
Addressing Younger Workers’ Needs: The Promoting U through Safety and Health (PUSH) Trial Outcomes


Abstract
:1. Introduction
2. Methods
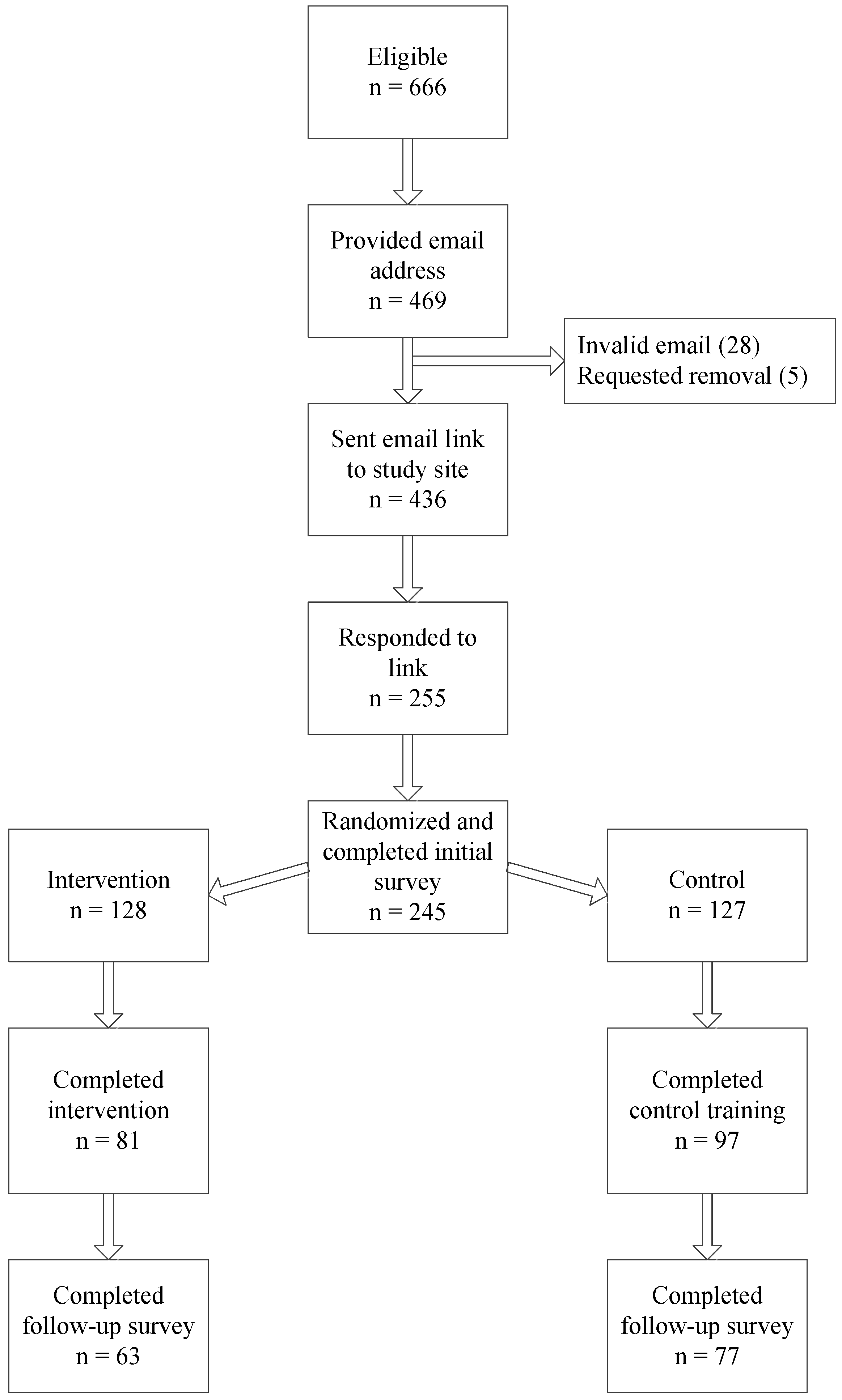
2.1. Study Population
2.2. Survey Instrument
2.3. PUSH Training
2.4. Control Condition
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Feasibility and Acceptability
3.3. Program Effects
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bureau of Labor Statistics. Employment and Unemployment among Youth—Summer 2014. Available online: http://www.bls.gov/news.release/archives/youth_08132014.pdf (accessed on 28 November 2015).
- Estes, C.R.; Jackson, L.L.; Castillo, D.N. Occupational injuries and deaths among younger workers—United States, 1998–2007. Morb. Mortal. Wkly. Rep. 2010, 59, 449–455. [Google Scholar]
- Frone, M.R. Predictors of work injuries among employed adolescents. J. Appl. Psychol. 1998, 83, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Rohlman, D.S.; Parish, M.; Elliot, D.L.; Montgomery, D.; Hanson, G. Characterizing the needs of a young working population: Making the case for total worker health in an emerging workforce. J. Occup. Environ. Med. 2013, 55, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Simoyi, P.; Frederick, L.; Niezen, C. Teenagers’ experience with occupational health and safety issues in West Virginia. Hum. Ecol. Risk Assess. 2001, 4, 1405–1415. [Google Scholar] [CrossRef]
- Westaby, J.D.; Lowe, J.D. Risk-taking orientation and injury among youth workers: Examining social influences of supervisors, coworkers and parents. J. Appl. Psychol. 2005, 90, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Parish, M.; Rohlman, D.S.; Elliot, D.L.; Lasarev, M. Factors associated with occupational injuries in seasonal young workers. Occup. Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.R.; Fischer, F.M.; Nagai, R.; Turte, S.L. Sleep patterns of day-working, evening high-schooled adolescents of San Paulo, Brazil. Chronobiol. Int. 2004, 21, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.R.; Carskadon, M.A. Sleep schedules and daytime functioning in adolescents. Child Dev. 1998, 69, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Sauter, S.L. Integrative approaches to safeguarding the health and safety of workers. Ind. Health 2013, 51, 559–561. [Google Scholar] [CrossRef] [PubMed]
- Merchant, J.A.; Hall, J.L.; Howard, J. Total Worker HealthTM symposium. J. Occup. Environ. Med. 2013, 55, S1–S7. [Google Scholar] [PubMed]
- Holman, D.M.; White, M.C. Dietary behaviors related to cancer prevention among pre-adolescents and adolescents: The gap between recommendations and reality. Nutr. J. 2011. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; Nelson, M.C.; Popkin, B.M. Longitudinal physical activity and sedentary behavior trends: Adolescence to adulthood. Am. J. Prev. Med. 2004, 27, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.J.; Sirard, J.R.; Neumark-Sztainer, D. Adolescents’ attitudes toward sports, exercise, and fitness predict physical activity 5 and 10 years later. Prev. Med. 2011, 52, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and unhealthy weight control behaviors during adolescence: Associations with 10-year changes in body mass index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, L.T.; Chase-Lansdale, P.L.; McDade, T.W.; Adam, E.K. Positive youth, healthy adults: Does positive well-being in adolescence predict better perceived health and fewer risky health behaviors in young adulthood? J. Adolesc. Health 2012, 50, 66–73. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Labor. Training Requirements in Osha Standards and Training Guidelines. Available online: https://www.osha.gov/Publications/osha2254.pdf (accessed on 28 November 2015).
- Runyan, C.W.; Schulman, M.; Dal Santo, J.; Bowling, J.M.; Agans, R.; Ta, M. Work-related hazards and workplace safety of U.S. adolescents working in the retail and service sectors. Pediatrics 2007, 119, 526–534. [Google Scholar] [CrossRef] [PubMed]
- National Counsel for Curriculum and Assessment. Curriculum Overload in Primary Schools. Available online: http://www.ncca.ie/en/Publications/Reports/Curriculum_overload_in_Primary_Schools_An_overview_of_national_and_international_experiences.pdf (accessed on 29 November 2015).
- Lenhart, A.; Purcell, K.; Smith, A.; Zickuhr, K. Social media and mobile internet use among teens and young adults. Available online: http://www.pewinternet.org/2010/02/03/social-media-and-young-adults/ (accessed on 28 November 2015).
- Rideout, V.; Foehr, U.; Roberts, D. Generation M2: Media in the Lives of 8- to 18-Year-Olds; Henry J. Kaiser Family Foundation: Menlo Park, CA, USA, 2010. [Google Scholar]
- Sitzmann, T.; Kraiger, K.; Stewart, D.; Wisher, R. The Comparative effectiveness of web-based and classroom instruction: A meta-analysis. Pers. Psychol. 2006, 59, 623–664. [Google Scholar] [CrossRef]
- Goldberg, L.; MacKinnon, D.P.; Elliot, D.L.; Moe, E.L.; Clarke, G.; Cheong, J. The adolescents training and learning to avoid steroids program: Preventing drug use and promoting healthy behaviors. Arch. Pediatr. Adolesc. Med. 2000, 154, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Elliot, D.L.; Goldberg, L.; Moe, E.L.; DeFrancesco, C.A.; Durham, M.B.; Hix-Small, H. Preventing substance use and disordered eating: Initial outcomes of the ATHENA (athletes targeting healthy exercise and nutrition alternatives) program. Arch. Pediatr. Adolesc. Med. 2004, 158, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Anger, W.K.; Patterson, L.; Fuchs, M.; Will, L.L.; Rohlman, D.S. Learning and recall of worker protection standard (WPS) training in vineyard workers. J. Agromed. 2009, 14, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.; Bloom, T.; Perrin, N.; Anger, W.K. A computer-based training intervention for work supervisors to respond to intimate partner violence. Saf. Health Work 2010, 1, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.; Anger, W.K.; Elliot, D.L.; Wipfli, B.; Gray, M. A new health promotion model for lone workers: Results of the Safety & Health Involvement for Truckers (SHIFT) pilot study. J. Occup. Environ. Med. 2009, 51, 1233–1246. [Google Scholar] [PubMed]
- Anger, W.K.; Rohlman, D.S.; Kirkpatrick, J.; Reed, R.R.; Lundeen, C.A.; Eckerman, D.A. cTrain: A computer-aided training system developed in SuperCard for teaching skills using behavioral education principles. Behav. Res. Methods Instrum. Comput. 2001, 33, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Geller, A.; Rutsch, L.; Kenausis, K.; Zhang, Z. Evaluation of the SunWise school program. J. Sch. Nurs. 2003, 19, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Horton, W. e-Learning by Design; John Wiley & Sons, Inc.: San Francisco, CA, USA, 2011. [Google Scholar]
- Burke, M.J.; Sarpy, S.A.; Smith-Crowe, K.; Chan-Serafin, S.; Salvador, R.O.; Islam, G. Relative effectiveness of worker safety and health training methods. Am. J. Public Health 2006, 96, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.A. Delivering Instruction to Adult Learners, 3rd ed.; Wall & Emerson, Inc.: Toronto, ON, Canada, 2008. [Google Scholar]
- Knowles, M.S.; Holton, E.F., III; Swanson, R.A. The Adult Learner, 8th ed.; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Contento, I.; Balch, G.I.; Bronner, Y.L.; Lytle, L.A.; Maloney, S.K.; Olson, C.M.; Swadener, S.S. The effectiveness of nutrition education and implications for nutrition education policy, programs, and research: A review of research. J. Nutr. Educ. 1995, 27, 277–418. [Google Scholar]
- Lorig, K.R.; Holman, H.R. Self-management and education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rothman, A.; Kiuiniemi, M. Treating people with information: an analysis and review of approaches to community risk information. J. Natl. Cancer Inst. Monogr. 1999, 25, 44–57. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health & Human Services. Preventing Drug Use among Children and Adolescents. 2003. Available online: http://drugabuse.gov/pdf/prevention/redbook.pdf (accessed on 29 November 2015). [Google Scholar]
- Thompson, C.; Koon, E.; Woodwell, W.H., Jr.; Beauvais, J. Training for the Next Economy: An Astd State of the Industry Report on Trends in Employer-Provided Training in the United States for 2002; American Society for Training and Development: Alexandria, VA, USA, 2002. [Google Scholar]
- Moore, D.; Tananis, C.A. Measuring change in a short-term educational program using a retrospective pretest design. Am. J. Educ. 2009, 30, 189–202. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G. Invalidity of true experiments self-report pretest biases. Eval. Rev. 1990, 14, 374–390. [Google Scholar] [CrossRef]
- Militello, L.K.; Kelly, S.A.; Melnky, B.M. Systematic review of text-messaging interventions to promote healthy behaviors in pediatric and adolescent populations: Implications for clinical practice and research. Worldviews Evid. Based Nur. 2012, 9, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating more physically active communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Knowledge Items | Pre-Test Percentage Correct |
|---|---|
| PUSH Training Safety and Lifestyle Items | |
| Best way to tell a coworker to stop horseplay | 68.5 |
| Which is a safety hazard | 97.8 |
| What to say if employer asks you to do something potentially hazardous | 89.3 |
| Which is not a biologic hazard | 80.9 |
| Best way to control a hazard | 49.4 |
| How to respond to being asked to work on new equipment without training | 57.3 |
| Best way to minimize effects of an emergency | 90.5 |
| When to wear appropriate personal protective equipment | 88.8 |
| How to respond to agitated customer | 94.4 |
| How to ask about your safety when asked to do a new task | 83.7 |
| How to talk with employer about safety hazard | 83.2 |
| What statement is not true about sexual harassment | 79.8 |
| Number of recommended servings of fruits and vegetables each day | 47.2 |
| Which is least healthy snack | 53.7 |
| How much exercise is recommended each day by the CDC | 29.8 |
| Which nutrient builds and repairs your body | 93.8 |
| Orange juice is what type of carbohydrate | 57.9 |
| You can be sleep deprived and not know it (T/F) | 97.2 |
| Chicken and fish are always the healthiest of the meat options at a fast food restaurant (T/F) | 55.6 |
| Alcohol and drug use by workers is related to more than half of all workplace injuries and fatalities (T/F) | 76.4 |
| If you are 16 years old and have a valid driver’s license you are allowed to drive a car on public streets as part of your job (T/F) | 39.9 |
| Practicing emergency protocols is an important part of preparing for emergencies (T/F) | 98.3 |
| The law says your employer is responsible for providing you with a safe and healthy workplace (T/F) | 93.3 |
| If you’re injured on the job, your employer must pay for your medical care (T/F) | 62.9 |
| Non-PUSH Content Items | |
| Which one is not an aspect of positive thinking | 86.0 |
| What is the first step to positive thinking | 70.2 |
| Skin cancer can be cured if it is caught early enough (T/F) | 85.4 |
| UV radiation is stronger around water, because the water reflects the sunlight (T/F) | 91.0 |
| Self-talk is the stream of unspoken thoughts in our head. Self-talk can be either positive or negative (T/F) | 96.6 |
| Construct | Items in the Construct | Alpha Reliability |
|---|---|---|
| Health Behavior | I bring healthy snacks to work | 0.59 |
| I eat breakfast everyday | ||
| I stick to healthy food options when I eat out | ||
| I get at least 8 h of sleep a night | ||
| I sometimes drive when I am drowsy or tired * | ||
| I make time for exercise each day | ||
| I avoid engaging in behaviors before work that could jeopardize my attention and judgment | ||
| Safety Behavior | I have looked at the emergency preparedness plans in my workplace | 0.73 |
| I read the information about a chemical before I use it | ||
| I ask for help or training before trying a new task at work | ||
| I communicate professionally at work | ||
| Health Attitudes | Hydration is important to staying focused and alert on the job | 0.76 |
| I think eating breakfast everyday is important | ||
| Proper nutrition is important to workplace safety | ||
| Getting enough sleep at night is important to me | ||
| I know how to deal with my emotions in a healthy way | ||
| I think on the job injuries are a serious and common problem | ||
| An injury I receive on the job could potentially have a long-lasting negative impact on my life | ||
| I know how to protect myself from injuries in my workplace | ||
| I know how to identify hazards in my workplace | ||
| I have the ability to improve the safety of my workplace | ||
| I can make a difference in the safety of my workplace | ||
| I am confident I would respond appropriately |
| Control (n = 97) | PUSH Intervention (n = 81) | |
|---|---|---|
| Demographics | ||
| Age (years) Age (years) | 18.2 (0.2) | 17.7 (0.2) |
| Percent Female Percent Female | 60.8% | 45.7% * |
| Percent White Percent White | 77.1% | 76.5% |
| Graduated High School | 56.7% | 45.7% |
| First Job | 75.3% | 81.5% |
| Anthropometrics | ||
| BMI (self-reported height and weight) | 23.2 (4.1) | 22.7 (4.4) |
| Underweight Underweight | 2.1% | 2.5% |
| Normal Normal | 77.9% | 77.5% |
| Overweight Overweight | 12.6% | 12.5% |
| Obese Obese | 7.4% | 7.5% |
| Attitudes and Behavior Constructs (1 to 7 scale, higher is healthier) | ||
| Health Behavior | 4.9 (0.1) | 4.9 (0.1) |
| Safety Behavior | 5.5 (0.1) | 5.7 (0.1) |
| Health Attitude | 5.8 (0.1) | 6.0 (0.1) |
| Safety Attitude | 5.4 (0.1) | 5.6 (0.2) |
| Other Health Behaviors | ||
| Average Hours Sleep per Night | 7.4 (0.1) | 7.1 (0.1) * |
| Drink Until Drunk Past Month | 26.8% | 19.8% |
| Diet ‡ | ||
| Sugary Snacks | 4.2 (0.2) | 3.3 (0.2) * |
| Drinks with Added Sugar | 3.6 (0.2) | 2.8 (0.2) * |
| Fast Food | 1.5 (0.1) | 1.3 (0.1) |
| Meals from Home Fast Food | 6.1 (0.2) | 5.9 (0.2) |
| Fruits and Vegetables | 6.6 (0.2) | 6.3 (0.2) |
| Exercise | ||
| At least 90 min each week | 77.4% | 85.2% |
| Control n = 97 | PUSH Intervention n = 81 | p Value | Cohen’s d | |||
|---|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | |||
| Knowledge Items | ||||||
| PUSH Training Knowledge Items (number correct) | 18.2 (0.4) | 18.2 (0.4) | 18.4 (0.5) | 20.2 (0.5) | <0.001 | 0.4 |
| Non-PUSH Training Knowledge Items (number correct) | 4.2 (0.1) | 4.6 (0.1) | 4.3 (0.2) | 4.4 (0.2) | 0.07 | −0.21 |
| Safety and Health Behavior and Attitude Constructs | ||||||
| Health Behavior | 4.9 (0.12) | 5.0 (0.13) | 4.9 (0.14) | 4.9 (0.15) | 0.220 | −0.15 |
| Safety Behavior | 5.5 (0.15) | 5.6 (0.15) | 5.7 (0.17) | 5.2 (0.18) | 0.009 | −0.36 |
| Health Attitude | 5.8 (0.13) | 5.9 (0.13) | 6.0 (0.15) | 5.6 (0.16) | 0.013 | −0.37 |
| Safety Attitude | 5.4 (0.13) | 5.6 (0.14) | 5.6 (0.15) | 5.4 (0.16) | 0.015 | −0.37 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rohlman, D.S.; Parish, M.; Elliot, D.L.; Hanson, G.; Perrin, N. Addressing Younger Workers’ Needs: The Promoting U through Safety and Health (PUSH) Trial Outcomes. Healthcare 2016, 4, 55. https://doi.org/10.3390/healthcare4030055
Rohlman DS, Parish M, Elliot DL, Hanson G, Perrin N. Addressing Younger Workers’ Needs: The Promoting U through Safety and Health (PUSH) Trial Outcomes. Healthcare. 2016; 4(3):55. https://doi.org/10.3390/healthcare4030055
Chicago/Turabian StyleRohlman, Diane S., Megan Parish, Diane L. Elliot, Ginger Hanson, and Nancy Perrin. 2016. "Addressing Younger Workers’ Needs: The Promoting U through Safety and Health (PUSH) Trial Outcomes" Healthcare 4, no. 3: 55. https://doi.org/10.3390/healthcare4030055
APA StyleRohlman, D. S., Parish, M., Elliot, D. L., Hanson, G., & Perrin, N. (2016). Addressing Younger Workers’ Needs: The Promoting U through Safety and Health (PUSH) Trial Outcomes. Healthcare, 4(3), 55. https://doi.org/10.3390/healthcare4030055