Stress Factors for the Paediatric and Adult Palliative Care Multidisciplinary Team and Workplace Wellbeing Solutions

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Data
3.2. Causes and Effects of Stress Perceived by Healthcare Professionals at Work
- -
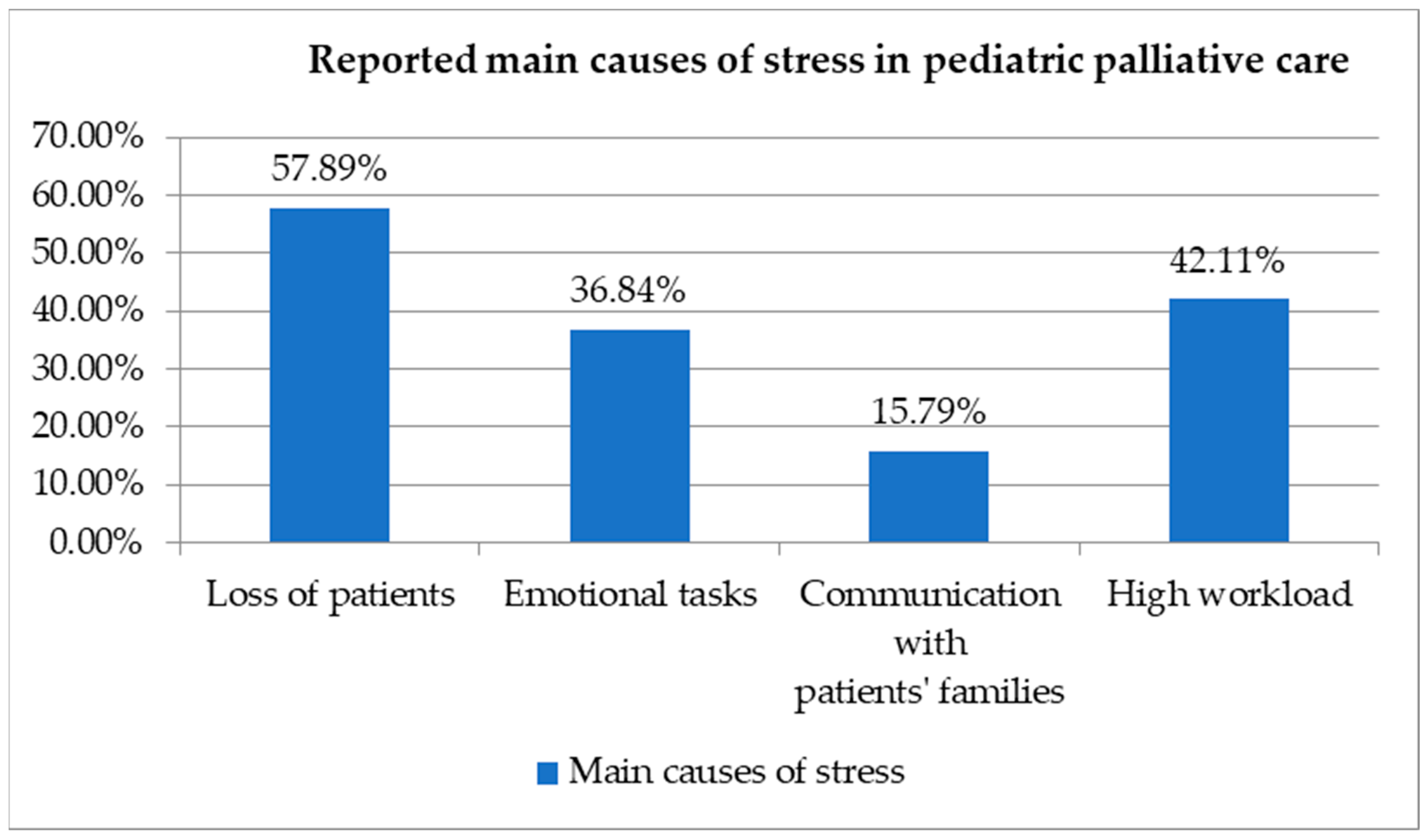
- There were many responses to the question “What do you consider to be the main causes of stress in your work in palliative care?”
- -
- High workload (57.1%) is considered by staff to be one of the main causes of stress in palliative care. The time and effort required to care for patients is higher in order to ensure the quality of care.
- -
- Moreover, 55.4% of respondents said that the difficult emotional burden of dealing with the suffering of patients and their families is a significant cause of stress.
- -
- In total, 6.4% of respondents said that the death of a patient has a profound emotional impact that requires adequate support to cope with the loss.
- -
- Furthermore, 26.8% of professionals reported that dialogue/communication with patients’ families and managing relationships with them was a significant source of stress. Additionally, 1.8% of participants mentioned the difficulty of working with doctors, patients’, and carers’ expectations and bureaucracy, administrative workload, and inadequate pay.
- -
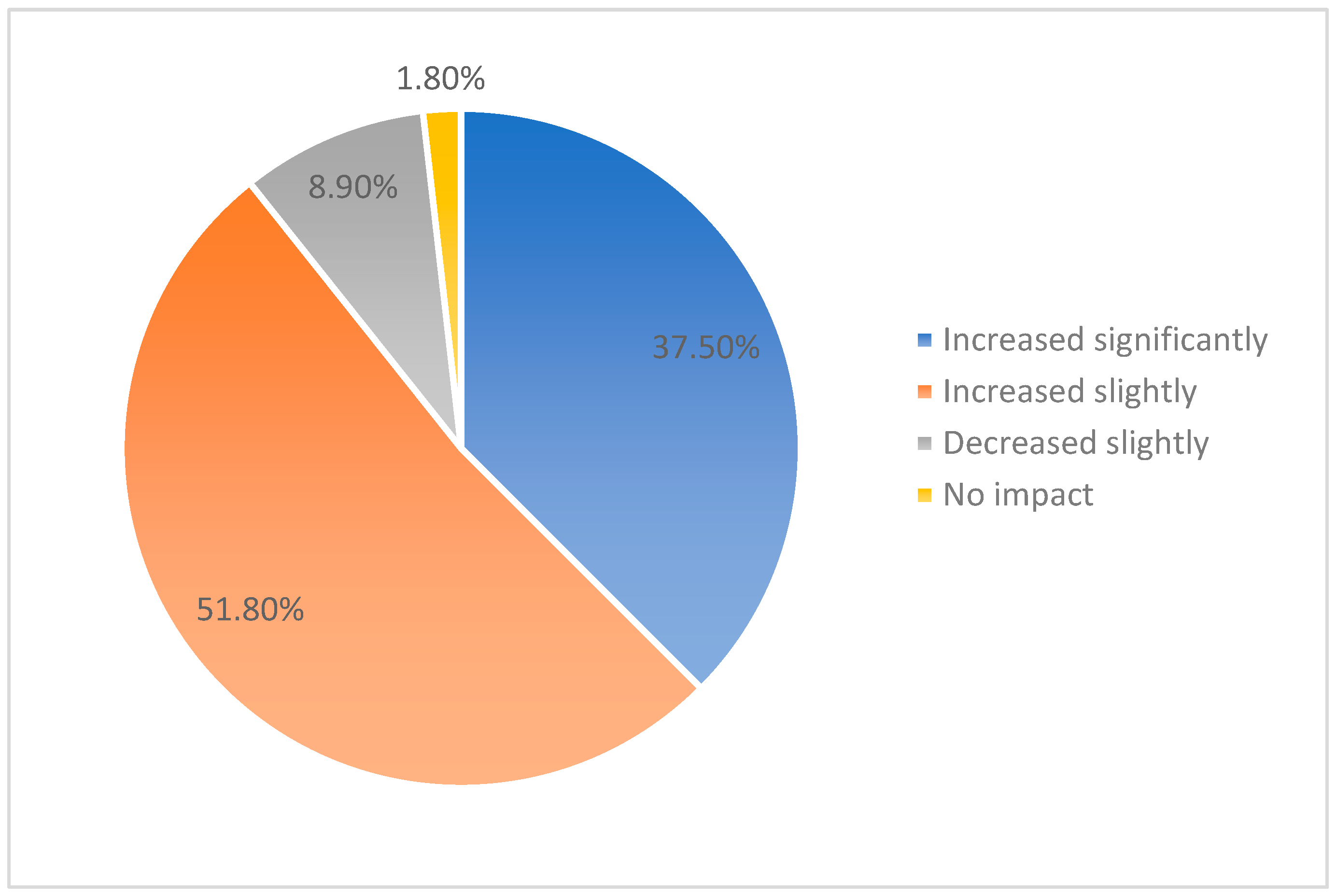
- In response to the question “How has the COVID-19 pandemic affected your level of stress and exhaustion?”, 51.8% of the survey group said that their level of stress and exhaustion had increased significantly in relation to the pandemic due to increased pressure on the healthcare system and challenges related to personal safety and managing the risk of infection.
- -
- Moreover, 37.5% of respondents reported that their levels of stress and fatigue had been slightly affected. Even if they did not experience a significant impact, the pandemic still had a negative effect on their psychological wellbeing and level of exhaustion.
- -
- Moreover, 1.8% of participants reported that their levels of stress and fatigue had decreased slightly because they had found ways to adapt and manage stress.
- -
- Furthermore, 8.9% of respondents reported that the pandemic had no effect on their levels of stress and exhaustion. This category of respondents may represent professionals who already had effective stress management strategies in place or had adequate resources and support (Figure 2).
- -
- In response to the question “How do you think paediatric palliative care differs from adult palliative care in terms of emotional impact and stress?”, 40.7% of respondents felt that there were differences in communication with patients and their families. Dealing with children and their parents involves complex, sensitive issues and making difficult decisions in a way that is appropriate to the child’s age and development.
- -
- In total, 72.2% of respondents cited special challenges related to children’s needs as a major stressor. Children have complex medical needs and can experience high levels of distress that are difficult to manage.
- -
- Moreover, 74.1% of paediatric palliative care professionals feel a strong emotional connection with the children they care for and their families, with profound satisfactions as well as significant emotional demands.
3.3. Expectations and Solutions for Improving Wellbeing at Work
- -
- In response to the question “What are your main expectations of your workplace in terms of supporting and improving wellbeing?”, 53.6% of respondents said that a key expectation was access to training and professional development programmes to improve their skills and keep up with new developments in palliative care. Additionally, 32.1% of workers cited the need for access to psychological counselling, 37.5% the need for emotional support, 51.8% the need for more recognition and appreciation of their work, and 1.8% the need for more respect, honesty, and tolerance.
- -
- When asked “How do you think you can be better helped to cope with difficult work situations?”, 48.2% of employees cited support from colleagues and teamwork, 46.4% considered access to stress management resources important, and 39.3% liked flexibility in working hours. In total, 33.9% said that constructive feedback and regular professional guidance can help them overcome challenging moments at work. Moreover, 5.4% mentioned other means of support: a balanced organisational climate based on trust and cooperation.
- -
- The open-ended question about additional suggestions for improving working conditions and reducing stress in palliative care had a wide range of responses. These included the following: promoting teamwork, organising team-building activities, increasing the number of vacation days, and providing regular debriefing sessions. This allows professionals to discuss difficult experiences and express their feelings.
- -
- In response to the question “What resources and support do you think would be essential to cope with specific work pressures in pediatric palliative care?”, 54% of workers felt that training in paediatric palliative care was essential to deal with the specific stress. In total, 46% believed that support groups and peer discussions are valuable resources for stress management, 40% would like to receive specialised psychological support, and 60% considered it was essential to implement organisational policies and practices that take into account the specificities and work challenges of paediatric palliative care as well as their personal health and wellbeing.
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rattner, M. Increasing our understanding of nonphysical suffering within palliative care: A scoping review. Palliat. Support. Care 2022, 20, 417–432. [Google Scholar] [CrossRef] [PubMed]
- Moresco, B.; Moore, D. Pediatric Palliative Care. Hosp. Pract. 2021, 49, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Peláez-Cantero, M.J.; Morales-Asencio, J.M.; Navarro-Mingorance, Á.; Madrid-Rodriguez, A.; Tavera-Tolmo, Á.; Escobosa-Sánchez, O.; Martino-Alba, R. End of life in patients attended by pediatric palliative care teams: What factors influence the place of death and compliance with family preferences? Eur. J. Pediatr. 2023, 182, 2369–2377. [Google Scholar] [CrossRef] [PubMed]
- Rico-Mena, P.; Güeita-Rodríguez, J.; Martino-Alba, R.; Castel-Sánchez, M.; Palacios-Ceña, D. The Emotional Experience of Caring for Children in Pediatric Palliative Care: A Qualitative Study among a Home-Based Interdisciplinary Care Team. Children 2023, 10, 700. [Google Scholar] [CrossRef] [PubMed]
- Buang, S.N.H.; Loh, S.W.; Mok, Y.H.; Lee, J.H.; Chan, Y.H. Palliative and Critical Care: Their Convergence in the Pediatric Intensive Care Unit. Front. Pediatr. 2022, 10, 907268. [Google Scholar] [CrossRef] [PubMed]
- Scholten, N.; Günther, A.L.; Pfaff, H.; Karbach, U. The size of the population potentially in need of palliative care in Germany--an estimation based on death registration data. BMC Palliat. Care 2016, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Aidoo, E.; Rajapakse, D. Overview of paediatric palliative care. BJA Educ. 2018, 19, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Brunetta, J.; Fahner, J.; Legemaat, M.; van den Bergh, E.; Krommenhoek, K.; Prinsze, K.; Kars, M.; Michiels, E. Age-Appropriate Advance Care Planning in Children Diagnosed with a Life-Limiting Condition: A Systematic Review. Children 2022, 9, 830. [Google Scholar] [CrossRef]
- Blazin, L.J.; Cecchini, C.; Habashy, C.; Kaye, E.C.; Baker, J.N. Communicating Effectively in Pediatric Cancer Care: Translating Evidence into Practice. Children 2018, 5, 40. [Google Scholar] [CrossRef]
- Palazzi, D.L.; Lorin, M.I.; Turner, T.L.; Ward, M.A.; Cabrera, A.G. Communicating with Pediatric Patients and Their Families: The Texas Children’s Hospital Guide for Physicians, Nurses and Other Healthcare Professionals; Texas Children’s Hospital: Houston, TX, USA, 2015. [Google Scholar]
- Scaccabarozzi, G.; Amodio, E.; Riva, L.; Corli, O.; Maltoni, M.; Di Silvestre, G.; Turriziani, A.; Morino, P.; Pellegrini, G.; Crippa, M. Clinical Care Conditions and Needs of Palliative Care Patients from Five Italian Regions: Preliminary Data of the DEMETRA Project. Healthcare 2020, 8, 221. [Google Scholar] [CrossRef]
- Siden, H. Pediatric Palliative Care for Children with Progressive Non-Malignant Diseases. Children 2018, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Chelazzi, C.; Villa, G.; Lanini, I.; Romagnoli, S.; Latronico, N. The adult and pediatric palliative care: Differences and shared issues. J. Anesth. Analg. Crit. Care 2023, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Saad, R.; Abu-Saad Huijer, H.; Noureddine, S.; Sailian, S.D. Pediatric palliative care through the eyes of healthcare professionals, parents and communities: A narrative review. Ann. Palliat. Med. 2022, 11, 3292–3314. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.I.; Allsop, M.J.; ElMokhallalati, Y.; Jackson, C.E.; Edwards, H.L.; Chapman, E.J.; Deliens, L.; Bennett, M.I. Duration of palliative care before death in international routine practice: A systematic review and meta-analysis. BMC Med. 2020, 18, 368. [Google Scholar] [CrossRef] [PubMed]
- Edú-Valsania, S.; Laguía, A.; Moriano, J.A. Burnout: A Review of Theory and Measurement. Int. J. Environ. Res. Public Health 2022, 19, 1780. [Google Scholar] [CrossRef] [PubMed]
- Kase, S.M.; Waldman, E.D.; Weintraub, A.S. A cross-sectional pilot study of compassion fatigue, burnout, and compassion satisfaction in pediatric palliative care providers in the United States. Palliat. Support. Care 2019, 17, 269–275. [Google Scholar] [CrossRef]
- Beaune, L.; Muskat, B.; Anthony, S.J. The emergence of personal growth amongst healthcare professionals who care for dying children. Palliat. Support. Care 2018, 16, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Vishnevsky, T.; Quinlan, M.M.; Kilmer, R.P.; Cann, A.; Danhauer, S.C. “The Keepers of Stories”: Personal Growth and Wisdom Among Oncology Nurses. J. Holist. Nurs. 2015, 33, 326–344. [Google Scholar] [CrossRef]
- Rourke, M.T. Compassion Fatigue in Pediatric Palliative Care Providers. Pediatr. Clin. N. Am. 2007, 54, 631–644. [Google Scholar] [CrossRef]
- McConnell, T.; Scott, D.; Porter, S. Healthcare staff ’s experience in providing end-of-life care to children: A mixed-method review. Palliat. Med. 2016, 30, 905–919. [Google Scholar] [CrossRef]
- Sansó, N.; Galiana, L.; Oliver, A.; Pascual, A.; Sinclair, S.; Benito, E. Palliative Care Professionals’ Inner Life: Exploring the Relationships among Awareness, Self-Care, and Compassion Satisfaction and Fatigue, Burnout, and Coping with Death. J. Pain Symptom Manag. 2015, 50, 200–207. [Google Scholar] [CrossRef]
- Choi, E.K.; Kang, J.; Park, H.Y.; Kim, Y.J.; Hong, J.; Yoo, S.H.; Kim, M.S.; Keam, B.; Park, H.Y. Moral Distress Regarding End-of-Life Care among Healthcare Personnel in Korean University Hospitals: Features and Differences Between Physicians and Nurses. J. Korean Med. Sci. 2023, 38, e169. [Google Scholar] [CrossRef] [PubMed]
- Cappi, V.; Riboni, S.; Grana, M.; Pierotti, E.; Ravelli, A.; Sutti, S.; Testa, S.; Spacci, A.; Artioli, G.; Sarli, L.; et al. Health professionals’ perception of appropriateness of care: A qualitative study in Italian pediatric hospices. Acta Biomed. 2020, 91, e2020013. [Google Scholar] [CrossRef]
- Lotz, J.D.; Jox, R.J.; Borasio, G.D.; Führer, M. Pediatric advance care planning from the perspective of health care professionals: A qualitative interview study. Palliat. Med. 2015, 29, 212–222. [Google Scholar] [CrossRef]
- Greenfield, K.; Holley, S.; Schoth, D.E.; Harrop, E.; Howard, R.F.; Bayliss, J.; Brook, L.; Jassal, S.S.; Johnson, M.; Wong, I.; et al. A mixed-methods systematic review and meta-analysis of barriers and facilitators to paediatric symptom management at end of life. Palliat. Med. 2020, 34, 689–707. [Google Scholar] [CrossRef]
- Pereira, A.G.; Linzer, M.; Berry, L.L. Mitigating Moral Injury for Palliative Care Clinicians. Palliat. Med. Rep. 2023, 4, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Pais, P.; Wightman, A. Addressing the Ethical Challenges of Providing Kidney Failure Care for Children: A Global Stance. Front. Pediatr. 2022, 10, 842783. [Google Scholar] [CrossRef] [PubMed]
- Sisk, B.A.; Mack, J.W.; Ashworth, R.; DuBois, J. Communication in pediatric oncology: State of the field and research agenda. Pediatr. Blood Cancer 2018, 65, e26727. [Google Scholar] [CrossRef] [PubMed]
- Klassen, A.; Gulati, S.; Dix, D. Health care providers’ perspectives about working with parents of children with cancer: A qualitative study. J. Pediatr. Oncol. Nurs. 2012, 29, 92–97. [Google Scholar] [CrossRef]
- Connor, E.O.; Corcoran, Y. Caring for a child with a life limiting condition: The experiences of nurses in an intellectual disability service provider. J. Intellect. Disabil. 2022, 26, 938–953. [Google Scholar] [CrossRef]
- Oberholzer, A.E.; Doolittle, B.R. Flourishing, religion, and burnout among caregivers working in pediatric palliative care. Int. J. Psychiatry Med. 2024, 00912174241229926. [Google Scholar] [CrossRef] [PubMed]
- Judith Roach, E.; Al Omari, O.; Elizabeth John, S.; Francis, F.; Arulappan, J.; Shakman, L.; Al Hashmi, A.; Al Sabei, S.; Khalaf, A. Challenges Experienced by Nurses in Providing Pediatric Palliative Care: An Interpretive Phenomenological Analysis. J. Palliat. Care 2023, 38, 355–363. [Google Scholar] [CrossRef]
- Francoeur, C.; Silva, A.; Hornby, L.; Wollny, K.; Lee, L.A.; Pomeroy, A.; Cayouette, F.; Scales, N.; Weiss, M.J.; Dhanani, S. Pediatric Death after Withdrawal of Life-Sustaining Therapies: A Scoping Review. Pediatr. Crit. Care Med. 2024, 25, e12–e19. [Google Scholar] [CrossRef]
- Hansen, G.; Burton-MacLeod, S.; Schellenberg, K.L. ALS Health care provider wellness. Amyotroph. Lateral Scler. Front. Degener. 2023, 25, 299–307. [Google Scholar] [CrossRef]
- Kates, J.; Gerolamo, A.; Pogorzelska-Maziarz, M. The impact of COVID-19 on the hospice and palliative care workforce. Public Health Nurs. 2021, 38, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Nestor, S.; O’ Tuathaigh, C.; O’ Brien, T. Assessing the impact of COVID-19 on healthcare staff at a combined elderly care and specialist palliative care facility: A cross-sectional study. Palliat. Med. 2021, 35, 1492–1501. [Google Scholar] [CrossRef] [PubMed]
- Feeley, T.; Ffrench-O’Carroll, R.; Tan, M.H.; Magner, C.; L’Estrange, K.; O’Rathallaigh, E.; Whelan, S.; Lyons, B.; O’Connor, E. A model for occupational stress amongst paediatric and adult critical care staff during COVID-19 pandemic. Int. Arch. Occup. Environ. Health 2021, 94, 1721–1737. [Google Scholar] [CrossRef] [PubMed]
- Luchian, N.; Popa, M.V.; Duceac, M.; Gurzu, I.L.; Gurzu, B.; Handra, C.; Duceac, L.D. The psychological impact of the COVID-19 pandemic among the medical-sanitary staff, a new challenge. Rom. J. Occup. Med. 2022, 73, 48–54. [Google Scholar] [CrossRef]
- Popa, M.V.; Luchian, N.; Gurzu, B.; Gurzu, I.L.; Duceac, L.D. Neurological complications in infection with the SARS-CoV-2 virus: Parkinson’s disease and the impact on professional reintegration—Case study. Rom. J. Occup. Med. 2022, 73, 35–39. [Google Scholar] [CrossRef]
- Popa, M.V.; Bogdan Goroftei, E.R.; Guțu, C.; Duceac, M.; Marcu, C.; Popescu, M.R.; Druguș, D.; Duceac, L.D. Observational study of post COVID-19 syndrome in healthcare workers infected with SARS-CoV-2 virus: General and oral cavity complications. Rom. J. Oral Rehabil. 2023, 15, 198–207. [Google Scholar]
- Ichim, D.L.; Duceac, D.L.; Marcu, C.; Iordache, A.C.; Ciomaga, I.M.; Luca, A.C.; Mitrea, G.; Goroftei, E.R.; Stafie, L. Synthesis and Characterization of Colistin Intercalated Nanoparticles Used to Combat Multi-Drug Resistant Microorganisms. Rev. Chim. 2019, 70, 3734–3737. [Google Scholar] [CrossRef]
- Duceac, L.D.; Mitrea, G.; Banu, E.L.; Ciuhodaru, M.I.; Ciomaga, I.M.; Ichim, D.L.; Marcu, C.; Luca, A.C. Synthesis and characterization of carbapeneme based nanohybrids as antimicrobial agents for multidrug resistant bacteria. Mater. Plast. 2019, 56, 388–391. [Google Scholar] [CrossRef]
- Duceac, L.D.; Banu, E.A.; Baciu, G.; Lupu, V.V.; Ciomaga, I.M.; Țarcă, E.; Mitrea, G.; Ichim, D.L.; Luca, A.C. Assessment of bacteria resistance according to antibiotics chemical structure. Rev. Chim. 2019, 70, 906–908. [Google Scholar] [CrossRef]
- Duceac, L.D.; Eva, L.; Dabija, M.; Ciuhodaru, T.; Guțu, G.; Romila, L.; Nazarie, S. Prevention and Limitation of Coronavirus SARS-CoV-2 Cases in Hospitals and Dental Medicine Offices. Int. J. Med. Dent. 2020, 24, 149–156. [Google Scholar]
- Vig, E.K. As the Pandemic Recedes, Will Moral Distress Continue to Surge? Am. J. Hosp. Palliat. Care 2022, 39, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Fish, E.C.; Lloyd, A. Moral distress amongst palliative care doctors working during the COVID-19 pandemic: A narrative-focussed interview study. Palliat. Med. 2022, 36, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, A.; Dunleavy, L.; Garner, I.; Preston, N.; Bajwah, S.; Cripps, R.; Fraser, L.K.; Maddocks, M.; Hocaoglu, M.; Murtagh, F.E.; et al. Experiences of staff providing specialist palliative care during COVID-19: A multiple qualitative case study. J. R. Soc. Med. 2022, 115, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.C.H.; Woo, R.K.W.; Kwok, D.K.; Yu, C.T.K.; Chiu, L.M. Impact of COVID-19 on Mental Health of Palliative Care Professionals and Services: A Mixed-Methods Survey Study. Am. J. Hosp. Palliat. Care 2022, 39, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Tertemiz, O.F.; Tüylüoğlu, E. Are signs of burnout and stress in palliative care workers different from other clinic workers? Agri 2020, 32, 79–84. [Google Scholar] [CrossRef]
- Ablett, J.R.; Jones, R.S. Resilience and well-being in palliative care staff: A qualitative study of hospice nurses’ experience of work. Psycho-Oncology 2007, 16, 733–740. [Google Scholar] [CrossRef]
- Dumitrache, M.; Duceac, L.D. Clinical protocols in pediatric palliative care—A need in clinical practice. Paliatia J. Palliat. Care 2023, 16, 44–48. [Google Scholar]
- Pacurari, N.; De Clercq, E.; Dragomir, M.; Colita, A.; Wangmo, T.; Elger, B.S. Challenges of paediatric palliative care in Romania: A focus groups study. BMC Palliat. Care 2021, 20, 178. [Google Scholar] [CrossRef] [PubMed]
- Bowden, M.J.; Mukherjee, S.; Williams, L.K.; DeGraves, S.; Jackson, M.; McCarthy, M.C. Work-related stress and reward: An Australian study of multidisciplinary pediatric oncology healthcare providers. Psycho-Oncology 2015, 24, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Kamau, C.; Medisauskaite, A.; Lopes, B. Orientations can avert psychosocial risks to palliative staff. Psycho-Oncology 2014, 23, 716–718. [Google Scholar] [CrossRef] [PubMed]
- Bresesti, I.; Folgori, L.; De Bartolo, P. Interventions to reduce occupational stress and burn out within neonatal intensive care units: A systematic review. Occup. Environ. Med. 2020, 77, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Markaki, A.; Baird, J.; Murray, P.; Edwards, R. Addressing Healthcare Professional Burnout: A Quality Improvement Intervention. Worldviews Evid. Based Nurs. 2020, 17, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Roseland, K.A.; Cook, M.; Connelly, P.; Dungan, J.R. Decreasing Nurses’ Anxiety about Pediatric End-of-Life Care with Simulation. J. Contin. Educ. Nurs. 2023, 54, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Beavis, J.; Davis, L.; McKenzie, S. Clinical Supervision for Support Workers in Paediatric Palliative Care: A Literature Review. Clin. Child Psychol. Psychiatry 2021, 26, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Ferrell, B.R.; Paice, J.A.; Coyne, P.J.; Economou, D.; Thaxton, C.A.; Wholihan, D.; Battista, V.; Haskamp, A. Outcomes of a National Training Curriculum to Advance Generalist Level Palliative Care. J. Palliat. Med. 2023, 26, 228–234. [Google Scholar] [CrossRef]
- Skedsmo, K.; Nes, A.A.G.; Stenseth, H.V.; Hofsø, K.; Larsen, M.H.; Hilderson, D.; Smis, D.; Hagelin, C.L.; Olaussen, C.; Solberg, M.T.; et al. Simulation-based learning in palliative care in postgraduate nursing education: A scoping review. BMC Palliat. Care 2023, 22, 30. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Purpose | Elements from the Questionnaire | Specific References |
|---|---|---|
| Assessment of stress and burnout in paediatric palliative care |
| Rico-Mena et al. (2023) [4] Blazin et al. (2018) [9] Saad et al. (2022) [14] Kase et al. (2019) [17] Beaune et al. (2018) [18] Pereira et al. (2023) [27] Sansó et al. (2015) [22] |
| Impact of COVID-19 on stress and burnout in palliative care |
| Kates et al. (2021) [36] Feeley et al. (2021) [38] Vig et al. (2022) [46] Bradshaw et al. (2022) [48] Chan et al. (2022) [49] |
| Expectations and solutions regarding the optimization of workplace wellbeing in paediatric palliative care |
| Rico-Mena et al. (2023) [4] Saad et al. (2022) [14] Sansó et al. (2015) [22] Pereira et al. (2023) [27] Green et al. (2020) [57] Beavis et al. (2021) [59] |
| Causes of Perceived Stress at Work | Number of Responses | Percent |
|---|---|---|
| Increased emotional involvement in childcare | 40 | 74.1% |
| Managing children’s suffering | 39 | 72.2% |
| High workload | 32 | 57.1% |
| Emotionally difficult tasks | 31 | 55.4% |
| Influencing personal perspective on life | 30 | 61.2% |
| Patients’ death | 26 | 46.4% |
| Communicating with children’s family | 22 | 26.8% |
| Impact on emotional balance | 18 | 36.7% |
| Impacts on family life | 6 | 12.2% |
| Other | 12 | 10% |
| Expectations and Solutions for Optimising Wellbeing at Work | Number of Responses | Percent |
|---|---|---|
| Training and development programs | 30 | 53.6% |
| Valuation and appreciation | 29 | 51.8% |
| Co-workers support | 27 | 48.2% |
| Access to stress management resources | 26 | 46.4% |
| Flexible working hours | 22 | 39.3% |
| Tasks management support | 21 | 37.5% |
| Positive feedback and regular appraisal | 19 | 33.9% |
| Access to psychological counselling support | 18 | 32.1% |
| Other | 6 | 6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popa, M.V.; Mîndru, D.E.; Hizanu, M.; Gurzu, I.L.; Anton-Păduraru, D.T.; Ștreangă, V.; Gurzu, B.; Guțu, C.; Elkan, E.M.; Duceac, L.D. Stress Factors for the Paediatric and Adult Palliative Care Multidisciplinary Team and Workplace Wellbeing Solutions. Healthcare 2024, 12, 868. https://doi.org/10.3390/healthcare12090868
Popa MV, Mîndru DE, Hizanu M, Gurzu IL, Anton-Păduraru DT, Ștreangă V, Gurzu B, Guțu C, Elkan EM, Duceac LD. Stress Factors for the Paediatric and Adult Palliative Care Multidisciplinary Team and Workplace Wellbeing Solutions. Healthcare. 2024; 12(9):868. https://doi.org/10.3390/healthcare12090868
Chicago/Turabian StylePopa, Maria Valentina, Dana Elena Mîndru, Mihaela Hizanu (Dumitrache), Irina Luciana Gurzu, Dana Teodora Anton-Păduraru, Violeta Ștreangă, Bogdan Gurzu, Cristian Guțu, Eva Maria Elkan, and Letiția Doina Duceac. 2024. "Stress Factors for the Paediatric and Adult Palliative Care Multidisciplinary Team and Workplace Wellbeing Solutions" Healthcare 12, no. 9: 868. https://doi.org/10.3390/healthcare12090868
APA StylePopa, M. V., Mîndru, D. E., Hizanu, M., Gurzu, I. L., Anton-Păduraru, D. T., Ștreangă, V., Gurzu, B., Guțu, C., Elkan, E. M., & Duceac, L. D. (2024). Stress Factors for the Paediatric and Adult Palliative Care Multidisciplinary Team and Workplace Wellbeing Solutions. Healthcare, 12(9), 868. https://doi.org/10.3390/healthcare12090868