
Suicide Interventions in Spain and Japan: A Comparative Systematic Review

 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
- -
- RQ1. What kind of elements were included in the interventions in each country?
- -
- RQ2. What prevention elements were included in Japan, but not in Spain?
- -
- Identify and analyze the specific elements included in suicide interventions implemented in Japan and Spain;
- -
- Compare and contrast the suicide-prevention elements that were part of the interventions in Japan and that were not present in the interventions in Spain;
- -
- Identify successful or innovative practices that could be adapted or implemented in the Spanish context in order to be an example to follow for improving suicide-prevention strategies.
2. Materials and Methods
2.1. Information Databases and Searches
2.2. Data Collection
2.3. Assessment of Risk of Bias and Reporting Quality
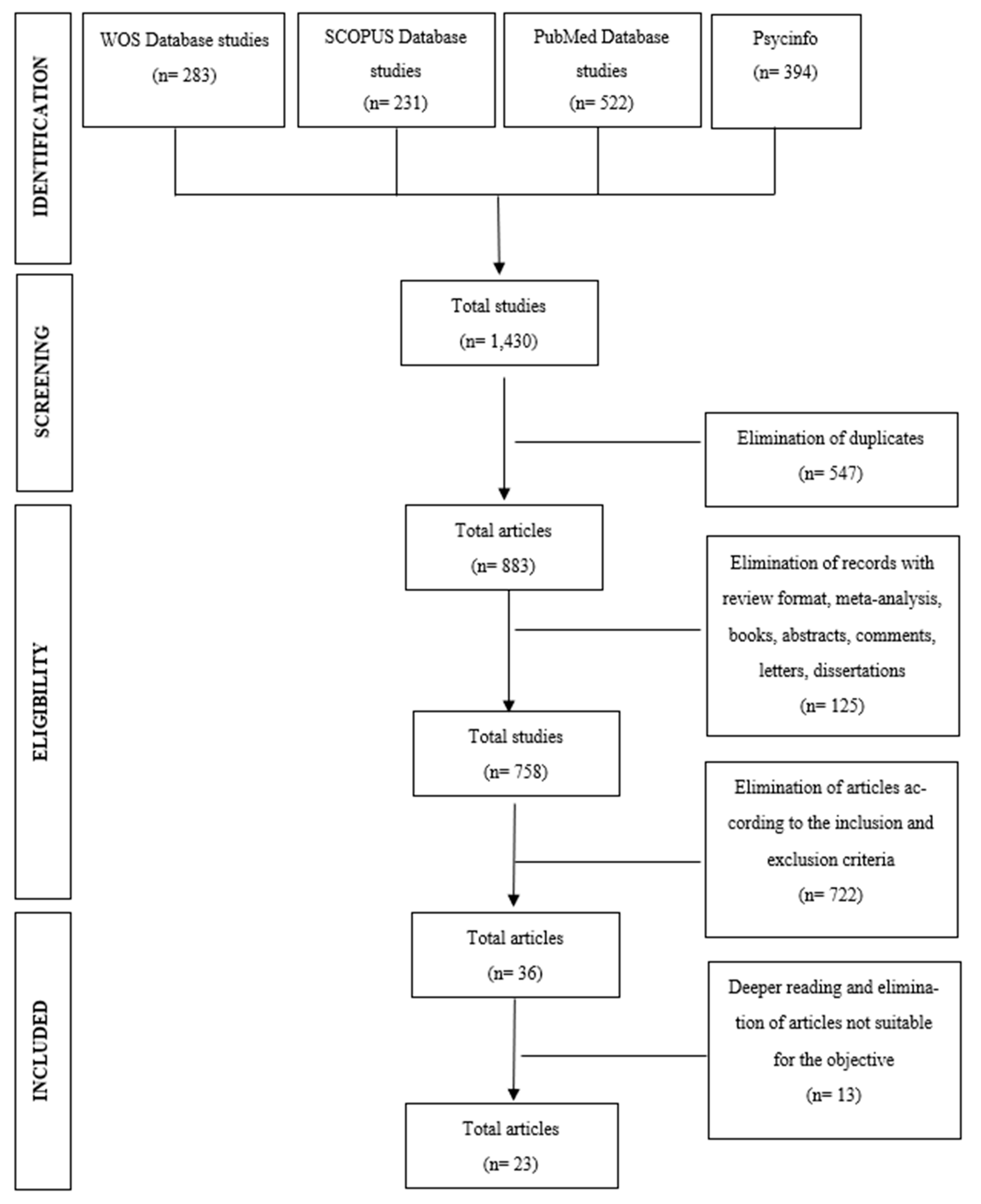
2.4. Study Selection
2.5. Data Analysis
3. Results
3.1. Methodological Quality Analysis
3.2. Sample Characteristics
3.3. Study Characteristics
3.3.1. Training Programs for Other Professional or Non-Professional People in Its Detection and/or Treatment
3.3.2. Health Promotion and Suicide-Prevention Interventions
3.3.3. Treatment of Suicidal Behavior Interventions
4. Discussion
- -
- The prior or subsequent training of those in charge of the interventions;
- -
- Greater complexity/completeness in remote interventions to compensate for the lack of contact;
- -
- A proactive approach in the deployment of interventions.
- -
- Spanish interventions focused on short-term outcomes;
- -
- Most of the interventions dedicated to prevention in Spain are still under evaluation, whereas Japanese interventions showed more contrasting results with long-term positive outcomes;
- -
- Japanese Interventions covered larger groups and mixed age ranges.
4.1. Intervention Types
4.2. Cultural Considerations
4.3. Limitations
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Instituto Nacional de Estadística. Defunciones Según la Causa de Muerte Primer Semestre 2023 (Datos Provisionales) y Año 2022 (Datos Definitivos). Notas de Prensa. pp. 1–9. Available online: https://www.ine.es/prensa/edcm_2022_d.pdf (accessed on 23 May 2023).
- Sáiz, P.A.; Bobes, J. Suicide prevention in Spain: An uncovered clinical need. Rev. Psiquiatr. Salud Ment. 2014, 7, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, M.; Endo, K. National Suicide Prevention, Local Mental Health Resources, and Suicide Rates in Japan. Crisis 2017, 38, 384–392. [Google Scholar] [CrossRef]
- NB Health. The National Plan for Suicide Prevention 1994–1998; Norwegian Board of Health: Oslo, Norway. Available online: https://www.med.uio.no/klinmed/english/research/centres/nssf/articles/prevention/The_national_plan_for_suicide_prevention_1994-1998.pdf (accessed on 23 May 2023).
- Hakanen, J.; Upanne, M. Evaluation strategy for Finland’s suicide prevention project. Crisis 1996, 17, 167–174. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2013: OECD Indicators; OECD Publishing: Paris, France, 2013. [Google Scholar] [CrossRef]
- Specified Non-Profit Organization OVA, Suicide Prevention in Japan. Available online: https://ova-japan.org/?page_id=7222 (accessed on 22 December 2023).
- Statista Research Department. Total Number of Suicides Committed in Japan from 2013 to 2022. Available online: https://www.statista.com/statistics/622065/japan-suicide-number/ (accessed on 2 July 2023).
- Japan Suicides Fall. The Japan Times. 2024. Available online: https://www.japantimes.co.jp/news/2024/01/26/japan/society/japan-suicides-fall/ (accessed on 22 December 2023).
- Matsumoto, R.; Motomura, E.; Okada, M. Impacts of Complete Unemployment Rates Disaggregated by Reason and Duration on Suicide Mortality from 2009–2022 in Japan. Healthcare 2023, 11, 2806. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Crumlish, J.A.; Evans, A.D. The COVID-19 pandemic and treating suicidal risk: The telepsychotherapy use of CAMS. J. Psychother. Integr. 2020, 30, 226–237. [Google Scholar] [CrossRef]
- Sufrate-Sorzano, T.; Jiménez-Ramón, E.; Garrote-Cámara, M.E.; Gea-Caballero, V.; Durante, A.; Júarez-Vela, R.; Santolalla-Arnedo, I. Health Plans for Suicide Prevention in Spain: A Descriptive Analysis of the Published Documents. Nurs. Rep. 2022, 12, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Yonemoto, N.; Kawashima, Y.; Endo, K.; Yamada, M. Implementation of gatekeeper training programs for suicide prevention in Japan: A systematic review. Int. J. Ment. Health Syst. 2019, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Kodaka, M.; Hikitsuchi, E.; Takai, M.; Okada, S.; Watanabe, Y.; Fukushima, K.; Yamada, M.; Inagaki, M.; Takeshima, T.; Matsumoto, T. Current Implementation of and Opinions and Concerns Regarding Suicide Education for Social Work Undergraduate Students in Japan: A Cross-Sectional Study. J. Soc. Work. Educ. 2018, 54, 79–93. [Google Scholar] [CrossRef]
- Office Government of Japan. General Principles of Suicide Prevention Policy. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-12200000-Shakaiengokyokushougaihokenfukushibu/0000172329.pdf (accessed on 2 July 2023).
- Okamura, K.; Komori, T.; Sugimoto, M.; Kawashima, Y.; Yamada, M.; Kishimoto, T. Implementation of evidence-based intervention for suicidal patients admitted to the emergency department: Implications from our real-world experience of assertive case management. Psychiatry Clin. Neurosci. 2021, 75, 108–109. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Wells, G.; Shea, B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch; Losos, M.; Tugwell, P.; Ga, S.W.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: https://api.semanticscholar.org/CorpusID:79550924 (accessed on 27 August 2023).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Albuixech-Garcia, R.; Julia-Sanchis, R.; Fernandez Molina, M.A.; Escribano, S. Impact of the Mental Health Care Continuity-Chain among Individuals Expressing Suicidal Behaviour in a Spanish Sample. Issues Ment. Health Nurs. 2020, 41, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Gabilondo, A.; Aristegi, E.; Gonzalez-Pinto, A.; Martin Zurimendi, J.; Mateos Del Pino, M.; Roca, R.; Zorrilla, I.; Iruin, A. Prevention of Suicidal Behavior with Telemedicine in Patients with a Recent Suicide Attempt: Is a 6-month Intervention Long Enough? Suicide Life Threat. Behav. 2020, 50, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Pons-Baños, J.; Ballester-Ferrando, D.; Riesco-Miranda, L.; Escoté-Llobet, S.; Jiménez-Nuño, J.; Fuentes-Pumarola, C.; Serra-Millàs, M. Sociodemographic and Clinical Characteristics Associated with Suicidal Behaviour and Relationship with a Nurse-Led Suicide Prevention Programme. Int. J. Environ. Res. Public Health 2020, 17, 8765. [Google Scholar] [CrossRef]
- Santamarina-Perez, P.; Mendez, I.; Eiroa-Orosa, F.J.; Singh, M.K.; Gorelik, A.; Picado, M.; Font, E.; Moreno, E.; Martínez, E.; Morer, A.; et al. Visual memory improvement in adolescents at high risk for suicide who are receiving psychotherapy at a community clinic. Psychiatry Res. 2021, 298, 113796. [Google Scholar] [CrossRef] [PubMed]
- Nozawa, K.; Ishii, A.; Asaoka, H.; Iwanaga, M.; Kumakura, Y.; Oyabu, Y.; Shinozaki, T.; Imamura, K.; Kawakami, N.; Miyamoto, Y. Effectiveness of an Online Peer Gatekeeper Training Program for Postsecondary Students on Suicide Prevention in Japan: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2022, 11, e34832. [Google Scholar] [CrossRef] [PubMed]
- Harada, C.; Hatanaka, M.; Kawano, K.; Katsumata, Y.; Kawashima, D.; Shojima, S.; Shiraga, K.; Kawamoto, S. Effect of a suicide prevention program in potentially high-risk adolescents defined by behavioral inhibition and behavioral activation systems. Jpn. J. Psychol. 2019, 90, 351–359. [Google Scholar] [CrossRef]
- Inui-Yukawa, M.; Miyaoka, H.; Yamamoto, K.; Kamijo, Y.; Takai, M.; Yonemoto, N.; Kawanishi, C.; Otsuka, K.; Tachikawa, H.; Hirayasu, Y. Effectiveness of assertive case management for patients with suicidal intent. Psychiatry Res. 2021, 304, 114125. [Google Scholar] [CrossRef]
- Oyama, H.; Sakashita, T. Community-based screening intervention for depression affects suicide rates among middle-aged Japanese adults. Psychol. Med. 2017, 47, 1500–1509. [Google Scholar] [CrossRef]
- Kawashima, Y.; Yonemoto, N.; Kawanishi, C.; Otsuka, K.; Mimura, M.; Otaka, Y.; Okamura, K.; Kinoshita, T.; Shirakawa, O.; Yoshimura, R.; et al. Two-day assertive-case-management educational program for medical personnel to prevent suicide attempts: A multicenter pre–post observational study. Psychiatry Clin. Neurosci. 2020, 74, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Angora, R.; Martinez-Alés, G.; Jiménez Arriero, M.Á.; Navío, M.; Baca-García, E. Evaluation of an Intensive-Reattempt-Prevention Programme Based on Problem-Solving Therapy in a Catchment Area of 430,000 People in Madrid, Spain (Evaluación de un Programa Intensivo de Prevención de Reintento de Suicidio (PIPRS) en un Área de Salud de 4). Actas Esp. Psiquiatr. 2022, 50, 134–143. [Google Scholar]
- López-Goñi, J.J.; Goñi-Sarriés, A. Effectiveness of a telephone prevention programme on the recurrence of suicidal behaviour One-year follow-up. Psychiatry Res. 2021, 302, 114029. [Google Scholar] [CrossRef] [PubMed]
- Pérez, V.; Elices, M.; Toll, A.; Bobes, J.; López-Solà, C.; Díaz-Marsá, M.; Grande, I.; López-Peña, P.; Rodríguez-Vega, B.; Ruiz-Veguilla, M.; et al. The Suicide Prevention and Intervention Study (SURVIVE): Study protocol for a multisite cohort study with nested randomized-controlled trials. Rev. Psiquiatr. Salud Ment. 2021, 16, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Reijas, T.; Ferrer, E.; González, A.; Iglesias, F. Evaluación de Un Programa de Intervención Intensiva En Conducta Suicida. Actas Españolas Psiquiatr. 2013, 41, 279–286. [Google Scholar]
- Santamarina-Perez, P.; Mendez, I.; Singh, M.K.; Berk, M.; Picado, M.; Font, E.; Moreno, E.; Martínez, E.; Morer, A.; Borràs, R.; et al. Adapted Dialectical Behavior Therapy for Adolescents with a High Risk of Suicide in a Community Clinic: A Pragmatic Randomized Controlled Trial. Suicide Life Threat. Behav. 2020, 50, 652–667. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, N.; Takeda, H.; Fujii, Y.; Suzuki, Y.; Kato, T.A.; Fujisawa, D.; Aoyama-Uehara, K.; Otsuka, K.; Mitsui, N.; Asakura, S.; et al. Effectiveness of suicide prevention gatekeeper training for university teachers in Japan. Asian J. Psychiatry 2021, 60, 102661. [Google Scholar] [CrossRef] [PubMed]
- Ono, Y.; Sakai, A.; Otsuka, K.; Uda, H.; Oyama, H.; Ishizuka, N.; Awata, S.; Ishida, Y.; Iwasa, H.; Kamei, Y.; et al. Effectiveness of a multimodal community intervention program to prevent suicide and suicide attempts: A quasi-experimental study. PLoS ONE 2013, 8, e74902. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Kato, T.A.; Sato, R.; Fujisawa, D.; Aoyama-Uehara, K.; Hashimoto, N.; Yonemoto, N.; Fukasawa, M.; Otsuka, K. Effectiveness of brief suicide management training programme for medical residents in Japan: A cluster randomized controlled trial. Epidemiol. Psychiatr. Sci. 2014, 23, 167–176. [Google Scholar] [CrossRef]
- Kawanishi, C.; Aruga, T.; Ishizuka, N.; Yonemoto, N.; Otsuka, K.; Kamijo, Y.; Okubo, Y.; Ikeshita, K.; Sakai, A.; Miyaoka, H.; et al. Assertive case management versus enhanced usual care for people with mental health problems who had attempted suicide and were admitted to hospital emergency departments in Japan (ACTION-J): A multicentre, randomised controlled trial. Lancet Psychiatry 2014, 1, 193–201. [Google Scholar] [CrossRef]
- Tachibana, Y.; Koizumi, N.; Mikami, M.; Shikada, K.; Yamashita, S.; Shimizu, M.; Machida, K.; Ito, H. An integrated community mental healthcare program to reduce suicidal ideation and improve maternal mental health during the postnatal period: The findings from the Nagano trial. BMC Psychiatry 2020, 20, 389. [Google Scholar] [CrossRef] [PubMed]
- Marco, J.H.; Fonseca, S.; Fernandez-Felipe, I.; García-Palacios, A.; Baños, R.; Perez, S.; Garcia-Alandete, J.; Guillen, V. Family connections vs treatment at usual optimized in the treatment of relatives of people with suicidal behavior disorder: Study protocol of a randomized control trial. BMC Psychiatry 2022, 22, 335. [Google Scholar] [CrossRef] [PubMed]
- Espandian, A.; Flórez, G.; Peleteiro, L.F.; Tajes, M.; Sáiz, P.A.; Villa, R.; Bobes, J. Intervention strategies in the prevention of suicidal behavior in substance use disorders patients in times of COVID-19. Adicciones 2021, 33, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Sueki, H.; Ueda, M. Short-Term Effect of the COVID-19 Pandemic on Suicidal Ideation A Prospective Cohort Study. Crisis J. Crisis Interv. Suicide Prev. 2022, 43, 315–322. [Google Scholar] [CrossRef]
- Ogawa, S.; Suzuki, H.; Takahashi, T.; Fujita, K.; Murayama, Y.; Sato, K.; Matsunaga, H.; Motohashi, Y.; Fujiwara, Y. Suicide Prevention Program with Cooperation from Senior Volunteers, Governments, and Schools: A Study of the Intervention Effects of “Educational Lessons Regarding SOS Output” Focusing on Junior High School Students. Children 2022, 9, 541. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Alés, G.; Jiménez-Sola, E.; Román-Mazuecos, E.; Sánchez-Castro, M.P.; de Dios, C.; Rodríguez-Vega, B.; Bravo-Ortiz, M.F. An Emergency Department-Initiated Intervention to Lower Relapse Risk after Attempted Suicide. Suicide Life Threat. Behav. 2019, 49, 1587–1599. [Google Scholar] [CrossRef] [PubMed]
- Mortier, P.; Vilagut, G.; Puértolas Gracia, B.; De Inés Trujillo, A.; Alayo Bueno, I.; Ballester Coma, L.; Cubedo, M.J.B.; Cardoner, N.; Colls, C.; Elices, M.; et al. Catalonia Suicide Risk Code Epidemiology (CSRC-Epi) study: Protocol for a population-representative nested case-control study of suicide attempts in Catalonia, Spain. BMJ Open 2020, 10, e037365. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, D.; Suzuki, Y.; Kato, T.A.T.A.; Hashimoto, N.; Sato, R.; Aoyama-Uehara, K.; Fukasawa, M.; Tomita, M.; Watanabe, K.; Kashima, H.; et al. Suicide intervention skills among Japanese medical residents. Acad. Psychiatry 2013, 37, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Obikane, E.; Sasaki, N.; Imamura, K.; Nozawa, K.; Vedanthan, R.; Cuijpers, P.; Shimazu, T.; Kamada, M.; Kawakami, N.; Nishi, D. Usefulness of Implementation Outcome Scales for Digital Mental Health (iOSDMH): Experiences from Six Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 15792. [Google Scholar] [CrossRef]
- Norimoto, K.; Ikeshita, K.; Kishimoto, T.; Okuchi, K.; Yonemoto, N.; Sugimoto, T.; Chida, F.; Shimoda, S.; Hirayasu, Y.; Kawanishi, C. Effect of assertive case management intervention on suicide attempters with comorbid Axis I and II psychiatric diagnoses: Secondary analysis of a randomised controlled trial. BMC Psychiatry 2020, 20, 311. [Google Scholar] [CrossRef]
- Kawashima, D.; Koga, Y.; Yoshioka, M. Feasibility of brief online gatekeeper training for japanese university students: A randomized controlled trial. Death Stud. 2022, 47, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Furuno, T.; Nakagawa, M.; Hino, K.; Yamada, T.; Kawashima, Y.; Matsuoka, Y.; Shirakawa, O.; Ishizuka, N.; Yonemoto, N.; Kawanishi, C.; et al. Effectiveness of assertive case management on repeat self-harm in patients admitted for suicide attempt: Findings from ACTION-J study. J. Affect. Disord. 2018, 225, 460–465. [Google Scholar] [CrossRef]
- Sakamoto, S.; Tanaka, E.; Kameyama, A.; Takizawa, T.; Takizawa, S.; Fujishima, S.; Nara, M.; Sakashita, T.; Oyama, H.; Ono, Y. The effects of suicide prevention measures reported through a psychoeducational video: A practice in Japan. Int. J. Soc. Psychiatry 2014, 60, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Sola, E.; Martinez-Ales, G.; Roman-Mazuecos, E.; Sanchez-Castro, P.; de Dios-Perrino, C.; Rodriguez-Vega, B.; Ortiz, M.F.B. Implementation of a suicide risk prevention program in the Autonomous Community of Madrid. The ARSUIC experience. Actas Esp. Psiquiatr. 2019, 47, 229–235. [Google Scholar] [PubMed]
- Bergmans, Y.; Kellington, K.; Smith, T.; Pond, A.; Goving, M.; Shelton, E.; Sayegh, C.; Syms, D.; Perivolaris, A. Providing virtual suicide prevention groups for people experiencing suicidality: Pivoting service delivery during the COVID-19 pandemic. Int. Soc. Work. 2021, 64, 801–805. [Google Scholar] [CrossRef]
- Luisa Barrigon, M.; Porras-Segovia, A.; Courtet, P.; Lopez-Castroman, J.; Berrouiguet, S.; Perez-Rodriguez, M.-M.; Artes, A.; Baca-Garcia, E.; MEmind Study Group. Smartphone-based Ecological Momentary Intervention for secondary prevention of suicidal thoughts and behaviour: Protocol for the SmartCrisis V.2.0 randomised clinical trial. BMJ Open 2022, 12, e051807. [Google Scholar] [CrossRef] [PubMed]
- Muela, A.; Balluerka, N.; Sansinenea, E.; Machimbarrena, J.M.; García-Ormaza, J.; Ibarretxe, N.; Eguren, A.; Baigorri, P. A Social-Emotional Learning Program for Suicide Prevention through Animal-Assisted Intervention. Animals 2021, 11, 3375. [Google Scholar] [CrossRef] [PubMed]
- Isabel Cebria, A.; Parra, I.; Pamias, M.; Escayola, A.; Garcia-Pares, G.; Punti, J.; Laredo, A.; Vallès, V.; Cavero, M.; Oliva, J.C.; et al. Effectiveness of a telephone management programme for patients discharged from an emergency department after a suicide attempt: Controlled study in a Spanish population. J. Affect. Disord. 2013, 147, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Cebria, A.I.; Pérez-Bonaventura, I.; Cuijpers, P.; Kerkhof, A.; Parra, I.; Escayola, A.; Garcia-Pares, G.; Oliva, J.C.; Punti, J.; Lopez, D.; et al. Telephone Management Program for Patients Discharged From an Emergency Department after a Suicide Attempt A 5-Year Follow-Up Study in a Spanish Population. Crisis 2015, 36, 345–352. [Google Scholar] [CrossRef]
- Fernández-Artamendi, S.; Al-Halabí, S.; Burón, P.; Rodríguez-Revuelta, J.; Garrido, M.; González-Blanco, L.; Garcia Alvarez, L.; Garcia-Portilla Gonzalez, M.P.; Saiz Martinez, P.A.; Bobes, J.; et al. Prevention of recurrent suicidal behavior: Case management and psychoeducation. Psicothema 2019, 31, 107–113. [Google Scholar]
- Gomes-da-Costa, S.; Solé, E.; Williams, E.; Giménez, A.; Garriga, M.; Pacchiarotti, I.; Vázquez, M.; Cavero, M.; Blanch, J.; Pérez, V.; et al. The impact of the Catalonia Suicide Risk Code (CSRC) in a tertiary hospital: Reduction in hospitalizations and emergency room visits for any reason but not for suicide attempt. Rev. Psiquiatr. Salud Ment. 2021, 16, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Alés, G.; Cruz Rodríguez, J.B.; Lázaro, P.; Domingo-Relloso, A.; Barrigón, M.L.; Angora, R.; Rodríguez-Vega, B.; Jiménez-Sola, E.; Sánchez-Castro, P.; Román-Mazuecos, E.; et al. Cost-effectiveness of a Contact Intervention and a Psychotherapeutic Program for Post-discharge Suicide Prevention. Can. J. Psychiatry 2021, 66, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Pérez, V.; Elices, M.; Prat, B.; Vieta, E.; Blanch, J.; Alonso, J.; Pifarré, J.; Mortier, P.; Cebrià, A.I.; Campillo, M.T.; et al. The Catalonia Suicide Risk Code: A secondary prevention program for individuals at risk of suicide. J. Affect. Disord. 2020, 268, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Sáiz, P.A.; Rodríguez-Revuelta, J.; González-Blanco, L.; Burón, P.; Al-Halabí, S.; Garrido, M.; García-Alvarez, L.; García-Portilla, P.; Bobes, J. Study protocol of a prevention of recurrent suicidal behaviour program based on case management (PSyMAC). Rev. Psiquiatr. Salud Ment. 2014, 7, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, N.; Suzuki, Y.; Kato, T.A.; Fujisawa, D.; Sato, R.; Aoyama-Uehara, K.; Fukasawa, M.; Asakura, S.; Kusumi, I.; Otsuka, K. Effectiveness of suicide prevention gatekeeper-training for university administrative staff in Japan. Psychiatry Clin. Neurosci. 2016, 70, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Nakagami, Y.; Kubo, H.; Katsuki, R.; Sakai, T.; Sugihara, G.; Naito, C.; Oda, H.; Hayakawa, K.; Suzuki, Y.; Fujisawa, D.; et al. Development of a 2-h suicide prevention program for medical staff including nurses and medical residents: A two-center pilot trial. J. Affect. Disord. 2018, 225, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Oyama, H.; Sakashita, T. Long-Term Effects of a Screening Intervention for Depression on Suicide Rates among Japanese Community-Dwelling Older Adults. Am. J. Geriatr. Psychiatry 2016, 24, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Saigo, T.; Hayashida, M.; Tayama, J.; Ogawa, S.; Bernick, P.; Takeoka, A.; Shirabe, S. Prevention of depression in first-year university students with high harm avoidance Evaluation of the effects of group cognitive behavioral therapy at 1-year follow-up. Medicine 2018, 97, e13009. [Google Scholar] [CrossRef] [PubMed]
- Shiraga, K.; Kawano, K.; Masaki, N.; Matoba, Y.; Takeshima, T. Mental health and involvement of residents of the Life Support Advisor in Iwate prefecture after the Great East Japan Earthquake: Suicide prevention in the affected area. J. Ment. Health 2013, 59, 75–83. [Google Scholar]
- Sueki, H.; Ito, J. Suicide prevention through online gatekeeping using search advertising techniques: A feasibility study. Crisis 2015, 36, 267–273. [Google Scholar] [CrossRef]
- Sueki, H.; Takahashi, A.; Ito, J. Changes in Suicide Ideation Among Users of Online Gatekeeping Using Search-Based Advertising. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2022, 27, 1339–1350. [Google Scholar] [CrossRef] [PubMed]
- Hofstra, E.; Nieuwenhuizen, C.; Bakker, M.; Özgül, D.; Elfeddali, I.; Jong, S.J.; van der Feltz-Cornelis, C.M. Effectiveness of suicide prevention interventions: A systematic review and meta-analysis. Gen. Hosp. Psychiatry 2019, 63, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Al-Halabí, S.; Fonseca-Pedrero, E. Suicidal Behavior Prevention: The Time to Act is Now. Clínica Salud 2021, 32, 89–92. [Google Scholar] [CrossRef]
- Matsubayashi, T.; Ueda, M.; Sawada, Y. The effect of public awareness campaigns on suicides: Evidence from Nagoya, Japan. J. Affect. Disord. 2014, 152–154, 526–529. [Google Scholar] [CrossRef]
- Feltz-Cornelis, C.M.; Sarchiapone, M.; Postuvan, V.; Volker, D.; Roskar, S.; Tancic Grum, A.; Carli, V.; McDaid, D.; O’Connor, R.; Maxwell, M.; et al. Best practice elements of multilevel suicide prevention strategies: A review of systematic reviews. Rev. Syst. Rev. Crisis 2011, 32, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Andrada, A.; Ness, S.J.; Alper, J. Engineering, Medicine. Strategies and Interventions to Reduce Suicide. In Proceedings of a Workshop; The National Academies Press: Washington, DC, USA, 2022. [Google Scholar]
- Strategies, P. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/suicide/prevention/index.html (accessed on 25 October 2023).
- Kotera, Y.; Newby, C.; Charles, A.; Ng, F.; Watson, E.; Davidson, L.; Nixdorf, R.; Bradstreet, S.; Brophy, L.; Brasier, C.; et al. Typology of Mental Health Peer Support Work Components: Systematised Review and Expert Consultation. Int. J. Ment. Health Addict. 2023. [Google Scholar] [CrossRef]
- Uneno, Y.; Kotera, Y.; Fujisawa, D. Development of a novel COMPAssion focused online psyChoTherapy for bereaved informal caregivers: The COMPACT feasibility trial protocol. BMJ Open 2022, 12, e067187. [Google Scholar] [CrossRef]
- Chen, J.; Choi, Y.J.; Sawada, Y. How is suicide different in Japan? Jpn. World Econ. 2009, 21, 140–150. [Google Scholar] [CrossRef]
- Anzai, T.; Fukui, K.; Ito, T.; Ito, Y.; Takahashi, K. Excess mortality from suicide during the early COVID-19 pandemic period in Japan: A time-series modeling before the pandemic. J. Epidemiol. 2021, 31, 152–156. [Google Scholar] [CrossRef]
- Fuse-Nagase, Y.; Marutani, T.; Tachikawa, H.; Iwami, T.; Yamamoto, Y.; Moriyama, T.; Yasumi, K. Increase in suicide rates among undergraduate students in japanese national universities during the COVID-19 pandemic. Psychiatry Clin. Neurosci. 2021, 75, 351–352. [Google Scholar] [CrossRef]
- Yoshioka, E.; Hanley, S.J.B.; Sato, Y.; Saijo, Y. Impact of the COVID-19 pandemic on suicide rates in Japan through December 2021: An interrupted time series analysis. Lancet Reg. Health West. Pac. 2022, 24, 100480. [Google Scholar] [CrossRef] [PubMed]
- López-de-la-Nieta, O.; Koeneke Hoenicka, M.A.; Martinez-Rubio, J.L.; Shinohara, K.; Esposito, G.; Iandolo, G. Exploration of the Spanish Version of the Attachment Style Questionnaire: A Comparative Study between Spanish, Italian, and Japanese Culture. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Brás, M.; Elias, P.; Cunha, F.F.; Martins, C.; Nunes, C.; Carmo, C. Vulnerability to Suicide Ideation: Comparative Study between Adolescents with and without Psychosocial Risk. Healthcare 2023, 11, 2663. [Google Scholar] [CrossRef] [PubMed]
- Paez, A. Gray literature: An important resource in systematic reviews. J. Evid.-Based Med. 2017, 10, 233–240. [Google Scholar] [CrossRef]
- OECD. Suicide. Society at a Glance 2016: OECD Social Indicators. 2016. Available online: https://doi.org/10.1787/soc_glance-2016-23-en (accessed on 23 December 2023).
- Kotera, Y.; Taylor, E.; Brooks-Ucheaga, M.; Edwards, A.M. Need for a tool to inform cultural adaptation in mental health interventions. Int. Soc. Study Behav. Dev. Bull. 2023, 1, 2–5. [Google Scholar]



{kind=link}
{kind=link}
| Study | Main Objective | Target Population | Aspects on Which It Intervenes | Place of Action | Duration | Components | Phase (Proven Effectiveness) | Modality | COVID Inclusion |
|---|---|---|---|---|---|---|---|---|---|
| Albuixech-García et al. (2020) [21] | Treatment. Examine sociodemographic factors linked to suicidal behavior and assess the impact of a nursing care protocol on follow-up for such patients. | 213 participants (13–91 years old); intervention group (51.6%); and control group (48.4%). | Suicidal behavior and related factors. | At hospital. | 2 h training session about the protocol. |
| Quasi-experimental study. | Face to face. | No |
| Angora et al. (2022) [30] | Treatment. To evaluate an intensive suicide-reattempt-prevention program using brief problem-solving therapy in conjunction with a case-management approach. | 871 patients (292 received treatment as part of ISRPP and 357 received treatment as usual (TAU)). | Suicide reattempt. | In clinical settings. | Eight weekly sessions. | Psychological assessment, explanation and planification of the intervention (discussion of different ways of coping with suicidal behavior, strategies for the management of suicidal thoughts, problem-solving, and focus on aspects of relapse prevention). | High cost-effectiveness. | Face-to-face consultations and telephone follow-ups. | No |
| Barrigon et al. (2022) [54] | Prevention. To evaluate the effectiveness of a smartphone-based Ecological Momentary Intervention to prevent suicidal thoughts and behavior. | Patients older than 18 years old. | Suicidal thoughts and behavior. | Outpatient intervention. | 12 months. | Safety plan with coping strategies, family contact options, relaxation videos, pre-recorded messages, health resource links, and emergency services. Enhanced app intervention with personalized well-being messages and information on accessing preferential or urgent care. Mental toolbox with relaxation, behavioral activation, and mentalization videos. | Still unproven effectiveness. | Smartphone-based. | No |
| Bergmans et al. (2021) [53] | Prevention. To show the lessons learned by The Skills for Safer Living (SfSL) team in shifting a comprehensive 20-week in-person intervention to a virtual model. | A group that includes all genders over 18 years old who have attempted suicide one or more times. | Key concerns about suicide and strategies and skills to improve mental health. | Online (Microsoft Teams) and telephone support. | 20 weeks. | Key concepts, strategies, and skills for common concerns (anxiety and suicidal ideation). Strategies: validating and humanizing the collective experience. | Pilot phase. | Group in-person intervention to a virtual model. | Yes |
| Cebrià et al. (2013) [56] | Treatment. To determine the effectiveness over one year of a specific telephone management program on patients discharged from an emergency department after a suicide attempt. | 296 patients without age limit. | Time elapsed between initial suicide attempt and subsequent one, changes in the annual rate of patients who reattempted suicide. | Emergency department of a hospital. | 12 months. | Brief interview to re-assess the risk of suicide. Ordinary 5–10 min telephone follow-up, detecting significant changes. And 15–45 min interventions for situations of crisis. In some cases, follow-up was arranged with a primary physician. | Results confirm the effectiveness. | Individual telephone format (fixed line and mobile telephone). | No |
| Cebrià et al. (2015) [57] | To determine the effectiveness over 5 years. | 296 patients without age limit. | Time elapsed between initial suicide attempt and subsequent one. | The emergency department of a hospital. | 12 months. | The experimental intervention included a series of measures to increase adherence to usual treatment and brief interventions in situations of crisis. | Limited long-term effectiveness. | Individual telephone format. | No |
| Espandian et al. (2021) [41] | Prevention. To carry out interviews and interventions for patients with suicide risk and substance-use disorders. | Patients with suicide risk and substance-use disorders. | Suicide risk. | In clinical settings. | Not specified. But recommend established time periods. |
| Limited research proving their effectiveness. | Face to face and by telephone. | Yes |
| Fernández-Artamendi et al. (2019) [58] | Treatment. To evaluate the differential effectiveness of the combination of various strategies for the prevention of the repetition of suicide attempts. | 163 patients with an age range between 18 and 80 who attended emergency services after a suicide attempt. | Suicide reattempts. | Emergency department of a hospital. | 30 months. | Interventions:
| No significant differences between the three groups in the number of suicide attempts nor in the number of patients with more than one suicide attempt. | Face to face, but on the phone if necessary. | No |
| Gabilondo et al. (2020) [22] | Treatment. To analyze the results of a 6-month telephone follow-up program for the prevention of suicidality in adult patients after a suicide attempt. | Adult patients (average age: control group 45.2, intervention group 41.2) treated in hospital emergency departments following a suicide attempt and subsequently discharged after a psychiatric evaluation. | Evaluate the current risk of suicidal behavior; reinforce adherence to treatment and follow-up from a healthcare professional; contribute to psychoeducation; and carry out a crisis intervention in case of emergency. | Home. | 6 months. | Psychoeducation; follow-up calls; and crisis intervention in case of an immediate risk situation. | Short-term intervention proved as effective, but not long-term. | Telephone. | No |
| Gomes-da-Costa et al. (2021) [59] | Prevention. To describe the CSRC preventive strategy experience in a tertiary hospital in Barcelona. | 365 patients (59.7% female), mean age 44.9 ranging from 18 to 92 years. | Suicide risk. | At a hospital clinic. | 12 months. | Three phases: 1. Alert and activation phase; 2. The psychiatrist completes the MINI suicidal module from a MINI interview; 3. Follow-up phone call and an appointment in the outpatient clinic. | CSRC protocol reduced hospitalizations and the mental healthcare utilization in the first year after discharge from the psychiatric emergency room. | Face to face and by telephone intervention. | No |
| Jiménez-Sola et al. (2019) [52] | Prevention. To evaluate the suicide-risk prevention program ARSUIC by estimating the degree of implementation, fulfilment, and effectiveness. | 1633 patients (mean age 39.08–42.85), who received medical and mental healthcare at the emergency department due to a suicide attempt. | Time between discharge and the first outpatient visit, proportion of suicide reattempts, attempt rate per person—year and time between attempts. | At the hospital. | Without specifying, an appointment with an outpatient psychiatrist. | Appointments with a psychiatrist without training in suicide prevention within a maximum of 7 days following discharge, plus their outpatients’ usual appointments. | Reduced the time between discharge after a suicide attempt and the first outpatient appointment. Decreased suicide attempts due to reattempts and the rate of attempts per patient and year. | Observational, retrospective. | No |
| López-Goñi et al. (2021) [31] | Treatment. To analyze the sociodemographic and clinical characteristics of the TFP group and the routine treatment group; to compare the differences between both groups, as well as the recurrence of suicidal behavior. | Patients older than 18 years admitted for a psychiatric emergency. The first sample n = 207. In the second, n = 203. | Suicidal behavior. | Outpatient intervention. | Over 12 months. | Psychiatric specialists conducted assessments, explained the study protocol, and conducted interviews. A year later, a team member reviewed electronic records, collecting specified follow-up variables. | Contradicts the recommendation of the previous research to be applied on patients who had repeated SAs several times and not in first-time patients. | Telephone-based. | No |
| Marco et al. (2022) [40] | Training. Verify the efficacy of the Family Connections intervention. | 124 participants, relatives of people diagnosed with suicidal behavior disorders. | Psychological variables: burden, anxiety, depression, and quality of life. | Clinical settings. | 12 2 h sessions once a week. | Psychoeducation, emotion-regulation training, interpersonal-skills training, communication skills training, and problem-solving training. | Results confirm the effectiveness. | Group, face-to-face format. | No |
| Martínez-Alés et al. (2021) [60] | Treatment. To determine the cost-effectiveness of two strategies for post-discharge suicide prevention, an enhanced contact intervention based on repeated in-person and telephone contacts, and an individual 2-month-long problem-solving psychotherapy program. | 1492 patients aged older than 18 years old. | Post-discharge suicide relapse. | In each general hospital’s emergency department. | Three outpatient appointments and telephone follow-ups; 2-month program of weekly individual psychotherapy sessions. | Individual psychotherapy based on a problem-solving-therapy approach, and 15-min-long follow-up telephone calls at months 1, 6, and 12. | Cost-effectiveness analysis. | Face to face and telephone. | No |
| Martínez-Alés et al. (2019) [44] | Treatment. To evaluate the clinical effectiveness of an intervention at reducing the risk of relapse among patients discharged from the emergency department after a suicide attempt. | 1775 patients, mean age 40.5, treated at a general hospital ED due to a suicide attempt. | Risk of relapse after a suicide attempt. | At an emergency department in a hospital. | A single appointment. | Follow up on single appointment within 7 days after discharge following a suicide attempt. | Confirm effectiveness. | Face to face. | No |
| Muela et al. (2021) [55] | Prevention. To describe a pilot study evaluating the Over Come-AAI program for preventing suicidal behavior. | 30 adolescents aged between 14 and 17 years. | Suicidal behavior and non-suicidal self-harm, and improvements in indicators closely related to suicidal behavior (mental pain, hopelessness, and depressive symptoms). | In a residential childcare setting. | Six sessions. | Pretest (evaluation questionnaires), intervention: 1. Facts, beliefs, and myths about suicide, progressive muscle relaxation; 2. Risks and protective factors of suicide and respiratory energization; 3. Warning signs of suicide and diaphragmatic breathing; 4. Connectivity, self-pity, and negative criticism and mindfulness; 5. Suicide-risk safety plan and mindfulness; 6. Closure and additional help resources and focus on emotions post-test. | Pilot study. | Group-based. | Yes |
| Pérez et al. (2021) [32] | Prevention. To determine the incidence of suicide attempts in Spain and their main risk factors; and to explore the effectiveness of different secondary prevention programs, compared to treatment as usual. | 2000 people (≥12 years of age) who have made a suicide attempt. | Suicidal behavior. | At the psychiatric emergency ward of public, general, or university hospital. | 12 months. | SURVIVE trial involves two interventions:
| Data will be obtained on the effectiveness of secondary prevention programs. | Face to face and telephone-based. | No |
| Pérez et al. (2020) [61] | Prevention. To describe the Catalonia Suicide Risk Code and its implementation. | 12,596 patients (8077 females with a mean age of 40 years and 4519 males with a mean age of 43) with an activated CSRC. | Detect suicide risk and risk factors like the diagnosis of a life-time psychiatric disorder, stressful life events, and hopelessness. | The emergency department of a hospital. | Not specified. | Combined risk assessment, appointments with a mental health professional, telephone calls, follow-up care of patients at risk of suicide, and a neuropsychiatric interview (MINI) MINI suicidality module. | Early implementation. | Face to face and telephone. | No |
| Pons-Baños et al. (2020) [23] | Prevention. To identify the sociodemographic and clinical characteristics of individuals with suicidal behavior, and to analyze differences between non-participants and participants in a nurse-led prevention program. | 753 adult patients (464 women) with suicidal behavior, mean age 43.44. | Suicidal behavior. | At hospital. | Over 12 months. | Coping strategies, crisis intervention, anxiety reduction, counselling, cognitive restructuring, and preventing substance abuse. | Effective intervention. | Face to face and by telephone intervention. | No |
| Reijas et al. (2013) [33] | Treatment. To evaluate the effectiveness in reducing repeated suicide attempts in the Intensive Intervention Program (IIP). | 191 patients, 89 in the treatment group and 102 patients in conventional treatment group, mean age 39.63. | Suicidal relapse. | At hospital. | 10 sessions (6 months). | Three phases, cognitive–behavioral therapy:
| Determine the effectiveness of the treatment. | Face to face and by telephone. | No |
| Sáiz et al. (2014) [62] | Treatment. To describe the PSyMAC protocol, a controlled study designed to prevent the recurrence of suicidal behaviors proposed by case management. | All patients older than 18 years to the Emergency Service of a hospital, after having made a suicide attempt. | Suicidal behavior. | Clinical settings. | Over 12 months, ten sessions (one per week). |
| Effectiveness already proven. | Face-to-face group sessions and telephone. | No |
| Santamarina-Perez et al. (2021) [24] | Prevention. To investigate cognitive differences among adolescents at risk for suicide versus healthy controls and identify cognitive changes associated with response to psychotherapy among adolescents at high risk for suicide. | 35 adolescents (12–17 years old) at high risk for suicide, and 14 healthy control adolescents. | Visual memory (lower performance on verbal memory and processing speed may be associated with a high risk for suicide). | Clinical settings, outpatient clinic. | 16 weeks. |
| Concludes that visual memory may be a potential marker of response to treatment in adolescents at high risk for suicide. | Face to face and intersession telephone contacts. Individual and group sessions. Adolescents and parents attended these GS separately. | No |
| Santamarina-Pérez et al. (2020) [34] | Prevention. To compare the effectiveness of an adapted form of Dialectical Behavior Therapy for Adolescents (DBT-A) and treatment as usual, plus group sessions (TAU + GS) to reduce suicidal risk for adolescents. | Hospital patients aged between 12 and 17 years 11 months with a high risk of suicide and with at least one parent or guardian willing to participate in family sessions. | Frequency of non-suicidal self-injury and number of suicide attempts, changes in the level of functionality, suicidal ideation, and depressive symptoms. | At the hospital. | 4 months. | Adapted form of dialectical behavior therapy for adolescents (DBT-A): individual sessions; weekly sessions of group skills training; weekly consultation team meetings for therapists; and telephone consultation service. | Trial design. | Face to face and by telephone. | No |
| Study | Main Objective | Target Population | Aspects on Which It Intervenes | Place of Action | Duration | Components | Phase (Proven Effectiveness) | Modality | COVID Inclusion |
|---|---|---|---|---|---|---|---|---|---|
| Furuno et al. (2018) [50] | Treatment. To evaluate whether assertive case-management intervention can reduce the number of repeat episodes of overall self-harm during the whole study period. | 914 patients, aged 20 years and older who were admitted to the emergency department. | Episodes of overall self-harm. | Clinical settings. | 18 months. | The ACTION-J intervention. Case management consisted of assessment, planning, encouragement, and coordination. | Similar effects on suicide-attempting patients with comorbid Axis I and II psychiatric diagnoses to those among patients who attempted suicide with only an Axis I diagnosis. | Face to face or by telephone. | No |
| Fujisawa et al. (2013) [46] | Prevention. To evaluate the self-assessed competence and confidence of medical residents about the management of potentially suicidal patients. | 114 medical residents, mean age 27.8. | Suicide-intervention skills. | Clinical settings. | 2 h. | A brief suicide-management education program for medical residents: lecture session (60 min) about depression and suicide, the five-step principles of mental health first aid: (1) Assess risk of suicide or harm; (2) Listen non-judgmentally; (3) Give reassurance and information; (4)Strengthen the demand for professional assistance."; and (5) Encourage self-help strategies. Role-play session (60 min), discussion, and final Q and A time. | Highlighting the need for improved suicide-management programs for junior medical residents in Japanese hospitals. | Group intervention. | No |
| Harada et al. (2019) [26] | Prevention. To examine whether the effects of a suicide-prevention education program for junior high school students were moderated by the risk level of students. | 28 high-risk minor students and 167 low-risk students. | Suicide risk. | Highschool. | four sessions. | GRIP short version contents: Session 1: Mind Pocket. Coping skills. Session 2: KINO (emotional expression game “KINO”). Session 3: Scenario Contest using the DVD teaching materials. Session 4: Scenario Contest 2, learn how to respond when you notice your friend self-harming. | Quantitative effectiveness of the program verified. | Group intervention. | No |
| Hashimoto et al. (2021) [35] | Training. To compare the effect of the GTK program to a general mental health lecture that lacked role play and to examine its generalizability. | 81 teachers from the Hokkaido University Sapporo Campus (mean age 47.2). | Competence and confidence in managing suicide intervention and behavioral intention as a gatekeeper. | At university. | One session with a 30 min lecture about mental health and 2 h role play. | Psychoeducation about mental health (depression and suicide), didactic lecture on basic gatekeeping skills, a video, role playing, and discussion groups. | Effectiveness already proven in middle and high schools; extend these findings to the university settings. | In person. | No |
| Hashimoto et al. (2016) [63] | Training. To investigate the effectiveness of the gatekeeper-training program for administrative staff in Japanese universities. | 76 administrative staff of Hokkaido University, both sexes, mean age: 36.3 | Competence and confidence in the management of suicidal students and behavioral intentions as a gatekeeper. | At university. | 2.5 h. | Psychoeducation about depression and suicide, lecture about suicide-intervention skills, a video, and a role-play session. | First study evaluating this program; significant improvement in scores on competence and confidence in the management of suicidal students. | In person. | No |
| Inui-Yukawa et al. (2021) [27] | Treatment. To examine the effectiveness of assertive case-management intervention in preventing suicidal behavior in self-poisoning patients. | 297 patients in the intervention group and 295 in the control group, 20 yearsor older. | Non-suicidal self-harm episodes and suicide attempts. | Clinical settings. | 18 months. | Assertive continuous case management. Main contents: planning regular interviews, collecting information on the background and treatment status of each patient and an assessment, offering encouragement to seek psychiatric treatment and the provision of psychoeducation, coordinating appointments with psychiatrists and primary care physicians. | Effective intervention when promptly introduced in a hospital setting following a suicide attempt, and especially effective for self-poisoning patients. | Face to face or by telephone. | No |
| Kawanishi et al. (2014) [38] | Treatment. To investigate whether assertive case management can reduce reattempts of suicide in people with mental health problems who had attempted suicide and were admitted to emergency departments. | 914 adult participants aged 20 years and older who had attempted suicide. | Suicide relapse. | At hospital emergency department. | 18 months. | Assertive case management:
| Assertive case management is feasible only in real-world clinical settings. | Face to face or by telephone. | No |
| Kawashima et al. (2022) [49] | Training. To investigate the effectiveness of brief online gatekeeper training for Japanese university students. | 49 university students (25 in a training group and 24 in a control group), age 21.32. | Knowledge about prevention of suicide, intervention skills, self-confidence, and prevention actions. | At university. | 2 months. | Web-based questionnaire that included variables such as suicide-prevention knowledge, skills, self-confidence, and demographic information. Information sheet describing the research objectives following a lecture. Follow-up 2 weeks after the training. | The training group showed an effect in terms of basic knowledge about suicide prevention and self-confidence. | Web-based. | No |
| Kawashima et al. (2020) [29] | Training. To evaluate the effect of an assertive-case-management training program. | 274 medical personnel, mean age 38.09. | Attitudes to suicide prevention, gatekeeper self-efficacy, suicide-intervention skills, and attitudes toward suicide. | At hospital. | 2 days (16 h). | Lectures, group workshops, and role-play practice sessions. Identification of risk factors for suicide, communication with suicide attempters, case management, discussion, psychoeducation for suicide attempters, case management in follow-up intervention, psychological state of bereaved family members and others, interprofessional collaboration and self-care in suicide prevention. | Decreased recurrence of suicidal behavior in attempters and improved attitudes toward suicide prevention. Increased self-efficacy and intervention skills after training. | Group training program | No |
| Nakagami et al. (2018) [64] | Training. To evaluate a newly developed suicide-intervention program among medical staff. | 74 medical staff members (42 nurses, mean age 38.74, 20 residents, mean age 26.35, 12 physicians, mean age 36.58). | Improve the detection and referral of at-risk individuals. | At hospitals. | 2 h. | Changes in knowledge, perceived skills, and confidence in the early intervention of depression and suicide-prevention. | Significant effects on improving perceived skills and confidence. | In person. | No |
| Norimoto et al. (2020) [48] | Treatment. To evaluate whether assertive case management can reduce the repetition of suicidal behaviors in patients who had attempted suicide with comorbid Axis I and II diagnoses. | 914 participants aged 20 years and older. | Suicidal relapse. | Clinical settings. | 18 months. | Assessment, planning, encouragement, and coordination involve the following: (1) Periodic face-to-face or telephone contact during and after emergency-department stays; (2) Gathering information on treatment status and social issues; (3) Encouraging treatment adherence; (4) Coordinating appointments with psychiatrists and primary care physicians; (5) Encouraging treatment return; (6) Referring to social services and support organizations, coordinating resource use; (7) Providing psychoeducation and information on social resources. | Effective and feasible. Reduced incident rate of repeat self-harm. | Internet-based system and face to face or telephone. | No |
| Nozawa et al. (2022) [25] | Training. To describe a research protocol to investigate the effect of a newly developed internet-delivered online peer GKT program to improve post-secondary student self-efficacy as gatekeepers for suicide countermeasures in Japan. | 320 students, 18–29 years old (intervention and control groups). | Self-efficacy as a gatekeeper, literacy of suicide, sense of coherence, stigma, help-seeking styles, psychological distress, self-esteem, resilience, behavior as gatekeepers. | Online. | Six sections (each 85 min). | Contents of the gatekeeper program:
| Results not yet published. | Online intervention. | Yes |
| Ogawa et al. (2022) [43] | Prevention. To examine the impact of a training initiative aimed at fostering support-seeking behavior among students. | 188 students (14 years old). The program involves senior volunteers reading picture books to students, with coordination among local government staff. | Worries and the seeking of social support. | High school. | 50 min lesson. | Activity/Content Part 1: Introduction: Explanation of health center and lesson content; Part 2: Stress coping/SOS output lecture and questions about stress awareness, stress coping, and how to seek help; Part 3: Picture-book reading; Part 4: Conclusion. Distribute support-center leaflets. Review of the lesson and write down thoughts. | There was an impact on the awareness (self-disclosure). | Group intervention. | No |
| Ono et al. (2013) [36] | Prevention. To examine the effectiveness of a community-based multimodal intervention for suicide prevention in rural areas with high suicide rates, compared with a parallel prevention-as-usual control group. | 631,133 persons (under 25, 25–65, or over 65 years old). | Reinforce human relationship and connectedness in the community by focusing on building social support networks and health-related resources. | Local governments and local health authorities collaborated and implemented the intervention programs. | 3.5 years. |
| Unclear effects on the overall rate ratio of the composite outcome in rural areas where the suicide rate was high. | Community-based. | No |
| Oyama and Sakashita (2017) [28] | Prevention. To test if a 4-year community-based intervention, including universal depression screening in target areas, and subsequent care and support for those identified as suffering from depression, would reduce suicide rates among middle-aged adults in rural areas with a high suicide rate. | 90,000 individuals from different Japanese municipalities’ middle-aged adult population (age range of 40–64 years). | Depression and suicide risk. | Clinical settings. | 3 years. | Standardized work plan: distribute public information leaflets and newsletters. Initial screening: depression scale administration. Telephone interview on major depressive episodes. Written feedback via mail. Health professionals contact those with depressive episodes, offering referrals to psychiatrists and support for ongoing treatment. | Statistically greater decrease in suicide rate in the intervention area than the comparison areas. Probably successful in reducing suicide rates. | Screening. | No |
| Oyama and Sakashita (2016) [65] | Prevention. To explore the long-term impact of a universal screening intervention for depression on suicide rates among older community-dwelling adults. | Japanese adults aged 60 years and older. A total of 41,337 people for intervention and 49,073 for control. | Suicide risk. | Clinical settings. | 2-year intervention. | Screening (self-administered questionnaire and telephone interview), educational components (90 min workshops taught by municipal public health nurses and open to the general public, and through local public newsletters), and usual care (regular check-ups). | Long-lasting effects in reducing suicide rates. | Screening. | No |
| Saigo et al. (2018) [66] | Prevention. To clarify how dysfunctional cognitions associated with depressive symptoms improved over 1 year because of G-CBT. | 42 students older than 22 years old. | Depression and dysfunctional cognitions. | At university. | Six sessions (60 min., except for the first and final sessions, which were each 90 min). | Psychoeducation on the CBT theory of the relationship between negative automatic thoughts and psychological symptoms, progressive muscle-relaxation training, cognitive-restructuring training, explanation of attribution theory and training in causal attribution therapy, assertiveness training to improve their social skills. | This G-CBT intervention led to decreases in depression scores. | Group therapy. | No |
| Sakamoto et al. (2014) [51] | Prevention. To report findings on the effect of a psychoeducational video as a suicide-prevention measure in a Japanese rural town. | 2000 residents aged between 30 and 79 years. | Knowledge about local suicide-prevention measures, advice on suicidal ideation and financial issues, attitudes toward suicide, actual and desired familiarity levels with relatives and neighbors, social support, and depressive symptoms. | Residencial. | 4 weeks. | Psychoeducational video. | Effectiveness of suicide-prevention measures. | Individual, in-person visits. | No |
| Shiraga et al. (2013) [67] | Training. To examine the work and mental health of a life-support advisor, and to discuss their role in suicide prevention in the affected area. | 19 respondents from local governments. | Physical symptoms, anxiety, and insomnia, social activity, disorders, and depressive tendency. | At a local government. | Started in 2011. Not specified. | The research method was a questionnaire survey (suicide-prevention questionnaire forms), completed after the training session. | The involvement of lifestyle-support counsellors increased. | Individual survey. | No |
| Sueki and Ito (2015) [68] | Training. To examine the feasibility and effects of online gatekeeping. | 139 consultation service users, mean age 23.8 years old. | To promote help seeking in those using web search services. | Online. | Between July and December 2013. Not specified. | Using Google AdWords, keyword-targeted advertisements for a website, and using suicide-related keywords. The advertisements were linked to the website, encouraging the use of an e-mail consultation service. An e-mail address for consultations and phrases to encourage viewers to use such services. | Using suicide- related search advertisements can allow us to contact suicidal Internet users. | Email-based. | No |
| Sueki et al. (2022) [69] | Prevention. To measure the suicidal ideation and depressive/anxiety tendencies of users of an email-based consultation service for suicide prevention. | 167 participants between 10 s and 50 s. | Suicidal ideation. | Online. | 4 weeks. |
| Suicidal ideation among users at high risk of suicide decreased approximately four weeks after using the service. | Email-based and phone. | No |
| Suzuki et al. (2014) [37] | Training. To evaluate the effectiveness of a brief suicide-management training program for Japanese medical residents compared with the usual lecture on suicidality. | 114 residents (intervention group n = 65, control group n = 49), mean age 27.5. | Suicidal behavior. | Clinical settings. | 2 h. | Structured educational program on managing people with depression and suicidal thoughts. The first part of the program was in lecture format, with factual information on depression and suicide in Japan. Action plans for the management of people with depression and suicidal thoughts. In the second part, a clinical scenario (DVD), role-play, was used. An interactive discussion. | Evaluated the effectiveness of the gatekeeper-training program. | Group intervention. | No |
| Tachibana et al. (2020) [39] | Prevention. To test the effectiveness of the intervention program proposed to reduce suicidal ideation and improve maternal mental health. | 464 women from Nagano’s city, mean age: 31.98 years old. | Prevent suicide in postnatal women at risk of psychosocial problems, reducing suicidal ideation and improving their mental health. | Clinical settings. | During 28 or 60 days postpartum. | Home visits, intervention (psychoeducation, collaboration with family members to create support, commitment to not getting hurt, and support in problem solving, risks, and benefits about psychotropics), and follow-up. | Suggests effectiveness for reducing suicidal ideation and improving maternal mental health. | In person. | No |
| Study | Evaluation Methods | Outcomes | Notable Aspects | |
|---|---|---|---|---|
| Angora et al. (2022) [30] | Assessment not included in the data-collection protocol for this research. | Percentage reduction and delay of suicide attempts. | Reinforcement of common treatment, providing flexible service tailored to the individual circumstances. | |
| Cebrià et al. (2013) [56] | Through an interview and considering days elapsed between the first suicide attempt and the percentages. | Time elapsed between initial suicide attempt and subsequent and short-term effects on suicide rates. | Reinforcement of the in-person intervention with the telephone is essential. | |
| Gabilondo et al. (2020) [22] | Average time until the first suicide reattempt, percentages of patients, survival analysis, and the use of emergency departments’ records. | Increased adhesion to treatment. | Important role of brief contact techniques, like by telephone. | |
| Jiménez-Sola et al. (2019) [52] | Hospital data records and time measurements. | Decrease in suicide attempts and increase in adherence to treatment. | Effectiveness assessment on a population level, considering broader environmental and contextual factors that may influence outcomes. | |
| Marco et al. (2022) [40] | Psychological variables’ scales and questionnaires, quality of life index, and subjects’ opinions. | Favors family acceptance and prevented suicidal behaviors. | Positive impact of changes in family members on the state of patients with suicidal behavior. | |
| Spanish interventions | Martínez-Alés et al. (2021) [60] | Observational methods. | Greater therapeutic contact not only improved patient outcomes, but also reduced costs. | Low cost and flexibility of the intervention. |
| Martínez-Alés et al. (2019) [44] | Observational methods. | Lower risk of suicide relapse. | Suicide risk prevention through enhanced contact post-discharge from healthcare settings (regular phone calls, home visits, assessments of mental health status, and ensuring connection to appropriate care resources). | |
| Reijas et al. (2013) [33] | Cohort comparison. | Lower risk of suicidal relapse. | Specific, simple, and economical intervention that involves comprehensive strategies. | |
| Sáiz et al. (2014) [62] | Psychological scales and numerical data related to suicidal behavior. | Decreased recurrence of suicidal behavior | The inclusion of a psychoeducation group (integrative psychoeducational model) using already-known tools. | |
| Santamarina-Perez et al. (2021) [24] | Sociodemographic scale, DSM-IV-TR diagnosis, global-level functioning scale, intelligence and verbal memory, and learning tests. | Detection of a risk factor for suicide in adolescents. | Effective results but limited to the study design. | |
| Harada et al. (2019) [26] | In-person interviews, Japanese version of the BIS/BAS scale, items related to counselling behavior, observation. | Acquisition of emotional and communication abilities. | Inclusion of emotional education and consultation skills in educational environments where the suicidal risk may still be low. | |
| Hashimoto et al. (2021) [35] | Suicide-intervention-response inventory. | Increase in skills and self-perception of effectiveness in its implementation. | A program focused on teachers rather than students. | |
| Hashimoto et al. (2016) [63] | Self-administered questionnaire. | Increased capacity to manage cases of suicidal behavior among students. | Compensates for the lack of closeness in university environments. | |
| Inui-Yukawa et al. (2021) [27] | In-person and telephone interviews. | Reduced incidence and prevalence of suicide. | It emphasizes early intervention, involving collaboration with community resources. | |
| Kawashima et al. (2022) [49] | Paper-and-pencil psychological assessment measures. | Impact on attitudes towards suicide, skills, and self-efficacy in the application of measures for its prevention. | Inclusion of assertive case management within formal training. | |
| Kawashima et al. (2020) [29] | True-and-false survey, psychological scales, and inventories. | Improved intervention skills and self-confidence in suicide prevention. | Enrichment of the virtual environment (case studies and role-playing) to allow a gatekeeper prevention program at a distance. | |
| Nakagami et al. (2018) [64] | Ten yes-or-no questions to evaluate knowledge, six questions on a five-point Likert scale for confidence, and original questionnaires for skills. | Increasement of mental health knowledge, confidence, and skills to prevent suicide. | Considerable effects in a short time intervention focusing on depression and suicidal behavior. | |
| Japanese interventions | Norimoto et al. (2020) [48] | Incidence proportion of the first episode of recurrent suicidal behavior. | Assertive case management was significantly effective for the Axis I group. | Delivering psychoeducational content and information about social resources before. |
| Oyama and Sakashita (2017) [28] | Observation of suicide rates. | Probably lower suicide rates. | Detection of cases of depression with a predisposition for suicidal behavior. | |
| Oyama and Sakashita (2016) [65] | Difference in changes in suicide rates and number of deaths from national registry data. | Long-lasting effects reducing suicide rates. | Importance of depression screening for suicide prevention. | |
| Saigo et al. (2018) [66] | Paper-and-pencil psychological-assessment measures. | Reduction levels of anxiety and depression that predispose people to suicidal behavior. | Prioritizing cognitive behavioral techniques | |
| Sakamoto et al. (2014) [51] | Questionnaire prepared by the authors. | Increase in knowledge about suicide. | Brief exclusive use of digital media (video) as prevention measure. | |
| Shiraga et al. (2013) [67] | Japanese version of the General Health Questionnaire. | Increased protective factors against suicide, specifically social support. | Community involvement in problems that affect peers. | |
| Sueki and Ito (2015) [68] | Suicidal ideation assessed through text in e-mails. | Increased use of help resources. | A passive procedure from professionals through new technologies to achieve adherence to treatment. | |
| Sueki et al. (2022) [69] | Online questionnaire survey for sociodemographic data, Japanese self-administered Suicidal Ideation Scale and K6 scale. | Significant reduction in suicidal thoughts and tendencies towards depression/anxiety. | Online counselling interventions more appropriate according to women and more effective in the ideation than in the intention phase. | |
| Tachibana et al. (2020) [39] | EPDS screening instrument. | Reduced suicide ideation. | Suicide case management for maternal patients encompasses tailored care and support, involving thorough assessment, monitoring, and intervention to address perinatal challenges and mental health issues. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rives, N.L.; Martín Chaparro, M.d.P.; Dhungel, B.; Gilmour, S.; Colman, R.D.; Kotera, Y. Suicide Interventions in Spain and Japan: A Comparative Systematic Review. Healthcare 2024, 12, 792. https://doi.org/10.3390/healthcare12070792
Martínez-Rives NL, Martín Chaparro MdP, Dhungel B, Gilmour S, Colman RD, Kotera Y. Suicide Interventions in Spain and Japan: A Comparative Systematic Review. Healthcare. 2024; 12(7):792. https://doi.org/10.3390/healthcare12070792
Chicago/Turabian StyleMartínez-Rives, Noelia Lucía, María del Pilar Martín Chaparro, Bibha Dhungel, Stuart Gilmour, Rory D. Colman, and Yasuhiro Kotera. 2024. "Suicide Interventions in Spain and Japan: A Comparative Systematic Review" Healthcare 12, no. 7: 792. https://doi.org/10.3390/healthcare12070792
APA StyleMartínez-Rives, N. L., Martín Chaparro, M. d. P., Dhungel, B., Gilmour, S., Colman, R. D., & Kotera, Y. (2024). Suicide Interventions in Spain and Japan: A Comparative Systematic Review. Healthcare, 12(7), 792. https://doi.org/10.3390/healthcare12070792