
Perceptions of Therapeutic Climbing for Patients with Multiple Sclerosis in Neurorehabilitation: A Qualitative Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
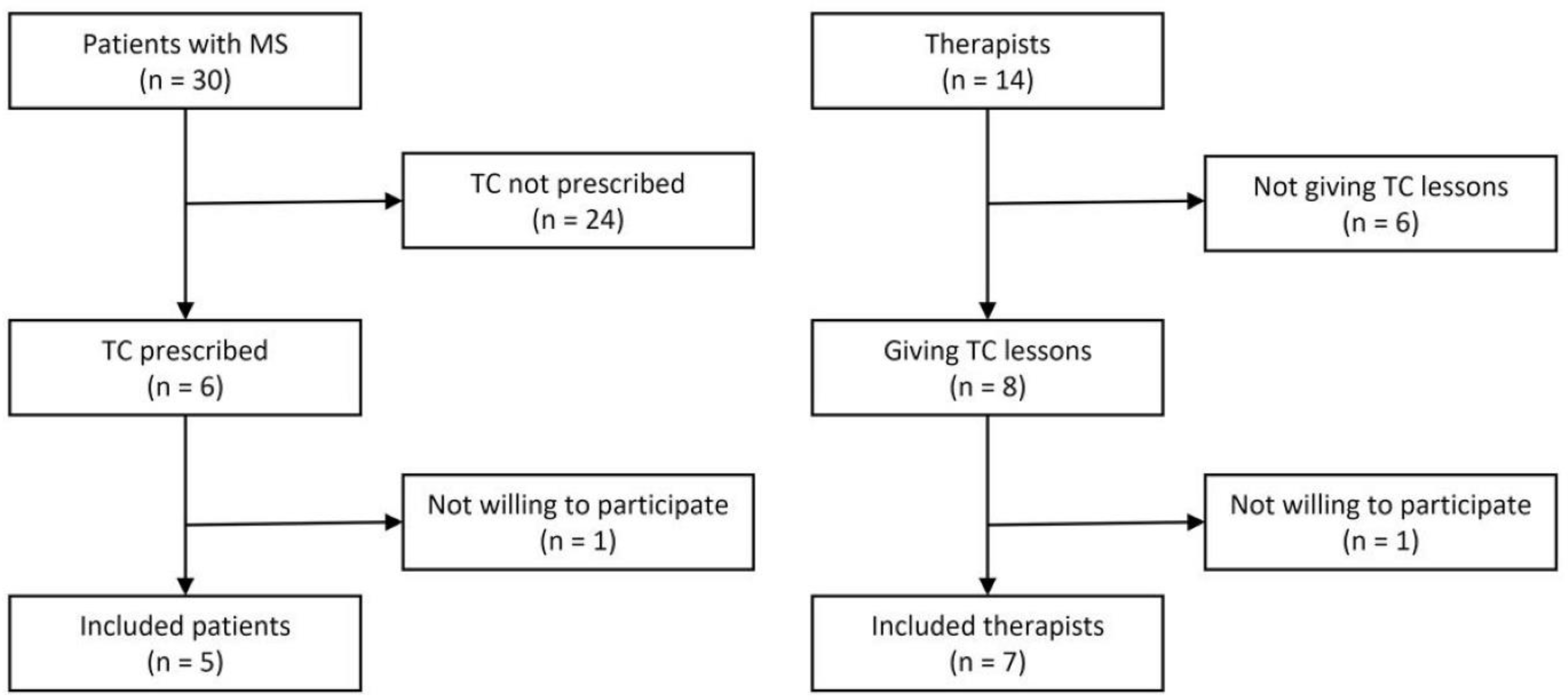
2.2. Participants
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Motivational Factors
And the big advantage is that the exercises are very short, and then you immediately have a success–and if you have no success, then you think to yourself that it also does not matter. […] But it is simple, uplifting. It is good for the mind. It raises your self-esteem again, and that’s a fun factor, where you know: “Yes, if I make it, then it’s good, and if not, it doesn’t matter”.(P2)
“You have quite a tunnel vision, then. For me, it is like this. I do not notice much around me. I am also quite sensitive to noise, but I am highly concentrated. I get into a flow and always want to do things right. So, I do not always want to do things halfway–I just want to do it right”.(P3)
“The motivation is to get it done. So certain movements, whether the basic position or coming up [the wall], reach as high as I can. The nice thing is that you see the result immediately. If it works or does not work, that is just great. And if it does not work, I just do it again. So that is really special, and I really enjoy it”.(P5)
“I liked that although I am thin, I have quite a bit of strength in my hands, and I can use that. I have a good feeling because I know: “You can do that”. And I am not at the mercy of the feeling that I am going to fail”.(P3)
3.2. Training Conditions
“And that is simply what distinguishes it from physiotherapy, where it is quite clear what is happening, for instance, squatting down or with the heels on the floor–just as great. It is just that with climbing, there is also the aspect of fun, while at the same time, it is somehow very intense, but that is good”.(P5)
“When you face challenges in climbing, you can’t just take it lightly. In other forms of training, you can adjust the weight to your preference; for instance, I could choose to train with 5 kilos. But in climbing, you’re contending with your own body weight. That’s the weight you must manage”.
“Because as a therapist, it starts relatively soon that I play with the intensities. If I see that the person is doing a great job and it is working great, I can think about doing a more difficult exercise for them. If I see that the exercise is already quite demanding, then I can make the next exercise easier”.(T2)
“I just have to rest for a short while after the training. […] Half an hour or hour and then I feel very fit again”.(P4)
“Longer [sessions] would avail to nothing because then you get into exhaustion, and then you are demotivated, because it does not work. So, because it is also a strength exercise, with this trunk stabilization, I think that is a good time interval. Just that long, not longer, not shorter”.(P2)
“It is a group, and group programs are usually just not so specific. Or let me put it this way: it is a clear extra effort if you give two patients completely different exercises”.(T5)
3.3. Training Content
“So, what I find good is that the exercises always go out from a fixed basic position, where the basic position always recalls this stability again and again. That is–with the shoulders down and abdominal tension and a bit of squatting–heels up”.(T1)
“And today–I climbed today for the second time–I climbed from wall to wall. It was great, both with overhang, it was really cool. […] It is structured great. First, you learn to do the basics and climb that way. […] Then, the arms relaxed, and I actually climbed from right to left and left to right today”.(P5)
3.4. Observed Effects
“Of course, [TC is] strengthening the muscles–be it upper arms or grip strength, lower extremities, or trunk stability, respectively. Another effect is, for example, torso stability, spinal stability, posture, but also coordination. And, of course, how to grasp things, how tightly you have to grip in order to be able to hold on. Balance is also trained for people to become a bit more mobile and secure in everyday life and minimize their risk of falling”.(T4)
“In the neck, shoulder, and upper back areas, I notice it already. And, of course, biceps, triceps, you feel very strongly. […] Anyways, you notice the strength, which then just increases a bit. The grip strength is what now just works properly”.(P3)
“I think climbing also has a high motivational character, so the patients gain self-confidence and security. By climbing not only at standing height but also a little higher, I believe that patients gain self-confidence and thus appear more self-assured”.(T4)
“I already felt like I fit in. I think I have improved not only my athletic activity but also my cognitive capability because you just have to think ahead: Where do I step? Where do I reach? […] That is not so easy for me, and that is why I actually found it good that I can combine both in one unit, both physically and then mentally a bit”.(P3)
3.5. Safety Protocol
“Well, it also has much to do with self-awareness, which is perhaps not the case with normal strength training, where I sit on the machine and simply move the leg press. There is just not as much body awareness as in climbing”.(T5)
“First of all, they need to have a certain strength in the forefeet–so that they can stand on their forefeet at all–and then hold themselves up with the upper extremities with both hands”.(T2)
“I mean–I have never had the case–but if any extremity would be paralyzed or that somebody has perhaps such feelings of numbness, I imagine that would be difficult. I would not know if that would not be rather frustrating if I felt that way”.(P3)
“I felt safe because the therapist was always behind me, and I know she catches me when something happens”.(P1)
“As a therapist, if you notice that it is unsafe, you can also stand directly behind the patients. That means that if they slip, it is safe so that they do not hurt themselves badly”.(T1)
“Such [mild] pain may occur again and again, in the shoulders, in the knee joint–but nothing more serious”.(T4)
“Once, it was too much for me. I think this morning was intense because I was training in half-hour intervals without a break–first climbing, then eating. And then, I had an intensity tremor in my hands, and then I noticed […] the trembling of the hands became significantly more, and it was difficult to eat”.(P3)
“I have to say that I cannot think of any MS patient who has stopped climbing with me because of fatigue. […] When patients stop, it is usually because of pain; those are more likely to be spine patients. […] Of course, what happens from time to time is that they say beforehand that they are totally exhausted. But then you try to arrange it, so the MS patient takes longer breaks”.(T5)
4. Discussion
4.1. Motivational Factors
4.2. Training Conditions
4.3. Observed Effects
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. ICD-10: International Statistical Classification of Diseases and Related Health Problems 10th Revision; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Tafti, D.; Ehsan, M.; Xixis, K.L. Multiple Sclerosis; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kesselring, J.; Beer, S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol. 2005, 4, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, A.; Marissal, J.P.; Pouyfaucon, M.; Vermersch, P.; Hautecoeur, P.; Dervaux, B. Social participation in patients with multiple sclerosis: Correlations between disability and economic burden. BMC Neurol. 2014, 14, 115. [Google Scholar] [CrossRef] [PubMed]
- Salter, A.; Fox, R.J.; Tyry, T.; Cutter, G.; Marrie, R.A. The association of fatigue and social participation in multiple sclerosis as assessed using two different instruments. Mult. Scler. Relat. Disord. 2019, 31, 165–172. [Google Scholar] [CrossRef]
- DeSousa, E.A.; Albert, R.H.; Kalman, B. Cognitive impairments in multiple sclerosis: A review. Am. J. Alzheimer’s Dis. Other Dement. 2002, 17, 23–29. [Google Scholar] [CrossRef]
- Petracca, M.; Pontillo, G.; Moccia, M.; Carotenuto, A.; Cocozza, S.; Lanzillo, R.; Brunetti, A.; Brescia Morra, V. Neuroimaging Correlates of Cognitive Dysfunction in Adults with Multiple Sclerosis. Brain Sci. 2021, 11, 346. [Google Scholar] [CrossRef]
- Iodice, R.; Aceto, G.; Ruggiero, L.; Cassano, E.; Manganelli, F.; Dubbioso, R. A review of current rehabilitation practices and their benefits in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2023, 69, 104460. [Google Scholar] [CrossRef] [PubMed]
- Leichtfried, V. Therapeutisches Klettern—Eine Extremsportart geht neue Wege. In Alpin und Höhenmedizin; Franz Berghold, H.B., Burtscher, M., Domej, W., Durrer, B., Fischer, R., Paal, P., Schaffert, W., Schobersberger, W., Sumann, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 107–117. [Google Scholar]
- Frühauf, A.; Heußner, J.; Niedermeier, M.; Kopp, M. Expert Views on Therapeutic Climbing—A Multi-Perspective, Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 3535. [Google Scholar] [CrossRef]
- Buechter, R.B.; Fechtelpeter, D. Climbing for preventing and treating health problems: A systematic review of randomized controlled trials. Ger. Med. Sci. 2011, 9, Doc19. [Google Scholar] [CrossRef]
- Liu, S.; Gong, X.; Li, H.; Li, Y. The Origin, Application and Mechanism of Therapeutic Climbing: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 9696. [Google Scholar] [CrossRef]
- Kern, C.; Elmenhorst, J.; Oberhoffer, R. Effect of sport climbing on patients with multiple sclerosis—Hints or evidence? Neurol. Rehabil. 2013, 4, 247–256. [Google Scholar]
- Gallotta, M.C.; Emerenziani, G.P.; Monteiro, M.D.; Iasevoli, L.; Iazzoni, S.; Baldari, C.; Guidetti, L. Psychophysical benefits of rock-climbing activity. Percept. Mot. Ski. 2015, 121, 675–689. [Google Scholar] [CrossRef]
- Mermier, C.M.; Robergs, R.A.; McMinn, S.M.; Heyward, V.H. Energy expenditure and physiological responses during indoor rock climbing. Br. J. Sports Med. 1997, 31, 224–228. [Google Scholar] [CrossRef]
- Rodio, A.; Fattorini, L.; Rosponi, A.; Quattrini, F.M.; Marchetti, M. Physiological adaptation in noncompetitive rock climbers: Good for aerobic fitness? J. Strength Cond. Res. 2008, 22, 359–364. [Google Scholar] [CrossRef]
- Fruhauf, A.; Sevecke, K.; Kopp, M. Current state of the scientific literature on effects of therapeutic climbing on mental health—Conclusion: A lot to do. Neuropsychiatr 2019, 33, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Steimer, J.; Weissert, R. Effects of Sport Climbing on Multiple Sclerosis. Front. Physiol. 2017, 8, 1021. [Google Scholar] [CrossRef] [PubMed]
- Velikonja, O.; Curic, K.; Ozura, A.; Jazbec, S.S. Influence of sports climbing and yoga on spasticity, cognitive function, mood and fatigue in patients with multiple sclerosis. Clin. Neurol. Neurosurg. 2010, 112, 597–601. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- NRZ Rosenhügel. Available online: https://www.nrz.at/ (accessed on 22 March 2023).
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Eppich, W.J.; Gormley, G.J.; Teunissen, P.W. In-Depth Interviews. In Healthcare Simulation Research: A Practical Guide; Nestel, D., Hui, J., Kunkler, K., Scerbo, M.W., Calhoun, A.W., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 85–91. [Google Scholar]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Kuckartz, U. Qualitative Text Analysis: A Guide to Methods, Practice & Using Software; SAGE Publications Ltd.: New York, NY, USA, 2014. [Google Scholar]
- Gabler, H. Motive im Sport: Motivationspsychologische Analysen und empirische Studien; Hofmann: Schorndorf, Germany, 2002. [Google Scholar]
- Jeng, B.; DuBose, N.G.; Martin, T.B.; Silic, P.; Flores, V.A.; Zheng, P.; Motl, R.W. An updated systematic review and quantitative synthesis of physical activity levels in multiple sclerosis. Am. J. Phys. Med. Rehabil. 2023. [Google Scholar] [CrossRef]
- Alpenverein, D.; Alpenverein, Ö.; Südtirol, A. Hoch Hinaus! Böhlau Verlag: Vienna, Austria, 2016. [Google Scholar]
- Gopal, A.; Bonanno, V.; Block, V.J.; Bove, R.M. Accessibility to Telerehabilitation Services for People with Multiple Sclerosis: Analysis of Barriers and Limitations. Int. J. MS Care 2022, 24, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y.; Takahashi, T.; Sawa, R.; Saitoh, M.; Morisawa, T.; Kagiyama, N.; Kasai, T.; Dinesen, B.; Hollingdal, M.; Refsgaard, J.; et al. Web Portals for Patients with Chronic Diseases: Scoping Review of the Functional Features and Theoretical Frameworks of Telerehabilitation Platforms. J. Med. Internet Res. 2022, 24, e27759. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Watts, P.B. Physiology of difficult rock climbing. Eur. J. Appl. Physiol. 2004, 91, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Gassner, L.; Dabnichki, P.; Langer, A.; Pokan, R.; Zach, H.; Ludwig, M.; Santer, A. The therapeutic effects of climbing: A systematic review and meta-analysis. PMR 2022, 15, 1194–1209. [Google Scholar] [CrossRef] [PubMed]
- Rzepka, M.; Tos, M.; Boron, M.; Gibas, K.; Krzystanek, E. Relationship between Fatigue and Physical Activity in a Polish Cohort of Multiple Sclerosis Patients. Medicina 2020, 56, 726. [Google Scholar] [CrossRef] [PubMed]
- Kalb, R.; Brown, T.R.; Coote, S.; Costello, K.; Dalgas, U.; Garmon, E.; Giesser, B.; Halper, J.; Karpatkin, H.; Keller, J.; et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult. Scler. 2020, 26, 1459–1469. [Google Scholar] [CrossRef]
- Dalgas, U.; Langeskov-Christensen, M.; Stenager, E.; Riemenschneider, M.; Hvid, L.G. Exercise as Medicine in Multiple Sclerosis-Time for a Paradigm Shift: Preventive, Symptomatic, and Disease-Modifying Aspects and Perspectives. Curr. Neurol. Neurosci. Rep. 2019, 19, 88. [Google Scholar] [CrossRef]
- Learmonth, Y.C.; Motl, R.W. Exercise Training for Multiple Sclerosis: A Narrative Review of History, Benefits, Safety, Guidelines, and Promotion. Int. J. Environ. Res. Public Health 2021, 18, 13245. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 1–11. [Google Scholar] [CrossRef]
- Reina-Gutiérrez, S.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; de Arenas-Arroyo, S.N.; López-Muñoz, P.; Álvarez-Bueno, C.; Guzmán-Pavón, M.J.; Torres-Costoso, A. The type of exercise most beneficial for quality of life in people with multiple sclerosis: A network meta-analysis. Ann. Phys. Rehabil. Med. 2022, 65, 101578. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Motl, R.W.; Scudder, M.R.; DeLuca, J. Systematic, Evidence-Based Review of Exercise, Physical Activity, and Physical Fitness Effects on Cognition in Persons with Multiple Sclerosis. Neuropsychol. Rev. 2016, 26, 271–294. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Code | Sex | Age | Duration of Disease (years) | EDSS Score | TC Units Attended |
|---|---|---|---|---|---|
| P1 | female | 59 | 22 | 3.0 | 3 |
| P2 | female | 54 | 24 | 3.5 | 6 |
| P3 | female | 35 | 11 | 3.5 | 11 |
| P4 | male | 37 | 5 | 2.0 | 7 |
| P5 | male | 35 | 1 | 2.5 | 6 |
| Code | Sex | Work Experience (years) | TC Experience (years) |
|---|---|---|---|
| T1 | male | 16 | 4 |
| T2 | female | 6 | 3 |
| T3 | female | 20 | 15 |
| T4 | male | 2 | 2 |
| T5 | male | 9 | 9 |
| T6 | female | 12 | 2 |
| T7 | male | 20 | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiffler, T.; Reiter, E.; Kapan, A.; Kranz, G.; Kotzian, S.T.; Haider, S. Perceptions of Therapeutic Climbing for Patients with Multiple Sclerosis in Neurorehabilitation: A Qualitative Study. Healthcare 2024, 12, 674. https://doi.org/10.3390/healthcare12060674
Schiffler T, Reiter E, Kapan A, Kranz G, Kotzian ST, Haider S. Perceptions of Therapeutic Climbing for Patients with Multiple Sclerosis in Neurorehabilitation: A Qualitative Study. Healthcare. 2024; 12(6):674. https://doi.org/10.3390/healthcare12060674
Chicago/Turabian StyleSchiffler, Tobias, Eva Reiter, Ali Kapan, Gottfried Kranz, Stefan Thomas Kotzian, and Sandra Haider. 2024. "Perceptions of Therapeutic Climbing for Patients with Multiple Sclerosis in Neurorehabilitation: A Qualitative Study" Healthcare 12, no. 6: 674. https://doi.org/10.3390/healthcare12060674
APA StyleSchiffler, T., Reiter, E., Kapan, A., Kranz, G., Kotzian, S. T., & Haider, S. (2024). Perceptions of Therapeutic Climbing for Patients with Multiple Sclerosis in Neurorehabilitation: A Qualitative Study. Healthcare, 12(6), 674. https://doi.org/10.3390/healthcare12060674