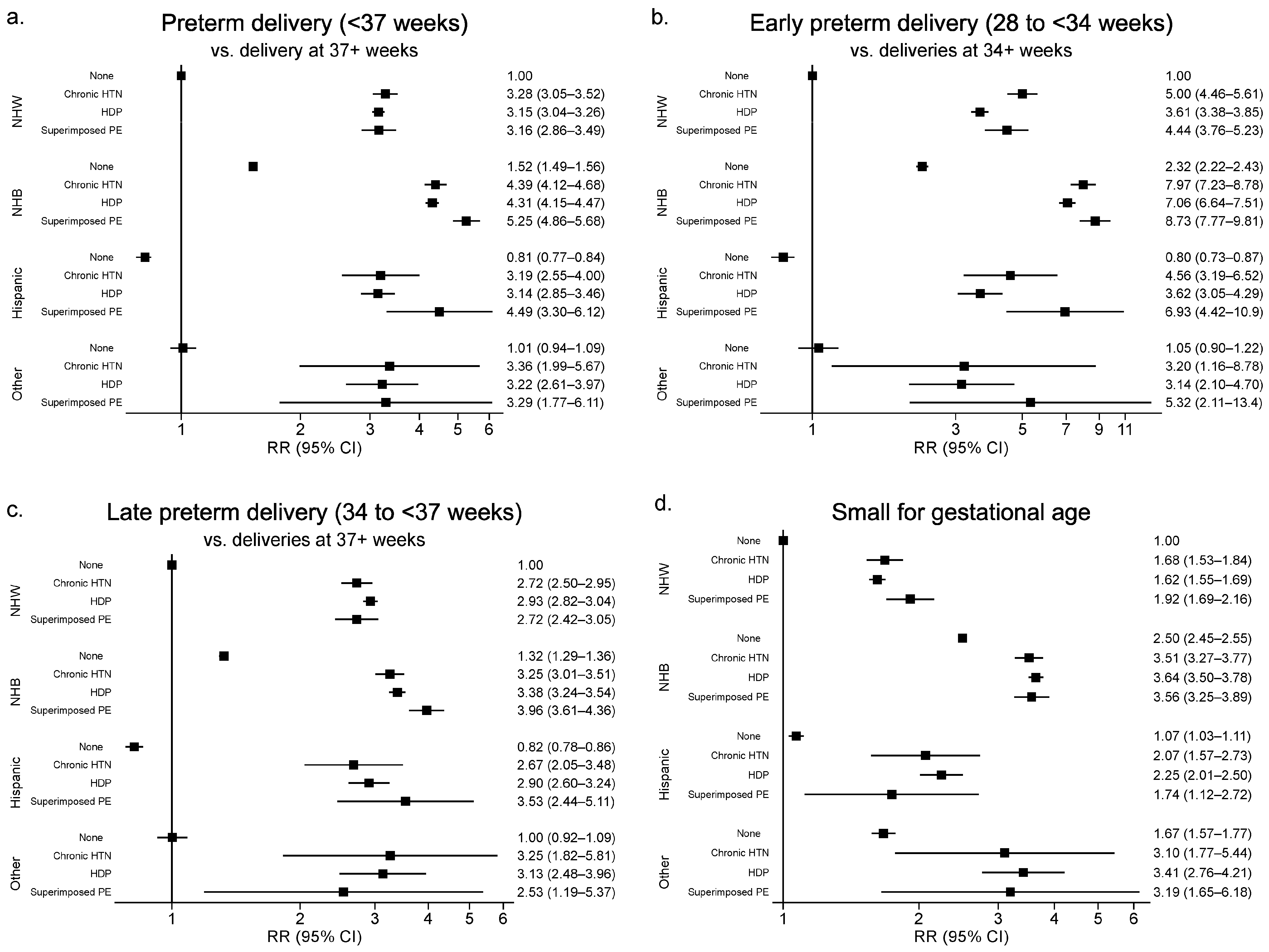
3.2. Joint Analysis of Race/Ethnicity, Chronic Hypertension, HDP and Superimposed Preeclampsia with PTD and SGA
3.2.1. Any Preterm Delivery (PTD)
3.2.2. Early Preterm Delivery (PTD)
3.2.3. Late Preterm Delivery (PTD)
3.2.4. Small for Gestational Age (SGA)
3.2.5. Sensitivity Analysis
4. Discussion
4.1. Prevention Strategies
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hutcheon, J.A.; Lisonkova, S.; Joseph, K.S. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Gemechu, K.S.; Assefa, N.; Mengistie, B. Prevalence of hypertensive disorders of pregnancy and pregnancy outcomes in Sub-Saharan Africa: A systematic review and meta-analysis. Women’s Health 2020, 16, 1745506520973105. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.L.; Ford, J.B.; Henderson-Smart, D.J.; Algert, C.S.; Morris, J.M. Hypertensive disorders in pregnancy: A population-based study. Med. J. Aust. 2005, 182, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, I.R.C.; Silva, W.B.M.; Cerqueira, G.S.G.; Novo, N.F.; Almeida, F.A.; Novo, J.L.V.G. Maternal and fetal outcome in women with hypertensive disorders of pregnancy: The impact of prenatal care. Ther. Adv. Cardiovasc. Dis. 2015, 9, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Ratnasiri, A.W.; Parry, S.S.; Arief, V.N.; DeLacy, I.H.; Lakshminrusimha, S.; Halliday, L.A.; DiLibero, R.J.; Basford, K.E. Temporal trends, patterns, and predictors of preterm birth in California from 2007 to 2016, based on the obstetric estimate of gestational age. Matern. Health Neonatol. Perinatol. 2018, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, K.K.; Dongarwar, D.; Alagili, D.E.; Maiyegun, S.O.; Salihu, H.M. Temporal trends and risk of small for gestational age (SGA) infants among Asian American mothers by ethnicity. Ann. Epidemiol. 2021, 63, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Harmon, Q.E.; Huang, L.; Umbach, D.M.; Klungsøyr, K.; Engel, S.M.; Magnus, P.; Skjærven, R.; Zhang, J.; Wilcox, A.J. Risk of Fetal Death With Preeclampsia. Obstet. Gynecol. 2015, 125, 628–635. [Google Scholar] [CrossRef]
- Roberti, R.; Rocca, M.; Iannone, L.F.; Gasparini, S.; Pascarella, A.; Neri, S.; Cianci, V.; Bilo, L.; Russo, E.; Quaresima, P.; et al. Status epilepticus in pregnancy: A literature review and a protocol proposal. Expert Rev. Neurother. 2022, 22, 301–312. [Google Scholar] [CrossRef]
- Bornstein, E.; Eliner, Y.; Chervenak, F.A.; Grünebaum, A. Concerning trends in maternal risk factors in the United States: 1989–2018. EClinicalMedicine 2020, 29–30, 100657. [Google Scholar] [CrossRef]
- Duckitt, K.; Harrington, D. Risk factors for pre-eclampsia at antenatal booking: Systematic review of controlled studies. BMJ 2005, 330, 565. [Google Scholar] [CrossRef]
- Bramham, K.; Parnell, B.; Nelson-Piercy, C.; Seed, P.T.; Poston, L.; Chappell, L.C. Chronic hypertension and pregnancy outcomes: Systematic review and meta-analysis. BMJ 2014, 348, g2301. [Google Scholar] [CrossRef] [PubMed]
- Al Khalaf, S.Y.; O’Reilly, É.J.; Barrett, P.M.; BLeite, D.F.; Pawley, L.C.; McCarthy, F.P.; Khashan, A.S. Impact of Chronic Hypertension and Antihypertensive Treatment on Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e018494. [Google Scholar] [CrossRef]
- Katz, J.; Lee, A.C.; Kozuki, N.; Black, R.E. Mortality Risk among Term and Preterm Small for Gestational Age Infants. Nestle Nutr. Inst. Workshop Ser. 2015, 81, 29–35. [Google Scholar] [CrossRef]
- Breathett, K.; Muhlestein, D.; Foraker, R.; Gulati, M. Differences in preeclampsia rates between African American and Caucasian women: Trends from the National Hospital Discharge Survey. J. Women’s Health 2014, 23, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Xiao, H.; Zheng, Y.; Yu, B.B. A Bayesian spatio-temporal analysis on racial disparities in hypertensive disorders of pregnancy in Florida, 2005–2014. Spat. Spatio-Temporal Epidemiol. 2019, 29, 43–50. [Google Scholar] [CrossRef]
- Kramer, M.S.; Ananth, C.V.; Platt, R.W.; Joseph, K.S. US Black vs White disparities in foetal growth: Physiological or pathological? Int. J. Epidemiol. 2006, 35, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Matoba, N.; Collins, J.W., Jr. Racial disparity in infant mortality. Semin. Perinatol. 2017, 41, 354–359. [Google Scholar] [CrossRef]
- Talge, N.M.; Mudd, L.M.; Sikorskii, A.; Basso, O. United States birth weight reference corrected for implausible gestational age estimates. Pediatrics 2014, 133, 844–853. [Google Scholar] [CrossRef]
- Alexander, G.R.; Kotelchuck, M. Quantifying the adequacy of prenatal care: A comparison of indices. Public Health Rep. 1996, 111, 408–418, discussion 419. [Google Scholar]
- Tayebi, T.; Hamzehgardeshi, Z.; Ahmad Shirvani, M.; Dayhimi, M.; Danesh, M. Relationship between Revised Graduated Index (R-GINDEX) of prenatal care utilization & preterm labor and low birth weight. Glob. J. Health Sci. 2014, 6, 131–137. [Google Scholar] [CrossRef]
- Amjad, S.; MacDonald, I.; Chambers, T.; Osornio-Vargas, A.; Chandra, S.; Voaklander, D.; Ospina, M.B. Social determinants of health and adverse maternal and birth outcomes in adolescent pregnancies: A systematic review and meta-analysis. Paediatr. Perinat. Epidemiol. 2019, 33, 88–99. [Google Scholar] [CrossRef]
- SAS Institute Inc. SAS for Windows; SAS Institute Inc.: Cary, NC, USA, 2012. [Google Scholar]
- Mendola, P.; Mumford, S.L.; Männistö, T.I.; Holston, A.; Reddy, U.M.; Laughon, S.K. Controlled Direct Effects of Preeclampsia on Neonatal Health After Accounting for Mediation by Preterm Birth. Epidemiology 2015, 26, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Lyu, X.; Zhang, W.; Zhang, J.; Wei, Y.; Guo, X.; Cui, S.; Yan, J.; Zhang, X.; Qiao, C.; Zhou, R.; et al. Morbidity and maternal and infant outcomes of hypertensive disorder in pregnancy in China in 2018. J. Clin. Hypertens. 2021, 23, 1194–1204. [Google Scholar] [CrossRef] [PubMed]
- Lailler, G.; Grave, C.; Gabet, A.; Regnault, N.; Deneux-Tharaux, C.; Kretz, S.; Mounier-Vehier, C.; Tsatsaris, V.; Plu-Bureau, G.; Blacher, J.; et al. Adverse Maternal and Infant Outcomes in Women With Chronic Hypertension in France (2010–2018): The Nationwide CONCEPTION Study. J. Am. Heart Assoc. 2023, 12, e027266. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.J.; Delagrange, H.; van Valkengoed, I.G.M.; de Groot, C.J.M.; van den Born, B.H.; Gordijn, S.J.; Ganzevoort, W. Hypertensive Disorders of Pregnancy and Cardiovascular Disease Risk Across Races and Ethnicities: A Review. Front. Cardiovasc. Med. 2022, 9, 933822. [Google Scholar] [CrossRef] [PubMed]
- Vanek, M.; Sheiner, E.; Levy, A.; Mazor, M. Chronic hypertension and the risk for adverse pregnancy outcome after superimposed pre-eclampsia. Int. J. Gynecol. Obstet. 2004, 86, 7–11. [Google Scholar] [CrossRef] [PubMed]
- McCowan, L.M.; Buist, R.G.; North, R.A.; Gamble, G. Perinatal morbidity in chronic hypertension. Br. J. Obstet. Gynaecol. 1996, 103, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Atkins, R.; Pontes, N.M.H.; Patterson, N.A.; Hinckson, A.; Aromolaran, D.; McCray, A.; Pontes, M.C.F. Effects of Race, Ethnicity, and Maternal Education on Infant Mortality. Nurs. Res. 2024, 73, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Okobi, O.E.; Ibanga, I.U.; Egbujo, U.C.; Egbuchua, T.O.; Oranu, K.P.; Oranika, U.S. Trends and Factors Associated With Mortality Rates of Leading Causes of Infant Death: A CDC Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) Database Analysis. Cureus 2023, 15, e45652. [Google Scholar] [CrossRef]
- Vital Statistics. South Carolina Department of Health and Environmental Control. South Carolina Vital and Morbidity Statistics 2019. Available online: https://scdhec.gov/sites/default/files/media/document/Vital-Morbidity-Statistics_2019.pdf (accessed on 27 April 2022).
- U.S. Department of Health and Human Services. Healthy People 2030. Available online: https://health.gov/healthypeople (accessed on 22 June 2022).
- Ghosh, G.; Grewal, J.; Männistö, T.; Mendola, P.; Chen, Z.; Xie, Y.; Laughon, S.K. Racial/ethnic differences in pregnancy-related hypertensive disease in nulliparous women. Ethn. Dis. 2014, 24, 283–289. [Google Scholar]
- Garovic, V.D.; Dechend, R.; Easterling, T.; Karumanchi, S.A.; Baird, S.M.; Magee, L.A.; Rana, S.; Vermunt, J.V.; August, P. Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement From the American Heart Association. Hypertension 2022, 79, e21–e41. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52. [CrossRef]
- LeFevre, M.L. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2014, 161, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; von Dadelszen, P.; Rey, E.; Ross, S.; Asztalos, E.; Murphy, K.E.; Menzies, J.; Sanchez, J.; Singer, J.; Gafni, A.; et al. Less-Tight versus Tight Control of Hypertension in Pregnancy. N. Engl. J. Med. 2015, 372, 407–417. [Google Scholar] [CrossRef]
- Afana, M.; Brinjikji, W.; Kao, D.; Jackson, E.; Maddox, T.M.; Childers, D.; Eagle, K.A.; Davis, M.B. Characteristics and In-Hospital Outcomes of Peripartum Cardiomyopathy Diagnosed During Delivery in the United States From the Nationwide Inpatient Sample (NIS) Database. J. Card. Fail. 2016, 22, 512–519. [Google Scholar] [CrossRef]
- Tanaka, M.; Jaamaa, G.; Kaiser, M.; Hills, E.; Soim, A.; Zhu, M.; Shcherbatykh, I.Y.; Samelson, R.; Bell, E.; Zdeb, M.; et al. Racial Disparity in Hypertensive Disorders of Pregnancy in New York State: A 10-Year Longitudinal Population-Based Study. Am. J. Public. Health 2007, 97, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Drosdzol-Cop, A.; Staniczek, J.; Orszulak, D.; Kowalczyk, K.; Fuchs, A.; Sieroszewski, P.; Wielgos, M.; Kalinka, J.; Huras, H.; Wegrzyn, P.; et al. The Polish Society of Gynecologists and Obstetricians’ Expert Group Recommendations regarding adolescent pregnancy. Ginekol. Pol. 2023, 94, 258–267. [Google Scholar] [CrossRef]
- Roeckner, J.T.; Pressman, K.; Odibo, L.; Duncan, J.R.; Odibo, A.O. Outcome-based comparison of SMFM and ISUOG definitions of fetal growth restriction. Ultrasound Obstet. Gynecol. 2021, 57, 925–930. [Google Scholar] [CrossRef]
- Martins, J.G.; Biggio, J.R.; Abuhamad, A. Society for Maternal-Fetal Medicine Consult Series #52: Diagnosis and management of fetal growth restriction: (Replaces Clinical Guideline Number 3, April 2012). Am. J. Obstet. Gynecol. 2020, 223, B2–B17. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | No HTN | Chronic HTN | HDP | Superimposed Preeclampsia | ||
|---|---|---|---|---|---|---|
| N = 666,905 | N = 594,383 | N = 12,180 | N = 53,582 | N = 6760 | ||
| (89.1%) | (1.8%) | (8.0%) | (1.0%) | |||
| Characteristic | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | |
| One year infant mortality | 2426 (0.4) | 2035 (0.3) | 73 (0.6) | 273 (0.5) | 45 (0.7) | |
| Any PTD (20 to <37 weeks) | 62,215 (9.3) | 47,043 (7.9) | 2722 (22.3) | 10,882 (20.3) | 1568 (23.2) | |
| Early PTD (20 to <34 weeks) | 15,908 (2.4) | 10,982 (1.8) | 991 (8.1) | 3362 (6.3) | 573 (8.5) | |
| Late PTD (34 to <37 weeks) | 46,307 (6.9) | 36,061 (6.1) | 1731 (14.2) | 7520 (14.0) | 995 (14.7) | |
| Small for gestational age | 71,301 (10.7) | 60,573 (10.2) | 1667 (13.7) | 8057 (15.0) | 1004 (14.9) | |
| Maternal age at delivery | 26.7 ± 5.9 | 26.6 ± 5.9 | 29.0 ± 5.9 | 26.7 ± 6.2 | 29.8 ± 6.2 | |
| Race | ||||||
| Non-Hispanic White | 381,325 (57.2) | 344,249 (57.9) | 5552 (45.6) | 28,693 (53.5) | 2831 (41.9) | |
| Non-Hispanic Black | 213,516 (32.0) | 182,473 (30.7) | 6025 (49.5) | 21,379 (39.9) | 3639 (53.8) | |
| Hispanic | 58,696 (8.8) | 55,082 (9.3) | 499 (4.1) | 2893 (5.4) | 222 (3.3) | |
| Other | 13,368 (2.0) | 12,579 (2.1) | 104 (0.9) | 617 (1.2) | 68 (1.0) | |
| Education | ||||||
| Less than high school | 136,541 (20.5) | 123,117 (20.7) | 2198 (18.0) | 10,280 (19.2) | 946 (14.0) | |
| High school graduate | 166,683 (25.0) | 147,431 (24.8) | 3244 (26.6) | 14,159 (26.4) | 1849 (27.4) | |
| Some college | 160,841 (24.1) | 141,764 (23.9) | 3260 (26.8) | 14,005 (26.1) | 1812 (26.8) | |
| College graduate and above | 202,840 (30.4) | 182,071 (30.6) | 3478 (28.6) | 15,138 (28.3) | 2153 (31.8) | |
| Rural residence b | 177,769 (26.7) | 159,071 (26.8) | 3391 (27.8) | 13,470 (25.1) | 1837 (27.2) | |
| Primary payer (during pregnancy) | ||||||
| Medicaid | 338,404 (50.7) | 299,558 (50.4) | 6818 (56.0) | 28,638 (53.4) | 3390 (50.1) | |
| Private | 253,216 (38.0) | 225,554 (37.9) | 4539 (37.3) | 20,310 (37.9) | 2813 (41.6) | |
| Self-pay | 36,443 (5.5) | 34,142 (5.7) | 399 (3.3) | 1735 (3.2) | 167 (2.5) | |
| Other | 33,442 (5.0) | 30,311 (5.1) | 348 (2.9) | 2463 (4.6) | 320 (4.7) | |
| WIC eligibility during pregnancy | 346,663 (52.0) | 306,109 (51.5) | 6680 (54.8) | 30,014 (56.0) | 3860 (57.1) | |
| Smoking during pregnancy | 80,396 (12.1) | 72,059 (12.1) | 1439 (11.8) | 6176 (11.5) | 722 (10.7) | |
| Pre-pregnancy BMI | 27.1 ± 6.7 | 26.6 ± 6.4 | 32.2 ± 7.9 | 30.3 ± 7.6 | 33.9 ± 7.8 | |
| Number of prior pregnancies | 1.0 ± 1.2 | 1.0 ± 1.2 | 1.6 ± 1.4 | 0.7 ± 1.1 | 1.0 ± 1.3 | |
| Previous cesarean section | ||||||
| No | 252,334 (37.8) | 224,950 (37.8) | 4659 (38.3) | 20,227 (37.7) | 2498 (37.0) | |
| Yes | 46,300 (6.9) | 40,599 (6.8) | 2029 (16.7) | 3170 (5.9) | 502 (7.4) | |
| Unknown | 368,271 (55.2) | 328,834 (55.3) | 5492 (45.1) | 30,185 (56.3) | 3760 (55.6) | |
| Previous preterm births | 19,822 (3.0) | 16,681 (2.8) | 1010 (8.3) | 1781 (3.3) | 350 (5.2) | |
| Prenatal care as measured by R-GINDEX | ||||||
| Inadequate | 118,499 (17.8) | 108,481 (18.3) | 1644 (13.5) | 7666 (14.3) | 708 (10.5) | |
| Intermediate | 147,374 (22.1) | 133,654 (22.5) | 2179 (17.9) | 10,456 (19.5) | 1085 (16.1) | |
| Adequate | 10,338 (1.6) | 9117 (1.5) | 191 (1.6) | 921 (1.7) | 109 (1.6) | |
| Intensive | 187,043 (28.0) | 159,513 (26.8) | 4638 (38.1) | 19,784 (36.9) | 3108 (46.0) | |
| No care | 6382 (1.0) | 5698 (1.0) | 158 (1.3) | 468 (0.9) | 58 (0.9) | |
| Missing | 197,269 (29.6) | 177,920 (29.9) | 3370 (27.7) | 14,287 (26.7) | 1692 (25.0) | |
| Pre-pregnancy diabetes or GDM | 41,624 (6.2) | 31,441 (5.3) | 2117 (17.4) | 6532 (12.2) | 1534 (22.7) | |
| Birth weight (g) | 3252.2 ± 566.8 | 3277.8 ± 541.3 | 3035.6 ± 738.4 | 3051.2 ± 699.2 | 2984.0 ± 737.2 | |
| Low birth weight (<2500 g) | 50,945 (7.6) | 38,051 (6.4) | 2239 (18.4) | 9304 (17.4) | 1351 (20.0) | |
| Very low birth weight (<1500 g) | 8226 (1.2) | 5304 (0.9) | 589 (4.8) | 1979 (3.7) | 354 (5.2) | |
| Size | ||||||
| Appropriate for gestational age | 536,023 (80.4) | 480,925 (80.9) | 9280 (76.2) | 40,670 (75.9) | 5148 (76.2) | |
| Small for gestational age | 71,301 (10.7) | 60,573 (10.2) | 1667 (13.7) | 8057 (15.0) | 1004 (14.9) | |
| Large for gestational age | 59,561 (8.9) | 52,867 (8.9) | 1233 (10.1) | 4854 (9.1) | 607 (9.0) | |
| Male baby | 340,208 (51.0) | 303,134 (51.0) | 6181 (50.7) | 27,474 (51.3) | 3419 (50.6) | |
| Infant Mortality | ||||
|---|---|---|---|---|
| No | Yes | |||
| N = 664,479 (99.6%) | N = 2426 (0.4%) | Adjusted * RR (95% CI) | ||
| Characteristic | n (%) or Mean ± SD | n (%) or Mean ± SD | ||
| No HTN | 592,348 (89.1) | 2035 (83.9) | referent | |
| Chronic HTN | 12,107 (1.8) | 73 (3.0) | 1.48 (1.16–1.88) | |
| HDP | 53,309 (8.0) | 273 (11.3) | 1.39 (1.21–1.58) | |
| Superimposed preeclampsia | 6715 (1.0) | 45 (1.9) | 1.79 (1.31–2.43) | |
| Maternal age at delivery | 26.7 ± 5.9 | 25.4 ± 6.0 | 0.98 (0.97–0.99) | |
| Race | ||||
| Non-Hispanic White | 380,150 (57.2) | 1175 (48.4) | referent | |
| Non-Hispanic Black | 212,425 (32.0) | 1091 (45.0) | 1.43 (1.30–1.57) | |
| Hispanic | 58,559 (8.8) | 137 (5.6) | 0.67 (0.54–0.82) | |
| Other | 13,345 (2.0) | 23 (0.9) | 0.75 (0.49–1.13) | |
| Education | ||||
| Less than high school | 135,854 (20.4) | 687 (28.3) | 1.53 (1.30–1.80) | |
| High school graduate | 165,949 (25.0) | 734 (30.3) | 1.41 (1.21–1.63) | |
| Some college | 160,251 (24.1) | 590 (24.3) | 1.29 (1.12–1.49) | |
| College graduate and above | 202,425 (30.5) | 415 (17.1) | referent | |
| Urban/rural (based on RUCA by zipcode of residence) | ||||
| Urban | 487,429 (73.4) | 1707 (70.4) | referent | |
| Rural | 177,050 (26.6) | 719 (29.6) | 0.96 (0.87–1.06) | |
| Primary payer (during pregnancy) from birth records | ||||
| Medicaid | 336,808 (50.7) | 1596 (65.8) | 1.38 (1.22–1.56) | |
| Private | 252,644 (38.0) | 572 (23.6) | referent | |
| Self-pay | 36,313 (5.5) | 130 (5.4) | 1.58 (1.27–1.98) | |
| Other | 33,337 (5.0) | 105 (4.3) | 1.34 (1.08–1.66) | |
| WIC eligibility during pregnancy | ||||
| No | 308,691 (46.5) | 935 (38.5) | referent | |
| Yes | 345,214 (52.0) | 1449 (59.7) | 0.81 (0.73–0.89) | |
| Smoking during pregnancy | ||||
| No | 584,301 (87.9) | 1871 (77.1) | referent | |
| Yes | 79,843 (12.0) | 553 (22.8) | 1.88 (1.69–2.09) | |
| Pre-pregnancy BMI | 27.1 ± 6.7 | 28.1 ± 7.3 | 1.01 (1.01–1.02) | |
| Number of prior pregnancies | 1.0 ± 1.2 | 1.1 ± 1.3 | 1.06 (1.02–1.10) | |
| Previous cesarean section | ||||
| No | 251,485 (37.8) | 849 (35.0) | referent | |
| Yes | 46,147 (6.9) | 153 (6.3) | 0.87 (0.73– 1.04) | |
| Unknown | 366,847 (55.2) | 1424 (58.7) | 1.07 (0.98–1.17) | |
| Previous preterm births | ||||
| No | 644,818 (97.0) | 2265 (93.4) | referent | |
| Yes | 19,661 (3.0) | 161 (6.6) | 1.96 (1.66–2.33) | |
| Sex of baby | ||||
| Male | 338,796 (51.0) | 1412 (58.2) | referent | |
| Female | 325,683 (49.0) | 1014 (41.8) | 0.75 (0.69–0.81) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, D.A.; Mateus, J.; Ash, E.; Turan, T.N.; Hunt, K.J.; Malek, A.M. The Association of Hypertensive Disorders of Pregnancy with Infant Mortality, Preterm Delivery, and Small for Gestational Age. Healthcare 2024, 12, 597. https://doi.org/10.3390/healthcare12050597
Wilson DA, Mateus J, Ash E, Turan TN, Hunt KJ, Malek AM. The Association of Hypertensive Disorders of Pregnancy with Infant Mortality, Preterm Delivery, and Small for Gestational Age. Healthcare. 2024; 12(5):597. https://doi.org/10.3390/healthcare12050597
Chicago/Turabian StyleWilson, Dulaney A., Julio Mateus, Emily Ash, Tanya N. Turan, Kelly J. Hunt, and Angela M. Malek. 2024. "The Association of Hypertensive Disorders of Pregnancy with Infant Mortality, Preterm Delivery, and Small for Gestational Age" Healthcare 12, no. 5: 597. https://doi.org/10.3390/healthcare12050597
APA StyleWilson, D. A., Mateus, J., Ash, E., Turan, T. N., Hunt, K. J., & Malek, A. M. (2024). The Association of Hypertensive Disorders of Pregnancy with Infant Mortality, Preterm Delivery, and Small for Gestational Age. Healthcare, 12(5), 597. https://doi.org/10.3390/healthcare12050597